1. Introduction
Epiretinal membrane (ERM) is a common retinal disease with a prevalence ranging from 2.2% to 28.9% [
1,
2,
3]. Fibrocellular proliferation at the vitreoretinal interface, above the internal limiting membrane (ILM), seems to be a key mechanism [
4]. ERMs are mainly idiopathic, and are less commonly secondary due to trauma, inflammatory disease, intraocular surgery or retinal detachment [
5]. Reduced visual acuity and metamorphopsia are the most frequent symptoms [
6]. Tractional stress caused by the ERMs may induce changes, such as increased retinal thickness; the formation of lamellar and full-thickness macular defects; and alterations of the outer foveal region [
4,
7]. Additionally, other cellular and vascular changes, such as hemodynamic changes in choroidal flow, leakage and disruption from the retinal capillary system, reduced uveal-scleral outflow and breakdown of the retinal pigment epithelium have been reported [
8,
9,
10].
In the last decade, high-resolution spectral-domain coherence tomography (SD-OCT) has emerged as a new non-invasive and reproducible technique for the diagnosis and follow-up treatment of different ocular diseases [
11,
12,
13,
14,
15,
16]. To date, this diagnostic tool is considered an essential component of the pre-operative assessment and allows for quantification of structural changes to the macula and specific retinal layers. Additionally, the possibility to investigate such changes and defining new descriptive terms have improved our pathophysiological understanding significantly, identifying possible prognostic factors, able to predict the functional outcomes in macular diseases [
1,
17,
18,
19,
20].
The central bouquet (CB) is a small circular island, less than 100 µm in diameter and located centrally at the fovea, detectable by OCT [
7,
21]. Govetto at al. classified tractional abnormalities of the CB and reported a correlation between morphologic progression and the corresponding best corrected visual acuity (BCVA) [
7]. Accordingly, they also developed a staging system for describing ERMs and observed that more severe stages of ERMs correlate with higher reduction of visual acuity [
4].
Pars plana vitrectomy (PPV) with ERM and ILM peeling is the gold standard to release tension and restore the normal structure of the retina [
22,
23,
24]. However, despite the progress towards a minimally invasive vitreoretinal surgery and high anatomical success rates, the postoperative visual outcomes are variable [
25,
26].
To our knowledge, previous studies have already described irregularities of the outer retinal anatomy in the context ERMs [
27,
28]. However, the influences of their surgical removal on specific changes in the CB morphology and correlations with functional outcome have only been investigated in the short-term [
29].
The aim of this study was to evaluate the impacts of different stages of ERM and CB abnormalities on the functional and anatomic outcomes following PPV with ERM and ILM peeling.
2. Materials and Methods
This is a retrospective study including all consecutive patients suffering from idiopathic ERM that underwent PPV with 23 or 27 g and ERM ± ILM peeling at the Triemli City Hospital Zurich between 2014 and 2018 with a minimum follow-up of 3 months. The study was approved by the local Ethics Committee (BASEC ID 2017-02306) and adhered to the tenets of the Declaration of Helsinki. All subjects signed an informed consent statement.
Patients were excluded if they had previous a PPV, a retinal photocoagulation procedure, history of ocular trauma, secondary ERM, myopia with an axial length >26 mm, amblyopia, diabetic retinopathy, retinal vascular occlusion or macular disorders potentially affecting surgical outcomes or a follow-up of less than 3 months. Patients with corneal disorders or other ocular pathologic features that could have interfered with the quality of SD-OCT images were also excluded.
All patients received a complete ophthalmologic assessment, including best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, intraocular pressure, dilated fundus examination and SD-OCT at baseline and at each visit during follow-up.
BCVA was measured through Snellen charts by a single, well-trained experienced ophthalmologist (M.B.), and converted into the logarithm of the minimum angle of resolution (LogMAR).
2.1. Image Acquisition
All eyes were evaluated by Heidelberg Spectralis Spectral Domain OCT System (SD-OCT) version 5.1.3.0 (Heidelberg Engineering, Heidelberg, Germany) with Heidelberg Eye Explorer version 1.6.2.0 (Heidelberg Engineering).
Cubic, 20° × 15° 37-line scans with a 120 µm spacing centered on the fovea were obtained for each eye. More than 20 scans were averaged for each measurement. A certified operator (M.P.B.) carried out all OCT examinations. Two masked expert investigators (M.P.B., F.R.) interpreted the SD-OCT images. A third (M.R.) investigator was consulted for the final decision in cases of disagreement.
ERM was defined as a thin highly reflective band either anterior to the neurosensory retina with focal areas of macular attachments or globally adherent to the retinal surface in SD-OCT B-scans [
24]. Furthermore, morphological appearance of the retina was evaluated in terms of the stage of ERM and the configuration of the outer retinal layers in the area of the CB.
2.2. Grading of ERM and CB Alterations
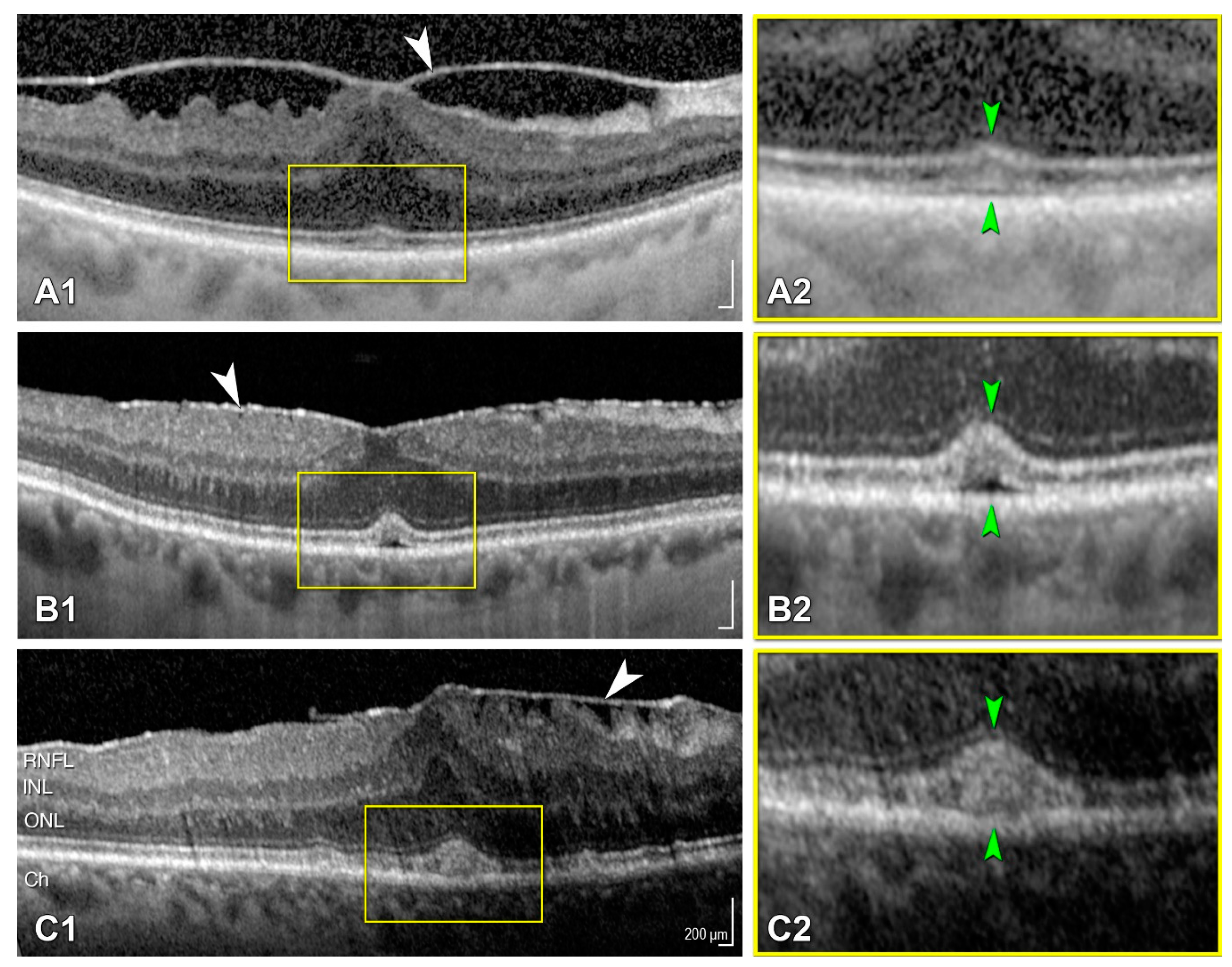
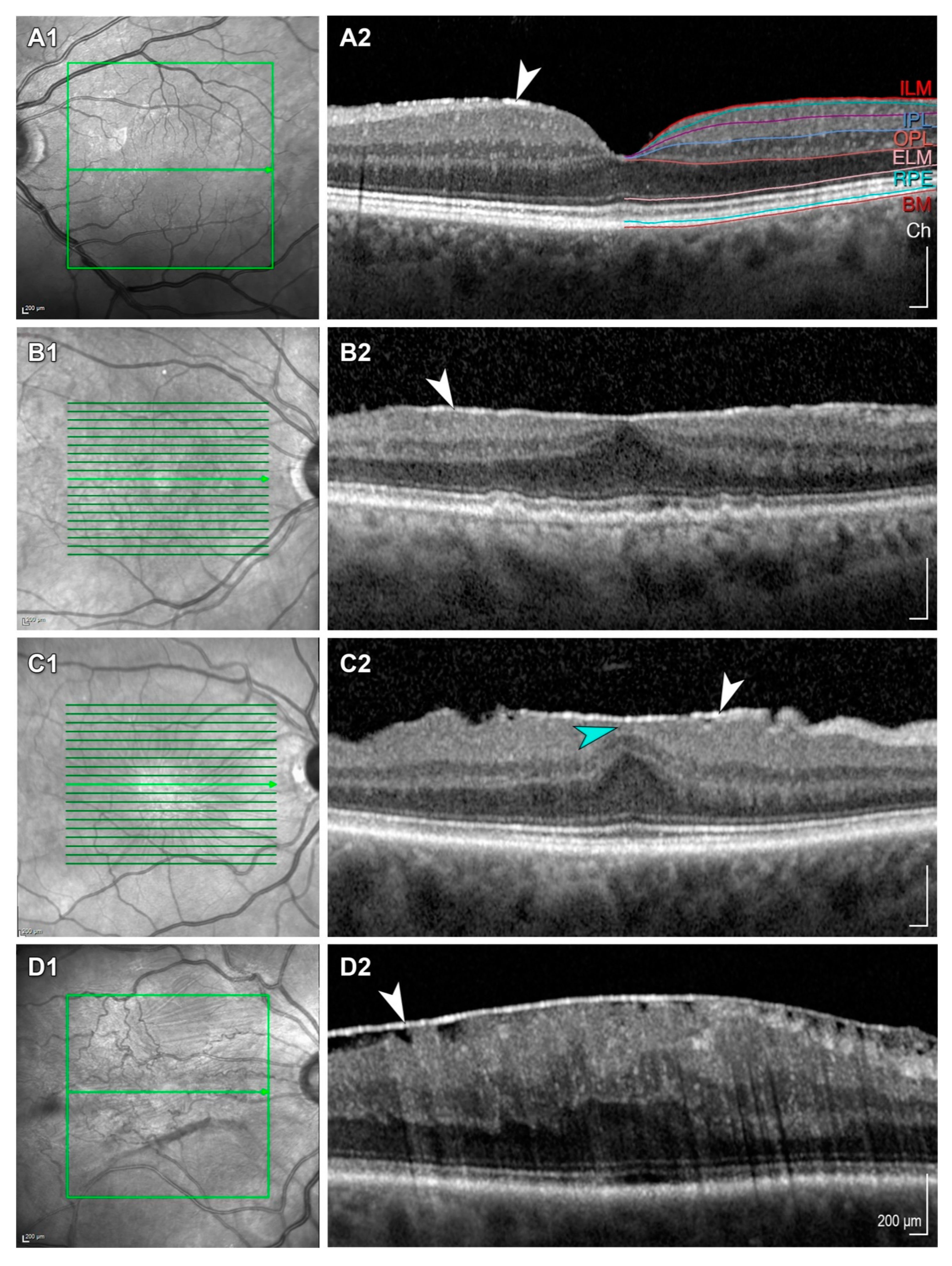
We used the classification systems of Govetto et al. for describing CB alterations and ERM (
Figure 1 and
Figure 2).
CB alterations were graded by severity from stage 1 to stage 3. A small, fuzzy hyperreflective area (cotton ball sign) between the interdigitation zone (IZ) and the ellipsoid zone (EZ) was classified as stage 1. At stage 2 a central hyporeflective pocket of subretinal fluid under the IZ was observed. Stage 3 depicts a larger collection of hyperreflective material somewhere between the retinal pigment epithelium and the EZ (
Figure 1).
ERM qualified as stage 1; only mild morphological changes were seen. Foveal depression had to be preserved, and all retinal layers had to be identifiable. At stage 2, a more progressive retinal distortion with loss of the foveal depression was present. In stage 3, ERM was continuous with ectopic inner foveal layers (EIFL) anomalously crossing the central foveal area along with loss of the foveal depression. Finally, in stage 4 significant retinal thickening and remarkable anatomic disruption of the macula was shown (
Figure 2).
2.3. Surgical Technique
All patients underwent a three-port PPV with ERM peeling by two vitreoretinal surgeons (S.M. and M.B.), combined with standard phacoemulsification in cases of phakic eyes. In all cases, 23 or 27-gauge instruments and the EVA system (D.O.R.C., The Netherlands) with a cut rate of up to 8000 cuts per minute and up to 650 mmHg of vacuum were used. The Resight viewing system (Zeiss, Germany) was utilized for non-contact visualization of the fundus during vitrectomy and peeling.
After placement of three microcannulas at the pars plana and connection of the infusion line, a core vitrectomy was performed. Triamcinolone was used to check for the presence of a complete posterior vitreous detachment (PVD). If not present, the PVD was induced with the cutter near the optic disc. A peripheral vitrectomy was then performed, followed by search for peripheral breaks by scleral indentation. Cryopexy or endolaser were applied as needed. The ERM was stained with Membrane Blue Dual (D.O.R.C., The Netherlands) and peeled with an end-gripping 27-gauge forceps. The ILM was then equally stained and peeled. After aspiration of any free-floating membrane pieces, the surgeon would either instill an air bubble into the eye or leave it filled with balanced saline solution. The microcannulas were removed and the sclerotomies sutured with Polysorb (Medtronic, USA) as needed. Topical antibiotics and steroids were prescribed for 1 month postoperatively.
2.4. Statistical Analysis
The data were analyzed using IBM SPSS (version 24.0, Chicago, IL, USA). Snellen BCVA was converted to logarithm of the minimum angle of resolution (LogMAR). A paired samples test (T-test) was performed to compare means of BCVA, CB and ERM grading before and after surgery. ANOVA analysis was used to evaluate influences of different CB and ERM stages on BCVA difference (BCVA before surgery—BCVA after surgery). A multiple linear regression was calculated to predict BCVA improvement at final follow-up based on BCVA before surgery, and ERM and CB alteration stages at baseline. A p value of <0.05 was considered statistically significant.
3. Results
For this study 151 patient records were reviewed. According to inclusion and exclusion criteria, 84 patients were excluded. Therefore, 67 subjects were considered in the statistical analysis. The cohort consisted of 23 (34%) females and 44 (66%) males. The mean age was 67 (61–87) years. The mean follow-up time was 20 months (3–70). Most surgeries were performed without phacoemulsification and implantation of a posterior chamber intraocular lens (n = 45; 67%). Prior to surgery, all patients presented with ERM (
Figure 2). The stages of ERM were homogenously distributed. At baseline, most patients did not show alterations of the CB (n = 45; 66%). CB alterations were detected in 22 eyes (34%) prior to surgery, with stage 1 alterations being the most common (
Table 1,
Figure 1).
Mean BCVA before was 0.42 (±0.26) LogMAR before surgery and 0.20 (±0.22) LogMAR after surgery (
p < 0.001). A mean improvement of 0.22 LogMAR units was reached, indicating a significant mean gain in vision of almost 2.5 lines (
Table 2).
The mean CB stage at baseline was 0.55 (±0.93) and improved to 0.27 (±0.59) following surgery (p = 0.002). Of all the patients with foveal changes at baseline (n = 22, 34%), a significant amount (n = 15, 68%) had lower grading of CB alteration after the surgery than before (p = 0.002). Only three (4.5%) eyes showed any increase in CB alteration stage. For the five eyes (7.5%) showing the most severe form of CB abnormality (Stage 3), four eyes (80%) showed improvements in their respective stages and one stayed the same. Most eyes with stage 1 originally showed no signs of CB alteration after surgery was performed (n = 6, 50%).
All eyes showed an improvement in ERM grading, with 98.5% reaching stage 0 (n = 66 vs. n = 67; p < 0.001). Remaining ERM fragments were detected in the OCT follow-up exam after surgery in only one patient. In this case, the ERM stage improved from stage 4 to stage 1 after surgery. At baseline, the mean ERM stage was 2.45 (±1.12), and it improved to 0.01 (±0.12) after surgery (p < 0.001).
No significant difference in BCVA changes was observed when comparing surgeries including cataract removal to those without (−0.16 vs. −0.25 LogMAR,
p = 0.196). No significant difference in BCVA improvement following surgery was found amongst different stages of ERM (
p = 0.528) and CB alterations (
p = 0.841) at baseline (
Table 3).
Neither ERM stage (p = 0.06) nor CB stage (p = 0.939) at baseline were statistically significant predictors of vision improvement following surgery.
A multiple linear regression was calculated to predict BCVA improvement at final follow-up based on BCVA before surgery, and ERM and CB alteration stages at baseline. A significant regression equation was found (F(3, 63) = 16.126, p < 0.000) with an R2 of 0.434.
Participant’s predicted BCVA improvement was equal to −0.051 to 0.652 (BCVA at baseline), 0.042 (ERM stage at baseline) or 0.002 (CB grade at baseline), where BCVA is measured in LogMAR. BCVA at baseline was a significant predictor of BCVA improvement after surgery, whereas ERM and CB stages at baseline were not.
4. Discussion
The aim of this study was to evaluate the long-term functional and anatomical outcomes after PPV with ERM and ILM peeling in patients with alterations of the CB. A significant overall mean gain in BCVA of 2.5 lines (0.22 LogMAR units) was achieved, and ERM was completely removed in the central macular region in 98.5% of eyes. After a mean follow-up of 20 months, the mean CB stage improved significantly (p = 0.002) from 0.55 to 0.27 and the mean ERM stage was reduced significantly from 2.45 to 0.01.
Confirming the results of our short-term follow-up study [
29], the preoperative stage of ERM did not have a statistically significant impact on the mean BCVA change following surgery (
p = 0.528). Looking at the presented long-term results, CB stage at baseline did not prove to be a significant predictor of BCVA change after surgery (
p = 0.939). This is contrary to the findings of our earlier results, where we found that the presence of alterations of the CB appeared to be an indicator for poorer functional outcomes in short-term follow-up [
29]. According to the results of the present study, the observed short-term effect of CB alterations on BCVA diminishes in the long-term.
Furthermore, BCVA at baseline was a significant predictor of BCVA improvement after surgery (p < 0.001). As expected, patients with higher BCVA at baseline reached better BCVA results in the long-term follow-up. Confirming the results of the short-term follow-up, when comparing the procedures that included cataract removal to those without, no significant difference could be observed in the in the visual and morphological outcome (p = 0.196).
Other studies have already described modifications of the outer retinal morphology [
27,
28]. Additionally, these changes were categorized into progressive stages beginning with the cotton ball sign, followed by foveolar detachment and resulting in an acquired vitelliform lesion as the final stage [
7]. While a progression in the stage of CB alteration has already been linked to a decrease in BCVA [
7], the influences of surgical removal of ERM on specific changes in the CB and the associated functional outcome have, to our knowledge, only been evaluated for short-term follow-up [
29]. Comparing the composition of our cohort to that of Govetto et al., CB alterations were more frequent (34% vs. 22%); however, the distribution of the different stages of CB alterations was comparable to their group (stage 1: 55% vs. 62.1%; stage 2: 23% vs. 17.2%; and stage 3: 23% vs. 20.7%).
In the present study, we did not detect a significant correlation between BCVA and the stage of ERM at baseline. This is contrary to the findings of other groups, which reported that higher ERM stages at baseline correlated with lower BCVA at baseline and after surgery respectively [
4,
30,
31].
As expected, most of the ERMs could be removed completely in the central foveal region (98.5%,
p < 0.001), leading to a significant gain in vision of almost 2.5 lines (
p < 0.001). These findings are coherent with those of other groups which have evaluated the influence of ERM removal on visual acuity outcome [
25,
26]. Kim et al. and Dawson et al. similarly described improvements in BCVA of more than two lines in 77% and 70% of their patients respectively [
29,
30].
Examination of the anatomical changes showed that 68% of the patients with changes of CB had lower grading of their CB alteration after the surgery (
p = 0.002), which is identical to the short-term results [
29].
Another important point that has not yet been discussed much regards the impacts of vessel and perfusion alterations caused by the ERM. The tangential and anteroposterior forces of the ERM typically lead to a thickening of the macular with displacement of the retinal vessels, leading to a decreased size of the foveal avascular zone (FAZ) and a reduced parafoveal vessel density (VD) [
31,
32]. However, vessel analyses of retinal substructures especially are quite different among studies, probably due to the error-prone retinal layer segmentation in ERM patients [
33]. After ERM-ILM peeling, the parafoveal VD seems to increase, whereas the foveal density decreases due to reorganization and enlargement of the FAZ [
17,
34]. However, in both cited studies the postoperative increase of VD did not correlate with BCVA improvement. In a recent study of our own group, we found a significant increase of choriocapillaris perfusion and a decrease in Sattler’s layer perfusion 3 months after ERM surgery [
35]. Interestingly, in multiple regression analysis the preoperative perfusion state of Sattler’s layer was a statistically significant predictor of the postoperative BCVA. We assumed that the preoperative Sattler’s layer perfusion could reflect the capacity of choroidal blood flow, which is able to shift into the smaller vessels of the choriocapillaris after release of the ERM forces. However, future research should focus on preoperative and postoperative vascular alterations in ERM eyes with the presence of CB lesions and the influence of postoperative BCVA.
The main limitation of our study is its retrospective design. However, we would like to highlight the strengths of this study, which include a mean follow-up of 20 months (range 3–70 months) and a homogenous distribution of ERM and CB alteration stages in pseudophakic and phakic eyes in a cohort of representative sample size. Further prospective, randomized studies with larger cohorts and longer follow-ups are demanded to verify the impacts of abnormalities of the CB on short-term and long-term postoperative morphological and functional outcomes.
5. Conclusions
In conclusion, the results of this study show that in the long-term, neither ERM, nor CB alteration staging seem to be relevant predictors for functional outcomes following PPV with ERM and ILM peeling. However, BCVA at baseline appears to be a strong predictor for BCVA improvement following surgery. Therefore, precise evaluation of the fovea and classification of possible CB abnormalities appears to be a valuable tool in in the short-term, but not in the long-term.
Author Contributions
Conceptualization, S.M. and M.P.B.; methodology, M.P.B., F.R., M.R. and C.B.; software; validation, M.P.B., F.R., M.R. and C.B.; formal analysis, S.M., M.D.T. and N.G.J.; investigation, M.P.B. and C.B.; resources, S.M. and M.B.; data curation, M.P.B. and C.B.; writing—original draft preparation, M.P.B. and M.D.T.; writing—review and editing, S.M. and M.D.T.; visualization and supervision, S.M. and M.P.B.; project administration, S.M., M.P.B. and M.D.T.; funding acquisition, S.M. and M.B. All authors have read and agreed to the published version of the manuscript.
Funding
The project was supported by the “Stiftung wissenschaftliche Forschung, Fonds Ophthalmologie, City Hospital Triemli” and the Werner H. Spross Foundation, 8063 Zürich, Switzerland.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of Zurich (BASEC ID 2017-02306).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
None of the authors has any conflict of interest or financial tie to disclose.
References
- Cheung, N.; Tan, S.-P.; Lee, S.Y.; Cheung, G.C.M.; Tan, G.; Kumar, N.; Cheng, C.-Y.; Wong, T.Y. Prevalence and Risk Factors for Epiretinal Membrane: The Singapore Epidemiology of Eye Disease Study. Br. J. Ophthalmol. 2017, 101, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.H.; Cheung, N.; Wang, J.J.; Islam, A.F.M.; Kawasaki, R.; Meuer, S.M.; Cotch, M.F.; Klein, B.E.K.; Klein, R.; Wong, T.Y. Prevalence and Risk Factors for Epiretinal Membranes in a Multi-Ethnic United States Population. Ophthalmology 2011, 118, 694–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- You, Q.; Xu, L.; Jonas, J.B. Prevalence and Associations of Epiretinal Membranes in Adult Chinese: The Beijing Eye Study. Eye 2007, 22, 874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Govetto, A.; Lalane, R.A.; Sarraf, D.; Figueroa, M.S.; Hubschman, J.P. Insights Into Epiretinal Membranes: Presence of Ectopic Inner Foveal Layers and a New Optical Coherence Tomography Staging Scheme. Am. J. Ophthalmol. 2017, 175, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Schumann, R.G.; Gandorfer, A.; Ziada, J.; Scheler, R.; Schaumberger, M.M.; Wolf, A.; Kampik, A.; Haritoglou, C. Hyalocytes in Idiopathic Epiretinal Membranes: A Correlative Light and Electron Microscopic Study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Tanikawa, A.; Shimada, Y.; Horiguchi, M. Comparison of Visual Acuity, Metamorphopsia, and Aniseikonia in Patients with an Idiopathic Epiretinal Membrane. Jpn. J. Ophthalmol. 2018, 62, 280–285. [Google Scholar] [CrossRef]
- Govetto, A.; Bhavsar, K.V.; Virgili, G.; Gerber, M.J.; Freund, K.B.; Curcio, C.A.; Burgoyne, C.F.; Hubschman, J.-P.; Sarraf, D. Tractional Abnormalities of the Central Foveal Bouquet in Epiretinal Membranes: Clinical Spectrum and Pathophysiological Perspectives. Am. J. Ophthalmol. 2017, 184, 167–180. [Google Scholar] [CrossRef]
- Toro, M.D.; Reibaldi, M.; Avitabile, T.; Bucolo, C.; Salomone, S.; Rejdak, R.; Nowomiejska, K.; Tripodi, S.; Posarelli, C.; Ragusa, M.; et al. MicroRNAs in the Vitreous Humor of Patients with Retinal Detachment and a Different Grading of Proliferative Vitreoretinopathy: A Pilot Study. Transl. Vis. Sci. Technol. 2020, 9, 23. [Google Scholar] [CrossRef]
- Gagliano, C.; Toro, M.D.; Avitabile, T.; Stella, S.; Uva, M.G. Intravitreal Steroids for the Prevention of PVR After Surgery for Retinal Detachment. Curr. Pharm. Des. 2015, 21, 4698–4702. [Google Scholar] [CrossRef]
- Russo, A.; Ragusa, M.; Barbagallo, C.; Longo, A.; Avitabile, T.; Uva, M.G.; Bonfiglio, V.; Toro, M.D.; Caltabiano, R.; Mariotti, C.; et al. MiRNAs in the Vitreous Humor of Patients Affected by Idiopathic Epiretinal Membrane and Macular Hole. PLoS ONE 2017, 12, e0174297. [Google Scholar] [CrossRef]
- Chisari, C.G.; Toro, M.D.; Cimino, V.; Rejdak, R.; Luca, M.; Rapisarda, L.; Avitabile, T.; Posarelli, C.; Rejdak, K.; Reibaldi, M.; et al. Retinal Nerve Fiber Layer Thickness and Higher Relapse Frequency May Predict Poor Recovery after Optic Neuritis in MS Patients. J. Clin. Med. 2019, 8, 2022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reibaldi, M.; Uva, M.G.; Avitabile, T.; Toro, M.D.; Zagari, M.; Mariotti, C.; Cennamo, G.; Reibaldi, A.; Longo, A. Intrasession Reproducibility of RNFL Thickness Measurements Using SD-OCT in Eyes with Keratoconus. Ophthalmic Surg Lasers Imaging 2012, 43, S83–S89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longo, A.; Avitabile, T.; Uva, M.G.; Bonfiglio, V.; Russo, A.; Toro, M.D.; Faro, S.; Reibaldi, M. Morphology of the Optic Nerve Head in Glaucomatous Eyes with Visual Field Defects in Superior or Inferior Hemifield. Eur. J. Ophthalmol. 2018, 28, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Longo, A.; Avitabile, T.; Uva, M.G.; Bonfiglio, V.; Russo, A.; Toro, M.D.; Gagliano, C.; Fallico, M.; Reibaldi, M. Optic Nerve Head in Central Retinal Vein Occlusion by Spectral-Domain OCT. Eur. J. Ophthalmol. 2017, 27, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Longo, A.; Reibaldi, M.; Uva, M.G.; Bonfiglio, V.; Strano, M.C.; Russo, A.; Toro, M.D.; Bellino, M.; Avitabile, T. Acute Serous Macular Detachment and Edema after Uncomplicated Phacoemulsification: A Case Series. Can. J. Ophthalmol. 2015, 50, 476–479. [Google Scholar] [CrossRef]
- Reibaldi, M.; Russo, A.; Avitabile, T.; Uva, M.G.; Franco, L.; Longo, A.; Toro, M.D.; Cennamo, G.; Mariotti, C.; Neri, P.; et al. Treatment of Persistent Serous Retinal Detachment in Vogt-Koyanagi-Harada Syndrome with Intravitreal Bevacizumab during the Systemic Steroid Treatment. Retina 2014, 34, 490–496. [Google Scholar] [CrossRef]
- Chen, H.; Chi, W.; Cai, X.; Deng, Y.; Jiang, X.; Wei, Y.; Zhang, S. Macular Microvasculature Features before and after Vitrectomy in Idiopathic Macular Epiretinal Membrane: An OCT Angiography Analysis. Eye 2018, 33, 619–628. [Google Scholar] [CrossRef]
- Reibaldi, M.; Parravano, M.; Varano, M.; Longo, A.; Avitabile, T.; Uva, M.G.; Zagari, M.; Toro, M.; Boscia, F.; Boccassini, B.; et al. Foveal Microstructure and Functional Parameters in Lamellar Macular Hole. Am. J. Ophthalmol. 2012, 154, 974–980.e1. [Google Scholar] [CrossRef]
- Fallico, M.; Jackson, T.L.; Chronopoulos, A.; Hattenbach, L.-O.; Longo, A.; Bonfiglio, V.; Russo, A.; Avitabile, T.; Parisi, F.; Romano, M.; et al. Factors Predicting Normal Visual Acuity Following Anatomically Successful Macular Hole Surgery. Acta Ophthalmol. 2020. [Google Scholar] [CrossRef]
- Reibaldi, M.; Avitabile, T.; Longo, A.; Uva, M.G.; Bonfiglio, V.; Russo, A.; Toro, M.D.; Stella, S.; Giovannini, A.; Viti, F.; et al. Correlation of Preoperative Retinal Pigment Epithelium Status with Foveal Microstructure in Repaired Macular Holes. Ophthalmologica 2014, 232, 194–199. [Google Scholar] [CrossRef]
- Rochon-Duvigneau, A. Recherches sur la fovea de la retine humaine et particulie`rement sur le bouquet des coˆnes centraux. Arch Anat Microsc 1907, 9, 315–342. [Google Scholar]
- Lee, J.W.; Kim, I.T. Outcomes of Idiopathic Macular Epiretinal Membrane Removal with and without Internal Limiting Membrane Peeling: A Comparative Study. Jpn. J. Ophthalmol. 2010, 54, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.J.; Hoang, Q.V.; Ridley-Lane, M.L.; Sebrow, D.B.; Dhrami-Gavazi, E.; Chang, S. Long-Term Retrospective Analysis of Visual Acuity and Optical Coherence Topographic Changes after Single Versus Double Peeling During Vitrectomy for Macular Epiretinal Membranes. Retina (Philadelphia, PA) 2016, 36, 2101–2109. [Google Scholar] [CrossRef] [PubMed]
- Reibaldi, M.; Longo, A.; Avitabile, T.; Bonfiglio, V.; Toro, M.D.; Russo, A.; Viti, F.; Nicolai, M.; Saitta, A.; Giovannini, A.; et al. Transconjunctival Nonvitrectomizing Vitreous Surgery versus 25-Gauge Vitrectomy in Patients with Epiretinal Membrane: A Prospective Randomized Study. Retina 2015, 35, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, Y.M.; Chung, E.J.; Lee, S.Y.; Koh, H.J. Structural and Functional Predictors of Visual Outcome of Epiretinal Membrane Surgery. Am. J. Ophthalmol. 2012, 153, 103–110.e1. [Google Scholar] [CrossRef]
- Dawson, S.R.; Shunmugam, M.; Williamson, T.H. Visual Acuity Outcomes Following Surgery for Idiopathic Epiretinal Membrane: An Analysis of Data from 2001 to 2011. Eye 2014, 28, 219–224. [Google Scholar] [CrossRef] [Green Version]
- Dupas, B.; Tadayoni, R.; Erginay, A.; Massin, P.; Gaudric, A. Subfoveal Deposits Secondary to Idiopathic Epiretinal Membranes. Ophthalmology 2009, 116, 1794–1798. [Google Scholar] [CrossRef]
- Chowers, I.; Tiosano, L.; Audo, I.; Grunin, M.; Boon, C.J.F. Adult-Onset Foveomacular Vitelliform Dystrophy: A Fresh Perspective. Prog. Retin. Eye Res. 2015, 47, 64–85. [Google Scholar] [CrossRef]
- Brinkmann, M.P.; Michels, S.; Brinkmann, C.; Rommel, F.; Ranjbar, M.; Johansen, N.G.; Becker, M. Epiretinal membrane surgery outcome in eyes with abnormalities of the central bouquet. Int. J. Retin. Vitr. 2021, 14, 7. [Google Scholar] [CrossRef]
- Govetto, A.; Virgili, G.; Rodriguez, F.J.; Figueroa, M.S.; Sarraf, D.; Hubschman, J.P. FUNCTIONAL AND ANATOMICAL SIGNIFICANCE OF THE ECTOPIC INNER FOVEAL LAYERS IN EYES WITH IDIOPATHIC EPIRETINAL MEMBRANES: Surgical Results at 12 Months. Retina (Philadelphia, PA) 2017, 39, 347–357. [Google Scholar] [CrossRef]
- Kim, Y.J.; Kim, S.; Lee, J.Y.; Kim, J.-G.; Yoon, Y.H. Macular Capillary Plexuses after Epiretinal Membrane Surgery: An Optical Coherence Tomography Angiography Study. Br. J. Ophthalmol. 2018, 102, 1086–1091. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, Y.; Shimada, H.; Shinojima, A.; Nakashizuka, H. Foveal Avascular Zone Area Analysis Using Optical Coherence Tomography Angiography Before and after Idiopathic Epiretinal Membrane Surgery. Retina 2019, 39, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Bontzos, G.; Kabanarou, S.A.; Garnavou-Xirou, C.; Gkizis, I.; Kontou, E.; Triantafyllou, D.; Xirou, T. Segmentation Errors and Motion Artifacts in OCT-A Associated with Epiretinal Membranes. Can. J. Ophthalmol. 2020, 55, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, R.; D’Aloisio, R.; Viggiano, P.; Borrelli, E.; Iafigliola, C.; Di Nicola, M.; Aharrh-Gnama, A.; Di Marzio, G.; Toto, L.; Mariotti, C.; et al. Early Retinal Flow Changes after Vitreoretinal Surgery in Idiopathic Epiretinal Membrane Using Swept Source Optical Coherence Tomography Angiography. JCM 2019, 8, 2067. [Google Scholar] [CrossRef] [Green Version]
- Rommel, F.; Brinkmann, M.P.; Sochurek, J.A.M.; Prasuhn, M.; Grisanti, S.; Ranjbar, M. Ocular Blood Flow Changes Impact Visual Acuity Gain after Surgical Treatment for Idiopathic Epiretinal Membrane. JCM 2020, 9, 1768. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 ,
, 


{kind=link}
{kind=link}