
Evaluation of Depth of Invasion in Oral Squamous Cell Carcinoma with Ultra-High Frequency Ultrasound: A Preliminary Study

 , ,
, ,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients Flow
2.2. UHFUS Acquisition Protocol and Image Postprocessing
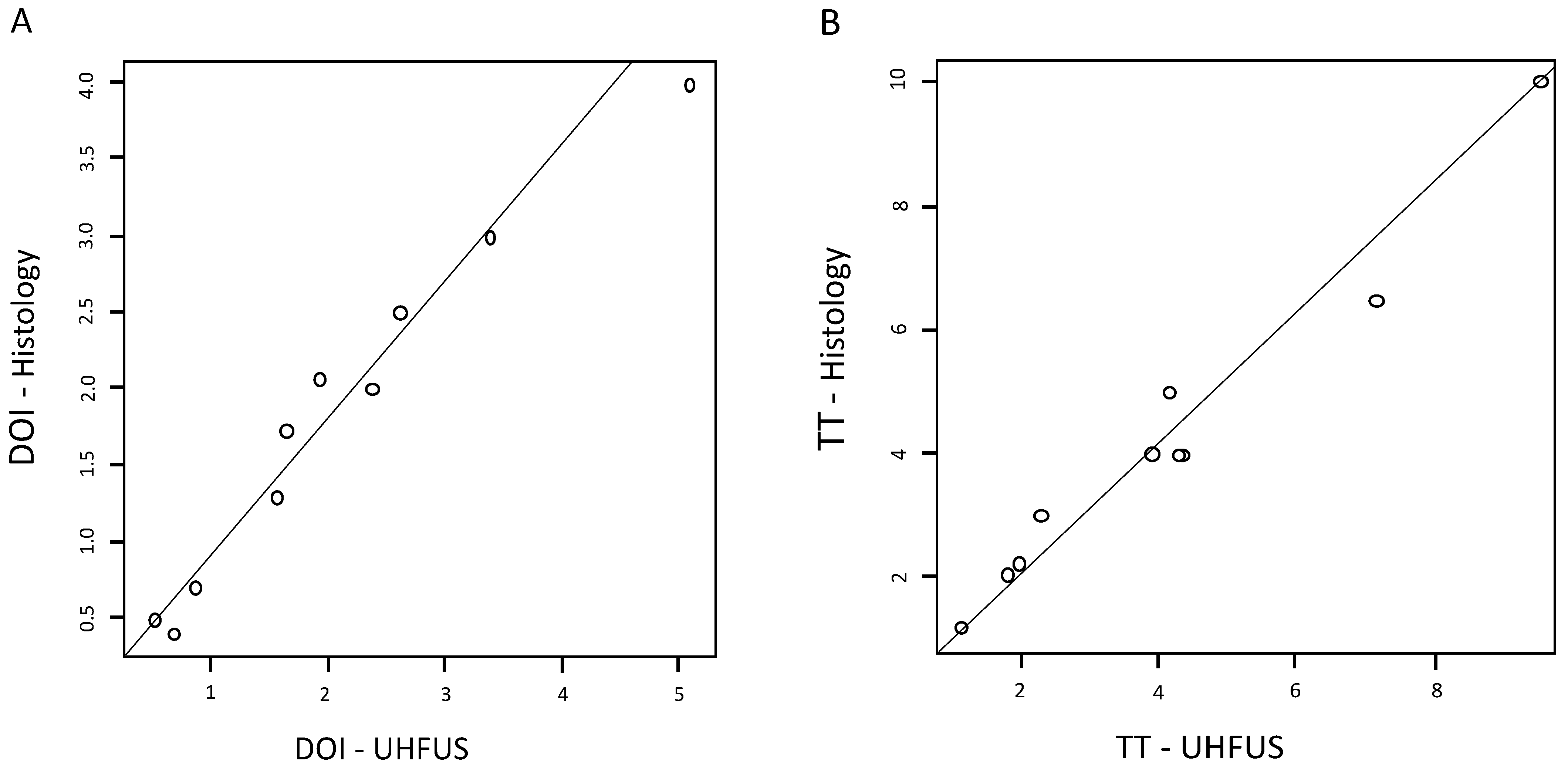
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Histology
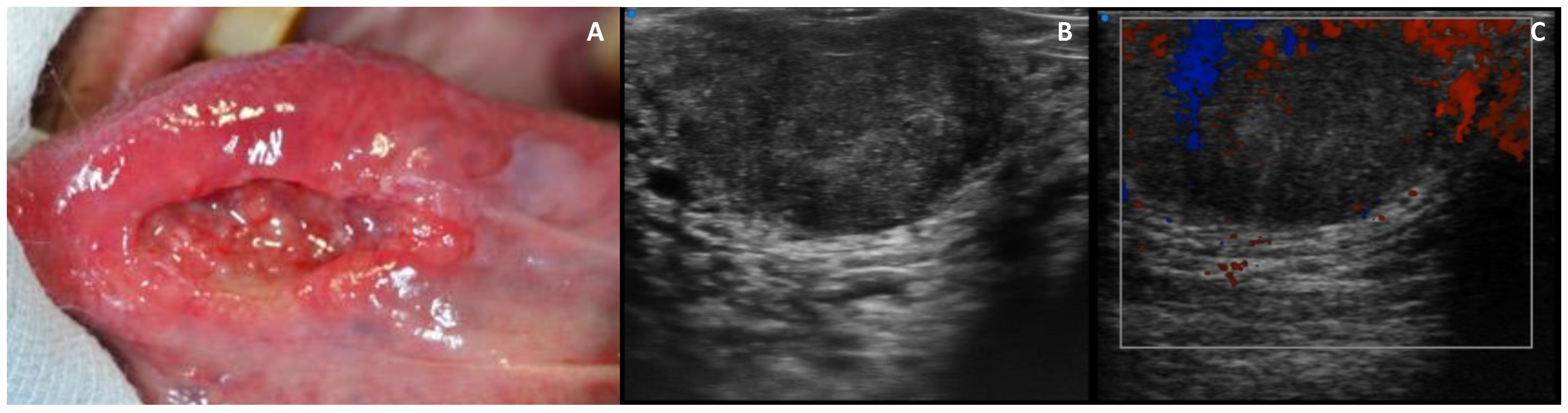
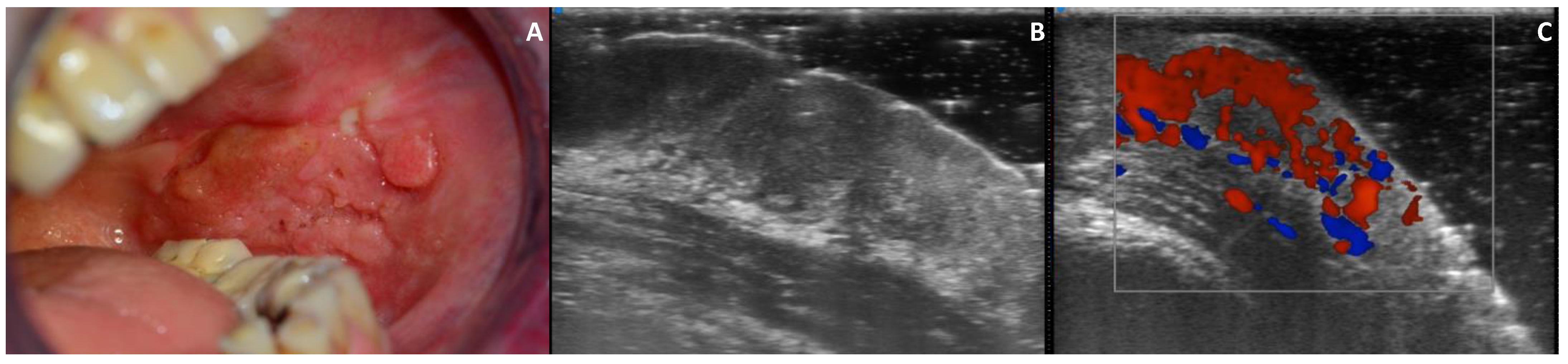
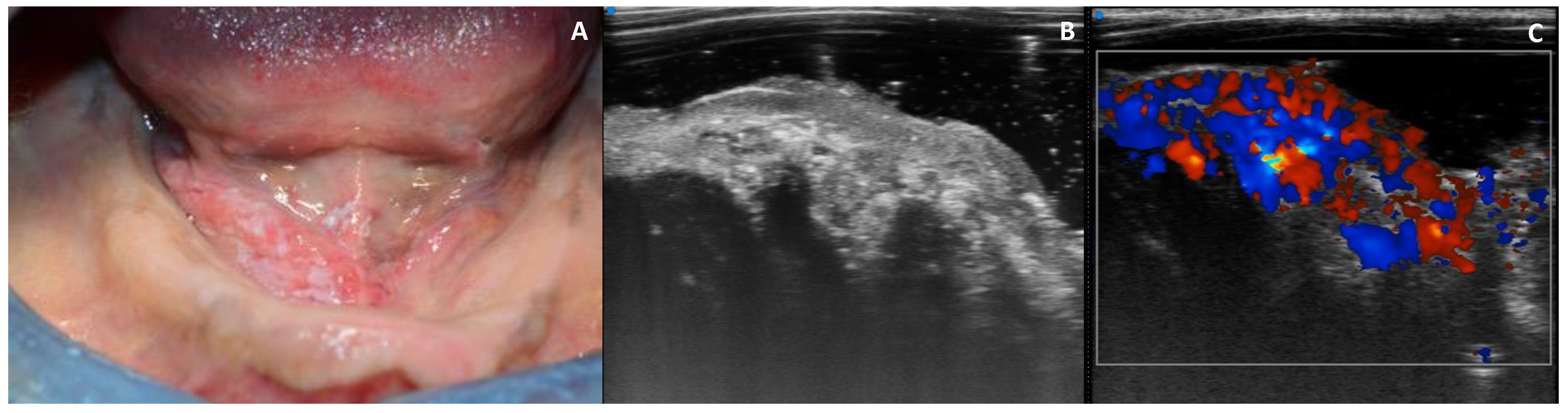
3.3. UHFUS Examination
3.4. Echogenicity
3.5. Vascularization
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dhanuthai, K.; Rojanawatsirivej, S.; Thosaporn, W.; Kintarak, S.; Subarnbhesaj, A.; Darling, M.; Kryshtalskyj, E.; Chiang, C.P.; Shin, H.I.; Choi, S.Y.; et al. Oral cancer: A multicenter study. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e23–e29. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Lin, Z.; Chen, J.; Yang, A.; Zhang, Q.; Xie, C.; Zhang, X.; Yang, Z.; Chen, W.; Song, M. Older age is a risk factor associated with poor prognosis of patients with squamous cell carcinoma of the oral cavity. Eur. Arch. Otorhinolaryngol. 2020, 277, 2573–2580. [Google Scholar] [CrossRef] [Green Version]
- Dik, E.A.; Willems, S.M.; Ipenburg, N.A.; Adriaansens, S.O.; Rosenberg, A.J.; van Es, R.J. Resection of early oral squamous cell carcinoma with positive or close margins: Relevance of adjuvant treatment in relation to local recurrence: Margins of 3 mm as safe as 5 mm. Oral Oncol. 2014, 50, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Nulent, T.J.K.; Noorlag, R.; Van Cann, E.M.; Pameijer, F.A.; Willems, S.M.; Yesuratnam, A.; Rosenberg, A.; de Bree, R.; van Es, R.J. Intraoral ultrasonography to measure tumor thickness of oral cancer: A systematic review and meta-analysis. Oral Oncol. 2018, 77, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Tarabichi, O.; Bulbul, M.G.; Kanumuri, V.V.; Faquin, W.C.; Juliano, A.F.; Cunnane, M.E.; Varvares, M.A. Utility of intraoral ultrasound in managing oral tongue squamous cell carcinoma: Systematic review. Laryngoscope 2019, 129, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Marchi, F.; Filauro, M.; Iandelli, A.; Carobbio, A.; Mazzola, F.; Santori, G.; Parrinello, G.; Canevari, F.; Piazza, C.; Peretti, G. Magnetic resonance vs. intraoral ultrasonography in the preoperative assessment of oral squamous cell carcinoma: A systematic review and meta-analysis. Front. Oncol. 2020, 9, 1571. [Google Scholar] [CrossRef] [Green Version]
- Shintani, S.; Yoshihama, Y.; Ueyama, Y.; Terakado, N.; Kamei, S.; Fijimoto, Y.; Hasegawa, Y.; Matsuura, H.; Matsumura, T. The usefulness of intraoral ultrasonography in the evaluation of oral cancer. Int. J. Oral Maxillofac. Surg. 2001, 30, 139–143. [Google Scholar] [CrossRef]
- Pollaers, K.; Hinton-Bayre, A.; Friedland, P.L.; Farah, C.S. AJCC 8th Edition oral cavity squamous cell carcinoma staging—Is it an improvement on the AJCC 7th Edition? Oral Oncol. 2018, 82, 23–28. [Google Scholar] [CrossRef]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and neck cancers—Major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef]
- Piazza, C.; Montalto, N.; Paderno, A.; Taglietti, V.; Nicolai, P. Is it time to incorporate ‘depth of infiltration’ in the T staging of oral tongue and floor of mouth cancer? Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 81–89. [Google Scholar] [CrossRef] [Green Version]
- van Lanschot, C.; Klazen, Y.P.; de Ridder, M.; Mast, H.; Ten Hove, I.; Hardillo, J.A.; Monserez, D.A.; Sewnaik, A.; Meeuwis, C.A.; Keereweer, S.; et al. Depth of invasion in early stage oral cavity squamous cell carcinoma: The optimal cut-off value for elective neck dissection. Oral Oncol. 2020, 111, 104940. [Google Scholar] [CrossRef]
- Izzetti, R.; Oranges, T.; Janowska, A.; Gabriele, M.; Graziani, F.; Romanelli, M. The application of ultra-high-frequency ultrasound in dermatology and wound management. Int. J. Low. Extrem. Wounds 2020, 19, 334–340. [Google Scholar] [CrossRef]
- Izzetti, R.; Vitali, S.; Aringhieri, G.; Nisi, M.; Oranges, T.; Dini, V.; Ferro, F.; Baldini, C.; Romanelli, M.; Caramella, D.; et al. Ultra-high frequency ultrasound, a promising diagnostic technique: Review of the literature and single-center experience. Can. Assoc. Radiol. J. 2021, 72, 418–431. [Google Scholar] [CrossRef]
- Aringhieri, G.; Izzetti, R.; Vitali, S.; Ferro, F.; Gabriele, M.; Baldini, C.; Caramella, D. Ultra-high frequency ultrasound (UHFUS) applications in Sjogren syndrome: Narrative review and current concepts. Gland Surg. 2020, 9, 2248–2259. [Google Scholar] [CrossRef] [PubMed]
- Izzetti, R.; Fantoni, G.; Gelli, F.; Faggioni, L.; Vitali, S.; Gabriele, M.; Caramella, D. Feasibility of intraoral ultrasonography in the diagnosis of oral soft tissue lesions: A preclinical assessment on an ex vivo specimen. Radiol. Med. 2018, 123, 135–142. [Google Scholar] [CrossRef]
- Izzetti, R.; Vitali, S.; Aringhieri, G.; Oranges, T.; Dini, V.; Nisi, M.; Graziani, F.; Gabriele, M.; Caramella, D. Discovering a new anatomy: Exploration of oral mucosa with ultra-high frequency ultrasound. Dentomaxillofac. Radiol. 2020, 49, 20190318. [Google Scholar] [CrossRef]
- Izzetti, R.; Vitali, S.; Aringhieri, G.; Caramella, D.; Nisi, M.; Oranges, T.; Dini, V.; Graziani, F.; Gabriele, M. The efficacy of ultra-high frequency ultrasonography in the diagnosis of intraoral lesions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 401–410. [Google Scholar] [CrossRef]
- Izzetti, R.; Vitali, S.; Oranges, T.; Dini, V.; Romanelli, M.; Caramella, D.; Gabriele, M. Intraoral ultra-high frequency ultrasound study of oral lichen planus: A pictorial review. Skin Res. Technol. 2020, 26, 200–204. [Google Scholar] [CrossRef] [PubMed]
- Izzetti, R.; Vitali, S.; Gabriele, M.; Caramella, D. Feasibility of a combination of intraoral UHFUS and CBCT in the study of peri-implantitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, e89–e94. [Google Scholar] [CrossRef]
- Oranges, T.; Vitali, S.; Benincasa, B.; Izzetti, R.; Lencioni, R.; Caramella, D.; Romanelli, M.; Dini, V. Advanced evaluation of hidradenitis suppurativa with ultra-high frequency ultrasound: A promising tool for the diagnosis and monitoring of disease progression. Skin Res. Technol. 2020, 26, 513–519. [Google Scholar] [CrossRef]
- Oranges, T.; Janowska, A.; Vitali, S.; Loggini, B.; Izzetti, R.; Romanelli, M.; Dini, V. Dermatoscopic and ultra-high frequency ultrasound evaluation in cutaneous postradiation angiosarcoma. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e741. [Google Scholar] [CrossRef] [PubMed]
- Ferro, F.; Izzetti, R.; Vitali, S.; Aringhieri, G.; Fonzetti, S.; Donati, V.; Dini, V.; Mosca, M.; Gabriele, M.; Caramella, D.; et al. Ultra-high frequency ultrasonography of labial glands is a highly sensitive tool for the diagnosis of Sjögren’s syndrome: A preliminary study. Clin. Exp. Rheumatol. 2020, 38, 210–215. [Google Scholar]
- Izzetti, R.; Ferro, F.; Vitali, S.; Nisi, M.; Fonzetti, S.; Oranges, T.; Donati, V.; Caramella, D.; Baldini, C.; Gabriele, M. Ultra-high frequency ultrasonography (UHFUS)-guided minor salivary gland biopsy: A promising procedure to optimize labial salivary gland biopsy in Sjögren’s syndrome. J. Oral Pathol. Med. 2021, 50, 485–491. [Google Scholar] [CrossRef]
- Izzetti, R.; Nisi, M.; Aringhieri, G.; Vitali, S.; Oranges, T.; Romanelli, M.; Caramella, D.; Graziani, F.; Gabriele, M. Ultra-high frequency ultrasound in the differential diagnosis of oral pemphigus and pemphigoid: An explorative study. Skin Res. Technol. 2021. [Google Scholar] [CrossRef]
- Moeckelmann, N.; Ebrahimi, A.; Tou, Y.K.; Gupta, R.; Low, T.H.; Ashford, B.; Ch’ng, S.; Palme, C.E.; Clark, J.R. Prognostic implications of the 8th edition American Joint Committee on Cancer (AJCC) staging system in oral cavity squamous cell carcinoma. Oral Oncol. 2018, 85, 82–86. [Google Scholar] [CrossRef]
- Songra, A.K.; Ng, S.Y.; Farthing, P.; Hutchison, I.L.; Bradley, P.F. Observation of tumour thickness and resection margin at surgical excision of primary oral squamous cell carcinoma—Assessment by ultrasound. Int. J. Oral Maxillofac. Surg. 2006, 35, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Yesuratnam, A.; Wiesenfeld, D.; Tsui, A.; Iseli, T.A.; Hoorn, S.V.; Ang, M.T.; Guiney, A.; Phal, P.M. Preoperative evaluation of oral tongue squamous cell carcinoma with intraoral ultrasound and magnetic resonance imaging-comparison with histopathological tumour thickness and accuracy in guiding patient management. Int. J. Oral Maxillofac. Surg. 2014, 43, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Angelelli, G.; Moschetta, M.; Limongelli, L.; Albergo, A.; Lacalendola, E.; Brindicci, F.; Favia, G.; Maiorano, E. Endocavitary sonography of early oral cavity malignant tumors. Head Neck 2017, 39, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Natori, T.; Koga, M.; Anegawa, E.; Nakashima, Y.; Tetsuka, M.; Yoh, J.; Kusukawa, J. Usefulness of intra-oral ultrasonography to predict neck metastasis in patients with tongue carcinoma. Oral Dis. 2008, 14, 591–599. [Google Scholar] [CrossRef]
- Brockhoff, H.C., 2nd; Kim, R.Y.; Braun, T.M.; Skouteris, C.; Helman, J.I.; Ward, B.B. Correlating the depth of invasion at specific anatomic locations with the risk for regional metastatic disease to lymph nodes in the neck for oral squamous cell carcinoma. Head Neck 2017, 39, 974–979. [Google Scholar] [CrossRef]
- Rocchetti, F.; Tenore, G.; Montori, A.; Cassoni, A.; Cantisani, V.; Di Segni, M.; Di Gioia, C.; Carletti, R.; Valentini, V.; Polimeni, A.; et al. Preoperative evaluation of tumor depth of invasion in oral squamous cell carcinoma with intraoral ultrasonography: A retrospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Umstattd, L.A.; Mills, J.C.; Critchlow, W.A.; Renner, G.J.; Zitsch, R.P., 3rd. Shrinkage in oral squamous cell carcinoma: An analysis of tumor and margin measurements in vivo, post-resection, and post-formalin fixation. Am. J. Otolaryngol. 2017, 38, 660–662. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Clinical Features of the Lesion | UHFUS Examination | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient | Age | Gender | Smoking Habit (Cigarettes/Day) | Site of Lesion | Presence of the Lesion (Months) | Growth Pattern | VAS | Mean Grey Value Distribution | Standard Deviation | Min | Max |
| 1 | 83 | F | YES (10 cig/day) | Tongue | 8 | Endophytic | 8 | 71.97 | 18.03 | 26.00 | 183.00 |
| 2 | 75 | F | YES (15 cig/day) | Gingiva | 4 | Endophytic | 4 | 61.08 | 40.77 | 9.00 | 235.00 |
| 3 | 68 | M | YES (20 cig/day) | Tongue | 6 | Endophytic | 1 | 60.32 | 15.08 | 20.00 | 126.00 |
| 4 | 58 | F | NO | Gingiva | 3 | Endophytic | 2 | 85.48 | 20.13 | 44.00 | 176.00 |
| 5 | 75 | F | NO | Buccal mucosa | 5 | Exophytic | 9 | 53.69 | 27.03 | 10.00 | 222.00 |
| 6 | 70 | M | NO | Tongue | 6 | Exophytic | 6 | 43.97 | 13.32 | 13.00 | 121.00 |
| 7 | 59 | M | YES (25 cig/day) | Tongue | 3 | Exophytic | 9 | 35.27 | 18.36 | 5.00 | 155.00 |
| 8 | 60 | F | YES (20 cig/day) | Tongue | 6 | Exophytic | 8 | 83.35 | 37.78 | 22.00 | 192.00 |
| 9 | 83 | M | NO | Mouth floor | 12 | Exophytic | 6 | 63.49 | 20.87 | 25.00 | 220.00 |
| 10 | 56 | F | YES (20 cig/day) | Tongue | 12 | Exophytic | 0 | 90.76 | 33.99 | 20.00 | 227.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izzetti, R.; Nisi, M.; Gennai, S.; Oranges, T.; Crocetti, L.; Caramella, D.; Graziani, F. Evaluation of Depth of Invasion in Oral Squamous Cell Carcinoma with Ultra-High Frequency Ultrasound: A Preliminary Study. Appl. Sci. 2021, 11, 7647. https://doi.org/10.3390/app11167647
Izzetti R, Nisi M, Gennai S, Oranges T, Crocetti L, Caramella D, Graziani F. Evaluation of Depth of Invasion in Oral Squamous Cell Carcinoma with Ultra-High Frequency Ultrasound: A Preliminary Study. Applied Sciences. 2021; 11(16):7647. https://doi.org/10.3390/app11167647
Chicago/Turabian StyleIzzetti, Rossana, Marco Nisi, Stefano Gennai, Teresa Oranges, Laura Crocetti, Davide Caramella, and Filippo Graziani. 2021. "Evaluation of Depth of Invasion in Oral Squamous Cell Carcinoma with Ultra-High Frequency Ultrasound: A Preliminary Study" Applied Sciences 11, no. 16: 7647. https://doi.org/10.3390/app11167647