
Evaluation of Organ Dose and Image Quality Metrics of Pediatric CT Chest-Abdomen-Pelvis (CAP) Examination: An Anthropomorphic Phantom Study

 ,
, 
Abstract
:Featured Application
Abstract
1. Introduction
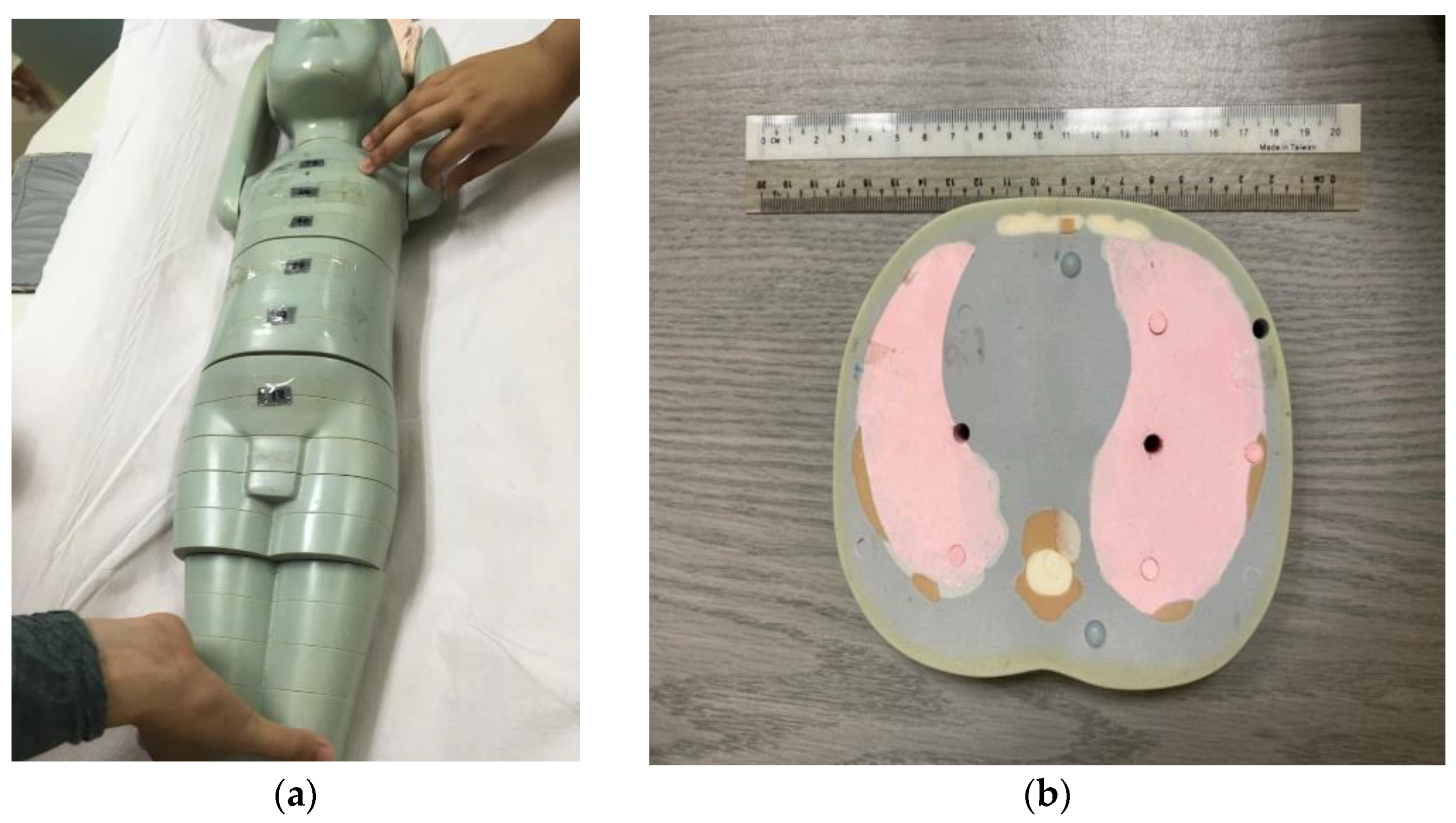
2. Materials and Methods
2.1. CT Radiation Dose
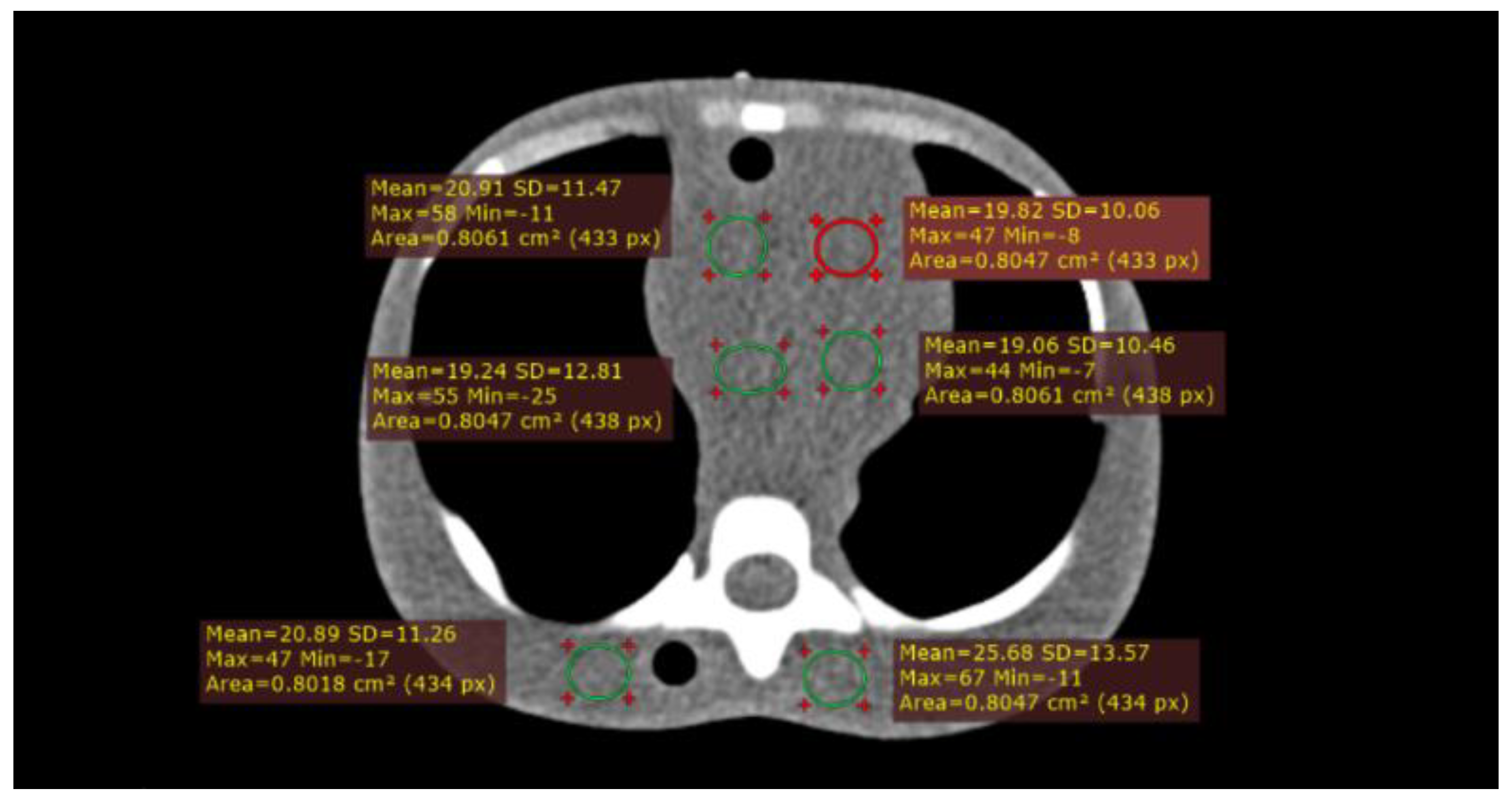
2.2. Image Quality Metrics
3. Results
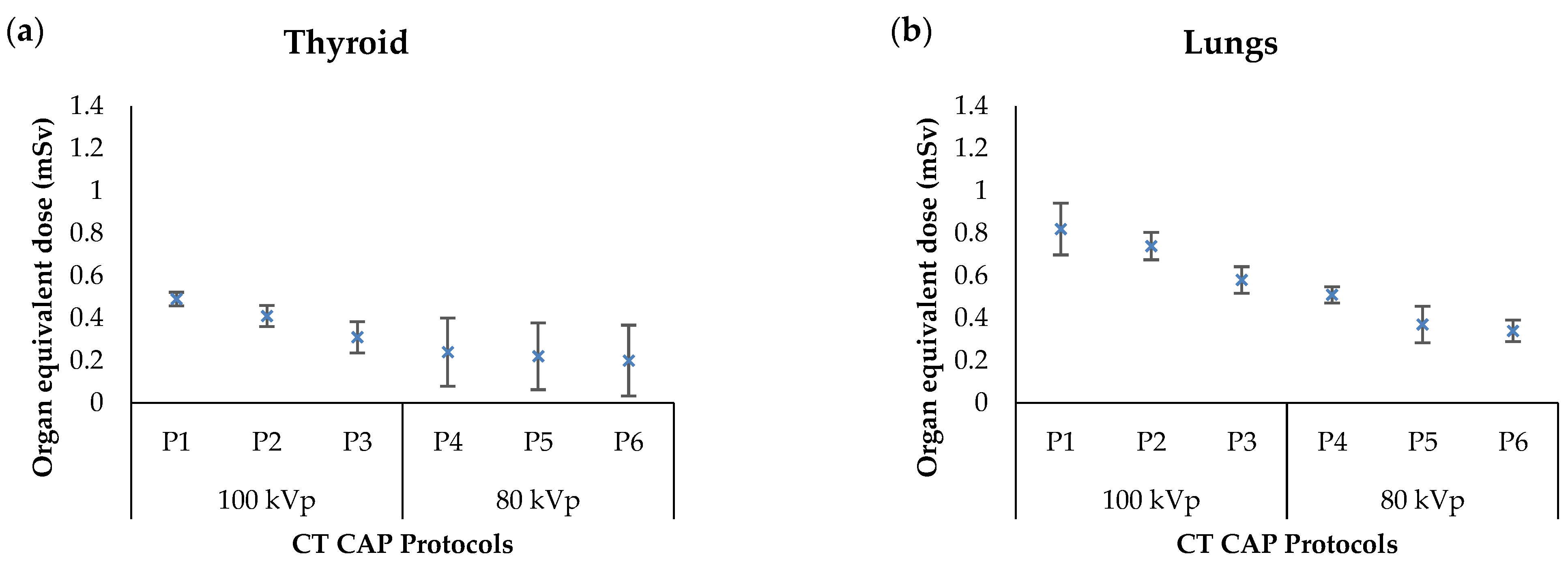
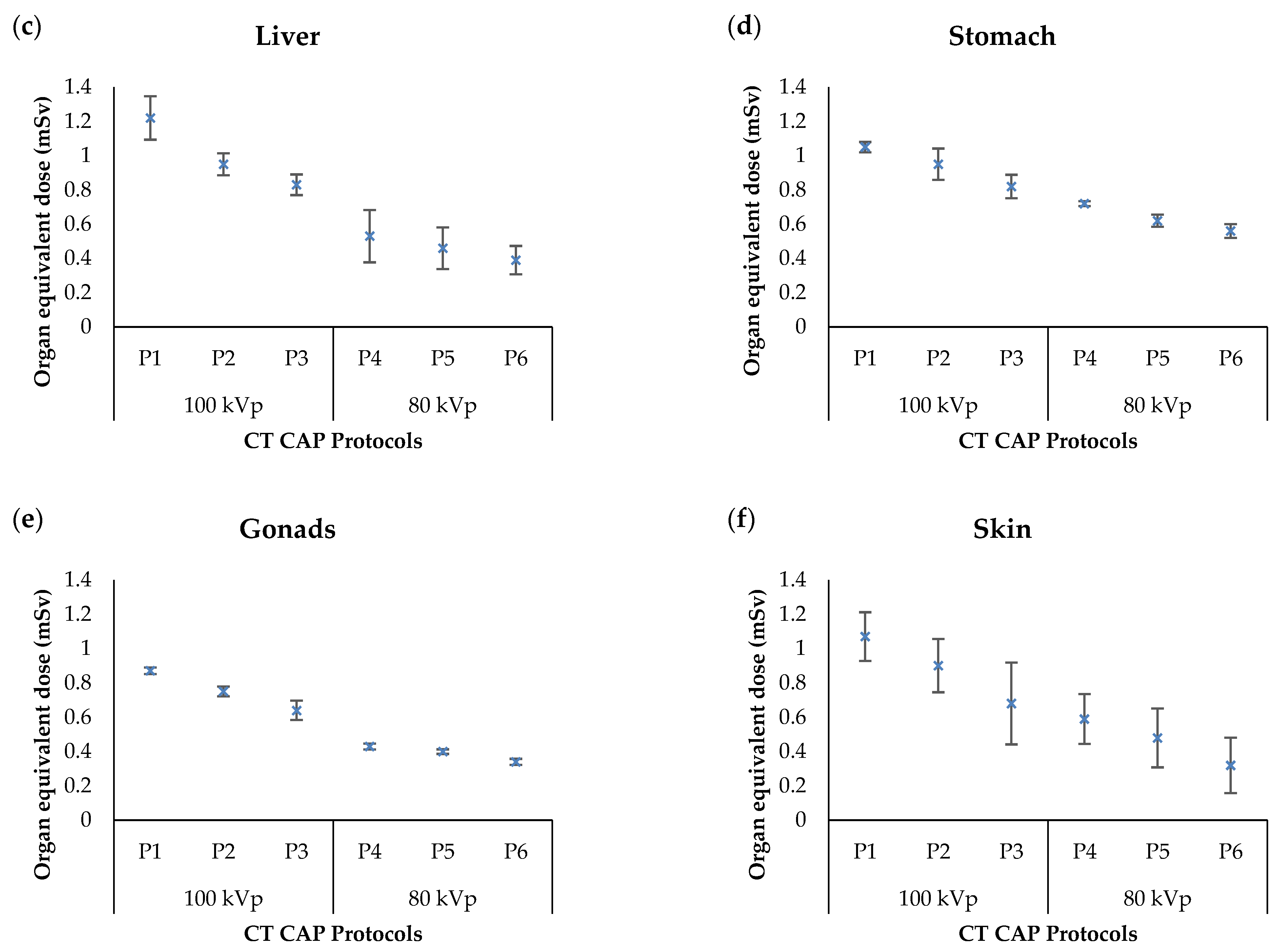
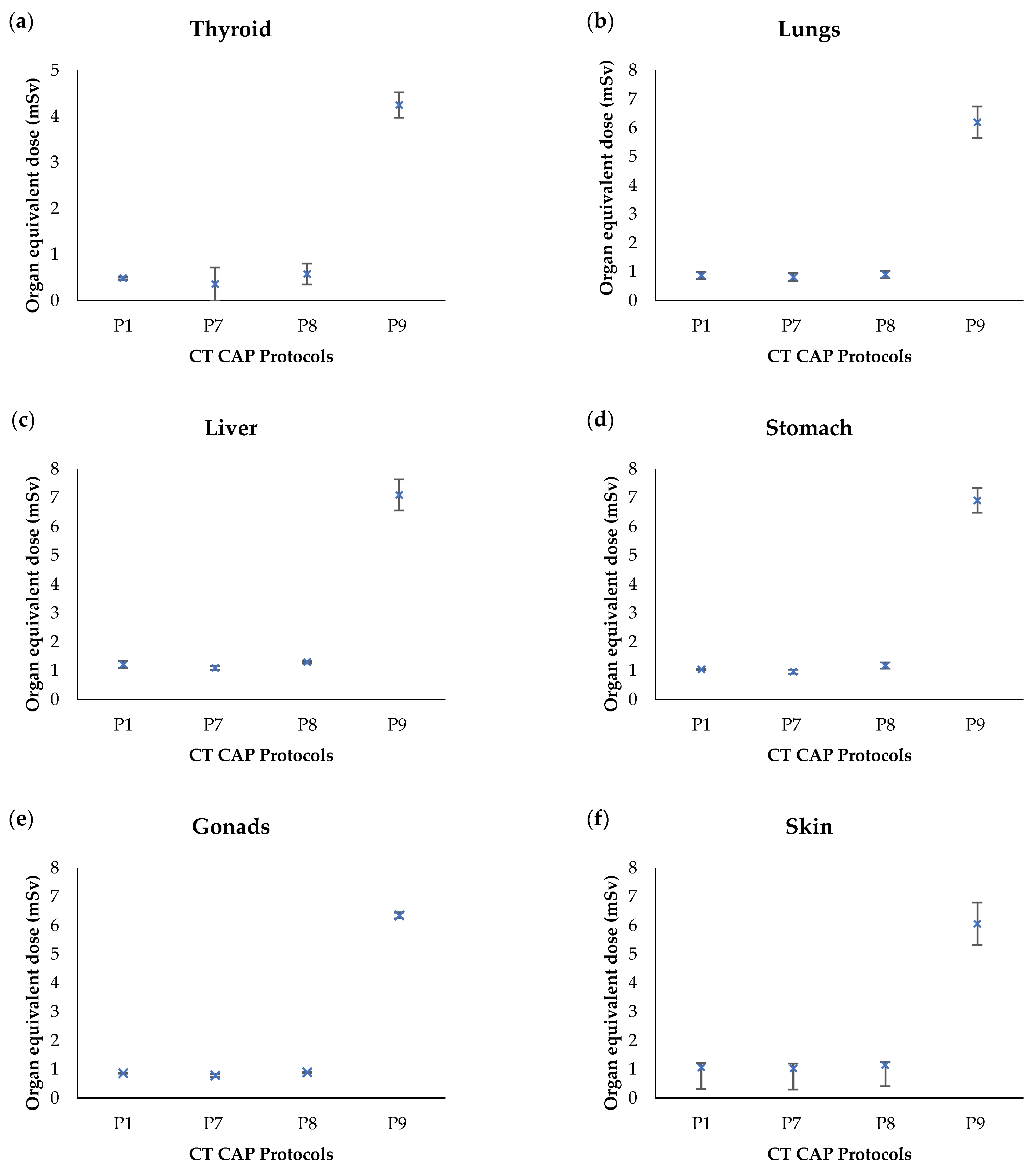
3.1. Organ Equivalent Dose
3.2. Analysis of Image Quality Metrics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Haleem, A.; Javaid, M. Role of CT and MRI in the design and development of orthopaedic model using additive manufacturing. J. Clin. Orthop. Trauma 2018, 9, 213–217. [Google Scholar] [CrossRef]
- Wang, J.; Fleischmann, D. Improving spatial resolution at CT: Development, benefits, and pitfalls. Radiology 2018, 289, 261–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubo, T. Vendor free basics of radiation dose reduction techniques for CT. Eur. J. Radiol. 2019, 110, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Laqmani, A.; Regier, M.; Veldhoen, S.; Backhaus, A.; Wassenberg, F.; Sehner, S.; Groth, M.; Nagel, H.-D.; Adam, G.; Henes, F.O. Improved image quality and low radiation dose with hybrid iterative reconstruction with 80kV CT pulmonary angiography. Eur. J. Radiol. 2014, 83, 1962–1969. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, A.E.; Damilakis, J. Automatic tube current modulation and tube voltage selection in pediatric computed tomography: A phantom study on radiation dose and image quality. Invest. Radiol. 2019, 54, 265–272. [Google Scholar] [CrossRef]
- Aw-Zoretic, J.; Seth, D.; Katzman, G.; Sammet, S. Estimation of effective dose and lifetime attributable risk from multiple head CT scans in ventriculoperitoneal shunted children. Eur. J. Radiol. 2014, 83, 1920–1924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muhammad, N.; Karim, M.; Hassan, H.; Kamarudin, M.; Wong, J.; Ibahim, M. Estimation of effective dose and organ cancer risk from paediatric computed tomography thorax-Abdomen-Pelvis examinations. Radiat. Phys. Chem. 2019, 165, 108438. [Google Scholar] [CrossRef]
- Al-Rammah, T.Y. CT radiation dose awareness among paediatricians. Ital. J. Pediatr. 2016, 42, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Krille, L.; Zeeb, H.; Jahnen, A.; Mildenberger, P.; Seidenbusch, M.; Schneider, K.; Weisser, G.; Hammer, G.; Scholz, P.; Blettner, M. Computed tomographies and cancer risk in children: A literature overview of CT practices, risk estimations and an epidemiologic cohort study proposal. Radiat. Environ. Biophys. 2012, 51, 103–111. [Google Scholar] [CrossRef]
- Perisinakis, K.; Tzedakis, A.; Pouli, S.; Spanakis, K.; Hatzidakis, A.; Damilakis, J. Comparison of patient dose from routine multi-phase and dynamic liver perfusion CT studies taking into account the effect of iodinated contrast administration. Eur. J. Radiol. 2019, 110, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Applegate, K.E.; Frush, D.P. Image gently: A Decade of international collaborations to promote appropriate imaging for children. J. Am. Coll. Radiol. 2017, 14, 956–957. [Google Scholar] [CrossRef] [Green Version]
- Parakh, A.; Kortesniemi, M.; Schindera, S.T. CT radiation dose management. Radiology 2016, 280, 663–673. [Google Scholar] [CrossRef]
- Alqahtani, S.J.M.; Welbourn, R.; Meakin, J.R.; Palfrey, R.M.; Rimes, S.J.; Thomson, K.; Knapp, K.M. Increased radiation dose and projected radiation-related lifetime cancer risk in patients with obesity due to projection radiography. J. Radiol. Prot. 2019, 39, 38–53. [Google Scholar] [CrossRef] [PubMed]
- Racine, D.; Ryckx, N.; Ba, A.; Becce, F.; Viry, A.; Verdun, F.R.; Schmidt, S. Task-based quantification of image quality using a model observer in abdominal CT: A multicentre study. Eur. Radiol. 2018, 28, 5203–5210. [Google Scholar] [CrossRef] [Green Version]
- Hashim, S.; Karim, M.K.A.; Bakar, K.; Sabarudin, A.; Chin, A.; Saripan, M.; Bradley, D. Evaluation of organ doses and specific k effective dose of 64-slice CT thorax examination using an adult anthropomorphic phantom. Radiat. Phys. Chem. 2016, 126, 14–20. [Google Scholar] [CrossRef]
- Gao, Y.; Quinn, B.; Mahmood, U.; Long, D.; Erdi, Y.; St. Germain, J.; Pandit-Taskar, N.; Xu, G.; Bolch, W.; Dauer, L. A comparison of pediatric and adult CT organ dose estimation methods. BMC Med. Imaging 2017, 17, 28. [Google Scholar] [CrossRef]
- Goodman, T.R.; Mustafa, A.; Rowe, E. Pediatric CT radiation exposure: Where we were, and where we are now. Pediatr. Radiol. 2019, 49, 469–478. [Google Scholar] [CrossRef]
- Stamm, G.; Nagel, H.D. CT-expo—A novel program for dose evaluation in CT. RöFo 2002, 174, 1570–1576. (In German) [Google Scholar]
- Hoang, J.K.; Reiman, R.E.; Nguyen, G.B.; Januzis, N.; Chin, B.B.; Lowry, C.; Yoshizumi, T.T. Lifetime attributable risk of cancer from radiation exposure during parathyroid imaging: Comparison of 4D CT and parathyroid scintigraphy. Am. J. Roentgenol. 2015, 204, W579–W585. [Google Scholar] [CrossRef] [PubMed]
- Samei, E.; Tian, X.; Segars, W.P.; Frush, D.P. Radiation risk index for pediatric CT: A patient-derived metric. Pediatr. Radiol. 2017, 47, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Gruber-Rouh, T.; Leithner, D.; Zierden, A.; Albrecht, M.H.; Wichmann, J.L.; Bodelle, B.; Elsabaie, M.; Scholtz, J.-E.; Kaup, M.; et al. Single-source chest-abdomen-pelvis cancer staging on a third generation dual-source CT system: Comparison of automated tube potential selection to second generation dual-source CT. Cancer Imaging 2016, 16, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, Y.; Quinn, B.; Pandit-Taskar, N.; Behr, G.; Mahmood, U.; Long, D.; Xu, G.; St. Germain, J.; Dauer, L. Patient-specific organ and effective dose estimates in pediatric oncology computed tomography. EJMP 2018, 45, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Abdulkadir, M.K.; Mat Rahim, N.A.Y.; Mazlan, N.S.; Daud, N.M.; Shuaib, I.L.; Osman, N.D. Dose optimisation in paediatric CT examination: Assessment on current scanning protocols associated with radiation dose. Radiat. Phys. Chem. 2020, 171, 108740. [Google Scholar] [CrossRef]
- Halid, B.; Karim, M.K.A.; Sabarudin, A.; Bakar, K.A.; Shariff, N.D. Assessment of lifetime attributable risk of stomach and colon cancer during abdominal ct examinations based on Monte Carlo simulation. In Proceedings of the 8th European Medical and Biological Engineering Conference; Springer International Publishing: New York, NY, USA, 2017; pp. 455–459. [Google Scholar]
- Seeram, E.; Davidson, R.; Bushong, S.; Swan, H. Optimizing the exposure indicator as a dose management strategy in computed radiography. Radiol. Technol. 2016, 87, 380–391. [Google Scholar]
- Tonkopi, E.; Duffy, S.; Abdolell, M.; Manos, D. Diagnostic reference levels and monitoring practice can help reduce patient dose from ct examinations. Am. J. Roentgenol. 2017, 208, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- Karim, M.K.A.; Hashim, S.; Bradley, D.A.; Bahruddin, N.A.; Ang, W.C.; Salehhon, N. Assessment of knowledge and awareness among radiology personnel regarding current computed tomography technology and radiation dose. J. Phys. Conf. Ser. 2016, 694, 012031. [Google Scholar] [CrossRef]
- Isa, I.; Rahmat, S.; Dom, S.; Kayun, Z.; Karim, M. The effects of mis-centering on radiation dose during CT head examination: A phantom study. J. X-ray Sci. Technol. 2019, 27, 631–639. [Google Scholar] [CrossRef]
- Shaffiq Said Rahmat, S.M.; Abdul Karim, M.K.; Che Isa, I.N.; Abd Rahman, M.A.; Noor, N.M.; Hoong, N.K. Effect of miscentering and low-dose protocols on contrast resolution in computed tomography head examination. Comput. Biol. Med. 2020, 123, 103840. [Google Scholar] [CrossRef]
- Harun, H.; Karim, M.; Abbas, Z.; Sabarudin, A.; Muniandy, S.; Razak, H.; Ng, K. The influence of iterative reconstruction level on image quality and radiation dose in CT pulmonary angiography examinations. Radiat. Phys. Chem. 2021, 178, 108989. [Google Scholar] [CrossRef]
- Harun, H.H.; Karim, M.K.A.; Abbas, Z.; Rahman, M.A.A.; Sabarudin, A.; Ng, K.H. Association of radiation doses and cancer risks from ct pulmonary angiography examinations in relation to body diameter. Diagnostics 2020, 10, 681. [Google Scholar] [CrossRef] [PubMed]
- McCollough, C.; Leng, S. Use of artificial intelligence in computed tomography dose optimisation. Ann. ICRP 2020, 49, 113–125. [Google Scholar] [CrossRef]
- Barrera, C.A.; Otero, H.J.; White, A.M.; Saul, D.; Biko, D.M. Image quality and radiation dose of ECG-triggered High-Pitch Dual-Source cardiac computed tomography angiography in children for the evaluation of central vascular stents. Int. J. Cardiovasc. Imaging 2019, 35, 367–374. [Google Scholar] [CrossRef]
- Cardenas, C.E.; McCarroll, R.E.; Court, L.E.; Elgohari, B.A.; Elhalawani, H.; Fuller, C.D.; Kamal, M.J.; Meheissen, M.A.M.; Mohamed, A.S.R.; Rao, A.; et al. Deep learning algorithm for auto-delineation of high-risk oropharyngeal clinical target volumes with built-in dice similarity coefficient parameter optimization function. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 468–478. [Google Scholar] [CrossRef]
- Gomez-Cardona, D.; Hayes, J.W.; Zhang, R.; Li, K.; Cruz-Bastida, J.P.; Chen, G.-H. Low-dose cone-beam CT via raw counts domain low-signal correction schemes: Performance assessment and task-based parameter optimization (Part II. Task-based parameter optimization). Med. Phys. 2018, 45, 1957–1969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berlin, S.C.; Weinert, D.M.; Vasavada, P.S.; Martinez-Rios, C.; Parikh, R.A.; Wien, M.A.; Jordan, D.W.; Novak, R.D. Successful dose reduction using reduced tube voltage with hybrid iterative reconstruction in pediatric abdominal CT. Am. J. Roentgenol. 2015, 205, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Nagayama, Y.; Oda, S.; Nakaura, T.; Tsuji, A.; Urata, J.; Furusawa, M.; Utsunomiya, D.; Funama, Y.; Kidoh, M.; Yamashita, Y. Radiation dose reduction at pediatric CT: Use of low tube voltage and iterative reconstruction. Radiographics 2018, 38, 1421–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambert, J.W.; Phelps, A.S.; Courtier, J.L.; Gould, R.G.; MacKenzie, J.D. Image quality and dose optimisation for infant CT using a paediatric phantom. Eur. Radiol. 2015, 26, 1387–1395. [Google Scholar] [CrossRef]
- Trattner, S.; Chelliah, A.; Prinsen, P.; Ruzal-Shapiro, C.B.; Xu, Y.; Jambawalikar, S.; Amurao, M.; Einstein, A.J. Estimating effective dose of radiation from pediatric cardiac CT angiography using a 64-MDCT scanner: New conversion factors relating dose-length product to effective dose. Am. J. Roentgenol. 2017, 208, 585–594. [Google Scholar] [CrossRef]
- Gariani, J.; Martin, S.P.; Botsikas, D.; Becker, C.D.; Montet, X. Evaluating the effect of increased pitch, iterative reconstruction and dual source CT on dose reduction and image quality. Br. J. Radiol. 2018, 91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booij, R.; Dijkshoorn, M.L.; Van Straten, M. Efficacy of a dynamic collimator for overranging dose reduction in a second- and third-generation dual source CT scanner. Eur. Radiol. 2017, 27, 3618–3624. [Google Scholar] [CrossRef] [Green Version]
- Messerli, M.; Dewes, P.; Scholtz, J.-E.; Arendt, C.; Wildermuth, S.; Vogl, T.J.; Bauer, R.W. Evaluation of an adaptive detector collimation for prospectively ECG-triggered coronary CT angiography with third-generation dual-source CT. Eur. Radiol. 2018, 28, 2143–2150. [Google Scholar] [CrossRef] [PubMed]
- Urikura, A.; Hara, T.; Yoshida, T.; Nishimaru, E.; Hoshino, T.; Nakaya, Y.; Endo, M. Overranging and overbeaming measurement in area detector computed tomography: A method for simultaneous measurement in volume helical acquisition. J. Appl. Clin. Med. Phys. 2019, 20, 160–165. [Google Scholar] [CrossRef]
- Flohr, T. CT Systems. Curr. Radiol. Rep. 2013, 1, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Chang, K.-P.; Hsu, T.-K.; Lin, W.-T.; Hsu, W.-L. Optimization of dose and image quality in adult and pediatric computed tomography scans. Radiat. Phys. Chem. 2017, 140, 260–265. [Google Scholar] [CrossRef]
- Harun, H.H.; Karim, M.K.A.; Muhammad, N.A.; Razak, H.R.A.; Sabarudin, A.; Muniandy, S.C. Effect of iterative reconstruction algorithm associated with low contrast detectability performance from CT pulmonary angiography examinations. J. Phys. Conf. Ser. 2020, 012029. [Google Scholar] [CrossRef]
- Meineke, A.; Rubbert, C.; Sawicki, L.M.; Thomas, C.; Klosterkemper, Y.; Appel, E.; Caspers, J.; Bethge, O.T.; Kröpil, P.; Antoch, G.; et al. Potential of a machine-learning model for dose optimization in CT quality assurance. Eur. Radiol. 2019, 29, 3705–3713. [Google Scholar] [CrossRef] [PubMed]
- Roshani, M.; Phan, G.; Faraj, R.H.; Phan, N.-H.; Roshani, G.H.; Nazemi, B.; Corniani, E.; Nazemi, E. Proposing a gamma radiation based intelligent system for simultaneous analyzing and detecting type and amount of petroleum by-products. Nucl. Eng. Technol. 2020. [Google Scholar] [CrossRef]
- Roshani, M.; Phan, G.; Roshani, G.H.; Hanus, R.; Nazemi, B.; Corniani, E.; Nazemi, E. Combination of X-ray tube and GMDH neural network as a nondestructive and potential technique for measuring characteristics of gas-oil–water three phase flows. Measurement 2021, 168, 108427. [Google Scholar] [CrossRef]
- Alla Takam, C.; Samba, O.; Tchagna Kouanou, A.; Tchiotsop, D. Spark architecture for deep learning-based dose optimization in medical imaging. Inform. Med. Unlocked. 2020, 19, 100335. [Google Scholar] [CrossRef]
- Singh, R.; Wu, W.; Wang, G.; Kalra, M.K. Artificial intelligence in image reconstruction: The change is here. Phys. Med. 2020, 79, 113–125. [Google Scholar] [CrossRef]
- Verdun, F.R.; Racine, R.D.; Ott, J.G.; Tapiovaara, T.M.; Toroi, P.; Bochud, F.O.; Veldkamp, W.J.H.; Schegerer, A.A.; Bouwman, R.W.; Giron, I.H.; et al. Image quality in CT: From physical measurements to model observers. Phys. Med. 2015, 31, 823–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Protocols | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| P1 | P2 | P3 | P4 | P5 | P6 | P7 | P8 | P9 | |
| Slice thickness recon (mm) | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Tube potential (kVp) | 100 | 100 | 100 | 80 | 80 | 80 | 100 | 100 | 100 |
| Effective tube current (mAs) | 27 | 23 | 19 | 33 | 31 | 26 | 27 | 26 | - |
| Ref. mAs | 210 | 180 | 150 | 210 | 180 | 150 | 210 | 210 | 210 |
| Number of detector | 64 | 64 | 64 | 64 | 64 | 64 | 32 | 64 | 64 |
| Slice collimation (mm) | 0.6 | 0.6 | 0.6 | 0.6 | 0.6 | 0.6 | 1.2 | 0.6 | 0.6 |
| Pitch | 1.4 | 1.4 | 1.4 | 1.4 | 1.4 | 1.4 | 1.4 | 1.2 | 1.4 |
| Dose Modulation | On | On | On | On | On | On | On | On | Off |
| Table Feed | 53.8 | 53.8 | 53.8 | 53.8 | 53.8 | 53.8 | 53.8 | 56.0 | 53.8 |
| Exposure time (s) | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
| Kernel filtration | B30f | B30f | B30f | B30f | B30f | B30f | B30f | B30f | B30f |
| CTDIvol (mGy) | 1.8 | 1.5 | 1.3 | 1.0 | 0.9 | 0.8 | 1.7 | 1.7 | 6.9 |
| DLP (mGy.cm) | 58 | 48 | 42 | 32 | 29 | 26 | 54 | 54 | 221 |
| E (DLP x k factor) | 1.6 | 1.3 | 1.2 | 0.9 | 0.8 | 0.7 | 1.5 | 1.5 | 6.2 |
| Selected Organ | Organ Equivalent Dose (mSv) | |||||
|---|---|---|---|---|---|---|
| 100 kVp | 80 kVp | |||||
| P1 (Ref. mAs 210) | P2 (Ref. mAs 180) | P3 (Ref. mAs 150) | P4 (Ref. mAs 210) | P5 (Ref. mAs 180) | P6 (Ref. mAs 150) | |
| Thyroid | 0.49 ± 0.03 | 0.41 ± 0.05 | 0.31 ± 0.07 | 0.24 ± 0.16 | 0.22 ±0.16 | 0.20 ± 0.17 |
| Lungs | 0.88 ± 0.12 | 0.74 ± 0.06 | 0.58 ± 0.06 | 0.51 ± 0.04 | 0.37 ±0.09 | 0.35 ± 0.05 |
| Liver | 1.22 ± 0.13 | 0.95 ± 0.06 | 0.83 ± 0.06 | 0.53 ± 0.15 | 0.46 ± 0.12 | 0.39 ± 0.08 |
| Stomach | 1.05 ± 0.03 | 0.95 ± 0.09 | 0.82 ± 0.07 | 0.72 ± 0.01 | 0.62 ± 0.04 | 0.56 ± 0.04 |
| Gonads | 0.87 ± 0.02 | 0.75 ± 0.03 | 0.64 ± 0.06 | 0.43 ± 0.02 | 0.40 ± 0.01 | 0.34 ± 0.02 |
| Skin | 1.07 ± 0.14 | 0.90 ± 0.16 | 0.68 ± 0.24 | 0.59 ± 0.14 | 0.48 ± 0.17 | 0.32 ± 0.16 |
| Selected Organs | Organ Equivalent Dose (mSv) | |||
|---|---|---|---|---|
| P1(R) | P7 (S.C = 1.2) | P8 (P = 1.2) | P9 (Off TCM) | |
| Thyroid | 0.49 ± 0.03 | 0.36 ± 0.36 | 0.58 ± 0.23 | 4.25 ± 0.27 |
| Lungs | 0.88 ± 0.12 | 0.82 ± 0.14 | 0.91 ± 0.13 | 6.2 ± 0.55 |
| Liver | 1.22 ± 0.13 | 1.10 ± 0.07 | 1.30 ± 0.04 | 7.10 ± 0.54 |
| Stomach | 1.05 ± 0.03 | 0.97 ± 0.07 | 1.18 ± 0.11 | 6.91 ± 0.42 |
| Gonads | 0.87 ± 0.02 | 0.79 ± 0.04 | 0.90 ± 0.02 | 6.35 ± 0.10 |
| Skin | 1.07 ± 0.14 | 1.04 ± 0.17 | 1.15 ± 0.11 | 6.06 ± 0.74 |
| Image Quality | CT CAP Protocol | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| P1 | P2 | P3 | P4 | P5 | P6 | P7 | P8 | P9 | |
| CT Number (Mean) | 22.5 ± 0.9 | 22.3 ± 0.9 | 19.9 ± 1.9 | 19.5 ± 0.8 | 20.3 ± 1.9 | 10.1 ± 1.3 | 22.6 ± 0.5 | 22.0 ± 0.9 | 21.4 ± 0.9 |
| Noise (SD) | 8.9 ± 1.1 | 9.3 ± 0.9 | 10.5 ± 1.6 | 10.8 ± 2.3 | 11.5 ± 0.6 | 13.1 ± 0.6 | 7.4 ± 1.0 | 8.8 ± 0.7 | 3.2 ± 0.2 |
| SNR | 2.54 ± 0.4 | 2.41 ± 0.2 | 1.93 ± 0.4 | 1.87±0.4 * | 1.77 ± 0.1 * | 0.77 ±0.1 * | 3.10 ± 0.4 | 2.51 ± 0.2 | 6.66 ± 0.5 * |
| CNR | 0.71 ± 0.1 | 0.69 ± 0.1 | 0.47 ± 0.1 | 0.59 ± 0.1 | 0.45 ± 0.1 * | 0.61 ± 0.1 | 0.54 ± 0.1 | 0.23 ± 0.1 * | 1.34 ± 0.2 * |
| FOM | 3.65 | 3.90 | 2.97 | 3.59 | 3.54 | 0.75 | 5.73 | 3.73 | 6.47 |
| Dunnett t-tests(p value) | Control | 1.000 | 0.058 | 0.611 | 0.028 | 0.779 | 0.255 | 0.000 | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muhammad, N.A.; Kayun, Z.; Abu Hassan, H.; Wong, J.H.D.; Ng, K.H.; Karim, M.K.A. Evaluation of Organ Dose and Image Quality Metrics of Pediatric CT Chest-Abdomen-Pelvis (CAP) Examination: An Anthropomorphic Phantom Study. Appl. Sci. 2021, 11, 2047. https://doi.org/10.3390/app11052047
Muhammad NA, Kayun Z, Abu Hassan H, Wong JHD, Ng KH, Karim MKA. Evaluation of Organ Dose and Image Quality Metrics of Pediatric CT Chest-Abdomen-Pelvis (CAP) Examination: An Anthropomorphic Phantom Study. Applied Sciences. 2021; 11(5):2047. https://doi.org/10.3390/app11052047
Chicago/Turabian StyleMuhammad, Nor Azura, Zunaide Kayun, Hasyma Abu Hassan, Jeannie Hsiu Ding Wong, Kwan Hoong Ng, and Muhammad Khalis Abdul Karim. 2021. "Evaluation of Organ Dose and Image Quality Metrics of Pediatric CT Chest-Abdomen-Pelvis (CAP) Examination: An Anthropomorphic Phantom Study" Applied Sciences 11, no. 5: 2047. https://doi.org/10.3390/app11052047