
Effect of Dietary Phenolic Compounds on Incidence of Type 2 Diabetes in the “Seguimiento Universidad de Navarra” (SUN) Cohort
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
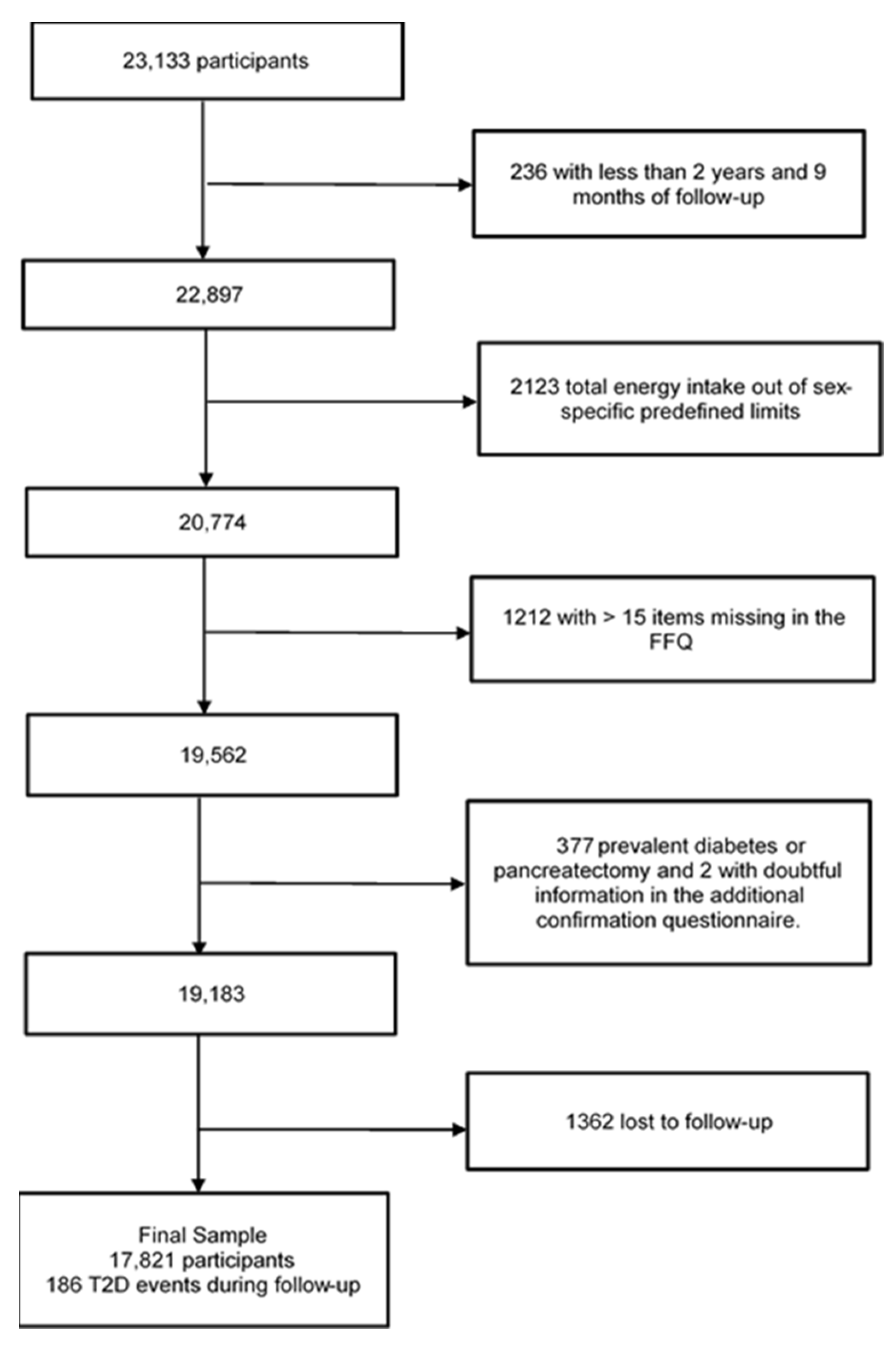
2.1. Study Population
2.2. Assessment of Food and PC Intake
2.3. Outcome Assessment
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diabetes. Available online: https://www.who.int/health-topics/diabetes#tab=tab_1 (accessed on 13 December 2022).
- Narayan, K.M.V.; Gregg, E.W.; Fagot-Campagna, A.; Engelgau, M.M.; Vinicor, F. Diabetes—A common, growing, serious, costly, and potentially preventable public health problem. Diabetes Res. Clin. Pract. 2000, 50 (Suppl. S2), S77–S84. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Martinez-González, M.Á.; Bulló, M.; Ros, E. The role of diet in the prevention of type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2011, 21, B32–B48. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 3.Prevention or Delay of Type 2 Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care 2021, 44 (Suppl. S1), S34–S39. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Chaimani, A.; Hoffmann, G.; Schwedhelm, C.; Boeing, H. A network meta-analysis on the comparative efficacy of different dietary approaches on glycaemic control in patients with type 2 diabetes mellitus. Eur. J. Epidemiol. 2018, 33, 157–170. [Google Scholar] [CrossRef] [Green Version]
- Sainsbury, E.; Kizirian, N.V.; Partridge, S.R.; Gill, T.; Colagiuri, S.; Gibson, A.A. Effect of dietary carbohydrate restriction on glycemic control in adults with diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2018, 139, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E. Benefits of the Mediterranean Diet: Insights From the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378. [Google Scholar] [CrossRef]
- McMacken, M.; Shah, S. A plant-based diet for the prevention and treatment of type 2 diabetes. J. Geriatr. Cardiol. 2017, 14, 342. [Google Scholar] [CrossRef]
- Dini, I.; Grumetto, L. Recent Advances in Natural Polyphenol Research. Molecules 2022, 27, 8777. [Google Scholar] [CrossRef]
- Kabera, J.N.; Semana, E.; Mussa, A.R.; He, X. Plant secondary metabolites: Biosynthesis, classification, function and pharmacological properties. J. Pharm. Pharmacol. 2014, 2, 377–392. Available online: https://www.academia.edu/download/59009920/1-JPP201402100120190423-15279-1jxae74.pdf (accessed on 19 December 2022).
- Tecchio Borsoi, F.; Angélica Neri-Numa, I.; Queiroz de Oliveira, W.; Fernandes de Araújo, F.; Maria Pastore, G. Dietary polyphenols and their relationship to the modulation of non-communicable chronic diseases and epigenetic mechanisms: A mini-review. Food Chem. Mol. Sci. 2022, 6, 100155. [Google Scholar] [CrossRef] [PubMed]
- Fraga, C.G.; Croft, K.D.; Kennedy, D.O.; Tomás-Barberán, F.A. The effects of polyphenols and other bioactives on human health. Food Funct. 2019, 10, 514–528. [Google Scholar] [CrossRef] [Green Version]
- Durazzo, A.; Lucarini, M.; Souto, E.B.; Cicala, C.; Caiazzo, E.; Izzo, A.A.; Novellino, E.; Santini, A. Polyphenols: A concise overview on the chemistry, occurrence, and human health. Phyther. Res. 2019, 33, 2221–2243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Lorenzo, C.; Colombo, F.; Biella, S.; Stockley, C.; Restani, P. Polyphenols and Human Health: The Role of Bioavailability. Nutrients 2021, 13, 273. [Google Scholar] [CrossRef] [PubMed]
- Sack, M.N.; Fyhrquist, F.Y.; Saijonmaa, O.J.; Fuster, V.; Kovacic, J.C. Basic Biology of Oxidative Stress and the Cardiovascular System: Part 1 of a 3-Part Series. J. Am. Coll. Cardiol. 2017, 70, 196–211. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferré, M.; Merino, J.; Sun, Q.; Fitó, M.; Salas-Salvadó, J. Dietary Polyphenols, Mediterranean Diet, Prediabetes, and Type 2 Diabetes: A Narrative Review of the Evidence. Oxid. Med. Cell. Longev. 2017, 2017, 6723931. [Google Scholar] [CrossRef]
- Pandey, K.B.; Rizvi, S.I. Plant polyphenols as dietary antioxidants in human health and disease. Oxid. Med. Cell. Longev. 2009, 2, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Pu, Y.; Xu, Y.; He, X.; Cao, J.; Ma, Y.; Jiang, W. Anti-diabetic and anti-obesity: Efficacy evaluation and exploitation of polyphenols in fruits and vegetables. Food Res. Int. 2022, 157, 111202. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Knaze, V.; Lujan-Barroso, L.; Romieu, I.; Scalbert, A.; Slimani, N.; Hjartåker, A.; Engeset, D.; Skeie, G.; Overvad, K.; et al. Differences in dietary intakes, food sources and determinants of total flavonoids between Mediterranean and non-Mediterranean countries participating in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Br. J. Nutr. 2013, 109, 1498–1507. [Google Scholar] [CrossRef]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Polyphenols and Glycemic Control. Nutrients 2016, 8, 17. [Google Scholar] [CrossRef] [PubMed]
- Carlos, S.; De La Fuente-Arrillaga, C.; Bes-Rastrollo, M.; Razquin, C.; Rico-Campà, A.; Martínez-González, M.A.; Ruiz-Canela, M. Mediterranean diet and health outcomes in the SUN cohort. Nutrients 2018, 10, 439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W. Nutritional Epidemiology; Oxford University Press: Oxford, UK, 2012; Volume 40. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- de la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-Gonzalez, M.A. Reproducibility of an FFQ validated in Spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mataix, J. Tabla de Composición de Alimentos, 5th ed.; Universidad de Granada: Granada, Spain, 2009. [Google Scholar]
- Moreiras, O.; Carbajar, A.; Cabrera, L.; Cuadrado, C. Tabla de Composición de Alimentos, 16th ed.; Pirámide: Madrid, Spain, 2013. [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [Green Version]
- Neveu, V.; Pérez-Jiménez, J.; Vos, F.; Crespy, V.; du Chaffaut, L.; Mennen, L.; Knox, C.; Eisner, R.; Cruz, J.; Wishart, D.; et al. Phenol-Explorer: An online comprehensive database on polyphenol contents in foods. Database 2010, 2010, bap024. [Google Scholar] [CrossRef]
- Pérez-Jiménez, J.; Neveu, V.; Vos, F.; Scalbert, A. Identification of the 100 richest dietary sources of polyphenols: An application of the Phenol-Explorer database. Eur. J. Clin. Nutr. 2010, 64, S112–S120. [Google Scholar] [CrossRef] [Green Version]
- Agencia Española de Seguridad Alimentaria y Nutrición (AESAN). Encuesta Nacional de Ingesta Dietética Española (National Dietary Intake Survey). 2011. Available online: https://docplayer.es/10558027-Enide-presentacion-n-de-enide-2011-encuesta-nacional-de-ingesta-dietetica-tica-espanola-aesan-aesan.html (accessed on 23 March 2022).
- Basu, S.; Yudkin, J.S.; Berkowitz, S.A.; Jawad, M.; Millett, C. Reducing chronic disease through changes in food aid: A microsimulation of nutrition and cardiometabolic disease among Palestinian refugees in the Middle East. PLoS Med. 2018, 15, e1002700. [Google Scholar] [CrossRef]
- Martínez-González, M.Á.; De La Fuente-Arrillaga, C.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Beunza, J.J.; Vazquez, Z.; Benito, S.; Tortosa, A.; Bes-Rastrollo, M. Adherence to Mediterranean diet and risk of developing diabetes: Prospective cohort study. BMJ 2008, 336, 1348–1351. [Google Scholar] [CrossRef] [Green Version]
- Bes-Rastrollo, M.; Pérez, J.R.; Sanchez-Villegas, A.; Alonso, A.; Martínez-González, M.A. Validation of self-reported weight and body mass index in a cohort of university graduates in Spain. Rev. Esp. Obes. 2005, 3, 352–358. [Google Scholar]
- Martinez-Gonzalez, M.A.; Lopez-Fontana, C.; Varo, J.J.; Sanchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ Follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Barrio-Lopez, M.T.; Bes-Rastrollo, M.; Beunza, J.J.; Fernandez-Montero, A.; Garcia-Lopez, M.; Martinez-Gonzalez, M.A. Validation of metabolic syndrome using medical records in the SUN cohort. BMC Public Health 2011, 11, 867. [Google Scholar] [CrossRef] [Green Version]
- Alonso, A.; Beunza, J.J.; Delgado-Rodríguez, M.; Martínez-González, M.A. Validation of self-reported diagnosis of hypertension in a cohort of university graduates in Spain. BMC Public Health 2005, 5, 94. [Google Scholar] [CrossRef] [Green Version]
- Rojo-Martínez, G.; Valdés, S.; Soriguer, F.; Vendrell, J.; Urrutia, I.; Pérez, V.; Ortega, E.; Ocón, P.; Montanya, E.; Menéndez, E.; et al. Incidence of diabetes mellitus in Spain as results of the nation-wide cohort [email protected] study. Sci. Rep. 2020, 10, 2765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gepner, Y.; Golan, R.; Harman-Boehm, I.; Henkin, Y.; Schwarzfuchs, D.; Shelef, I.; Durst, R.; Kovsan, J.; Bolotin, A.; Leitersdorf, E.; et al. Effects of Initiating Moderate Alcohol Intake on Cardiometabolic Risk in Adults With Type 2 Diabetes: A 2-Year Randomized, Controlled Trial. Ann. Intern. Med. 2015, 163, 569–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Valderas-Martinez, P.; Casas, R.; Arranz, S.; Guillén, M.; Lamuela-Raventos, R.M.; Llorach, R.; Andres-Lacueva, C.; et al. Effects of red wine polyphenols and alcohol on glucose metabolism and the lipid profile: A randomized clinical trial. Clin. Nutr. 2013, 32, 200–206. [Google Scholar] [CrossRef]
- Napoli, R.; Cozzolino, D.; Guardasole, V.; Angelini, V.; Zarra, E.; Matarazzo, M.; Cittadini, A.; Saccà, L.; Torella, R. Red wine consumption improves insulin resistance but not endothelial function in type 2 diabetic patients. Metabolism 2005, 54, 306–313. [Google Scholar] [CrossRef]
- Castilla, P.; Echarri, R.; Dávalos, A.; Cerrato, F.; Ortega, H.; Teruel, J.L.; Lucas, M.F.; Gómez-Coronado, D.; Ortuño, J.; A Lasunción, M. Concentrated red grape juice exerts antioxidant, hypolipidemic, and antiinflammatory effects in both hemodialysis patients and healthy subjects. Am. J. Clin. Nutr. 2006, 84, 252–262. [Google Scholar] [CrossRef] [Green Version]
- Cordain, L.; Melby, C.L.; E Hamamoto, A.; O’Neill, D.; Cornier, M.-A.; A Barakat, H.; Israel, R.G.; O Hill, J. Influence of moderate chronic wine consumption on insulin sensitivity and other correlates of syndrome X in moderately obese women. Metabolism 2000, 49, 1473–1478. [Google Scholar] [CrossRef]
- Beulens, J.W.J.; Van Beers, R.M.; Stolk, R.P.; Schaafsma, G.; Hendriks, H.F.J. The Effect of Moderate Alcohol Consumption on Fat Distribution and Adipocytokines. Obesity 2006, 14, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Hokayem, M.; Blond, E.; Vidal, H.; Lambert, K.; Meugnier, E.; Feillet-Coudray, C.; Coudray, C.; Pesenti, S.; Luyton, C.; Lambert-Porcheron, S.; et al. Grape polyphenols prevent fructose-induced oxidative stress and insulin resistance in first-degree relatives of type 2 diabetic patients. Diabetes Care 2013, 36, 1454–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmers, S.; Konings, E.; Bilet, L.; Houtkooper, R.H.; van de Weijer, T.; Goossens, G.H.; Hoeks, J.; van der Krieken, S.; Ryu, D.; Kersten, S.; et al. Calorie restriction-like effects of 30 days of resveratrol supplementation on energy metabolism and metabolic profile in obese humans. Cell Metab. 2011, 14, 612–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wedick, N.M.; Pan, A.; Cassidy, A.; Rimm, E.B.; Sampson, L.; Rosner, B.; Willett, W.; Hu, F.B.; Sun, Q.; van Dam, R.M. Dietary flavonoid intakes and risk of type 2 diabetes in US men and women. Am. J. Clin. Nutr. 2012, 95, 925–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamora-Ros, R.; Forouhi, N.G.; Sharp, S.J.; González, C.A.; Buijsse, B.; Guevara, M.; van der Schouw, Y.T.; Amiano, P.; Boeing, H.; Bredsdorff, L.; et al. The Association Between Dietary Flavonoid and Lignan Intakes and Incident Type 2 Diabetes in European PopulationsThe EPIC-InterAct study. Diabetes Care 2013, 36, 3961–3970. [Google Scholar] [CrossRef] [Green Version]
- Barre, D.E.; Mizier-Barre, K.A. Lignans’ Potential in Pre and Post-onset Type 2 Diabetes Management. Curr. Diabetes Rev. 2019, 16, 2–11. [Google Scholar] [CrossRef]
- Sun, Q.; Wedick, N.M.; Pan, A.; Townsend, M.K.; Cassidy, A.; Franke, A.A.; Rimm, E.B.; Hu, F.B.; van Dam, R.M. Gut microbiota metabolites of dietary lignans and risk of type 2 diabetes: A prospective investigation in two cohorts of U. S. Women Diabetes Care 2014, 37, 1287–1295. [Google Scholar] [CrossRef] [Green Version]
- Ylönen, K.; Saloranta, C.; Kronberg-Kippilä, C.; Groop, L.; Aro, A.; Virtanen, S.M. Associations of dietary fiber with glucose metabolism in nondiabetic relatives of subjects with type 2 diabetes: The Botnia Dietary Study. Diabetes Care 2003, 26, 1979–1985. [Google Scholar] [CrossRef] [Green Version]
- Shaposhnikov, S.; Hatzold, T.; El Yamani, N.; Stavro, P.M.; Lorenzo, Y.; Dusinska, M.; Reus, A.; Pasman, W.; Collins, A. Coffee and oxidative stress: A human intervention study. Eur. J. Nutr. 2018, 57, 533–544. [Google Scholar] [CrossRef]
- Vinayagam, R.; Jayachandran, M.; Xu, B. Antidiabetic Effects of Simple Phenolic Acids: A Comprehensive Review. Phytother Res. 2016, 30, 184–199. [Google Scholar] [CrossRef]
- De Bock, M.; Derraik, J.G.; Brennan, C.M.; Biggs, J.B.; Morgan, P.E.; Hodgkinson, S.C.; Hofman, P.L.; Cutfield, W.S. Olive (Olea europaea L.) Leaf Polyphenols Improve Insulin Sensitivity in Middle-Aged Overweight Men: A Randomized, Placebo-Controlled, Crossover Trial. PLoS ONE 2013, 8, e57622. [Google Scholar] [CrossRef] [PubMed]
- Bozzetto, L.; Annuzzi, G.; Pacini, G.; Costabile, G.; Vetrani, C.; Vitale, M.; Griffo, E.; Giacco, A.; De Natale, C.; Cocozza, S.; et al. Polyphenol-rich diets improve glucose metabolism in people at high cardiometabolic risk: A controlled randomised intervention trial. Diabetologia 2015, 58, 1551–1560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annuzzi, G.; Bozzetto, L.; Costabile, G.; Giacco, R.; Mangione, A.; Anniballi, G.; Vitale, M.; Vetrani, C.; Cipriano, P.; Della Corte, G.; et al. Diets naturally rich in polyphenols improve fasting and postprandial dyslipidemia and reduce oxidative stress: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 99, 463–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, X.; Tresserra-Rimbau, A.; Estruch, R.; Martínez-González, M.A.; Medina-Remón, A.; Castañer, O.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.M. Effects of Polyphenol, Measured by a Biomarker of Total Polyphenols in Urine, on Cardiovascular Risk Factors After a Long-Term Follow-Up in the PREDIMED Study. Oxid. Med. Cell Longev. 2016, 2016, 2572606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsui, T.; Ueda, T.; Oki, T.; Sugita, K.; Terahara, N.; Matsumoto, K. Alpha-glucosidase inhibitory action of natural acylated anthocyanins. 2. alpha-Glucosidase inhibition by isolated acylated anthocyanins. J. Agric. Food Chem. 2001, 49, 1952–1956. [Google Scholar] [CrossRef] [PubMed]
- Demirer, B.; Yardimci, H.; Basmaz, S.E. Inflammation level in type 2 diabetes is associated with dietary advanced glycation end products, Mediterranean diet adherence and oxidative balance score: A pathway analysis. J. Diabetes Complicat. 2022, 37, 108354. [Google Scholar] [CrossRef]
- Sun, C.; Zhang, F.; Ge, X.; Yan, T.; Chen, X.; Shi, X.; Zhai, Q. SIRT1 improves insulin sensitivity under insulin-resistant conditions by repressing PTP1B. Cell Metab. 2007, 6, 307–319. [Google Scholar] [CrossRef] [Green Version]
- Milne, J.C.; Lambert, P.D.; Schenk, S.; Carney, D.P.; Smith, J.J.; Gagne, D.J.; Jin, L.; Boss, O.; Perni, R.B.; Vu, C.B.; et al. Small molecule activators of SIRT1 as therapeutics for the treatment of type 2 diabetes. Nature 2007, 450, 712–716. [Google Scholar] [CrossRef] [Green Version]
- Fujii, H.; Yokozawa, T.; Kim, Y.A.; Tohda, C.; Nonaka, G.I. Protective effect of grape seed polyphenols against high glucose-induced oxidative stress. Biosci. Biotechnol. Biochem. 2006, 70, 2104–2111. [Google Scholar] [CrossRef]
- Burkholder-Cooley, N.M.; Rajaram, S.S.; Haddad, E.H.; Oda, K.; Fraser, G.E.; Jaceldo-Siegl, K. Validating polyphenol intake estimates from a food-frequency questionnaire by using repeated 24-h dietary recalls and a unique method-of-triads approach with 2 biomarkers. Am. J. Clin. Nutr. 2017, 105, 685–694. [Google Scholar] [CrossRef] [Green Version]
- Medina-Remón, A.; Casas, R.; Tressserra-Rimbau, A.; Ros, E.; Martínez-González, M.A.; Fitó, M.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventos, R.M.; Estruch, R.; et al. Polyphenol intake from a Mediterranean diet decreases inflammatory bi-omarkers related to atherosclerosis: A substudy of the PREDIMED trial. Br. J. Clin. Pharmacol. 2017, 83, 114–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina-Remón, A.; Barrionuevo-González, A.; Zamora-Ros, R.; Andres-Lacueva, C.; Estruch, R.; Martínez-González, M.A.; Diez-Espino, J.; Lamuela-Raventos, R.M. Rapid Folin-Ciocalteu method using microtiter 96-well plate cartridges for solid phase extraction to assess urinary total phenolic compounds, as a biomarker of total polyphenols intake. Anal. Chim. Acta 2009, 634, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Medina-Remón, A.; Tresserra-Rimbau, A.; Pons, A.; Tur, J.; Martorell, M.; Ros, E.; Buil-Cosiales, P.; Sacanella, E.; Covas, M.; Corella, D.; et al. Effects of total dietary polyphenols on plasma nitric oxide and blood pressure in a high cardiovascular risk cohort. The PREDIMED randomized trial. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Manach, C.; Scalbert, A.; Morand, C.; Rémésy, C.; Jiménez, L. Polyphenols: Food sources and bioavailability. Am. J. Clin. Nutr. 2004, 79, 727–747. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Energy-Adjusted Quintiles of Total Phenolic Compounds Intake | |||||
|---|---|---|---|---|---|
| Q1 (n = 3565) | Q2 (n = 3564) | Q3 (n = 3564) | Q4 (n = 3564) | Q5 (n = 3564) | |
| Age (years) | 32.8 (10.2) | 35.89 (11.2) | 37.67 (11.52) | 39.46 (11.83) | 41.4 (12.4) |
| Sex (% women) | 56.1% | 60.2% | 62.2% | 62.7% | 63.9% |
| Total phenolic compounds (mg/day) | 415.9 (98.3) | 602.6 (39.6) | 734.6 (39.0) | 892.4 (55.8) | 1279.4 (329.1) |
| Flavonoids (mg/day) | 203.9 (86.1) | 314.9 (78.4) | 397.6 (91.4) | 497.8 (117.1) | 776.4 (312.8) |
| Lignans (mg/day) | 1.6 (0.6) | 1.9 (0.6) | 2.2 (0.7) | 2.4 (0.8) | 2.9 (1.3) |
| Phenolic acids (mg/day) | 182.7 (70.3) | 250.2 (74.4) | 293.9 (85.7) | 345.7 (107.6) | 442.7 (179.6) |
| Stilbenes (mg/day) | 0.6 (1.2) | 0.9 (1.7) | 1.2 (2.1) | 1.5 (2.7) | 1.8 (3.8) |
| Other phenolic compounds (mg/day) | 27.1 (19.1) | 34.6 (19.9) | 39.8 (21.8) | 45.0 (27.6) | 55.5 (51.7) |
| Body mass Index (kg/m2) | 23.5 (3.6) | 23.5 (3.4) | 23.5 (3.5) | 23.5 (3.4) | 23.3 (3.5) |
| Physical activity (METS-h/week) | 18.7 (21.5) | 19.6 (20.5) | 22.2 (22.5) | 23.3 (23.1) | 26.4 (27.4) |
| University education (years) | 5.0 (1.5) | 5.1 (1.5) | 5.1 (1.6) | 5.1 (1.5) | 5.0 (1.5) |
| TV watching time (hours) | 1.7 (1.3) | 1.6 (1.2) | 1.6 (1.1) | 1.6 (1.1) | 1.5 (1.1) |
| Smoking | |||||
| Current smoker | 23.8% | 22.9% | 22.7% | 23.7% | 22.2% |
| Former smoker | 25.7% | 26.3% | 28.6% | 28.3% | 29.7% |
| Never smoker | 49.9% | 50.1% | 48.2% | 47.3% | 47.5% |
| Package-years of smoking | 6.5 (11.5) | 5.7 (9.6) | 5.8 (9.5) | 5.9 (9.4) | 6.2 (9.7) |
| Marital status (% married) | 37.8% | 46.2% | 52.2% | 54.7% | 58.1% |
| Dyslipidemia at baseline | 15.4% | 15.0% | 17.2% | 17.4% | 18.1% |
| Hypertension at baseline | 10.5% | 10.3% | 10.5% | 9.4% | 10.1% |
| Family history of diabetes | 15.6% | 15.9% | 15.1% | 15.0% | 15.7% |
| CVD at baseline | 1.4% | 1.4% | 1.4% | 1.2% | 1.5% |
| Hormone replacement therapy (% of women) | 0.85% | 1.5% | 2% | 2.15% | 3.1% |
| Total energy intake (Kcal/day) | 2580 (567.2) | 2293 (584) | 2236 (596) | 2297 (592) | 2470 (614) |
| Carbohydrate intake (% energy) | 42.6 (7.5) | 42.4 (6.9) | 43.0 (6.7) | 44.0 (6.8) | 46.2 (7.5) |
| Protein intake (% energy) | 17.9 (3.2) | 18.5 (3.1) | 18.6 (3.0) | 18.4 (3.2) | 17.7 (3.1) |
| Fat intake (% energy) | 37.9 (6.6) | 37.3 (6.0) | 36.4 (5.9) | 35.3 (6.0) | 33.9 (6.6) |
| Dietary fiber intake (g/day) | 19.7 (7.4) | 19.8 (7.5) | 21.3 (7.8) | 23.7 (8.7) | 29.5 (12.1) |
| Alcohol intake (g/day) | 5.5 (9.3) | 6.0 (8.6) | 6.4 (8.8) | 7.1 (9.9) | 7.6 (11.6) |
| Adherence to MDS (0–9 score) | 3.4 (1.6) | 3.8 (1.6) | 4.2 (1.7) | 4.6 (1.7) | 5.1 (1.7) |
| Glycemic Index (0–100) | 54.2 (4.6) | 53.0 (4.2) | 52.2 (4.0) | 51.5 (4.1) | 49.9 (4.0) |
| Phenolic Compounds Classes and Subclasses | Mean (mg/d) ± SD, (%) | Food Sources * (% of Contribution) |
|---|---|---|
| Flavonoids | 435.7 ± 237.7, (55.5) | |
| Anthocyanins | 38.4 ± 44, (4.9) | Cherries (44.9), strawberries (15.7), red wine (14.8), grapes (13.3), olives (8.1), beans (1.3). |
| Chalcones | 0.003 ± 0.006, (<0.01) | Beer (100). |
| Dihydrochalcones | 1.95 ± 2.6, (0.25) | Apples (100). |
| Dihydroflavonols | 1.42 ± 3.3, (0.18) | Red wine (98.3), other wines (1.7). |
| Flavan-3-ols | 21.23 ± 16.1, (2.7) | Apples (27.6), chocolate (21.1), red wine (15.4), peaches (10.1), cherries (6.4), grapes (5.4), strawberries (2.9), green beans (2.5), banana (2.5) lentils (1.3). |
| Flavanones | 75.1 ± 76.5, (9.5) | Oranges (43.4), natural orange juice (34.4), fruit juices from concentrate (18.8), tomato (1.4), other fruit juices (1.3). |
| Flavones | 17.6 ± 13.3, (17.6) | Other vegetables (37.4), natural orange juice (17.6), cookies (10.1), olives (6), fruit juices from concentrate (4.6), chocolate cookies (3), watermelon (2.8), industrial bakery (2.3) pastries (2.2), croquettes (1.8), peppers (1.7), pizza (1.4), cupcake (1.1). |
| Flavonols | 57.4 ± 36.2, (7.3) | Lettuce (36.3), Swiss chard leaves (29.1), asparagus (11.4), olives (3.2), nuts (3), green beans (2.7), cabbage (1.7), chocolate (1.6), tomato (1.5), apples (1.5). |
| Isoflavonoids | 0.04 ± 0.3, (0.04) | Beans (69.6), nuts (27.7), beer (2.6). |
| Proanthocyanidins | 222.6 ± 199.1 (28.4) | Chocolate (43.8), apple (22), cherries (11.8), strawberries (5.2), grapes (4.4), nuts (4.2), red wine (3.3), beans (3.2). |
| Lignans | 2.2 ± 0.96, (0.3) | Carrot and pumpkin (12.3), olive oil (11.4), tomato (9), broccoli and cabbage (7.6), oranges (7), green beans (6), peaches (4.4), pepper (3.5), strawberries (3), asparagus (2.8), red wine (2.8), cold tomato soup (2.8), cookies (2.8), apples (2.3), grapes (1.8), eggplant zucchini and cucumber (1.7), kiwi (1.4), dried fruit (1.4), fried potatoes (1.3), melon (1.3), nuts (1.1). |
| Phenolic acids | 304.1 ± 152.4, (38.8) | |
| Hydroxybenzoic acids | 32 ± 25.3, (4.1) | Nuts (35), olives (16.5), strawberries (12.7), carrots and pumpkin (12.3), Swiss chard leaves (7.7), red wine (5.6), beer (2.6), apples (1.4). |
| Hydroxycinnamic acids | 267 ± 140.3, (34.1) | Coffee (33.3), decaffeinated coffee (12.7), other vegetable (8.5) carrots and pumpkin (7.7) cherries (6.5), French fries (5.5), olives (4.7), apple (4.3), baked or boiled potatoes (3) tomato (1.85), peaches (1.4), nuts (1.4), orange juice (1.3) red wine (1.2). |
| Hydroxyphenylpropanoic acids | 0.6 ± 0.9, (0.07) | Olives (100). |
| Hydroxyphenylacetic acids | 4.5 ± 7.1, (4.5) | Olives (96.4), red wine (2.7). |
| Stilbenes | 1.24 ± 2.6, (0.15) | Red wine (89.3), grapes (3.6), other wines (3.5), strawberries (2.3). |
| Other phenolic compounds | 40.9 ± 33.7, (5.2) | |
| Alkylmethoxyphenols | 0.3 ± 0.5, (0.03) | Decaffeinated coffee (84.3) beer (15.7). |
| Alkylphenols | 8 ± 11.2, (1) | Breakfast cereals (43.4), whole-grain bread (41.5), pasta (8.2), cookies (2.3). |
| Furanocoumarins | 0.4 ± 0.7, (0.05) | Other vegetables (100). |
| Hydroxybenzaldehydes | 0.2 ± 0.43, (0.2) | Red wine (91), beer (2.7), other wines (2.6), olives (1.8), whisky (1.4). |
| Hydroxybenzoketones | 0.001 ± 0.002, (<0.01) | Beer (100) |
| Hydroxycoumarins | 0.05 ± 0.09, (<0.01) | Beer (75.4), other wines (24.6) |
| Methoxyphenols | 0.03 ± 0.09, (<0.01) | Decaffeinated coffee (100) |
| Tyrosols | 27.4 ± 30.5, (3.5) | Olives (64.9), olive oil (29.7), red wine (3.4), cold tomato soup (1.2). |
| Other phenolic compounds (subclass) | 4.6 ± 6.5 (0.6) | Orange juice (66.7), other fruits juice (22.2), Coffee (6.1), apples (2.5), olives (1.5) |
| Energy-Adjusted Quintiles of Total Phenolic Compounds Intake | Low Intake vs. Medium–High Intake | ||||||
|---|---|---|---|---|---|---|---|
| 1 n = 3565 | 2 n = 3564 | 3 n = 3564 | 4 n = 3564 | 5 n = 3564 | p for Trend | Q1 vs. Q2–Q5 | |
| Total phenolic compounds | |||||||
| Median intake (mg/d) | 434.9 | 602.6 | 733.4 | 887.8 | 1180.1 | ||
| Cases | 29 | 32 | 36 | 41 | 48 | ||
| Person-years | 45,183 | 45,561 | 45,243 | 44,585 | 44,180 | ||
| Age-sex adjusted HR (95% CI) | 1 (Ref.) | 0.82 (0.50–1.37) | 0.80 (0.49–1.30) | 0.77 (0.48–1.25) | 0.77 (0.48–1.25) | 0.39 | 1.26 (0.84–1.88) |
| Multivariable adjusted model 1 | 1 (Ref.) | 1.03 (0.58–1.85) | 0.81 (0.45–1.44) | 0.85 (0.48–1.49) | 0.68 (0.39–1.20) | 0.12 | 1.21 (0.74–1.95) |
| Restricted to >50 years old | 1 (Ref.) | 1.26 (0.68–2.35) | 0.87 (0.46–1.64) | 1.05 (0.57–1.94) | 0.85 (0.46–1.58) | 0.44 | 1.00 (0.60–1.69) |
| Repeated measurements model 1 | 1 (Ref.) | 0.93 (0.51–1.64) | 0.72 (0.40–1.30) | 0.83 (0.48–1.45) | 0.67 (0.38–1.15) | 0.15 | 1.29 (0.80–2.09) |
| Restricted to >50 years old | 1 (Ref.) | 0.88 (0.48–1.63) | 0.95 (0.53–1.70) | 0.92 (0.51–1.65) | 0.80 (0.45–1.45) | 0.56 | 1.12 (0.69–1.82) |
| Flavonoids | |||||||
| Median intake (mg/d) | 191.4 | 302.4 | 388.5 | 499.3 | 724.7 | ||
| Cases | 29 | 35 | 35 | 47 | 40 | ||
| Person-years | 45,728 | 45,180 | 45,561 | 44,160 | 44,122 | ||
| Age-sex adjusted HR (95% CI) | 1 (Ref.) | 0.98 (0.60–1.61) | 0.79 (0.48–1.30) | 0.98 (0.61–1.57) | 0.76 (0.47–1.21) | 0.27 | 1.14 (0.76–1.72) |
| Multivariable adjusted model 1 | 1 (Ref.) | 0.96 (0.54–1.71) | 0.67 (0.38–1.22) | 0.97 (0.55–1.69) | 0.71 (0.4–1.24) | 0.32 | 1.23 (0.76–1.98) |
| Restricted to >50 years old | 1 (Ref.) | 1.14 (0.62–2.11) | 0.71 (0.37–1.34) | 0.96 (0.52–1.78) | 0.67 (0.37–1.2) | 0.20 | 1.16 (0.69–1.95) |
| Repeated measurements model 1 | 1 (Ref.) | 0.79 (0.45–1.40) | 0.68 (0.38–1.18) | 0.78 (0.45–1.37) | 0.71 (0.41–1.26) | 0.42 | 1.35 (0.85–2.14) |
| Restricted to >50 years old | 1 (Ref.) | 0.68 (0.38–1.22) | 0.64 (0.35–1.15) | 0.78 (0.43–1.39) | 0.56 (0.31–1.00) | 0.15 | 1.52 (0.95–2.44) |
| Lignans | |||||||
| Median intake (mg/d) | 1.2 | 1.7 | 2.1 | 2.5 | 3.4 | ||
| Cases | 29 | 42 | 27 | 47 | 41 | ||
| Person-years | 46,726 | 46,246 | 45,187 | 44,094 | 42,500 | ||
| Age-sex adjusted HR (95% CI) | 1 (Ref.) | 1.06 (0.66–1.70) | 0.67 (0.40–1.14) | 1.05 (0.65–1.68) | 0.85 (0.53–1.36) | 0.57 | 1.10 (0.73–1.65) |
| Multivariable adjusted model 1 | 1 (Ref.) | 0.94 (0.55–1.61) | 0.63 (0.35–1.146 | 0.92 (0.53–1.61) | 0.78 (0.44–1.35) | 0.47 | 1.20 (0.75–1.92) |
| Restricted to >50 years old | 1 (Ref.) | 0.57 (0.32–1.04) | 0.65 (0.36–1.17) | 0.77 (0.43–1.38) | 0.67 (0.37–1.2) | 0.50 | 1.53 (0.95–2.45) |
| Repeated measurements model 1 | 1 (Ref.) | 0.90 (0.52–1.56) | 0.68 (0.37–1.24) | 0.95 (0.54–1.66) | 0.81 (0.46–1.43) | 0.67 | 1.19 (0.74–1.92) |
| Restricted to >50 years old | 1 (Ref.) | 0.51 (0.28–0.93) | 0.64 (0.35–1.16) | 0.98 (0.56–1.72) | 0.59 (0.34–1.03) | 0.53 | 1.52 (0.96–2.40) |
| Phenolic acids intake | |||||||
| Median intake (mg/d) | 147.7 | 221.9 | 285.7 | 352.5 | 482.4 | ||
| Cases | 19 | 41 | 35 | 36 | 55 | ||
| Person-years | 44,495 | 44,995 | 44,582 | 45,418 | 45,262 | ||
| Age-sex adjusted HR (95% CI) | 1 (Ref.) | 1.39 (0.80–2.40) | 1.19 (0.68–2.09) | 1.08 (0.61–1.88) | 1.44 (0.82–2.53) | 0.36 | 0.78 (0.48–1.26) |
| Multivariable adjusted model 1 | 1 (Ref.) | 1.50 (0.79–2.83) | 1.31 (0.69–2.49) | 1.33 (0.7–2.51) | 1.19 (0.63–2.25) | 0.84 | 0.75 (0.43–1.32) |
| Restricted to >50 years old | 1 (Ref.) | 1.16 (0.64–2.12) | 1.07 (0.57–1.99) | 1.04 (0.56–1.94) | 0.99 (0.52–1.84) | 0.76 | 0.94 (0.56–1.55) |
| Repeated measurements model 1 | 1 (Ref.) | 1.41 (0.75–2.68) | 1.39 (0.74–2.64) | 1.32 (0.70–2.51) | 1.17 (0.62–2.22) | 0.81 | 0.75 (0.43–1.33) |
| Restricted to >50 years old | 1 (Ref.) | 1.08 (0.60–1.96) | 1.22 (0.67–2.20) | 0.83 (0.44–1.55) | 1.01 (0.54–1.90) | 0.81 | 0.96 (0.60–1.57) |
| Stilbenes intake | |||||||
| Median intake (mg/d) | −0.0 | 0.1 | 0.4 | 0.8 | 3.6 | ||
| N | 3564 | 3564 | 3564 | 3564 | 3564 | ||
| Cases | 29 | 26 | 31 | 40 | 60 | ||
| Person-years | 45,603 | 44,073 | 44,221 | 44,409 | 46,446 | ||
| Age-sex adjusted HR (95% CI) | 1 (Ref.) | 1.02 (0.60–1.73) | 0.84 (0.50–1.39) | 0.83 (0.51–1.34) | 0.75 (0.46–1.21) | 0.20 | 1.20 (0.81–1.80) |
| Multivariable adjusted model 1 | 1 (Ref.) | 0.91 (0.48–1.72) | 0.58 (0.31–1.08) | 0.84 (0.46–1.53) | 0.67 (0.37–1.21) | 0.31 | 1.38 (0.83–2.28) |
| Restricted to >50 years old | 1 (Ref.) | 0.58 (0.31–1.09) | 0.75 (0.4–1.42) | 0.64 (0.34–1.2) | 0.51 (0.27–0.95) * | 0.09 | 1.66 (0.99–2.79) |
| Repeated measurements model 1 | 1 (Ref.) | 0.87 (0.47–1.64) | 0.55 (0.29–1.02) | 0.75 (0.42–1.37) | 0.67 (0.39–1.17) | 0.50 | 1.42 (0.86–2.32) |
| Restricted to >50 years old | 1 (Ref.) | 0.59 (0.32–1.07) | 0.64 (0.34–1.21) | 0.64 (0.35–1.18) | 0.46 (0.25–0.85) * | 0.08 | 1.75 (1.06–2.90) * |
| Other phenolic compounds intake | |||||||
| Median intake (mg/d) | 14.2 | 25.3 | 34.0 | 45.2 | 72.4 | ||
| Cases | 34 | 33 | 29 | 40 | 50 | ||
| Person-years | 46,187 | 45,737 | 45,103 | 43,789 | 43,936 | ||
| Age-sex adjusted HR (95% CI) | 1 (Ref.) | 0.88 (0.55–1.43) | 0.80 (0.49–1.31) | 1.07 (0.67–1.69) | 1.11 (0.70–1.75) | 0.33 | 1.03 (0.71- 1.5) |
| Multivariable adjusted model 1 | 1 (Ref.) | 0.74 (0.42–1.29) | 0.70 (0.39–1.25) | 1.10 (0.64–1.89) | 1.08 (0.63–1.87) | 0.22 | 1.10 (0.7–1.72) |
| Restricted to >50 years old | 1 (Ref.) | 0.94 (0.49–1.82) | 0.92 (0.47–1.84) | 1.93 (1.04–3.59) | 1.38 (0.74–2.58) | 0.08 | 0.79 (0.46–1.33) |
| Repeated measurements model 1 | 1 (Ref.) | 0.73 (0.42–1.28) | 0.82 (0.46–1.45) | 1.04 (0.61–1.80) | 1.01 (0.59–1.74) | 0.46 | 1.10 (0.71–1.72) |
| Restricted to >50 years old | 1 (Ref.) | 0.85 (0.45–1.62) | 1.03 (0.55–1.96) | 1.76 (0.96–3.23) | 1.12 (0.61–2.06) | 0.33 | 0.87 (0.52–1.45) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vázquez-Ruiz, Z.; Martínez-González, M.Á.; Vitelli-Storelli, F.; Bes-Rastrollo, M.; Basterra-Gortari, F.J.; Toledo, E. Effect of Dietary Phenolic Compounds on Incidence of Type 2 Diabetes in the “Seguimiento Universidad de Navarra” (SUN) Cohort. Antioxidants 2023, 12, 507. https://doi.org/10.3390/antiox12020507
Vázquez-Ruiz Z, Martínez-González MÁ, Vitelli-Storelli F, Bes-Rastrollo M, Basterra-Gortari FJ, Toledo E. Effect of Dietary Phenolic Compounds on Incidence of Type 2 Diabetes in the “Seguimiento Universidad de Navarra” (SUN) Cohort. Antioxidants. 2023; 12(2):507. https://doi.org/10.3390/antiox12020507
Chicago/Turabian StyleVázquez-Ruiz, Zenaida, Miguel Ángel Martínez-González, Facundo Vitelli-Storelli, Maira Bes-Rastrollo, Francisco Javier Basterra-Gortari, and Estefanía Toledo. 2023. "Effect of Dietary Phenolic Compounds on Incidence of Type 2 Diabetes in the “Seguimiento Universidad de Navarra” (SUN) Cohort" Antioxidants 12, no. 2: 507. https://doi.org/10.3390/antiox12020507