
New Insights into Cutaneous Asepsis: Synergism between Pfaffia and Rosemary Extracts

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Minimum Inhibitory, Minimum Bactericidal, and Fractional Inhibitory Concentrations of P. paniculata and R. officinalis
2.2. Biofilm Viability Measured by MTT Analysis
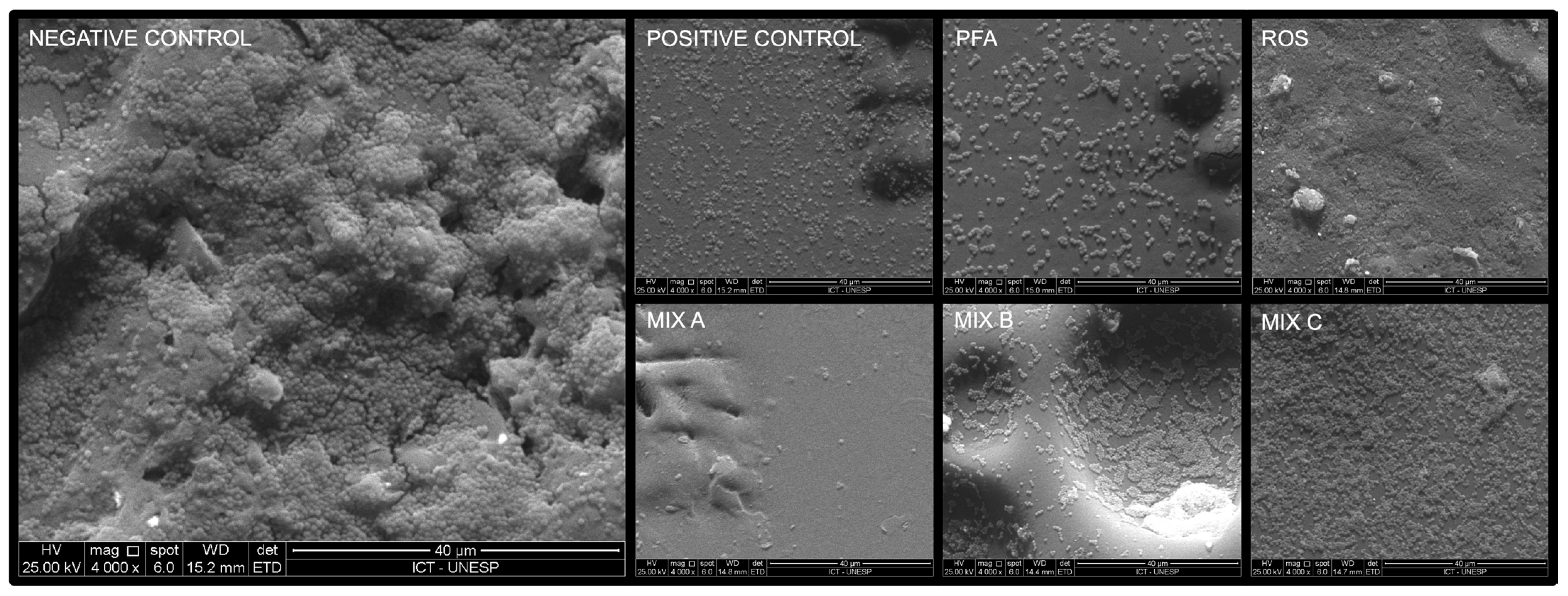
2.3. Scanning Electron Microscopy Analysis
2.4. Cell Viability Measured by MTT Analysis
3. Discussion
4. Materials and Methods
4.1. Bacterial Strains and Plants Extracts
4.2. Determination of Minimum Inhibitory and Minimum Bactericidal Concentration
4.3. Monotypic and Cutaneous Model Biofilm
4.4. Bacterial Viability by MTT Analysis
4.5. Antimicrobial Analysis by Scanning Electron Microscopy
4.6. Human Keratinocytes Viability by MTT Analysis
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rosenthal, V.D.; Yin, R.; Nercelles, P.; Rivera-Molina, S.E.; Jyoti, S.; Dongol, R.; Aguilar-De-Moros, D.; Tumu, N.; Alarcon-Rua, J.; Stagnaro, J.P.; et al. International Nosocomial Infection Control Consortium (INICC) report of health care associated infections, data summary of 45 countries for 2015 to 2020, adult and pediatric units, device-associated module. Am. J. Infect. Control 2024, in press. [Google Scholar] [CrossRef] [PubMed]
- Assis, S.F.; Vieira, D.F.V.B.; Sousa, F.R.E.G.; Pinheiro, C.E.O.; Prado, P.R.D. Adverse events in critically ill patients: A cross-sectional study. Rev. Esc. Enferm. USP 2022, 56, e20210481. [Google Scholar] [CrossRef] [PubMed]
- Manoukian, S.; Stewart, S.; Dancer, S.; Graves, N.; Mason, H.; McFarland, A.; Robertson, C.; Reilly, J. Estimating excess length of stay due to healthcare-associated infections: A systematic review and meta-analysis of statistical methodology. J. Hosp. Infect. 2018, 100, 222–235. [Google Scholar] [CrossRef] [PubMed]
- Allegranzi, B.; Bagheri Nejad, S.; Combescure, C.; Graafmans, W.; Attar, H.; Donaldson, L.; Pittet, D. Burden of endemic health-care-associated infection in developing countries: Systematic review and meta-analysis. Lancet 2011, 377, 228–241. [Google Scholar] [CrossRef] [PubMed]
- Li Pomi, F.; Papa, V.; Borgia, F.; Vaccaro, M.; Allegra, A.; Cicero, N.; Gangemi, S. Rosmarinus officinalis and Skin: Antioxidant Activity and Possible Therapeutical Role in Cutaneous Diseases. Antioxidants 2023, 12, 680. [Google Scholar] [CrossRef] [PubMed]
- Elston, M.J.; Dupaix, J.P.; Opanova, M.I.; Atkinson, R.E. Cutibacterium acnes (formerly Proprionibacterium acnes) and Shoulder Surgery. Hawai’i J. Health Soc. Welf. 2019, 78 (Suppl. S2), 3–5. [Google Scholar]
- Anand, S.; Pogorelić, Z.; Singh, A.; Llorente Muñoz, C.M.; Krishnan, N.; Dhua, A.K.; Goel, P.; Bajpai, M. Comparison of Unnoticed Glove Perforations during Minimally Invasive versus Open Surgeries: A Systematic Review and Meta-Analysis. Children 2022, 9, 179. [Google Scholar] [CrossRef] [PubMed]
- Amini Tapouk, F.; Nabizadeh, R.; Mirzaei, N.; Hosseini Jazani, N.; Yousefi, M.; Valizade Hasanloei, M.A. Comparative efficacy of hospital disinfectants against nosocomial infection pathogens. Antimicrob. Resist. Infect. Control 2020, 9, 115. [Google Scholar] [CrossRef]
- Mehrad, B.; Clark, N.M.; Zhanel, G.G.; Lynch, J.P., 3rd. Antimicrobial resistance in hospital-acquired gram-negative bacterial infections. Chest 2015, 147, 1413–1421. [Google Scholar] [CrossRef]
- Chapman, A.K.; Aucott, S.W.; Milstone, A.M. Safety of chlorhexidine gluconate used for skin antisepsis in the preterm infant. J. Perinatol. 2012, 32, 4–9. [Google Scholar] [CrossRef]
- Roode, G.J.; Bütow, K.W. A Descriptive Study of Chlorhexidine as a Disinfectant in Cleft Palate Surgery. Clin. Med. Res. 2018, 16, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.; Christie, J.; Liu, Z.; Westby, M.J.; Jefferies, J.M.; Hudson, T.; Edwards, J.; Mohapatra, D.P.; Hassan, I.A.; Dumville, J.C. Antiseptics for burns. Cochrane Database Syst. Rev. 2017, 7, CD011821. [Google Scholar] [CrossRef] [PubMed]
- Rodenak-Kladniew, B.; Castro, M.A.; Gambaro, R.C.; Girotti, J.; Cisneros, J.S.; Viña, S.; Padula, G.; Crespo, R.; Castro, G.R.; Gehring, S.; et al. Cytotoxic Screening and Enhanced Anticancer Activity of Lippia alba and Clinopodium nepeta Essential Oils-Loaded Biocompatible Lipid Nanoparticles against Lung and Colon Cancer Cells. Pharmaceutics 2023, 15, 2045. [Google Scholar] [CrossRef]
- Atanasov, A.G.; Zotchev, S.B.; Dirsch, V.M.; International Natural Product Sciences Taskforce; Supuran, C.T. Natural products in drug discovery: Advances and opportunities. Nat. Rev. Drug Discov. 2021, 20, 200–216. [Google Scholar] [CrossRef]
- de Oliveira, J.R.; Camargo, S.E.A.; de Oliveira, L.D. Rosmarinus officinalis L. (rosemary) as therapeutic and prophylactic agent. J. Biomed. Sci. 2019, 26, 5. [Google Scholar] [CrossRef] [PubMed]
- Paula-Ramos, L.; da Rocha Santos, C.E.; Camargo Reis Mello, D.; Nishiama Theodoro, L.; De Oliveira, F.E.; Back Brito, G.N.; Junqueira, J.C.; Jorge, A.O.C.; de Oliveira, L.D. Klebsiella pneumoniae Planktonic and Biofilm Reduction by Different Plant Extracts: In Vitro Study. Sci. World J. 2016, 2016, 3521413. [Google Scholar] [CrossRef]
- Foster, A.L.; Cutbush, K.; Ezure, Y.; Schuetz, M.A.; Crawford, R.; Paterson, D.L. Cutibacterium acnes in shoulder surgery: A scoping review of strategies for prevention, diagnosis, and treatment. J. Shoulder Elb. Surg. 2021, 30, 1410–1422. [Google Scholar] [CrossRef] [PubMed]
- Dörfel, D.; Maiwald, M.; Daeschlein, G.; Müller, G.; Hudek, R.; Assadian, O.; Kampf, G.; Kohlmann, T.; Harnoss, J.C.; Kramer, A. Comparison of the antimicrobial efficacy of povidone-iodine-alcohol versus chlorhexidine-alcohol for surgical skin preparation on the aerobic and anaerobic skin flora of the shoulder region. Antimicrob. Resist. Infect. Control 2021, 10, 17. [Google Scholar] [CrossRef]
- Manilal, A.; Sabu, K.R.; Shewangizaw, M.; Aklilu, A.; Seid, M.; Merdikios, B.; Tsegaye, B. In vitro antibacterial activity of medicinal plants against biofilm-forming methicillin-resistant Staphylococcus aureus: Efficacy of Moringa stenopetala and Rosmarinus officinalis extracts. Heliyon 2020, 6, e03303. [Google Scholar] [CrossRef]
- de Oliveira, J.R.; de Jesus, D.; Figueira, L.W.; de Oliveira, F.E.; Pacheco Soares, C.; Camargo, S.E.; Jorge, A.O.; de Oliveira, L.D. Biological activities of Rosmarinus officinalis L. (rosemary) extract as analyzed in microorganisms and cells. Exp. Biol. Med. 2017, 242, 625–634. [Google Scholar] [CrossRef]
- Weckesser, S.; Engel, K.; Simon-Haarhaus, B.; Wittmer, A.; Pelz, K.; Schempp, C.M. Screening of plant extracts for antimicrobial activity against bacteria and yeasts with dermatological relevance. Phytomedicine 2007, 14, 508–516. [Google Scholar] [CrossRef]
- Fu, Y.; Zu, Y.; Chen, L.; Efferth, T.; Liang, H.; Liu, Z.; Liu, W. Investigation of antibacterial activity of rosemary essential oil against Propionibacterium acnes with atomic force microscopy. Planta Medica 2007, 73, 1275–1280. [Google Scholar] [CrossRef] [PubMed]
- Boutahiri, S.; Eto, B.; Bouhrim, M.; Mechchate, H.; Saleh, A.; Al Kamaly, O.; Drioiche, A.; Remok, F.; Samaillie, J.; Neut, C.; et al. Lavandula pedunculata (Mill.) Cav. Aqueous Extract Antibacterial Activity Improved by the Addition of Salvia rosmarinus Spenn., Salvia lavandulifolia Vahl and Origanum compactum Benth. Life 2022, 12, 328. [Google Scholar] [CrossRef] [PubMed]
- Manville, R.W.; Hogenkamp, D.; Abbott, G.W. Ancient medicinal plant rosemary contains a highly efficacious and isoform-selective KCNQ potassium channel opener. Commun. Biol. 2023, 6, 644. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Extract | S. aureus | S. epidermidis | C. acnes | ||||||
|---|---|---|---|---|---|---|---|---|---|
| MIC | MBC | FIC | MIC | MBC | FIC | MIC | MBC | FIC | |
| P. paniculata | 25 | 25 | - | 25 | Absent | - | 6.25 | 50 | - |
| Mix A | 25 | 25 | IND | 50 | Absent | ANT | 3.12 | 25 | SYN |
| Mix B | 50 | 50 | IND | 50 | Absent | ANT | 3.12 | 25 | SYN |
| Mix C | 50 | 50 | IND | 50 | Absent | ANT | 6.25 | 6.25 | IND |
| R. officinalis | 50 | Absent | - | 25 | Absent | - | 0.195 | 6.25 | - |
| Groups | S. aureus | S. epidermidis | ||
|---|---|---|---|---|
| % Evolution | p Value | % Evolution | p Value | |
| Negative control (BHI) | +100 | +100 | ||
| P. paniculata 50 mg/mL | −19.20 | ns | −45.87 | **** |
| P. paniculata 100 mg/mL | −62.64 | **** | −76.64 | **** |
| R. officinalis 50 mg/mL | −46.63 | *** | −56.24 | **** |
| R. officinalis 100 mg/mL | −78.56 | **** | −80.11 | **** |
| Mix A 50 mg/mL | −18.46 | ns | −79.13 | **** |
| Mix A 100 mg/mL | −79.10 | **** | −79.13 | **** |
| Mix B 50 mg/mL | −34.95 | * | −78.38 | **** |
| Mix B 100 mg/mL | −82.68 | **** | −79.48 | **** |
| Mix C 50 mg/mL | −78.53 | **** | −77.65 | **** |
| Mix C 100 mg/mL | −80.77 | **** | −72.71 | **** |
| Positive control (CHX 0.12%) | −42.3 | **** | −74.9 | **** |
| Groups | C. acnes | Heterotypic Biofilms | ||
|---|---|---|---|---|
| % Evolution | p Value | % Evolution | p Value | |
| Negative control (BHI) | +100 | +100 | ||
| P. paniculata 50 mg/mL | +260.60 | **** | −88.73 | **** |
| P. paniculata 100 mg/mL | +51.32 | * | −91.78 | **** |
| R. officinalis 50 mg/mL | +17.97 | ns | −90.90 | **** |
| R. officinalis 100 mg/mL | +48.32 | ns | −92.82 | **** |
| Mix A 50 mg/mL | −46.33 | ns | −93.46 | **** |
| Mix A 100 mg/mL | −56.36 | * | −93.77 | **** |
| Mix B 50 mg/mL | +68.84 | *** | −92.77 | **** |
| Mix B 100 mg/mL | −36.26 | ns | −93.50 | **** |
| Mix C 50 mg/mL | −36.26 | ns | −92.78 | **** |
| Mix C 100 mg/mL | −47.31 | ns | −91.78 | **** |
| Positive control (CHX 0.12%) | −50.5 | ** | −85.8 | **** |
| Groups | % Viability | p Value |
|---|---|---|
| Negative control (culture medium) | 100 | |
| P. paniculata 50 mg/mL | 70.3 | **** |
| P. paniculata 100 mg/mL | 60.1 | **** |
| R. officinalis 50 mg/mL | 91.3 | **** |
| R. officinalis 100 mg/mL | 60.1 | **** |
| Mix A 50 mg/mL | 70.8 | **** |
| Mix A 100 mg/mL | 59.7 | **** |
| Mix B 50 mg/mL | 68.8 | **** |
| Mix B 100 mg/mL | 59.7 | **** |
| Mix C 50 mg/mL | 65.9 | **** |
| Mix C 100 mg/mL | 59.1 | **** |
| Positive control (CHX 0.06%) | 14.6 | **** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, D.G.; Carrouel, F.; Silva, T.C.A.; Rozzatto, M.C.; Hasna, A.A.; Santos, C.E.R.; Morais, F.V.; de Oliveira, L.D.; de Paula Ramos, L. New Insights into Cutaneous Asepsis: Synergism between Pfaffia and Rosemary Extracts. Antibiotics 2024, 13, 226. https://doi.org/10.3390/antibiotics13030226
Miranda DG, Carrouel F, Silva TCA, Rozzatto MC, Hasna AA, Santos CER, Morais FV, de Oliveira LD, de Paula Ramos L. New Insights into Cutaneous Asepsis: Synergism between Pfaffia and Rosemary Extracts. Antibiotics. 2024; 13(3):226. https://doi.org/10.3390/antibiotics13030226
Chicago/Turabian StyleMiranda, Diego Garcia, Florence Carrouel, Tatiane Cristina Alberti Silva, Mariana Cafalchio Rozzatto, Amjad Abu Hasna, Carlos Eduardo Rocha Santos, Flavia Villaça Morais, Luciane Dias de Oliveira, and Lucas de Paula Ramos. 2024. "New Insights into Cutaneous Asepsis: Synergism between Pfaffia and Rosemary Extracts" Antibiotics 13, no. 3: 226. https://doi.org/10.3390/antibiotics13030226