
Paraoxonase/Arylesterase Activity of Serum Paraoxonase-1 and Schizophrenia: A Systematic Review and Meta-Analysis

1
Department of Biomedical Sciences, University of Sassari, 07100 Sassari, Italy
2
Discipline of Clinical Pharmacology, College of Medicine and Public Health, Flinders University, Bedford Park, SA 5042, Australia
3
Department of Clinical Pharmacology, Flinders Medical Centre, Southern Adelaide Local Health Network, Bedford Park, SA 5042, Australia
*
Author to whom correspondence should be addressed.
Antioxidants 2023, 12(8), 1484; https://doi.org/10.3390/antiox12081484
Submission received: 16 June 2023
/
Revised: 18 July 2023
/
Accepted: 20 July 2023
/
Published: 25 July 2023
(This article belongs to the Special Issue Oxidative Stress, Inflammation and Antioxidant Defense System in Psychiatric Disorders)
Abstract
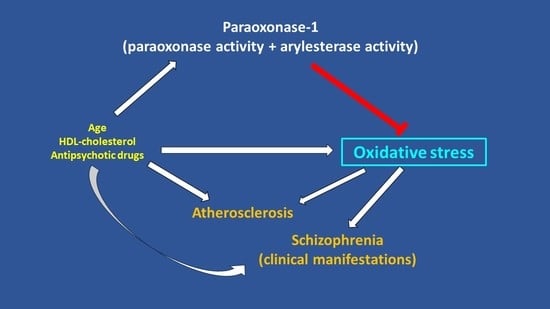
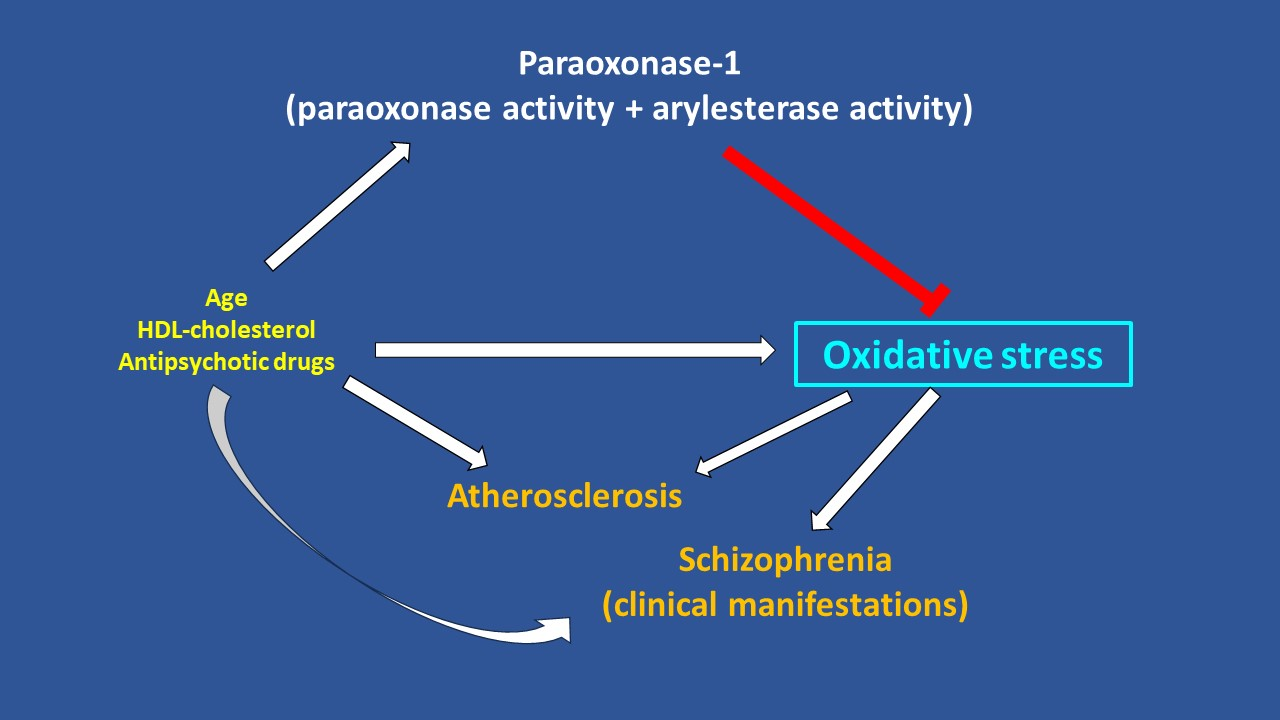
:The presence of a pro-oxidant state in patients with schizophrenia may account for the increased risk of atherosclerosis and cardiovascular disease in this group and supports the potential utility of circulating biomarkers of oxidative stress for risk stratification and management. We investigated this issue by conducting a systematic review and meta-analysis of the association between the circulating concentrations of paraoxonase-1, an antioxidant calcium-dependent high-density lipoprotein (HDL)-associated esterase, with paraoxonase and arylesterase activity in schizophrenia. We searched electronic databases from inception to 31 May 2023 for studies investigating paraoxonase-1 in patients with schizophrenia and healthy controls and assessed the risk of bias and the certainty of evidence (PROSPERO registration number: CRD42023435442). Thirteen studies were identified for analysis. There were no significant between-group differences in paraoxonase (standard mean difference, SMD = 0.12, 95% CI −0.23 to 0.48, p = 0.50; extremely low certainty of evidence) or arylesterase activity (SMD = −0.08, 95% CI −0.39 to 0.23, p = 0.61; very low certainty of evidence). However, in meta-regression and subgroup analysis we observed significant associations between the SMD of paraoxonase and age (p = 0.003), HDL–cholesterol (p = 0.029), and study country (p = 0.04), and the SMD of arylesterase and age (p = 0.007), body mass index (p = 0.012), HDL–cholesterol (p = 0.002), and pharmacological treatment for schizophrenia (p < 0.001). In the absence of overall between-group differences, our systematic review and meta-analysis suggests that alterations in paraoxonase-1 may reflect a pro-oxidant state in specific subgroups of patients with schizophrenia that require further assessment in appropriately designed studies.
1. Introduction
There is increasing evidence from experimental models and human studies that schizophrenia and associated psychiatric disorders, e.g., schizoaffective disorder, are characterised by a dysregulated immune system and a pro-oxidative state [1,2,3,4,5]. Local inflammation (neuroinflammation) and abnormalities in the balance between antioxidant and pro-oxidant mechanisms are likely to be involved in the pathogenesis and the progression of schizophrenia [6,7,8,9]. However, the co-existence of a systemic pro-inflammatory and pro-oxidant state may also account for the increased risk of several other disease states in patients with schizophrenia, which imposes a further health and financial burden to this patient group as well as to healthcare systems worldwide [10,11,12,13]. For example, several epidemiological studies have recently reported a significant increase in the risk of atherosclerosis and cardiovascular disease, conditions that are also characterised by a pro-inflammatory and pro-oxidant state, in patients with schizophrenia [14,15,16,17,18]. These observations support the proposition that oxidative stress plays a critical pathophysiological role in the onset and the progression of schizophrenia and in the association between schizophrenia and atherosclerosis and cardiovascular disease. Furthermore, they suggest that the identification of circulating biomarkers of oxidative stress may be useful for risk stratification as well as for the monitoring of the clinical effects of specific antipsychotic and cardioprotective treatments in patients with schizophrenia [1,19,20,21,22,23,24,25]. One such potential biomarker is paraoxonase-1, an antioxidant calcium-dependent high-density lipoprotein (HDL)-associated glycoprotein esterase containing 354 amino acids which possesses a combined paraoxonase and arylesterase activity [26]. The hydrophobic sequence located in the N-terminal region of paraoxonase-1 favors its interaction with HDL [27,28].
The paraoxonase multi-gene family is widely expressed in mammals and includes paraoxonase-1, paraoxonase-2, and paraoxonase-3 [26]. Paraoxonase-1 and paraoxonase-3 are mainly present in the circulation whereas paraoxonase-2 is located intracellularly [29]. Paraoxonase-1 is the most studied in basic research and clinical studies as it has a wider range of substrates and circulating concentrations that are at least twofold those of paraoxonase-3 [30,31]. Consequently, the assessment of circulating paraoxonase-1 likely reflects the majority of circulating paraoxonase activity. This includes paraoxonase activity (which uses the substrate paraoxon) and arylesterase activity (which uses the substrate phenylacetate) [31,32,33,34]. A number of studies have recently highlighted the potential clinical utility of measuring the circulating concentrations of paraoxonase-1 in several disease states, particularly in autoimmune, circulatory, and respiratory disorders [35,36,37,38,39,40,41]. Paraoxonase-1 exerts a critical role in maintaining the antioxidant effects of HDL, and its reduction is believed to promote a dysfunctional HDL which, in turn, can paradoxically favor the onset of atherosclerosis and other inflammatory conditions [28,42,43,44,45,46]. For example, in a meta-analysis of six observational studies including a total of 15,064 subjects, the pooled age-adjusted risk ratio (RR) for any cardiovascular event per each one standard deviation (SD) increase in paraoxonase-1 concentration was 0.87 (95% confidence intervals, CI, 0.80 to 0.96, p = 0.005) [47]. Therefore, a reduction in paraoxonase-1 concentration might account for a systemic pro-oxidative state as well as the increased cardiovascular risk observed in patients with schizophrenia.
We investigated this issue by conducting a systematic review and meta-analysis of studies reporting circulating paraoxonase-1 concentrations in patients with schizophrenia and healthy controls and assessing possible associations between the effect size of paraoxonase and arylesterase activity and pre-defined variables. We speculated that schizophrenia is associated with a significant reduction in the enzymatic activity of paraoxonase and arylesterase, reflecting the presence of a pro-oxidant state in this patient group.
2. Methods
2.1. Literature Search
We searched PubMed, Web of Science, and Scopus from inception to 31 May 2023. The following terms and their combination were used in the systematic search: “paraoxonase” or “PON” or “arylesterase” and “schizophrenia” or “acute psychotic disorder” or “schizoaffective disorder”. Two independent investigators screened the abstracts and, if relevant, individual articles according to the following criteria: (i) the assessment of plasma or serum paraoxonase-1 concentrations; (ii) the assessment of paraoxonase and/or arylesterase activity in patients with schizophrenia and in healthy controls (case-control design); (iii) the assessment of 10 or more patients; (iv) the use of English language; and (v) the availability of the full-text of the article. The 2 investigators also searched the references of individual articles for additional studies. A third investigator was involved in case of disagreement.
Extracted parameters included: first author, year of publication, study country, number of participants, age, sex distribution, body mass index, serum concentrations of paraoxonase, arylesterase, and HDL–cholesterol, and pharmacological treatment for schizophrenia. We assessed the risk of bias (Joanna Briggs Institute critical appraisal checklist for analytical studies; studies addressing ≥ 75% checklist items were adjudicated as low risk [48]) and the certainty of evidence (grades of recommendation, assessment, development and evaluation, GRADE, working group system [49,50]). We fully complied with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 statement (Supplementary Tables S1 and S2) [51] and registered our review in the International Prospective Register of Systematic Reviews (PROSPERO registration number: CRD42023435442).
2.2. Statistical Analysis
Forest plots of standardized mean differences (SMD) and 95% confidence intervals (CIs) were generated to evaluate the presence of differences in paraoxonase-1 concentrations between patients with schizophrenia and healthy controls (statistical significance set at p < 0.05). Means and standard deviations were extrapolated from medians and interquartile ranges or ranges [52,53], or using the Graph Data Extractor software (San Diego, CA, USA). The presence of between-study SMD heterogeneity was assessed using the Q statistic (statistical significance set at p < 0.10) and the I2 statistic. [54,55,56]. The stability of the effect size was assessed in a sensitivity analysis [57]. Publication bias was assessed with the Begg’s and Egger’s tests [58,59] and the “trim-and-fill” method [60]. Univariate meta-regression and subgroup analyses were conducted to investigate the presence of associations between the effect size and several pre-defined variables: age, proportion of males, year of publication, study country, sample size, body mass index, HDL–cholesterol concentrations, and pharmacological treatment for schizophrenia. Statistical analyses were performed using Stata 14 (STATA Corp, College Station, TX, USA).
3. Results
3.1. Systematic Search
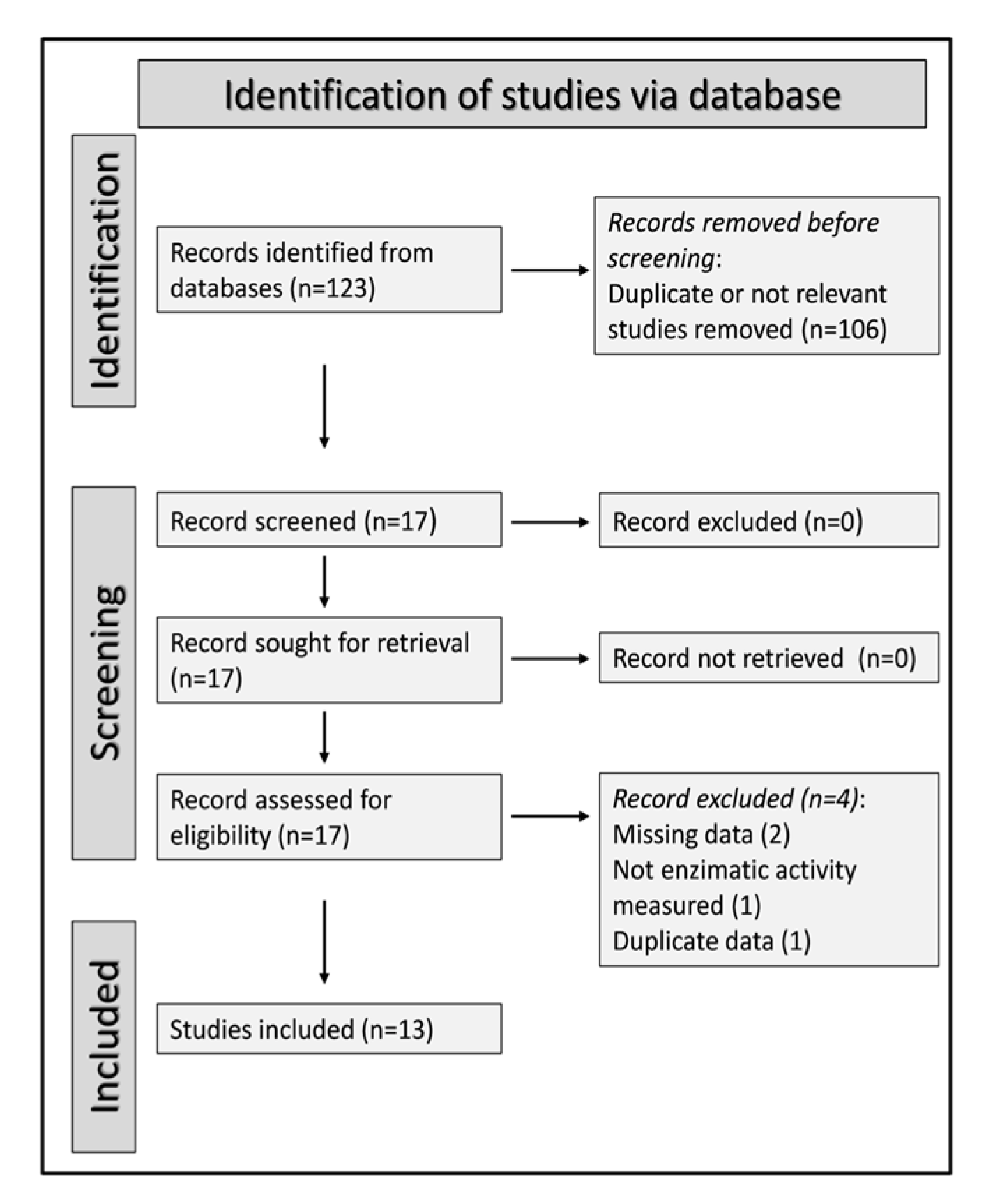
A flow chart of the screening process is described in Figure 1. After identifying a total of 123 articles, 106 were excluded as they were either duplicates or not relevant to the search strategy. After a full-text revision of the remaining 17 articles, 4 were further excluded (missing information: 2 studies; duplicate data: 1 study; paraoxonase-1 assay not performed as enzyme activity: 1 study), leaving 13 studies for final analysis [61,62,63,64,65,66,67,68,69,70,71,72,73]. The selected studies, published between 2007 and 2018, investigated a total of 825 patients with schizophrenia with a mean age of 36 years (66% males) and 725 healthy controls with a mean age of 36 years (58% males; Table 1).
3.2. Paraoxonase Activity
Nine studies that included 13 study groups investigated paraoxonase activity in a total of 570 patients with schizophrenia (mean age 37 years, 65% males) and 512 healthy controls (mean age 38 years, 59% males) [61,62,63,64,65,68,69,70,71]. Seven studies were conducted in Turkey [61,62,63,68,69,70,71], one in Romania [64], and one in Tunisia [65]. Patients received pharmacological treatment for schizophrenia in 11 study groups [61,62,63,64,65,68,69,70,71] and no treatment in the remaining 2 [61,68]. The enzymatic activity of paraoxonase was evaluated by using paraoxon as a substrate in all the selected studies [61,62,63,64,65,68,69,70,71]. Furthermore, all studies had a low risk of bias (Supplementary Table S3) [61,62,63,64,65,68,69,70,71].
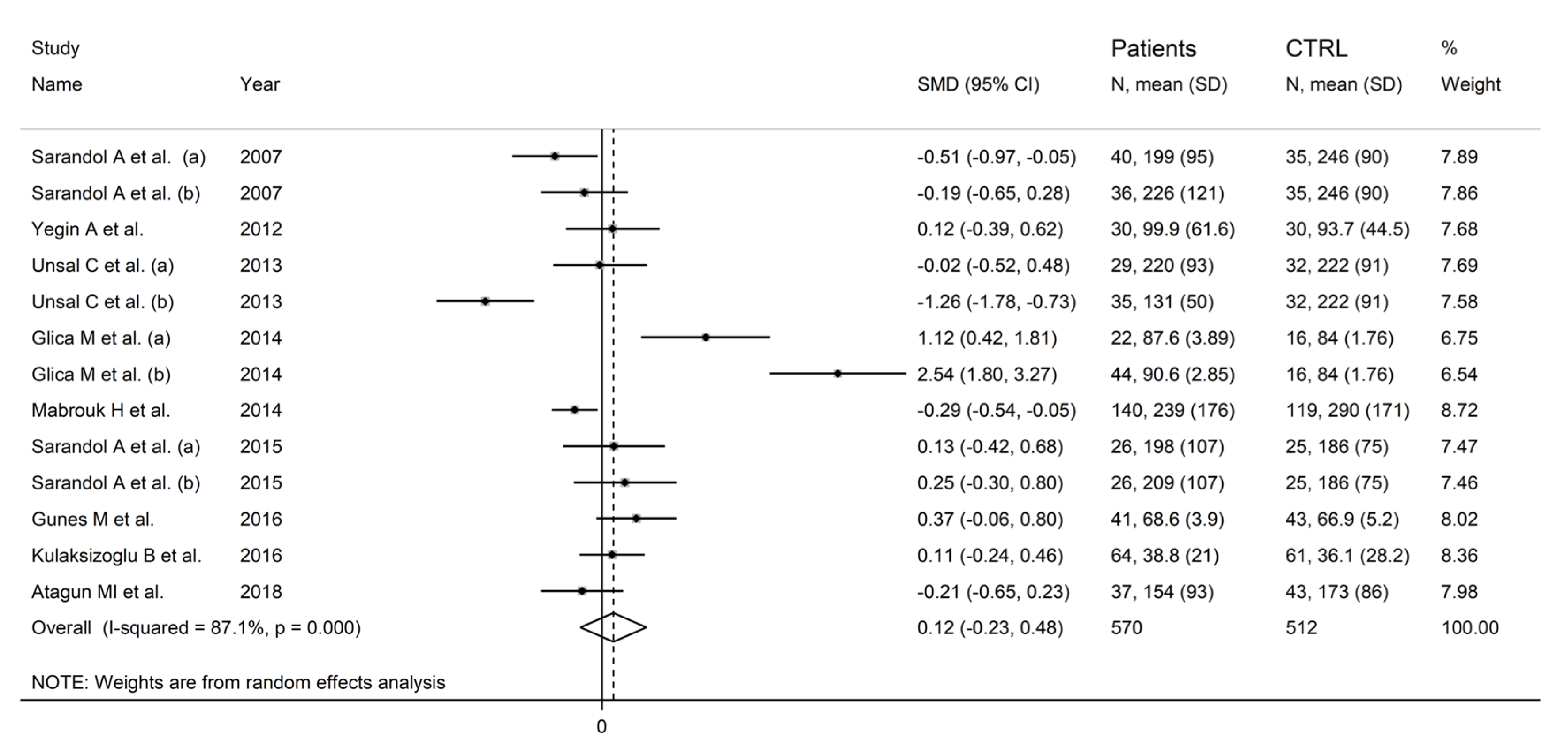
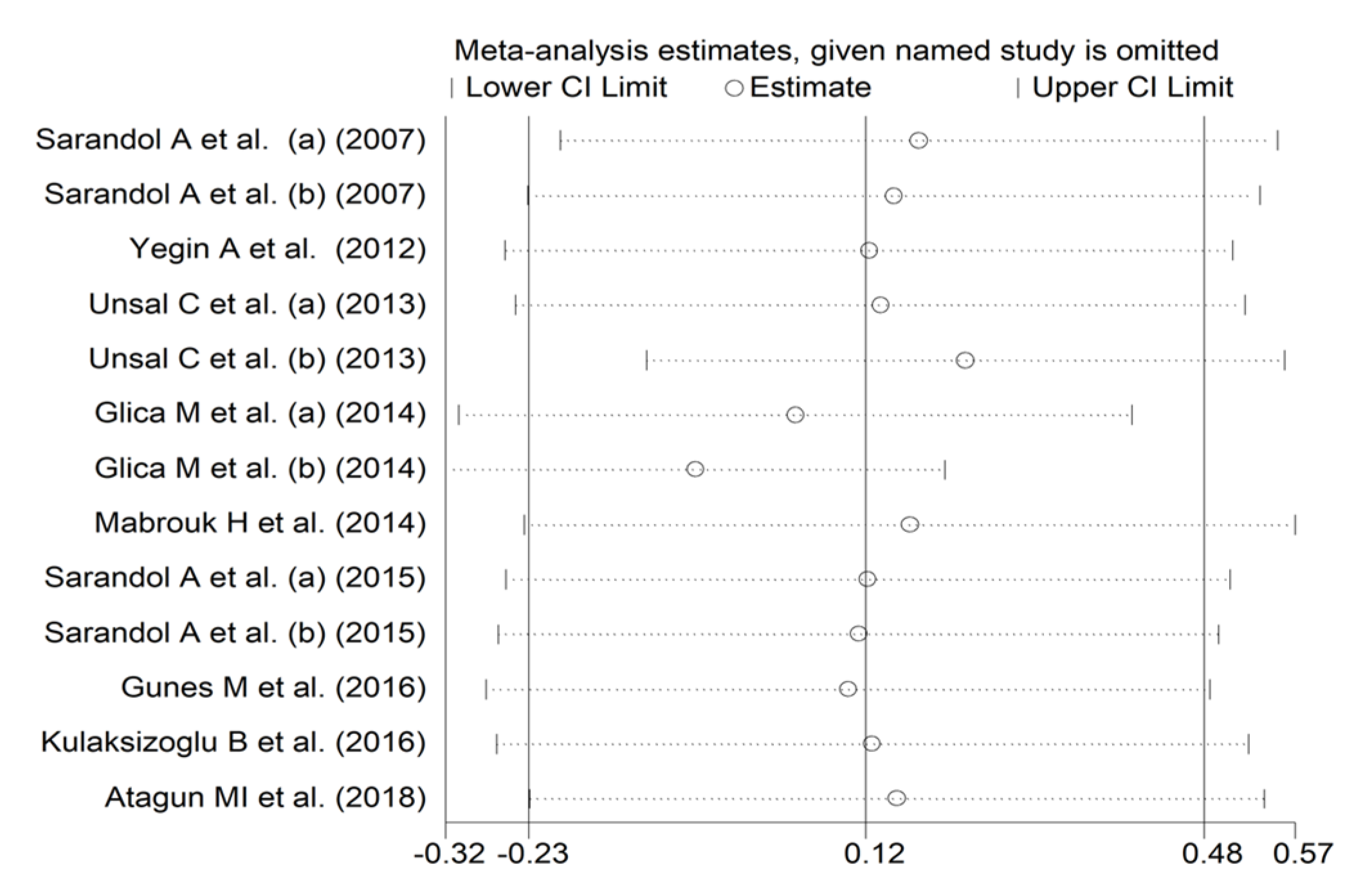
In forest plots, paraoxonase activity was non-significantly different between control subjects and patients with schizophrenia (SMD = 0.12, 95% CI −0.23 to 0.48, p = 0.50; I2 = 87.1%, p < 0.001; Figure 2). A sensitivity analysis showed stability of the effect size, with the corresponding SMD values ranging between −0.06 and 0.13 (Figure 3).
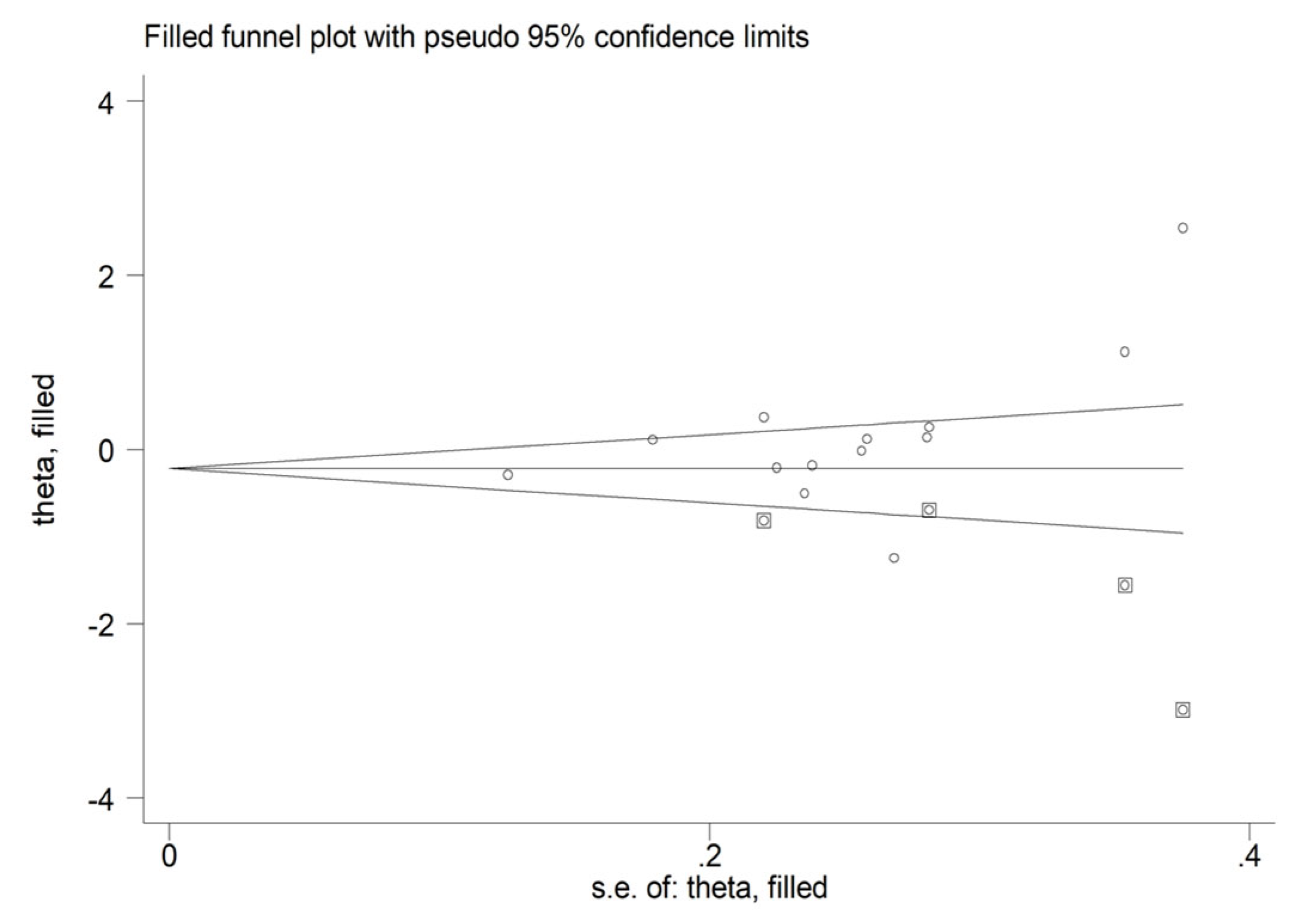
There was a significant publication bias with the Begg’s test (p = 0.04) but not with the Egger’s test (p = 0.10). The “trim-and-fill” procedure identified four studies to be added to the funnel plot (Figure 4). The resulting SMD was −0.23 (95% CI −0.62 to 0.16, p = 0.25).
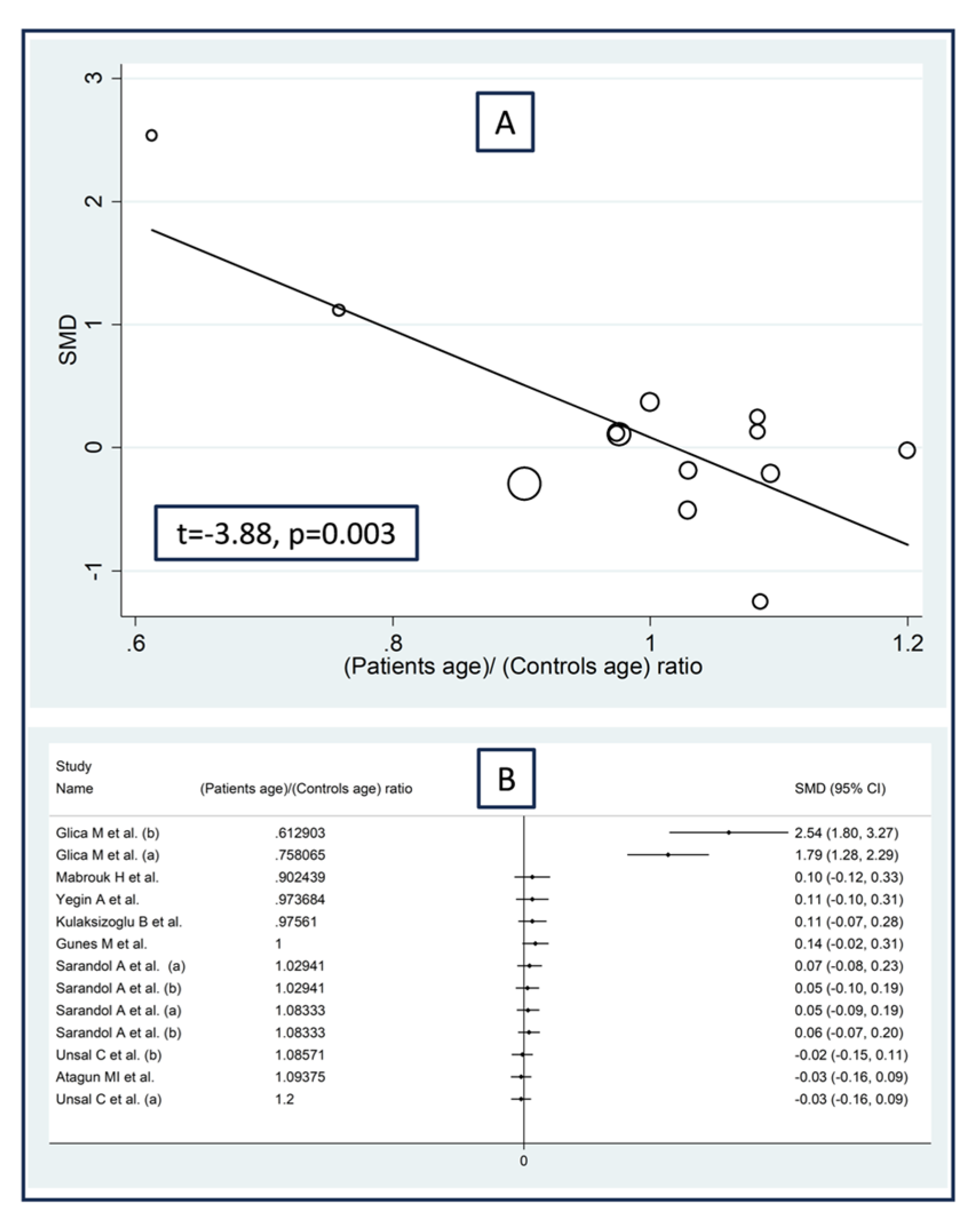
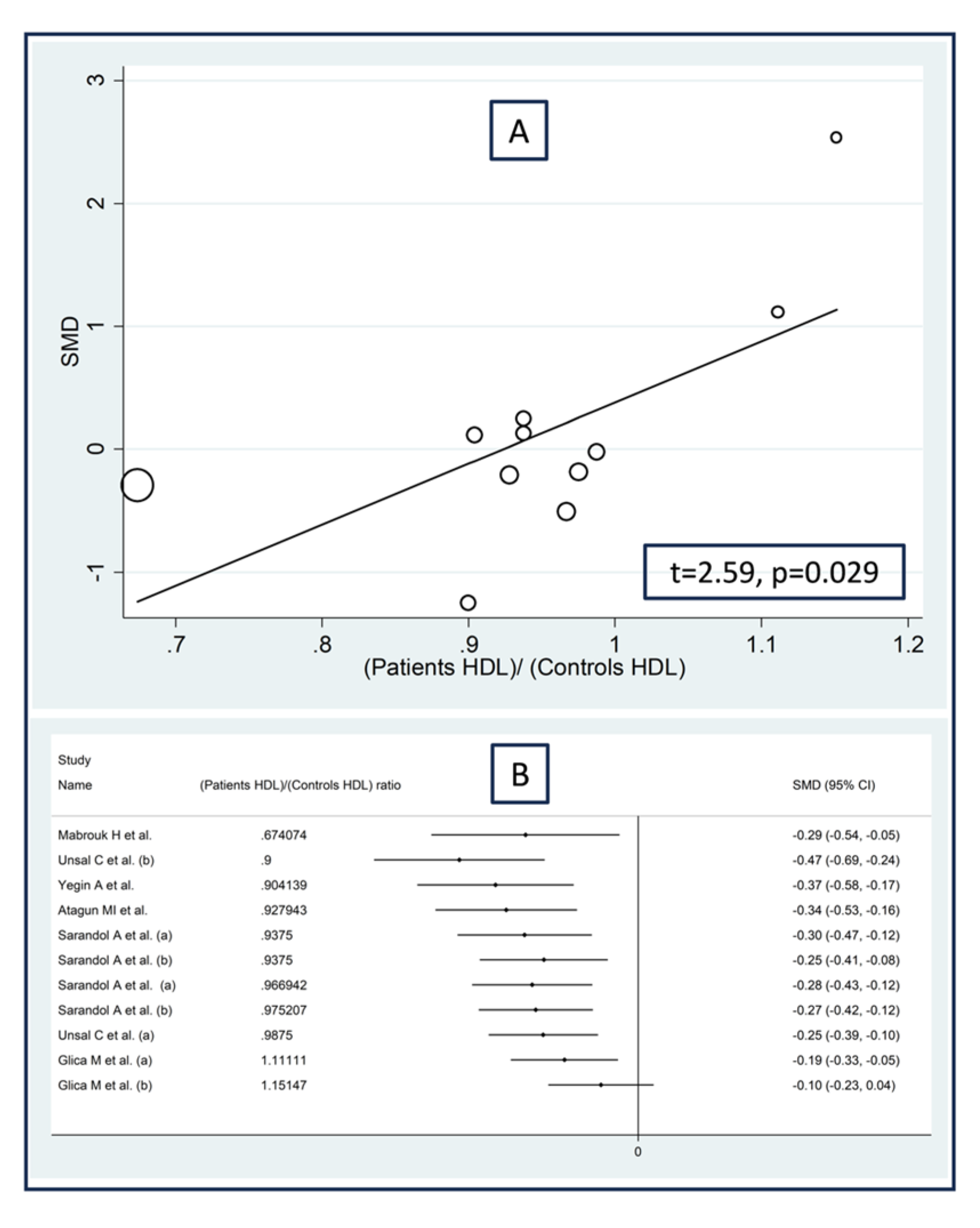
Non-significant associations were observed between the effect size of paraoxonase activity and the proportion of males (t = −1.68, p = 0.13), the publication year (t = 0.76, p = 0.46), the sample size (t = −0.79, p = 0.45), or the body mass index (t = 2.24, p = 0.052) in the meta-regression analysis. By contrast, there was a significant negative association with the patient/control age ratio (t = −3.88, p = 0.003; Figure 5A) and a significant positive association between the effect size and the patient/control HDL–cholesterol ratio (t = 2.59, p = 0.029; Figure 6A). These associations were also confirmed using the metacum analysis command (Figure 5B and Figure 6B).
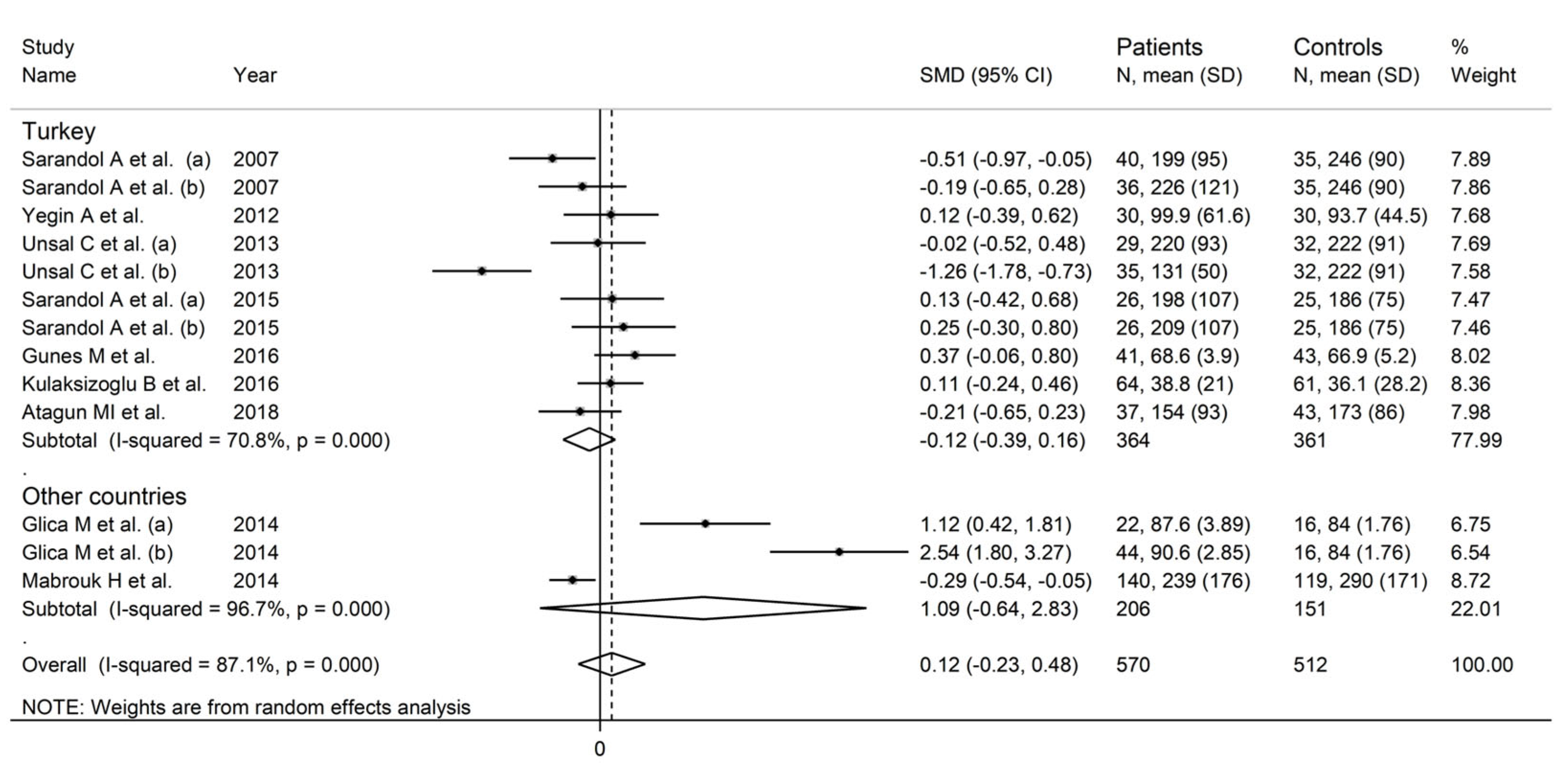
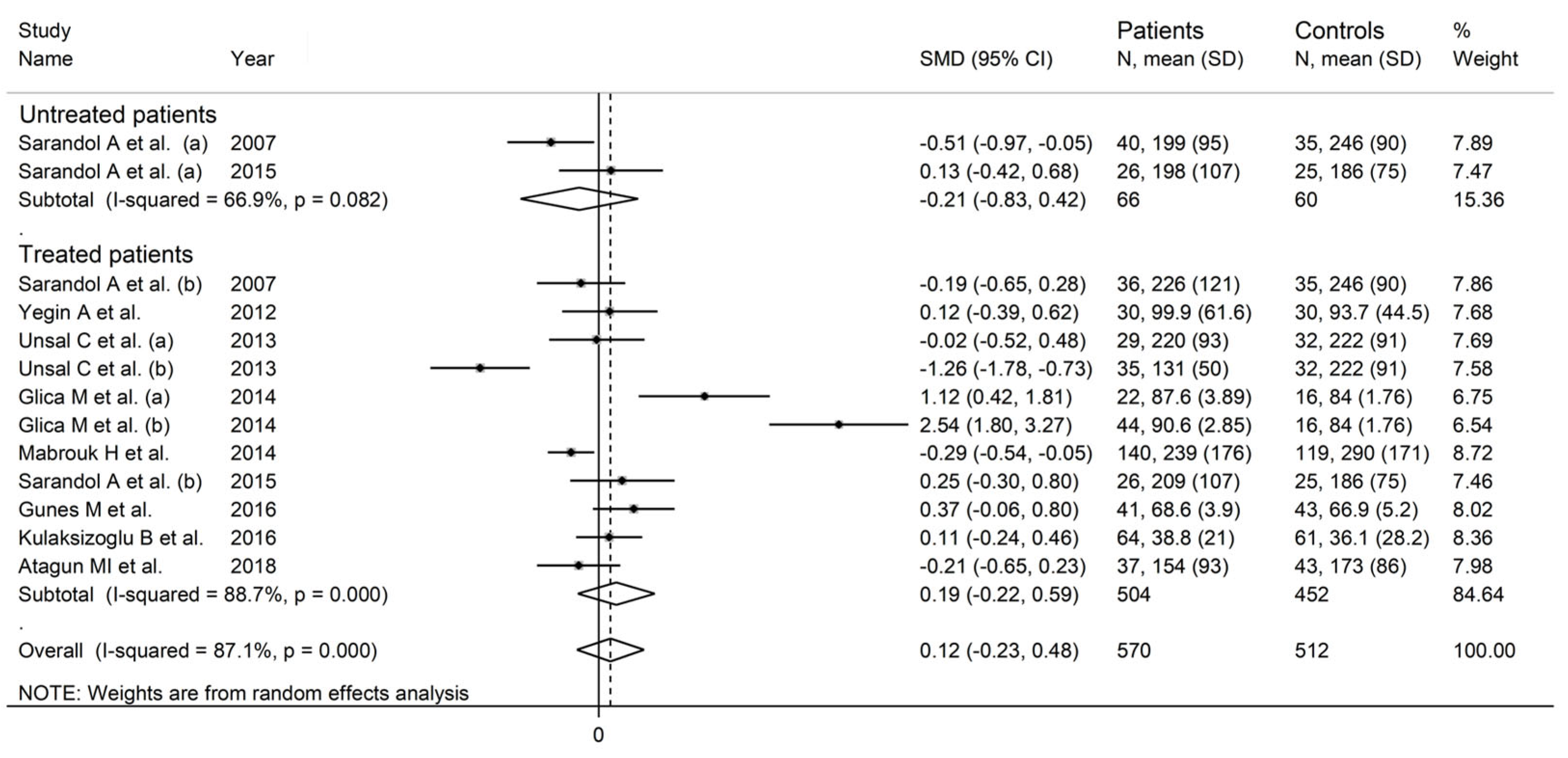
In a subgroup analysis, the SMD was significantly smaller (p = 0.04) in studies conducted in Turkey (SMD = −0.12, 95% CI −0.39 to 0.16, p = 0.41; I2 = 70.8%, p < 0.001) than those conducted in other countries (SMD = 1.09, 95% CI −0.64 to 2.83, p = 0.22; I2 = 96.7%, p < 0.001; Figure 7). There were non-significant differences (p = 0.58) in the pooled SMD between studies performed in untreated patients (SMD = −0.21, 95% CI −0.83 to 0.42, p = 0.51; I2 = 66.9%, p = 0.082) and those in treated patients (SMD = 0.19, 95% CI −0.22 to 0.59, p = 0.37; I2 = 88.7%, p < 0.001; Figure 8).
The low level of certainty for cross-sectional studies (rating 2, ⊕⊕⊝⊝) was downgraded to extremely low (rating 0, ⊝⊝⊝⊝) after considering the high and unexplained heterogeneity, the relatively high imprecision, and the presence of publication bias.
3.3. Arylesterase Activity
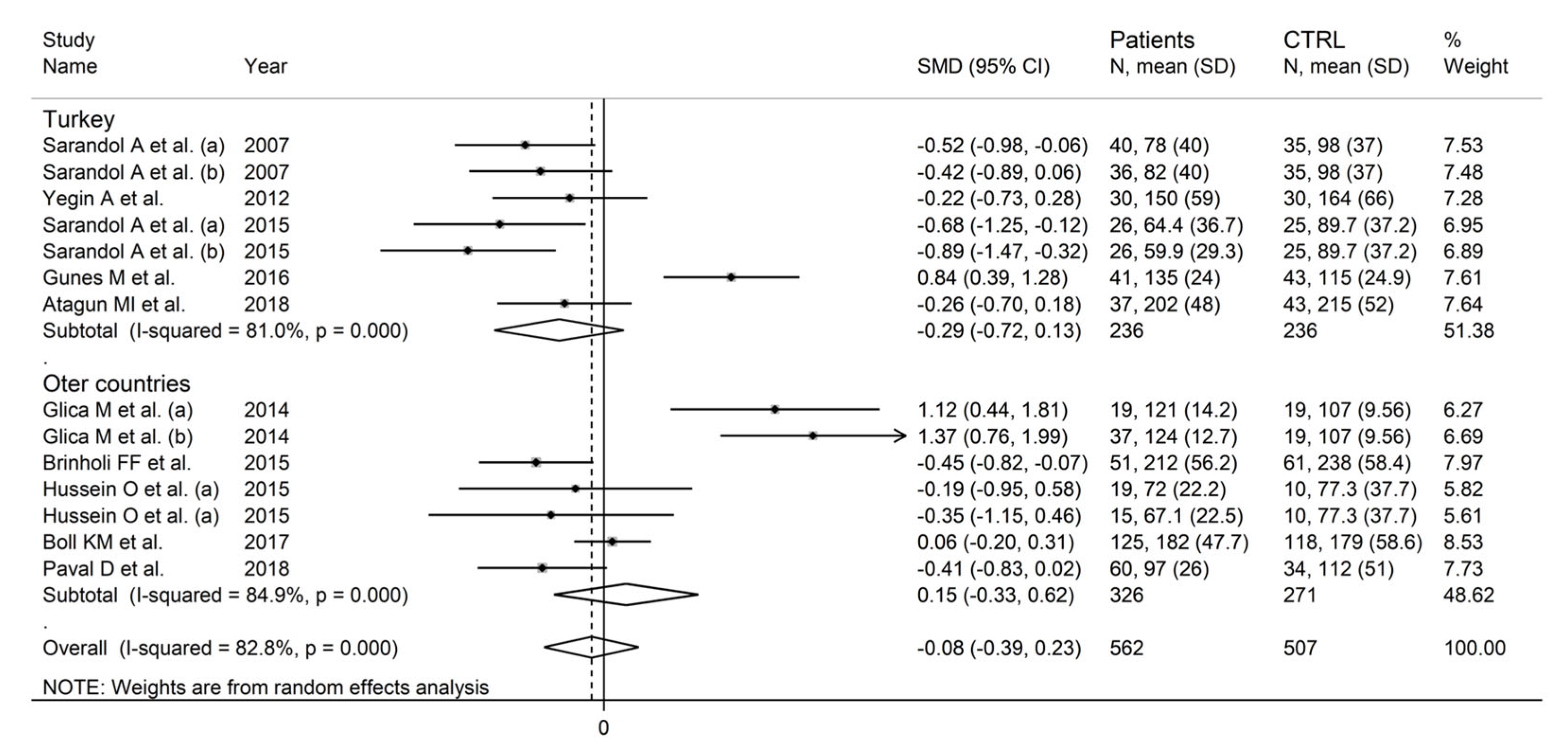
Ten studies including 14 study groups, all with a low risk of bias (Supplementary Table S3), reported arylesterase activity in a total of 562 patients (mean age 34 years, 65% males) and 507 healthy controls (mean age 35 years, 59% males) [61,62,64,66,67,68,69,71,72,73]. Five studies were conducted in Turkey [61,62,68,69,71], two in Romania [64,73], two in Brazil [66,72], and one in Israel [67]. Ten study groups investigated patients receiving pharmacological treatment for schizophrenia [61,62,64,67,68,69,71,72,73] and four untreated patients [61,66,67,68]. Arylesterase activity was evaluated by using phenylacetate as a substrate in all studies [61,62,64,66,67,68,69,71,72,73].
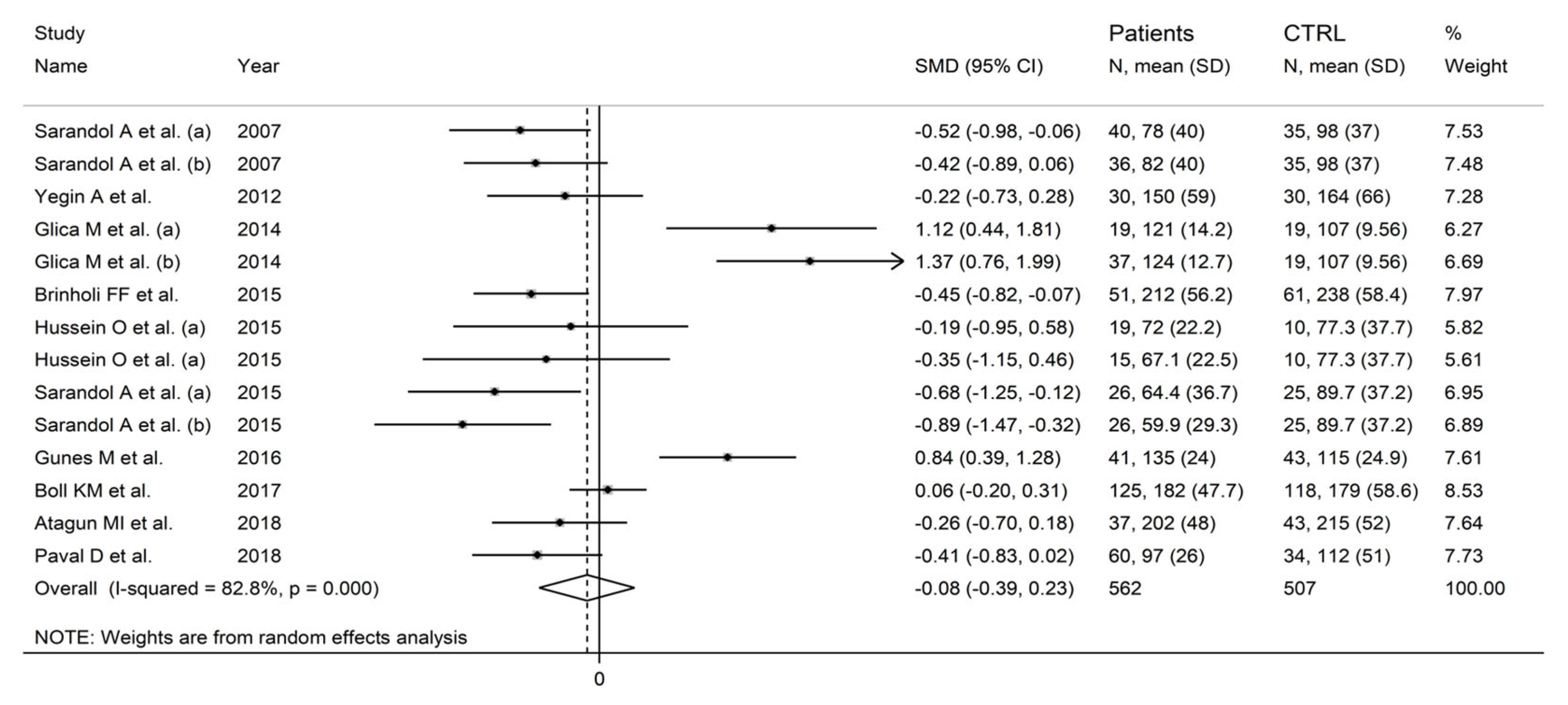
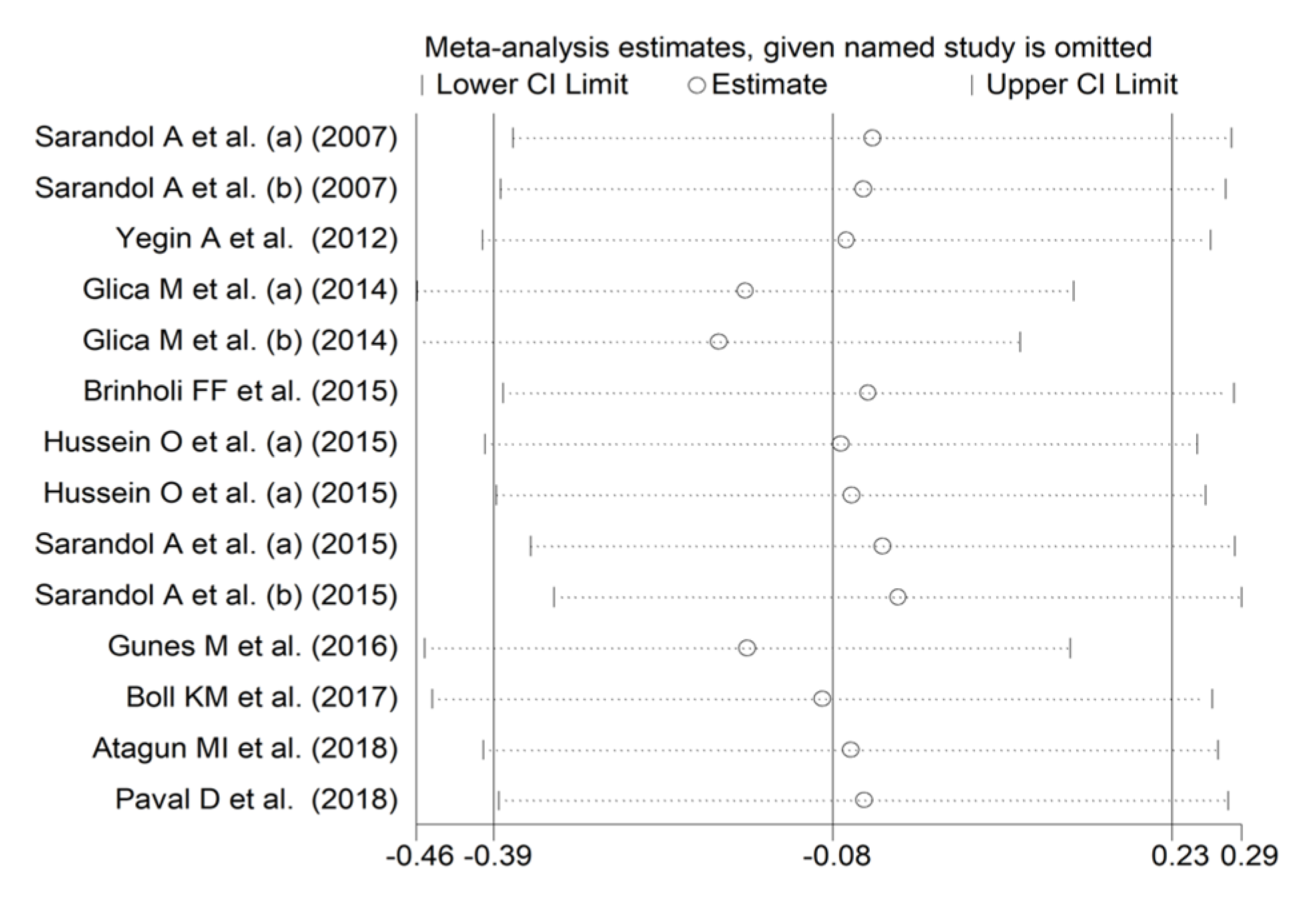
In forest plots, arylesterase activity was non-significantly different between control subjects and patients with schizophrenia (SMD = −0.08, 95% CI −0.39 to 0.23; p = 0.61; I2 = 82.8%, p < 0.001; Figure 9). A sensitivity analysis showed stability of the results, with pooled SMD values ranging between −0.16 and −0.02; Figure 10).
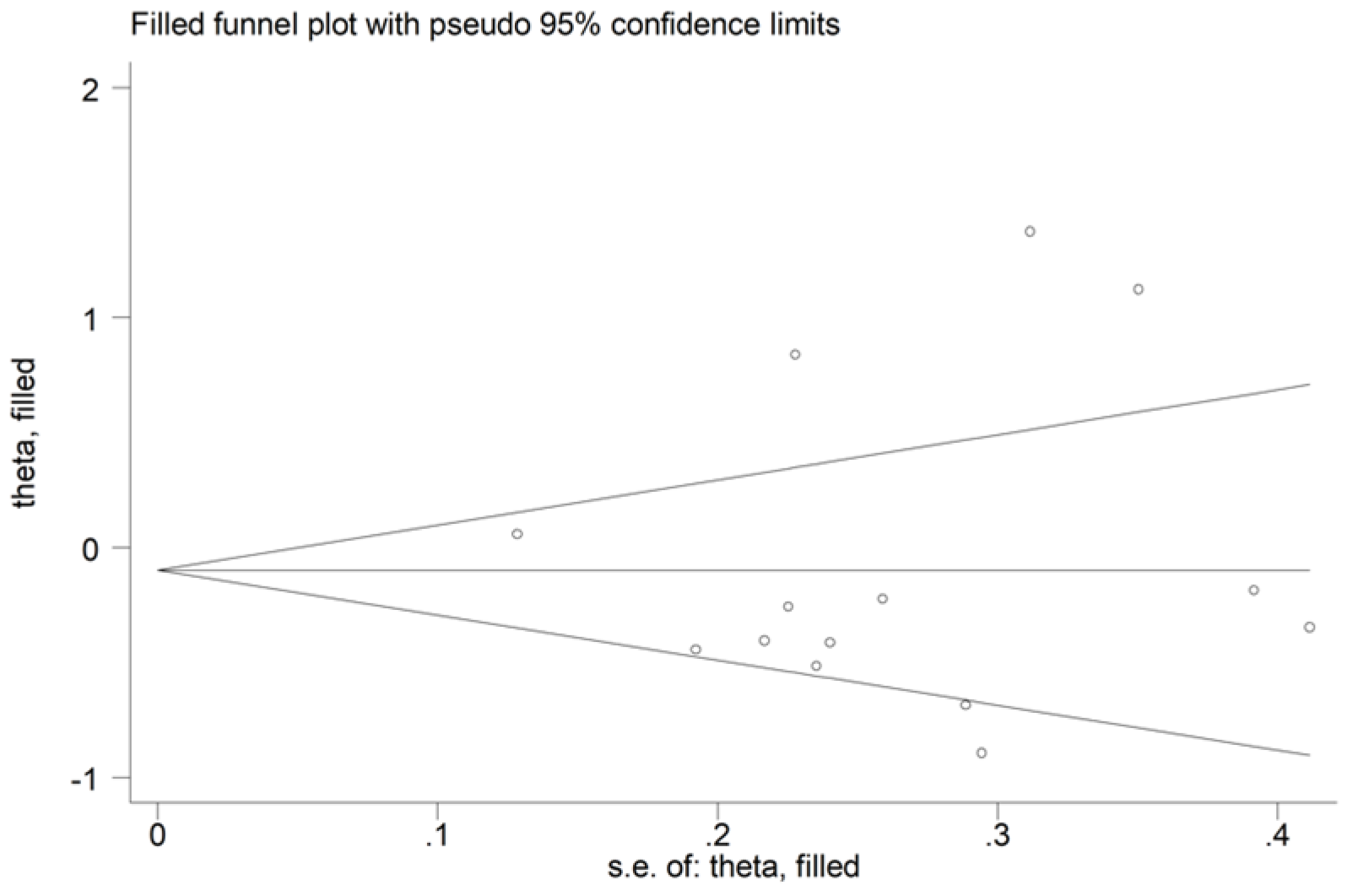
There was no publication bias with the Begg’s test (p = 0.66), the Egger’s test (p = 0.75), or the “trim-and-fill” method (Figure 11).
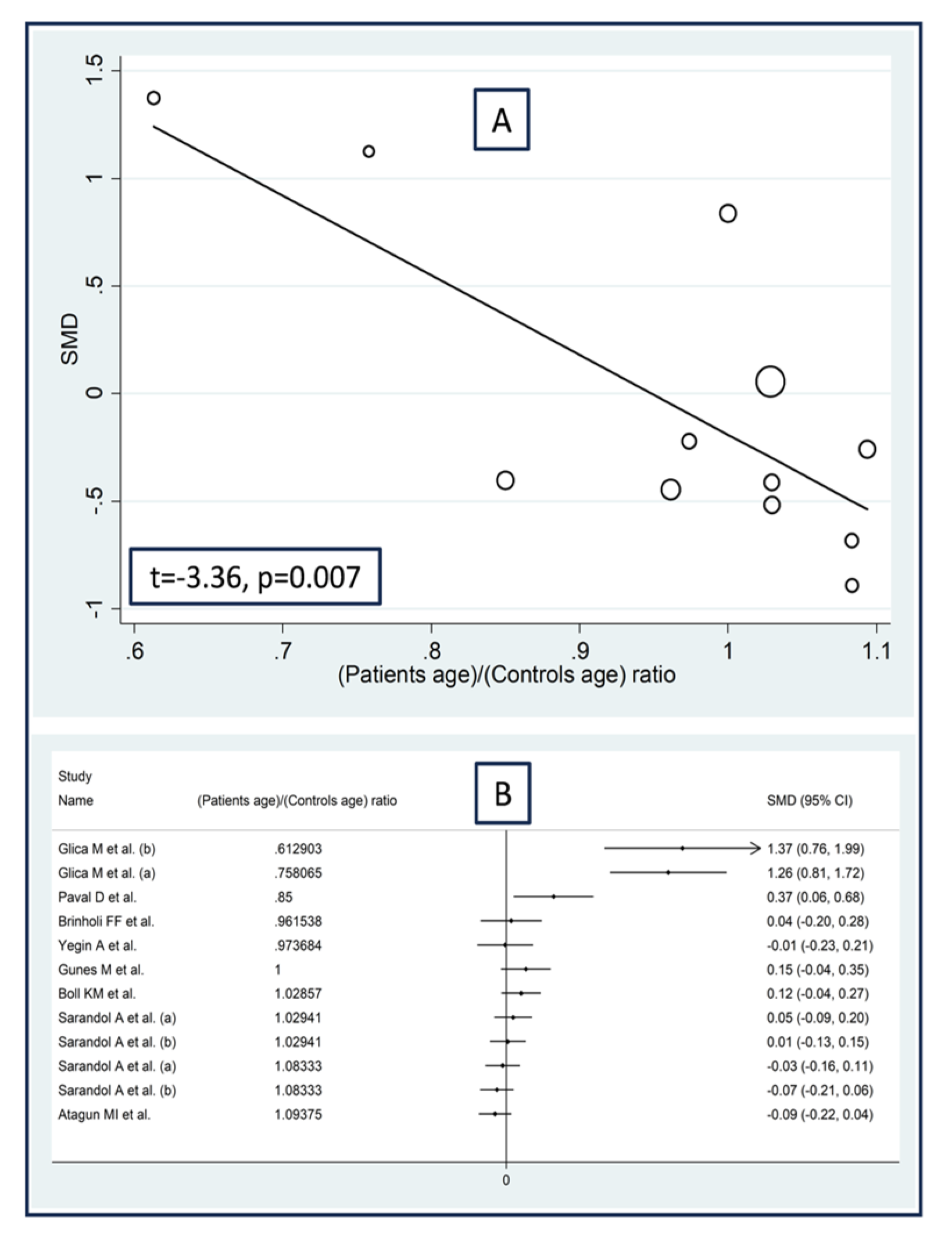
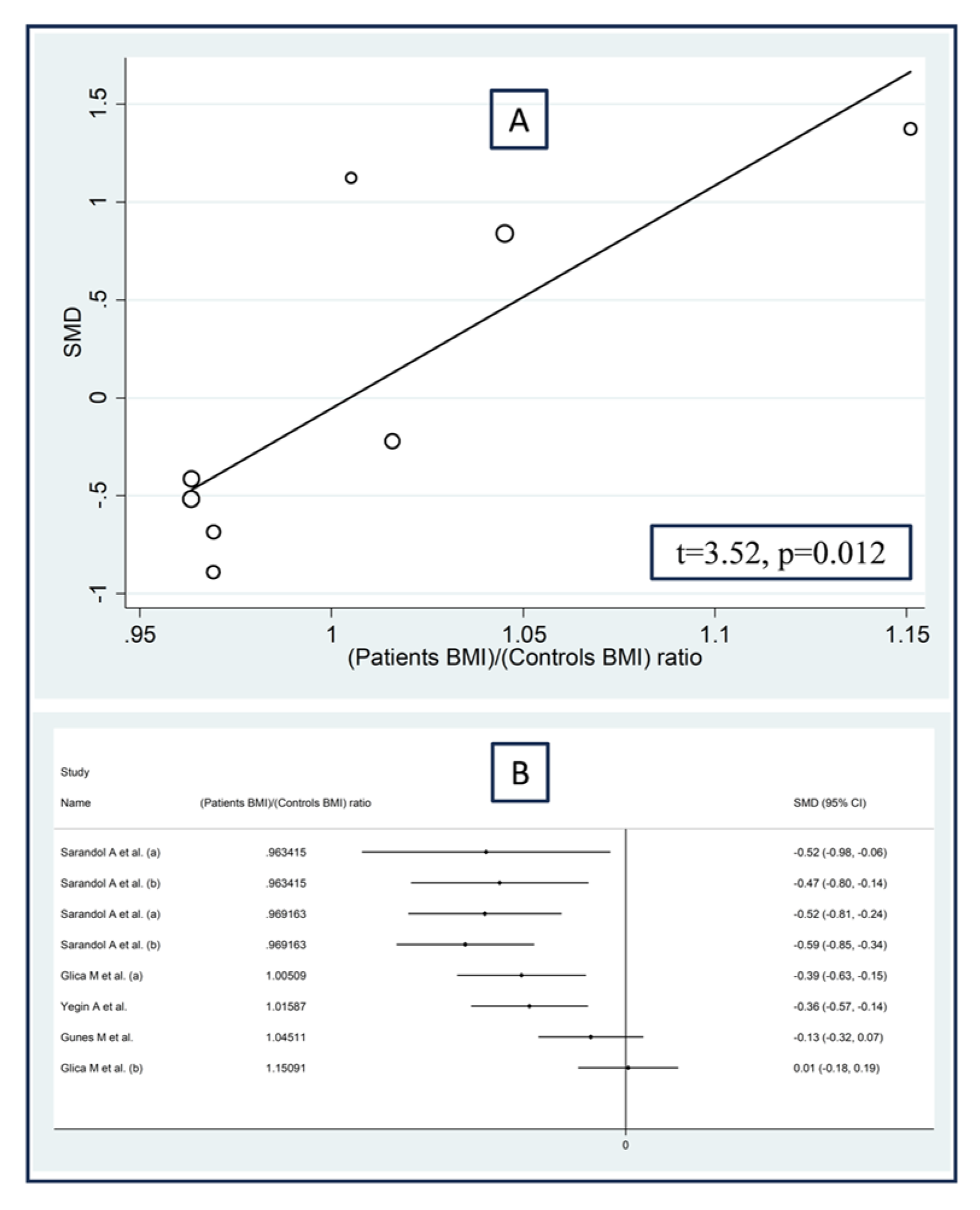
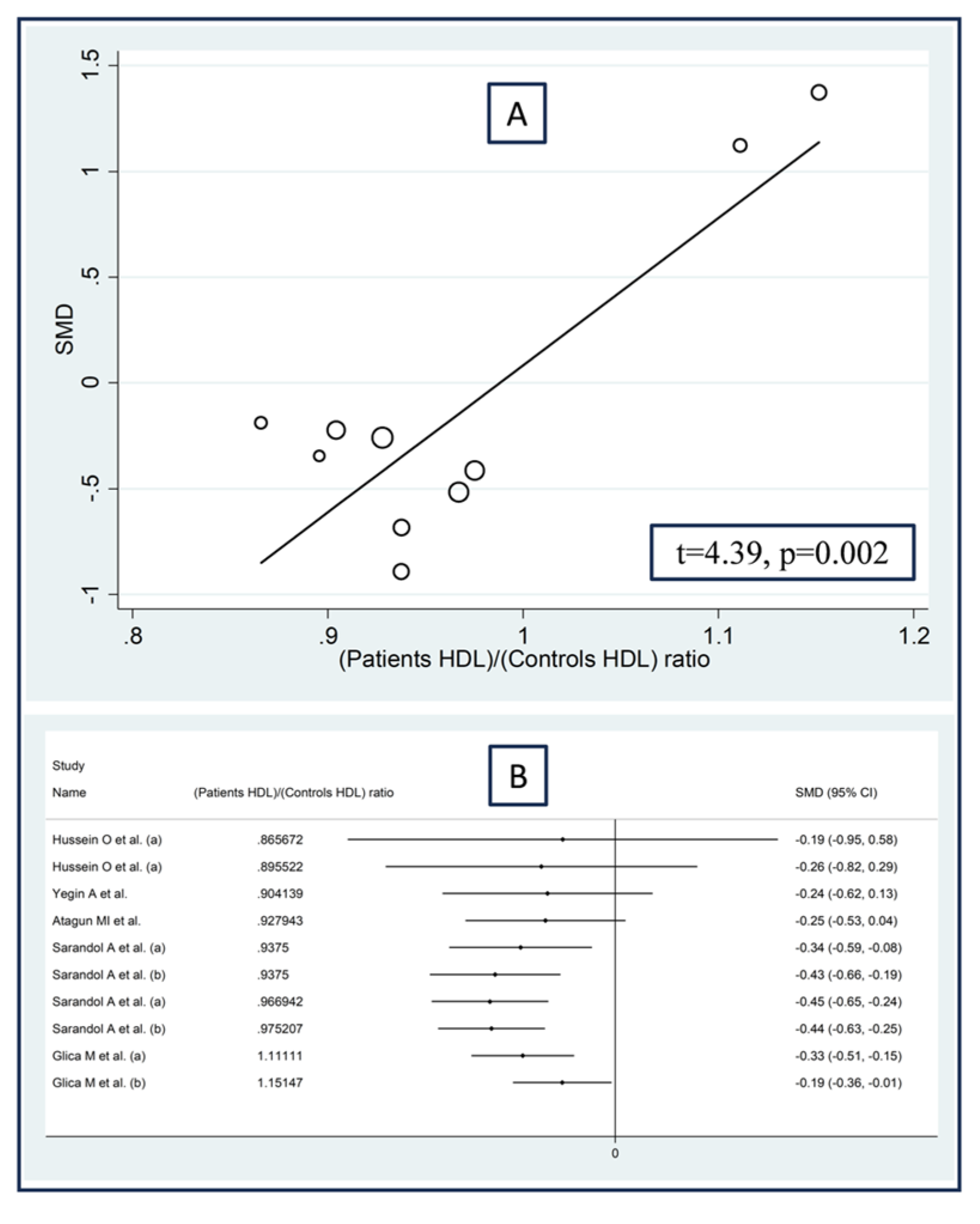
No significant associations were observed in meta-regression between the effect size and the proportion of males (t = −1.07, p = 0.31), the publication year (t = 0.46, p = 0.65), or the sample size (t = −0.02, p = 0.99). By contrast, we observed significant positive associations between the effect size and the patient/control age ratio (t = −3.36, p = 0.007; Figure 12A), the patient/control body mass index ratio (t = 3.52, p = 0.012; Figure 13A), and the patient/control HDL–cholesterol ratio (t = 4.39, p = 0.002; Figure 14A). Similar results were observed using the metacum analysis command (Figure 12B, Figure 13B and Figure 14B).
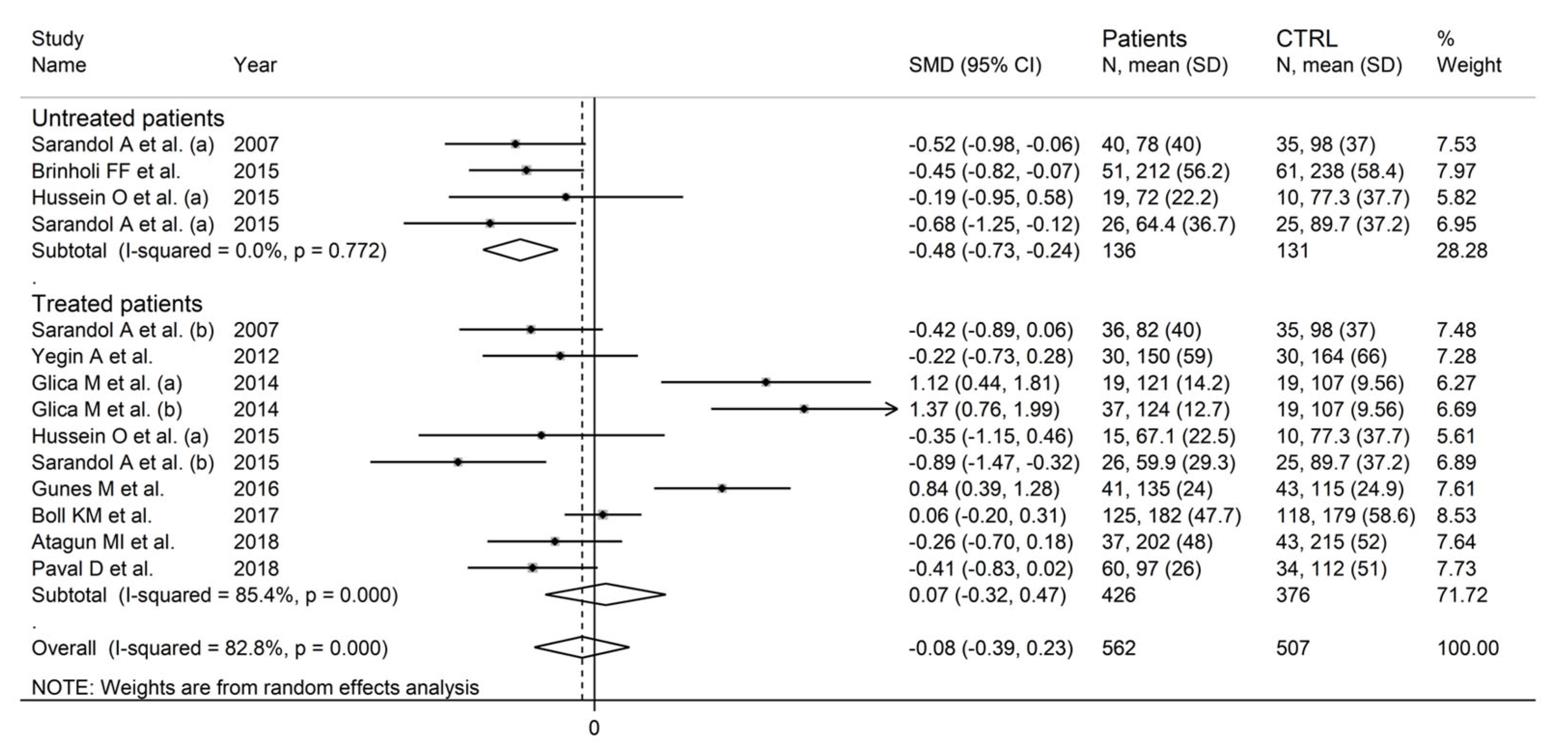
In the subgroup analysis, there were non-significant differences (p = 0.23) in SMD values between studies conducted in Turkey (SMD = −0.29, 95% CI −0.72 to 0.13, p = 0.18; I2 = 81.0%, p < 0.001) and those conducted in other countries (SMD = 0.15, 95% CI −0.33 to 0.62, p = 0.54; I2 = 84.9%, p < 0.001; Figure 15). By contrast, the pooled SMD was significantly lower in studies conducted in untreated patients (SMD = −0.48, 95% CI −0.73 to −0.24, p < 0.001; I2 = 0.0%, p = 0.77) but not in those conducted in treated patients (SMD = 0.07, 95% CI −0.32 to 0.47, p = 0.71; I2 = 85.4%, p < 0.001; Figure 16), with a virtually absent heterogeneity in the former subgroup.
The low level of certainty for cross-sectional studies (rating 2, ⊕⊕⊝⊝) was downgraded to very low (rating 1, ⊕⊝⊝⊝) after taking into account the relatively high imprecision (relatively large confidence intervals).
4. Discussion
In our systematic review and meta-analysis, the enzymatic activity of paraoxonase and arylesterase, two essential components of circulating paraoxonase-1, were non-significantly different between patients with schizophrenia and healthy controls. However, in a meta-regression analysis we identified the presence of significant associations between the effect size of paraoxonase activity and patient/control age and HDL–cholesterol ratios, and between the effect size of arylesterase activity and patient/control age, body mass index, and HDL–cholesterol ratios. Furthermore, in a subgroup analysis the effect size of paraoxonase activity was significantly associated with the study country, whereas the effect size of arylesterase was significantly associated with pharmacological treatment for schizophrenia. In sensitivity analyses, the pooled SMD values of paraoxonase and arylesterase activity were not substantially influenced by individual studies, suggesting stability of the results of the meta-analysis.
The increasing evidence of a state of oxidative stress associated with schizophrenia has stimulated a significant body of research investigating the clinical significance of alterations in the redox state in this condition as well as other associated co-morbidities. In this context, studies have recently investigated the association between several biomarkers of oxidative stress, the duration of schizophrenia, and specific symptoms and psychopathological features of the disease, with contrasting results in terms of the direction of the observed associations [9,74]. Pending the results of additional investigations seeking to address this issue, the observed inconsistency in the available evidence could be related, at least in part, to the multiple biochemical and molecular pathways involved in redox homeostatic mechanisms and the complex analytical procedures required for the determination of biomarkers of oxidative stress in the blood and other biological matrices, with the potential for error [75,76]. Another factor that is likely to play an important role is represented by the interindividual variability in the clinical and demographic characteristics of the study participants [9].
In terms of inter-individual variability in patient characteristics, there is good evidence that the redox state can be significantly influenced by age [77], gender [78], and several other sociodemographic and biochemical factors, particularly cigarette smoking, C-reactive protein concentrations, hyperglycaemia, nutrients, physical activity, and body mass index [79,80]. This complexity could explain, at least in part, some of the results of our meta-regression and subgroup analyses, particularly the significant negative associations between the SMD of paraoxonase/arylesterase activity and the patient/control age ratio and the significant positive associations between the SMD of paraoxonase/arylesterase and the patient/control HDL–cholesterol ratio. In other words, our analyses suggest that further studies are more likely to observe significant reductions in paraoxonase/arylesterase activity in subgroups of schizophrenic patients with older age and low HDL–cholesterol concentrations rather than older patients with high HDL–cholesterol concentrations and younger patients with low or high HDL–cholesterol concentrations. This hypothesis is also in line with the reported associations between schizophrenia and other conditions characterized by a pro-oxidative state, particularly atherosclerosis and cardiovascular disease, that are also more likely to affect older schizophrenic patients with relatively low HDL–cholesterol concentrations, given the established role of advancing age and low HDL–cholesterol as cardiovascular risk factors [81,82].
The presence of a strong association between schizophrenia and atherosclerotic cardiovascular disease has been highlighted in a systematic review and meta-analysis that included 38 studies, of which 29 were longitudinal, assessing a total of 1,591,106 patients with schizophrenia. In cross-sectional studies, schizophrenia was significantly associated with the presence of coronary heart disease (adjusted odds ratio, OR = 1.52, 95% CI 1.48 to 1.56, p < 0.001), cerebrovascular disease (adjusted OR = 2.05, 95% CI 1.59 to 2.64, p < 0.001), and congestive heart failure (adjusted OR = 1.60, 95% CI 1.06 to 2.40, p = 0.02). Similar results were observed in longitudinal studies where schizophrenia was significantly associated with incident cardiovascular disease (adjusted hazard ratio, HR = 1.95, 95% CI 1.41 to 2.70, p < 0.001), incident coronary heart disease (adjusted HR = 1.59, 95% CI 1.08 to 2.35, p = 0.02), incident cerebrovascular disease (adjusted HR = 1.57, 1.09 to 2.25, p = 0.02), and incident congestive heart failure (unadjusted relative risk, RR = 1.80, 95% CI 1.15 to 2.79, p = 0.009) [14]. A number of mechanisms have been suggested to account for the increased cardiovascular risk in patients with schizophrenia, including the high prevalence of smoking, unhealthy dietary patterns, and physical inactivity [17,83]. Studies have also reported a significant reduction in the concentrations of HDL–cholesterol, a cholesterol fraction that is critically linked with paraoxonase-1, in patients with schizophrenia [84,85,86]. In one study, patients with acute-phase schizophrenia had significantly lower HDL concentrations compared to healthy subjects (43 ± 14 vs. 53 ± 13 mg/dL, p = 0.03). Interestingly, a significant increase in HDL–cholesterol was observed in patients who responded to three-week treatment with atypical antipsychotic drugs (+4 ± 8 mg/dL, p = 0.007) but not with conventional antipsychotics (+0.5 ± 14 mg/dL, p = 0.82) [87]. The beneficial effects of some antipsychotic agents on HDL–cholesterol concentrations have also been reported in a systematic review and meta-analysis of 22 studies that investigated the effects of 10 different antipsychotics in 7073 patients compared to placebos in 2189 patients. Aripiprazole and brexpiprazole were the antipsychotic agents causing the greatest increase in HDL–cholesterol concentrations vs. placebo [88]. Additional studies should investigate the presence of possible associations between paraoxonase/arylesterase activity, individual cardiovascular risk factors, and clinical cardiovascular endpoints (e.g., myocardial infarction, stroke, and congestive heart failure) in schizophrenia. These studies should also determine whether such associations are influenced by age, sex, ethnicity, specific disease subtypes, HDL–cholesterol concentrations, and treatment with specific antipsychotic drugs.
Another interesting observation in our subgroup analysis was the presence of significant reductions in arylesterase activity in studies of untreated patients but not in those of patients receiving pharmacological treatment for schizophrenia. Albeit hypothesis-generating, this finding suggests that treatment with antipsychotic drugs might increase arylesterase activity to levels that are comparable to those observed in healthy subjects. This would dilute the differences in arylesterase activity between treated patients and healthy controls. A systematic review and meta-analysis published in 2011 did not report any conclusive evidence regarding the effect of antipsychotic drugs on oxidative stress [89]. However, a more recent systematic review has reported that olanzapine, paliperidone, risperidone, and haloperidol prevent oxidative stress-induced neurotoxicity in in vitro studies [90]. Clearly, more research is warranted to investigate the effect of individual antipsychotic drugs on oxidative stress in patients with schizophrenia in studies that also include a range of genetic polymorphisms of paraoxonase as a potential modulating factor [91,92,93,94]. This issue is particularly relevant as there is good evidence that treatment with antipsychotic medications, particularly atypical antipsychotics, is also associated with weight gain, insulin resistance, diabetes, and dyslipidaemia in this patient group, with a consequent increase in the overall cardiovascular risk [95,96,97]. At the same time, however, a large observational study in 62,250 patients with schizophrenia followed for 20 years has reported that antipsychotic treatment is associated with reduced all-cause mortality and cardiovascular mortality in schizophrenia, with an adjusted HR of 0.62 (95% CI 0.57 to 0.67) for cardiovascular mortality. Notably, even in the presence of significant variability, virtually all studied antipsychotic agents were associated with a reduced risk of cardiovascular mortality in this study, particularly quetiapine (HR = 0.51, 95% CI 0.43 to 0.61), aripiprazole (HR = 0.52, 95% CI 0.30 to 0.89), clozapine (HR = 0.55, 95% CI 0.46 to 0.64), and risperidone (HR = 0.64, 95% CI 0.56 to 0.73) [98]. In another study, the duration of treatment with antipsychotics (including typical and atypical antipsychotics) was significantly associated with a reduced risk of cardiovascular events in patients with schizophrenia (adjusted OR = 0.95, 95% CI 0.91 to 0.99, p = 0.014) after adjusting for age, urea, creatinine, uric acid, thyroxine, leukocytes, body mass index, and diastolic blood pressure [99]. Large, well-designed prospective studies are likely to shed light on the complex interplay between schizophrenia, oxidative stress assessed by measuring paraoxonase/arylesterase activity, antipsychotic drugs, and cardiovascular disease.
Strengths of our study are the combined assessment of paraoxonase and arylesterase enzymatic activity, essential components of paraoxonase-1, the comprehensive set of meta-regression and subgroup analyses, the rigorous assessment of the risk of bias and the certainty of evidence, and the stability of the results after sequentially removing individual studies in a sensitivity analysis. A significant limitation is that a significant proportion of studies was conducted in one country, Turkey, which limits the generalisability of the results to other patient populations, particularly European, North American, and Eastern Asian patients. This issue requires further research as studies conducted in USA and South Africa have reported the presence of significant ethnic-related differences in paraoxonase-1 [100,101,102].
5. Conclusions
Our study has shown the presence of non-significant differences in circulating paraoxonase-1, expressed as paraoxonase and arylesterase enzyme activity, between patients with schizophrenia and healthy controls. However, the results of meta-regression and subgroup analyses suggest that such differences may be significant in subgroups of patients with schizophrenia, particularly older patients with relatively low HDL–cholesterol concentrations. Further studies should address this issue by investigating paraoxonase-1 and the possible effects of antipsychotic drugs and other antioxidant strategies on disease progression and cardiovascular risk in these subgroups and consider the modulating effect of genetic polymorphisms of paraoxonase-1 and ethnic differences.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/antiox12081484/s1, Table S1: PRISMA 2020 for abstracts checklist; Table S2: PRISMA 2020 checklist; Table S3: The Joanna Briggs Institute critical appraisal checklist.
Author Contributions
A.Z., S.S. and A.A.M. conceived the study, conducted the literature search, and analyzed the data. A.A.M. wrote the first draft. A.Z., S.S. and A.A.M. reviewed further drafts and the final version. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The relevant data are available from A.Z. upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Upthegrove, R.; Khandaker, G.M. Cytokines, Oxidative Stress and Cellular Markers of Inflammation in Schizophrenia. Curr. Top. Behav. Neurosci. 2020, 44, 49–66. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.J.; Rogers, J.C.; Katshu, M.; Liddle, P.F.; Upthegrove, R. Oxidative Stress and the Pathophysiology and Symptom Profile of Schizophrenia Spectrum Disorders. Front. Psychiatry 2021, 12, 703452. [Google Scholar] [CrossRef] [PubMed]
- Rambaud, V.; Marzo, A.; Chaumette, B. Oxidative Stress and Emergence of Psychosis. Antioxidants 2022, 11, 1870. [Google Scholar] [CrossRef] [PubMed]
- Mandal, P.K.; Gaur, S.; Roy, R.G.; Samkaria, A.; Ingole, R.; Goel, A. Schizophrenia, Bipolar and Major Depressive Disorders: Overview of Clinical Features, Neurotransmitter Alterations, Pharmacological Interventions, and Impact of Oxidative Stress in the Disease Process. ACS Chem. Neurosci. 2022, 13, 2784–2802. [Google Scholar] [CrossRef]
- Fisar, Z. Biological hypotheses, risk factors, and biomarkers of schizophrenia. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2023, 120, 110626. [Google Scholar] [CrossRef]
- Vallee, A. Neuroinflammation in Schizophrenia: The Key Role of the WNT/beta-Catenin Pathway. Int. J. Mol. Sci. 2022, 23, 2810. [Google Scholar] [CrossRef]
- Abruzzo, P.M.; Panisi, C.; Marini, M. The Alteration of Chloride Homeostasis/GABAergic Signaling in Brain Disorders: Could Oxidative Stress Play a Role? Antioxidants 2021, 10, 1316. [Google Scholar] [CrossRef]
- Morris, G.; Walker, A.J.; Walder, K.; Berk, M.; Marx, W.; Carvalho, A.F.; Maes, M.; Puri, B.K. Increasing Nrf2 Activity as a Treatment Approach in Neuropsychiatry. Mol. Neurobiol. 2021, 58, 2158–2182. [Google Scholar] [CrossRef]
- Juchnowicz, D.; Dzikowski, M.; Rog, J.; Waszkiewicz, N.; Zalewska, A.; Maciejczyk, M.; Karakula-Juchnowicz, H. Oxidative Stress Biomarkers as a Predictor of Stage Illness and Clinical Course of Schizophrenia. Front. Psychiatry 2021, 12, 728986. [Google Scholar] [CrossRef]
- Lafeuille, M.H.; Dean, J.; Fastenau, J.; Panish, J.; Olson, W.; Markowitz, M.; Duh, M.S.; Lefebvre, P. Burden of schizophrenia on selected comorbidity costs. Expert Rev. Pharm. Outcomes Res. 2014, 14, 259–267. [Google Scholar] [CrossRef]
- Mizuki, Y.; Sakamoto, S.; Okahisa, Y.; Yada, Y.; Hashimoto, N.; Takaki, M.; Yamada, N. Mechanisms Underlying the Comorbidity of Schizophrenia and Type 2 Diabetes Mellitus. Int. J. Neuropsychopharmacol. 2021, 24, 367–382. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Jin, D.; Palmer, N.; Fox, K.; Kohane, I.S.; Smoller, J.W.; Yu, K.H. Large-scale real-world data analysis identifies comorbidity patterns in schizophrenia. Transl. Psychiatry 2022, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Tanaka, A.; Kishi, T.; Li, Y.; Matsunaga, M.; Tanihara, S.; Iwata, N.; Ota, A. Recent findings on subjective well-being and physical, psychiatric, and social comorbidities in individuals with schizophrenia: A literature review. Neuropsychopharmacol. Rep. 2022, 42, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Solmi, M.; Veronese, N.; Bortolato, B.; Rosson, S.; Santonastaso, P.; Thapa-Chhetri, N.; Fornaro, M.; Gallicchio, D.; Collantoni, E.; et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: A large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry 2017, 16, 163–180. [Google Scholar] [CrossRef] [Green Version]
- Hennekens, C.H.; Hennekens, A.R.; Hollar, D.; Casey, D.E. Schizophrenia and increased risks of cardiovascular disease. Am. Heart J. 2005, 150, 1115–1121. [Google Scholar] [CrossRef]
- Rossom, R.C.; Hooker, S.A.; O’Connor, P.J.; Crain, A.L.; Sperl-Hillen, J.M. Cardiovascular Risk for Patients with and without Schizophrenia, Schizoaffective Disorder, or Bipolar Disorder. J. Am. Heart Assoc. 2022, 11, e021444. [Google Scholar] [CrossRef]
- Nielsen, R.E.; Banner, J.; Jensen, S.E. Cardiovascular disease in patients with severe mental illness. Nat. Rev. Cardiol. 2021, 18, 136–145. [Google Scholar] [CrossRef]
- Marche, J.C.; Bannay, A.; Baillot, S.; Dauriac-Le Masson, V.; Leveque, P.; Schmitt, C.; Laprevote, V.; Schwan, R.; Dobre, D. Prevalence of severe cardiovascular disease in patients with schizophrenia. Encephale 2022, 48, 125–131. [Google Scholar] [CrossRef]
- Fraguas, D.; Diaz-Caneja, C.M.; Ayora, M.; Hernandez-Alvarez, F.; Rodriguez-Quiroga, A.; Recio, S.; Leza, J.C.; Arango, C. Oxidative Stress and Inflammation in First-Episode Psychosis: A Systematic Review and Meta-analysis. Schizophr. Bull. 2019, 45, 742–751. [Google Scholar] [CrossRef]
- Panda, P.; Verma, H.K.; Lakkakula, S.; Merchant, N.; Kadir, F.; Rahman, S.; Jeffree, M.S.; Lakkakula, B.; Rao, P.V. Biomarkers of Oxidative Stress Tethered to Cardiovascular Diseases. Oxidative Med. Cell. Longev. 2022, 2022, 9154295. [Google Scholar] [CrossRef]
- Caruso, G.; Grasso, M.; Fidilio, A.; Tascedda, F.; Drago, F.; Caraci, F. Antioxidant Properties of Second-Generation Antipsychotics: Focus on Microglia. Pharmaceuticals 2020, 13, 457. [Google Scholar] [CrossRef] [PubMed]
- Dietrich-Muszalska, A.; Kolodziejczyk-Czepas, J.; Nowak, P. Comparative Study of the Effects of Atypical Antipsychotic Drugs on Plasma and Urine Biomarkers of Oxidative Stress in Schizophrenic Patients. Neuropsychiatr. Dis. Treat. 2021, 17, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Mangoni, A.A. A Systematic Review and Meta-Analysis of the Effect of Statins on Glutathione Peroxidase, Superoxide Dismutase, and Catalase. Antioxidants 2021, 10, 1841. [Google Scholar] [CrossRef]
- Zinellu, A.; Paliogiannis, P.; Usai, M.F.; Carru, C.; Mangoni, A.A. Effect of statin treatment on circulating malondialdehyde concentrations: A systematic review and meta-analysis. Ther. Adv. Chronic Dis. 2019, 10, 2040622319862714. [Google Scholar] [CrossRef]
- Zinellu, A.; Sotgia, S.; Mangoni, A.A.; Sanna, M.; Satta, A.E.; Carru, C. Impact of cholesterol lowering treatment on plasma kynurenine and tryptophan concentrations in chronic kidney disease: Relationship with oxidative stress improvement. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Mackness, M.; Mackness, B. Human paraoxonase-1 (PON1): Gene structure and expression, promiscuous activities and multiple physiological roles. Gene 2015, 567, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Mackness, B.; Durrington, P.N.; Mackness, M.I. Human serum paraoxonase. Gen. Pharmacol. Vasc. Syst. 1998, 31, 329–336. [Google Scholar] [CrossRef]
- Deng, S.; Xu, Y.; Zheng, L. HDL Structure. Adv. Exp. Med. Biol. 2022, 1377, 1–11. [Google Scholar] [CrossRef]
- Aviram, M.; Rosenblat, M. Paraoxonases 1, 2, and 3, oxidative stress, and macrophage foam cell formation during atherosclerosis development. Free. Radic. Biol. Med. 2004, 37, 1304–1316. [Google Scholar] [CrossRef]
- Reddy, S.T.; Wadleigh, D.J.; Grijalva, V.; Ng, C.; Hama, S.; Gangopadhyay, A.; Shih, D.M.; Lusis, A.J.; Navab, M.; Fogelman, A.M. Human paraoxonase-3 is an HDL-associated enzyme with biological activity similar to paraoxonase-1 protein but is not regulated by oxidized lipids. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 542–547. [Google Scholar] [CrossRef] [Green Version]
- Mu, X.; Yi, X.; Xiao, S.; Wang, C.; Chen, G.; Li, Y. Substrates for Paraoxonase. Curr. Pharm. Des. 2018, 24, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, W.N. Serum esterases. II. An enzyme hydrolysing diethyl p-nitrophenyl phosphate (E600) and its identity with the A-esterase of mammalian sera. Biochem. J. 1953, 53, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Jakubowski, H. Calcium-dependent human serum homocysteine thiolactone hydrolase. A protective mechanism against protein N-homocysteinylation. J. Biol. Chem. 2000, 275, 3957–3962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthukrishnan, S.; Shete, V.S.; Sanan, T.T.; Vyas, S.; Oottikkal, S.; Porter, L.M.; Magliery, T.J.; Hadad, C.M. Mechanistic Insights into the Hydrolysis of Organophosphorus Compounds by Paraoxonase-1: Exploring the Limits of Substrate Tolerance in a Promiscuous Enzyme. J. Phys. Org. Chem. 2012, 25, 1247–1260. [Google Scholar] [CrossRef] [Green Version]
- Zinellu, A.; Fois, A.G.; Sotgia, S.; Zinellu, E.; Bifulco, F.; Pintus, G.; Mangoni, A.A.; Carru, C.; Pirina, P. Plasma protein thiols: An early marker of oxidative stress in asthma and chronic obstructive pulmonary disease. Eur. J. Clin. Investig. 2016, 46, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, A.; Fois, A.G.; Sotgia, S.; Sotgiu, E.; Zinellu, E.; Bifulco, F.; Mangoni, A.A.; Pirina, P.; Carru, C. Arginines Plasma Concentration and Oxidative Stress in Mild to Moderate COPD. PLoS ONE 2016, 11, e0160237. [Google Scholar] [CrossRef] [Green Version]
- Erre, G.L.; Bassu, S.; Giordo, R.; Mangoni, A.A.; Carru, C.; Pintus, G.; Zinellu, A. Association between Paraoxonase/Arylesterase Activity of Serum PON-1 Enzyme and Rheumatoid Arthritis: A Systematic Review and Meta-Analysis. Antioxidants 2022, 11, 2317. [Google Scholar] [CrossRef]
- Pau, M.C.; Zinellu, A.; Zinellu, E.; Pintus, G.; Carru, C.; Fois, A.G.; Mangoni, A.A.; Pirina, P. Paraoxonase-1 Concentrations in Obstructive Sleep Apnoea: A Systematic Review and Meta-Analysis. Antioxidants 2022, 11, 766. [Google Scholar] [CrossRef]
- Bassu, S.; Mangoni, A.A.; Argiolas, D.; Carru, C.; Pirina, P.; Fois, A.G.; Zinellu, A. A systematic review and meta-analysis of paraoxonase-1 activity in asthma. Clin. Exp. Med. 2022. [Google Scholar] [CrossRef]
- Bassu, S.; Mangoni, A.A.; Satta, R.; Argiolas, D.; Carru, C.; Zinellu, A. Paraoxonase and arylesterase activity of serum PON-1 enzyme in psoriatic patients: A systematic review and meta-analysis. Clin. Exp. Med. 2023, 23, 301–311. [Google Scholar] [CrossRef]
- Bassu, S.; Zinellu, A.; Sotgia, S.; Mangoni, A.A.; Floris, A.; Farina, G.; Passiu, G.; Carru, C.; Erre, G.L. Oxidative Stress Biomarkers and Peripheral Endothelial Dysfunction in Rheumatoid Arthritis: A Monocentric Cross-Sectional Case-Control Study. Molecules 2020, 25, 3855. [Google Scholar] [CrossRef] [PubMed]
- Durrington, P.N.; Bashir, B.; Soran, H. Paraoxonase 1 and atherosclerosis. Front. Cardiovasc. Med. 2023, 10, 1065967. [Google Scholar] [CrossRef]
- Navab, M.; Anantharamaiah, G.M.; Reddy, S.T.; Van Lenten, B.J.; Ansell, B.J.; Fogelman, A.M. Mechanisms of disease: Proatherogenic HDL—An evolving field. Nat. Clin. Pract. Endocrinol. Metab. 2006, 2, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Fisher, E.A.; Feig, J.E.; Hewing, B.; Hazen, S.L.; Smith, J.D. High-density lipoprotein function, dysfunction, and reverse cholesterol transport. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2813–2820. [Google Scholar] [CrossRef] [Green Version]
- Pirillo, A.; Catapano, A.L.; Norata, G.D. Biological Consequences of Dysfunctional HDL. Curr. Med. Chem. 2019, 26, 1644–1664. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, G.; Fasciolo, G.; Tomajoli, M.T.M.; Carlucci, A.; Ascione, E.; Salvatore, A. Effects of superoxide anion attack on the lipoprotein HDL. Mol. Cell. Biochem. 2023, 478, 1059–1066. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Bakker, S.J.; James, R.W.; Dullaart, R.P. Serum paraoxonase-1 activity and risk of incident cardiovascular disease: The PREVEND study and meta-analysis of prospective population studies. Atherosclerosis 2016, 245, 143–154. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Systematic reviews of etiology and risk. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; Johanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Balshem, H.; Helfand, M.; Schunemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Tobias, A. Assessing the influence of a single study in the meta-analysis estimate. Stata Tech. Bull. 1999, 47, 15–17. [Google Scholar]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Sarandol, A.; Kirli, S.; Akkaya, C.; Ocak, N.; Eroz, E.; Sarandol, E. Coronary artery disease risk factors in patients with schizophrenia: Effects of short term antipsychotic treatment. J. Psychopharmacol. 2007, 21, 857–863. [Google Scholar] [CrossRef]
- Yegin, A.; Ay, N.; Aydin, O.; Yargici, N.; Eren, E.; Yilmaz, N. Increased Oxidant Stress and Inflammation in Patients with Chronic Schizophrenia. Int. J. Clin. Med. 2012, 3, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Unsal, C.; Albayrak, Y.; Albayrak, N.; Kuloglu, M.; Hashimoto, K. Reduced serum paraoxonase 1 (PON1) activity in patients with schizophrenia treated with olanzapine but not quetiapine. Neuropsychiatr. Dis. Treat. 2013, 9, 1545–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilca, M.; Piriu, G.; Gaman, L.; Delia, C.; Iosif, L.; Atanasiu, V.; Stoian, I. A study of antioxidant activity in patients with schizophrenia taking atypical antipsychotics. Psychopharmacology 2014, 231, 4703–4710. [Google Scholar] [CrossRef] [PubMed]
- Mabrouk, H.; Mechria, H.; Mechri, A.; Azizi, I.; Neffati, F.; Douki, W.; Gaha, L.; Najjar, M.F. Paraoxonase 1 activity and lipid profile in schizophrenic patients. Asian J. Psychiatry 2014, 9, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Brinholi, F.F.; Noto, C.; Maes, M.; Bonifacio, K.L.; Brietzke, E.; Ota, V.K.; Gadelha, A.; Cordeiro, Q.; Belangero, S.I.; Bressan, R.A.; et al. Lowered paraoxonase 1 (PON1) activity is associated with increased cytokine levels in drug naive first episode psychosis. Schizophr. Res. 2015, 166, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Hussein, O.; Izikson, L.; Bathish, Y.; Dabur, E.; Hanna, A.; Zidan, J. Anti-atherogenic properties of high-density lipoproteins in psychiatric patients before and after two months of atypical anti-psychotic therapy. J. Psychopharmacol. 2015, 29, 1262–1270. [Google Scholar] [CrossRef]
- Sarandol, A.; Sarandol, E.; Acikgoz, H.E.; Eker, S.S.; Akkaya, C.; Dirican, M. First-episode psychosis is associated with oxidative stress: Effects of short-term antipsychotic treatment. Psychiatry Clin. Neurosci. 2015, 69, 699–707. [Google Scholar] [CrossRef]
- Gunes, M.; Camkurt, M.A.; Bulut, M.; Demir, S.; Ibiloglu, A.O.; Kaya, M.C.; Atli, A.; Kaplan, I.; Sir, A. Evaluation of Paraoxonase, Arylesterase and Malondialdehyde Levels in Schizophrenia Patients Taking Typical, Atypical and Combined Antipsychotic Treatment. Clin. Psychopharmacol. Neurosci. 2016, 14, 345–350. [Google Scholar] [CrossRef] [Green Version]
- Kulaksizoglu, B.; Kulaksizoglu, S. Relationship between neutrophil/lymphocyte ratio with oxidative stress and psychopathology in patients with schizophrenia. Neuropsychiatr. Dis. Treat. 2016, 12, 1999–2005. [Google Scholar] [CrossRef] [Green Version]
- Atagun, M.I.; Tunc, S.; Alisik, M.; Erel, O. Phenotypic Variants of Paraoxonase Q192R in Bipolar Disorder, Depression and Schizophrenia. Turk. J. Psychiatry 2017, 29, 79–86. [Google Scholar] [CrossRef]
- Boll, K.M.; Noto, C.; Bonifacio, K.L.; Bortolasci, C.C.; Gadelha, A.; Bressan, R.A.; Barbosa, D.S.; Maes, M.; Moreira, E.G. Oxidative and nitrosative stress biomarkers in chronic schizophrenia. Psychiatry Res. 2017, 253, 43–48. [Google Scholar] [CrossRef]
- Paval, D.; Nemes, B.; Rusu, R.L.; Dronca, E. Genotype-phenotype Analysis of Paraoxonase 1 in Schizophrenic Patients Treated with Atypical Antipsychotics. Clin. Psychopharmacol. Neurosci. 2018, 16, 32–38. [Google Scholar] [CrossRef] [Green Version]
- Solberg, D.K.; Refsum, H.; Andreassen, O.A.; Bentsen, H. A five-year follow-up study of antioxidants, oxidative stress and polyunsaturated fatty acids in schizophrenia. Acta Neuropsychiatr. 2019, 31, 202–212. [Google Scholar] [CrossRef]
- Frijhoff, J.; Winyard, P.G.; Zarkovic, N.; Davies, S.S.; Stocker, R.; Cheng, D.; Knight, A.R.; Taylor, E.L.; Oettrich, J.; Ruskovska, T.; et al. Clinical Relevance of Biomarkers of Oxidative Stress. Antioxid. Redox Signal. 2015, 23, 1144–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrocco, I.; Altieri, F.; Peluso, I. Measurement and Clinical Significance of Biomarkers of Oxidative Stress in Humans. Oxidative Med. Cell. Longev. 2017, 2017, 6501046. [Google Scholar] [CrossRef] [PubMed]
- Sohal, R.S.; Orr, W.C. The redox stress hypothesis of aging. Free. Radic. Biol. Med. 2012, 52, 539–555. [Google Scholar] [CrossRef] [Green Version]
- Kander, M.C.; Cui, Y.; Liu, Z. Gender difference in oxidative stress: A new look at the mechanisms for cardiovascular diseases. J. Cell. Mol. Med. 2017, 21, 1024–1032. [Google Scholar] [CrossRef] [PubMed]
- Grattagliano, I.; Palmieri, V.O.; Portincasa, P.; Moschetta, A.; Palasciano, G. Oxidative stress-induced risk factors associated with the metabolic syndrome: A unifying hypothesis. J. Nutr. Biochem. 2008, 19, 491–504. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Dietrich, M.; Norkus, E.P.; Morrow, J.D.; Hudes, M.; Caan, B.; Packer, L. Factors associated with oxidative stress in human populations. Am. J. Epidemiol. 2002, 156, 274–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weverling-Rijnsburger, A.W.; Jonkers, I.J.; van Exel, E.; Gussekloo, J.; Westendorp, R.G. High-density vs low-density lipoprotein cholesterol as the risk factor for coronary artery disease and stroke in old age. Arch. Intern. Med. 2003, 163, 1549–1554. [Google Scholar] [CrossRef] [Green Version]
- Neumann, J.T.; Thao, L.T.P.; Callander, E.; Chowdhury, E.; Williamson, J.D.; Nelson, M.R.; Donnan, G.; Woods, R.L.; Reid, C.M.; Poppe, K.K.; et al. Cardiovascular risk prediction in healthy older people. Geroscience 2022, 44, 403–413. [Google Scholar] [CrossRef] [PubMed]
- Lambert, T.J.; Velakoulis, D.; Pantelis, C. Medical comorbidity in schizophrenia. Med. J. Aust. 2003, 178, S67–S70. [Google Scholar] [CrossRef] [PubMed]
- Morris, G.; Puri, B.K.; Bortolasci, C.C.; Carvalho, A.; Berk, M.; Walder, K.; Moreira, E.G.; Maes, M. The role of high-density lipoprotein cholesterol, apolipoprotein A and paraoxonase-1 in the pathophysiology of neuroprogressive disorders. Neurosci. Biobehav. Rev. 2021, 125, 244–263. [Google Scholar] [CrossRef] [PubMed]
- Sankaranarayanan, A.; Jenkins, Z.; Castle, D.; Andrade, C. Serum lipids and suicidality among patients with schizophrenia. Schizophr. Res. 2020, 215, 479–481. [Google Scholar] [CrossRef]
- Nandeesha, H.; Keshri, N.; Rajappa, M.; Menon, V. Association of hyperglycaemia and hyperlipidaemia with cognitive dysfunction in schizophrenia spectrum disorder. Arch. Physiol. Biochem. 2023, 129, 497–504. [Google Scholar] [CrossRef]
- Huang, T.L.; Chen, J.F. Serum lipid profiles and schizophrenia: Effects of conventional or atypical antipsychotic drugs in Taiwan. Schizophr. Res. 2005, 80, 55–59. [Google Scholar] [CrossRef]
- Pillinger, T.; McCutcheon, R.A.; Vano, L.; Mizuno, Y.; Arumuham, A.; Hindley, G.; Beck, K.; Natesan, S.; Efthimiou, O.; Cipriani, A.; et al. Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: A systematic review and network meta-analysis. Lancet Psychiatry 2020, 7, 64–77. [Google Scholar] [CrossRef]
- Lepping, P.; Delieu, J.; Mellor, R.; Williams, J.H.; Hudson, P.R.; Hunter-Lavin, C. Antipsychotic medication and oxidative cell stress: A systematic review. J. Clin. Psychiatry 2011, 72, 273–285. [Google Scholar] [CrossRef]
- Chen, A.T.; Nasrallah, H.A. Neuroprotective effects of the second generation antipsychotics. Schizophr. Res. 2019, 208, 1–7. [Google Scholar] [CrossRef]
- Furlong, C.E.; Cole, T.B.; Jarvik, G.P.; Costa, L.G. Pharmacogenomic considerations of the paraoxonase polymorphisms. Pharmacogenomics 2002, 3, 341–348. [Google Scholar] [CrossRef]
- Li, H.L.; Liu, D.P.; Liang, C.C. Paraoxonase gene polymorphisms, oxidative stress, and diseases. J. Mol. Med. 2003, 81, 766–779. [Google Scholar] [CrossRef] [PubMed]
- Moreira, E.G.; Boll, K.M.; Correia, D.G.; Soares, J.F.; Rigobello, C.; Maes, M. Why Should Psychiatrists and Neuroscientists Worry about Paraoxonase 1? Curr. Neuropharmacol. 2019, 17, 1004–1020. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, A.K.; Maes, M.; Supasitthumrong, T.; Maes, A.; Michelin, A.P.; de Oliveira Semeao, L.; de Lima Pedrao, J.V.; Moreira, E.G.; Kanchanatawan, B.; Barbosa, D.S. Deficit schizophrenia and its features are associated with PON1 Q192R genotypes and lowered paraoxonase 1 (PON1) enzymatic activity: Effects on bacterial translocation. CNS Spectr. 2021, 26, 406–415. [Google Scholar] [CrossRef]
- De Hert, M.; Detraux, J.; van Winkel, R.; Yu, W.; Correll, C.U. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat. Rev. Endocrinol. 2011, 8, 114–126. [Google Scholar] [CrossRef]
- Correll, C.U.; Detraux, J.; De Lepeleire, J.; De Hert, M. Effects of antipsychotics, antidepressants and mood stabilizers on risk for physical diseases in people with schizophrenia, depression and bipolar disorder. World Psychiatry 2015, 14, 119–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotella, F.; Cassioli, E.; Calderani, E.; Lazzeretti, L.; Ragghianti, B.; Ricca, V.; Mannucci, E. Long-term metabolic and cardiovascular effects of antipsychotic drugs. A meta-analysis of randomized controlled trials. Eur. Neuropsychopharmacol. 2020, 32, 56–65. [Google Scholar] [CrossRef]
- Taipale, H.; Tanskanen, A.; Mehtala, J.; Vattulainen, P.; Correll, C.U.; Tiihonen, J. 20-year follow-up study of physical morbidity and mortality in relationship to antipsychotic treatment in a nationwide cohort of 62,250 patients with schizophrenia (FIN20). World Psychiatry 2020, 19, 61–68. [Google Scholar] [CrossRef] [Green Version]
- Chung, K.H.; Chen, P.H.; Kuo, C.J.; Tsai, S.Y.; Huang, S.H.; Wu, W.C. Risk factors for early circulatory mortality in patients with schizophrenia. Psychiatry Res. 2018, 267, 7–11. [Google Scholar] [CrossRef]
- Davis, K.A.; Crow, J.A.; Chambers, H.W.; Meek, E.C.; Chambers, J.E. Racial differences in paraoxonase-1 (PON1): A factor in the health of southerners? Environ. Health Perspect. 2009, 117, 1226–1231. [Google Scholar] [CrossRef] [Green Version]
- Woudberg, N.J.; Goedecke, J.H.; Blackhurst, D.; Frias, M.; James, R.; Opie, L.H.; Lecour, S. Association between ethnicity and obesity with high-density lipoprotein (HDL) function and subclass distribution. Lipids Health Dis. 2016, 15, 92. [Google Scholar] [CrossRef] [Green Version]
- Thyagarajan, B.; Jacobs, D.R., Jr.; Carr, J.J.; Alozie, O.; Steffes, M.W.; Kailash, P.; Hayes, J.H.; Gross, M.D. Factors associated with paraoxonase genotypes and activity in a diverse, young, healthy population: The Coronary Artery Risk Development in Young Adults (CARDIA) study. Clin. Chem. 2008, 54, 738–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
PRISMA 2020 flow diagram.

Figure 2.
Paraoxonase activity in patients with schizophrenia and healthy controls. (a) and (b) refer to different arms of the same study [61,62,63,64,65,68,69,70,71].

Figure 3.
Sensitivity analysis of the association between paraoxonase activity and schizophrenia. (a) and (b) refer to different arms of the same study [61,62,63,64,65,68,69,70,71].

Figure 4.
Funnel plot of paraoxonase activity and schizophrenia after “trimming-and-filling”.

Figure 5.
Association between the effect size of paraoxonase activity and patient/control age ratio (A), and cumulative meta-analysis of paraoxonase activity based on patient/control age ratio (B). (a) and (b) refer to different arms of the same study [61,62,63,64,65,68,69,70,71].

Figure 6.
Association between the effect size of paraoxonase activity and patient/control HDL–cholesterol ratio (A), and cumulative meta-analysis of paraoxonase activity based on patient/control HDL–cholesterol ratio (B). (a) and (b) refer to different arms of the same study [61,62,63,64,65,68,71].

Figure 7.
Paraoxonase activity in schizophrenic patients and healthy controls according to study country. (a) and (b) refer to different arms of the same study [61,62,63,64,65,68,69,70,71].

Figure 8.
Paraoxonase activity in schizophrenic patients and healthy controls according to pharmacological treatment of schizophrenia. (a) and (b) refer to different arms of the same study [61,62,63,64,65,68,69,70,71].

Figure 9.
Arylesterase activity in patients with schizophrenia and healthy controls. (a) and (b) refer to different arms of the same study [61,62,64,66,67,68,69,71,72,73].

Figure 10.
Sensitivity analysis of the association between arylesterase activity and schizophrenia. (a) and (b) refer to different arms of the same study [61,62,64,66,67,68,69,71,72,73].

Figure 11.
Funnel plot of the association between arylesterase activity and schizophrenia after “trimming-and-filling”.
Figure 11.
Funnel plot of the association between arylesterase activity and schizophrenia after “trimming-and-filling”.

Figure 12.
Association between the effect size of arylesterase activity and patient/control age ratio (A), and cumulative meta-analysis of arylesterase activity based on patient/control age ratio (B). (a) and (b) refer to different arms of the same study [61,62,64,66,68,69,71,72,73].

Figure 13.
Association between the effect size of arylesterase activity and patient/control body mass index ratio (A), and cumulative meta-analysis of arylesterase activity based on patient/control body mass index ratio (B). (a) and (b) refer to different arms of the same study [61,62,64,68,69].

Figure 14.
Association between the effect size of arylesterase activity and patient/control HDL–cholesterol ratio (A), and cumulative meta-analysis of arylesterase activity based on patient/control HDL–cholesterol ratio (B). (a) and (b) refer to different arms of the same study [61,62,64,67,68,71].

Figure 15.
Arylesterase activity in schizophrenic patients and healthy controls according to study country. (a) and (b) refer to different arms of the same study [61,62,64,66,67,68,69,71,72,73].

Figure 16.
Arylesterase activity in schizophrenic patients and healthy controls according to pharmacological treatment of schizophrenia. (a) and (b) refer to different arms of the same study [61,62,64,66,67,68,69,71,72,73].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Characteristics of the selected studies.
| Controls | Patients with Schizophrenia | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | n | Age (Years) | M/F | PON Mean ± SD (U/L) | ARE Mean ± SD (kU/L) | HDL Mean (mg/dL or mmol/L) | n | Age (Years) | M/F | PON Mean ± SD (U/L) | ARE Mean ± SD (kU/L) | HDL Mean (mg/dL or mmol/L) |
| Sarandol A. et al. (a), 2007, Turkey [61] | 35 | 34 | 17/18 | 246 ± 90 | 98 ± 37 | 1.2 | 40 | 35 | 18/22 | 199 ± 95 | 78 ± 40 | 1.2 |
| Sarandol A. et al. (b) 2007, Turkey [61] | 35 | 34 | NR | 246 ± 90 | 98 ± 37 | 1.2 | 36 | 35 | NR | 226 ± 121 | 82 ± 40 | 1.2 |
| Yegin A. et al., 2012, Turkey [62] | 30 | 38 | 30/0 | 93.7 ± 44.5 | 164 ± 66 | 45.9 | 30 | 37 | 30/0 | 99.9 ± 61.6 | 150 ± 59 | 41.5 |
| Unsal C. et al. (a), 2013, Turkey [63] | 32 | 35 | 21/11 | 222 ± 91 | NR | 40 | 29 | 42 | 14/15 | 220 ± 93 | NR | 39.5 |
| Unsal C. et al. (b), 2013, Turkey [63] | 32 | 35 | 21/11 | 222 ± 91 | NR | 40 | 35 | 38 | 15/20 | 131 ± 50 | NR | 36 |
| Gilca M. et al. (a), 2014, Romania [64] | 16 | 62 | NR | 84.0 ± 1.8 | 107.4 ± 9.6 | 37.2 | 22 | 47 | NR | 87.5 ± 3.9 | 121.0 ± 14.2 | 41.3 |
| Gilca M. et al. (b), 2014, Romania [64] | 16 | 62 | NR | 84.0 ± 1.8 | 107.4 ± 9.6 | 37.2 | 44 | 38 | NR | 90.6 ± 2.8 | 123.6 ± 12.7 | 42.8 |
| Mabrouk H. et al., 2014, Tunisia [65] | 119 | 41 | 64/55 | 290 ± 171 | NR | 1.35 | 140 | 37 | 116/24 | 239 ± 176 | NR | 0.91 |
| Brinholi F.F. et al., 2015, Brazil [66] | 61 | 26 | 32/29 | NR | 237.8 ± 58.4 | NR | 51 | 25 | 36/15 | NR | 212.2 ± 56.2 | NR |
| Hussein O. et al. (a), 2015, Israel [67] | 10 | NR | 13/6 | NR | 77.3 ± 37.7 | 1.34 | 19 | 35 | 4/6 | NR | 72 ± 22.2 | 1.2 |
| Hussein O. et al. (a), 2015, Israel [67] | 10 | NR | NR | NR | 77.3 ± 37.7 | 1.34 | 15 | NR | NR | NR | 67.1 ± 22.5 | 1.2 |
| Sarandol A. et al. (a), 2015, Turkey [68] | 25 | 24 | 10/15 | 186 ± 75 | 89.7 ± 37.2 | 48 | 26 | 26 | 10/16 | 198 ± 107 | 64.4 ± 36.7 | 45 |
| Sarandol A. et al. (b), 2015, Turkey [68] | 25 | 24 | 10/15 | 186 ± 75 | 89.7 ± 37.2 | 48 | 26 | 26 | 10/16 | 209 ± 107 | 59.9 ± 29.3 | 45 |
| Gunes M. et al., 2016, Turkey [69] | 43 | 35 | 36/7 | 66.9 ± 5.2 | 114.5 ± 24.9 | NR | 41 | 35 | 35/6 | 68.6 ± 3.9 | 135 ± 24 | NR |
| Kulaksizoglu B. et al., 2016, Turkey [70] | 61 | 41 | 33/28 | 36.1 ± 28.2 | NR | NR | 64 | 40 | 36/28 | 38.7 ± 21.0 | NR | NR |
| Boll K.M. et al., 2017, Brazil [72] | 118 | 35 | 74/44 | NR | 178.6 ± 58.6 | NR | 125 | 36 | 85/40 | NR | 181.6 ± 47.7 | NR |
| Atagun M.I. et al., 2018, Turkey [71] | 43 | 32 | 20/23 | 186 ± 75 | 215 ± 52 | 46.63 | 37 | 35 | 19/18 | 154 ± 93 | 202 ± 48 | 43.27 |
| Paval D. et al., 2018, Romania [73] | 34 | 40 | 12/22 | NR | 112 ± 51 | 1.21 | 60 | 34 | 42/18 | NR | 97 ± 26 | 1.17 |
Legend: PON, paraoxonase-1; ARE, arylesterase; HDL, high-density lipoprotein cholesterol; M, male; F, female; NR, not reported. (a) and (b) refer to different arms of the same study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zinellu, A.; Sedda, S.; Mangoni, A.A. Paraoxonase/Arylesterase Activity of Serum Paraoxonase-1 and Schizophrenia: A Systematic Review and Meta-Analysis. Antioxidants 2023, 12, 1484. https://doi.org/10.3390/antiox12081484
AMA Style
Zinellu A, Sedda S, Mangoni AA. Paraoxonase/Arylesterase Activity of Serum Paraoxonase-1 and Schizophrenia: A Systematic Review and Meta-Analysis. Antioxidants. 2023; 12(8):1484. https://doi.org/10.3390/antiox12081484
Chicago/Turabian StyleZinellu, Angelo, Stefania Sedda, and Arduino A. Mangoni. 2023. "Paraoxonase/Arylesterase Activity of Serum Paraoxonase-1 and Schizophrenia: A Systematic Review and Meta-Analysis" Antioxidants 12, no. 8: 1484. https://doi.org/10.3390/antiox12081484
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.