
Preventing Multidrug-Resistant Bacterial Transmission in the Intensive Care Unit with a Comprehensive Approach: A Policymaking Manual
 , ,
, ,
Abstract
:1. Introduction
2. The Path of the ICU-Acquired Infections
3. Hand-Hygiene
4. Environmental Cleaning
5. Identification of Risk Factors for Colonization
6. ICU Design Workflow
7. Antimicrobial Surveillance and Stewardship
8. Systematic Approach and Integration
9. Policy-Making Manual
9.1. Framework for Developing Policy Recommendations on Preventing MDR Bacterial Transmission in ICUs
9.2. Proposed Policy Recommendations for Preventing MDR Bacterial Transmission in ICUs
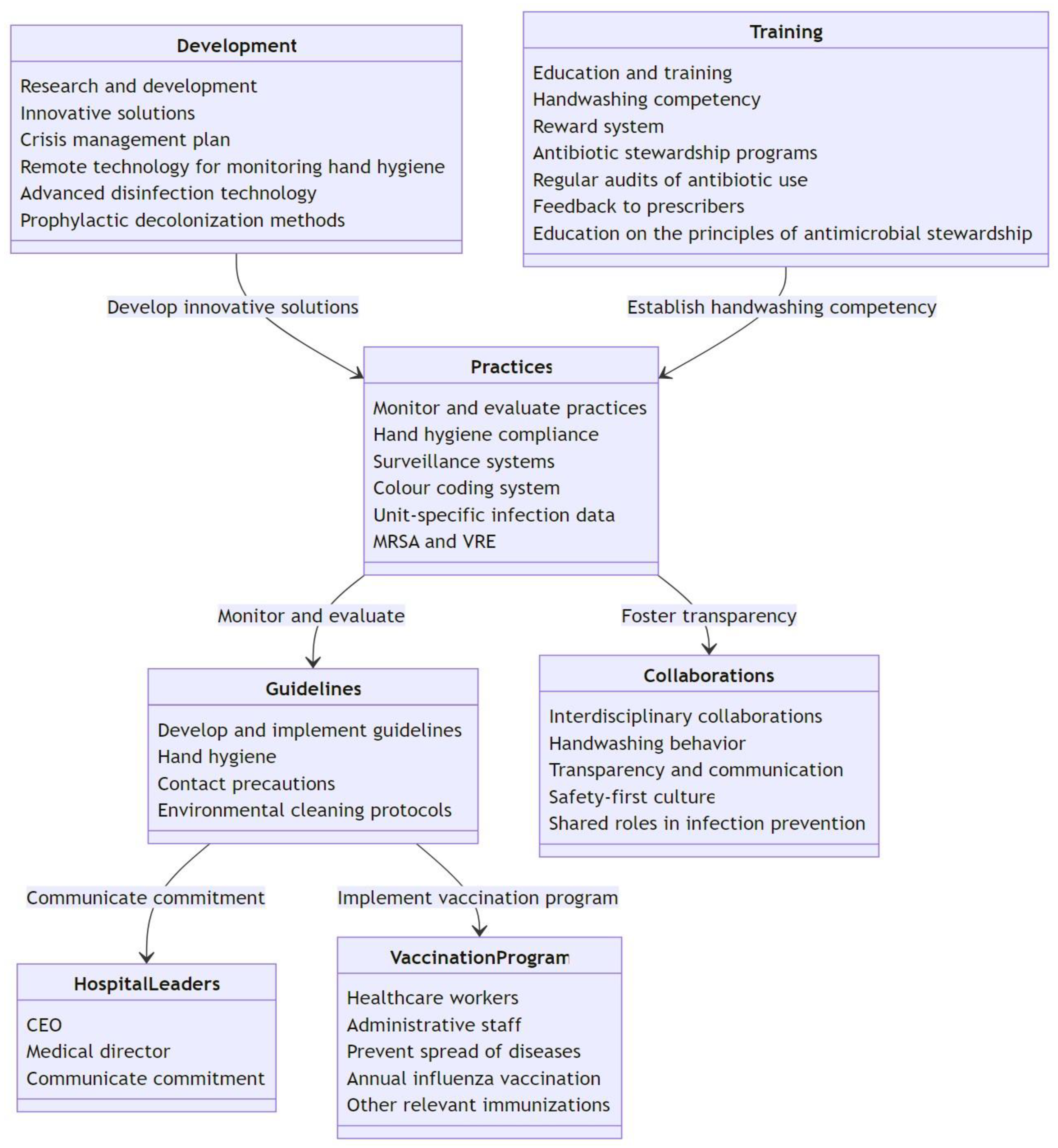
- Develop and implement evidence-based infection prevention and control guidelines tailored to ICUs, including those for hand hygiene, contact precautions, and environmental cleaning protocols. Ensure that hospital leaders such as the CEO and medical director actively communicate their commitment to these guidelines and infection control measures through regular communication channels. Implement a comprehensive vaccination program for healthcare workers and administrative staff to prevent the spread of vaccine-preventable diseases in ICUs. This should include annual influenza vaccination and other relevant immunizations.
- Continuously monitor and evaluate infection control practices, identifying areas for improvement to ensure best practices are consistently in use. Implement a system for monitoring hand hygiene compliance and provide regular feedback to clinical units, including unit-specific infection data for MRSA and VRE. Encourage the use of surveillance systems to track and monitor the prevalence and spread of multidrug-resistant organisms (MDROs) in ICUs. These data can be used to inform infection control strategies and to assess the effectiveness of interventions. Implement a color-coding system to separate different areas and prevent cross-contamination. This will make it easier for the staff to identify and adhere to specific cleaning protocols for each area. Adopt quality and cost-based selection criteria for interventions, such as annual cost reduction based on patient-day and infection reductions, use manpower, and benchmark the implementation duration for each intervention.
- Promote strong interdisciplinary collaborations between all relevant specialists to foster a safety-first culture and shared stress roles in infection prevention in medical settings. Encourage all personnel in supervisory roles to model appropriate handwashing behavior and address poor handwashing practices among their staff, creating a culture of accountability and emphasizing the importance of hand hygiene in preventing MDR transmission. Foster a culture of transparency and open communication regarding infection control issues. This includes reporting and discussing infection rates, outbreaks, and control measures in a nonpunitive manner, which can help identify problems and solutions more effectively.
- Allocate resources for the research and development of novel technologies and practices, targeting the reduction in environmental contamination and cross-transmission. Invest in the development and implementation of innovative solutions, such as remote technology for monitoring hand hygiene compliance, advanced disinfection technology for decontaminating surfaces, and prophylactic decolonization methods for healthcare workers, such as adequate and updated personal protective equipment and decontamination devices, such as mobile phone UV tanks. Develop and implement a robust crisis management plan to ensure the continuity of infection control measures during emergencies or outbreaks. This should include contingency plans for staff shortages, supply chain disruptions, and increased patient volume.
- Chronically reinforce education and training in core infection prevention and control practices in sequential sessions given to ICU personnel, with a focus on their roles in enhancing both visible engagement and ensuring foundational knowledge of preventive approaches. Establish handwashing as a core competency for all clinical staff with regular assessments and the reinforcement of proper techniques. Recognize and reward individuals or teams that demonstrate exemplary hand hygiene practices through formal and informal recognition systems. Advocate for the implementation of ASPs to optimize the use of antimicrobials, reduce the risk of antibiotic resistance, and improve patient outcomes. This should include regular audits on antibiotic use, feedback to prescribers, and education on the principles of antimicrobial stewardship.
9.3. Proposed Program Analysis for Enforcing Hand Hygiene Standards in ICUs
- (1)
- Leadership commitment: Implement a policy that requires hospital leaders, such as the CEO and medical director, to actively communicate their commitment to hand hygiene and infection control measures. This can be achieved through regular communication channels such as hospital publications, emails, and meetings. Policy discussions should explore the potential benefits and challenges of incorporating innovative technologies, such as UV or gaseous decontamination, into healthcare cleaning practices. Encourage all personnel in supervisory roles to model appropriate handwashing behaviors and address poor handwashing practices among staff. This can help to create a culture of accountability and emphasize the importance of hand hygiene in preventing MDROs transmission.
- (2)
- Hand hygiene education: Develop a comprehensive hand hygiene education program for all ICU employees and physicians. This program should include information on the correct handwashing procedure, the importance of hand hygiene in preventing MDROs transmission, and the use of appropriate hand hygiene products. All recommendations and educational materials should be supported by evidence in the scientific literature and involve collaboration between professional societies, public institutions, and industry stakeholders. The importance of incorporating evidence-based recommendations and involving relevant specialists in educational practices cannot be overemphasized in the policymaking process.
- (3)
- Hand hygiene competency: Establish handwashing as a core competency for all clinical staff with regular assessments and the reinforcement of proper techniques. New hires should receive handwashing fact sheets and sample hand hygiene products as part of their orientation. Training programs, educational content, and goals should be explained clearly and extensively to employees regardless of their background, stature, or hierarchical position. Ensure that the hiring and dismissal processes consider the candidate’s commitment to hand hygiene and infection control practices, reinforcing the organization’s values and expectations regarding hand hygiene and the prevention of MDROs transmission.
- (4)
- Monitoring and feedback: Implement a system for monitoring hand hygiene compliance and providing regular feedback to clinical units. This could include unit-specific infection data for MRSA and VRE as well as using outbreaks or high infection rates as opportunities to review and reinforce handwashing practices. Different approaches should be considered to communicate feedback and possible audit results, given their potential impact on healthcare personnel and patient safety based on cultural differences, system hierarchies, and the goals of each intervention. Develop a policy to recognize and reward individuals or teams who demonstrate exemplary hand hygiene practices. This could include formal recognition such as awards or certificates or informal recognition such as praise or positive feedback from supervisors. For instance, National Health Service cleaning standards use a star rating system displayed in each area, whereas the DIN 13063 guidelines emphasize the need for clear communication of results to employees at the execution level [82].
10. Materials and Methods
10.1. Study Design and Data Collection
10.2. Data Analysis and Synthesis
10.3. Limitations and Gaps in the Literature
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABHS | Alcohol-Based Hand Sanitizers |
| AHHMS | Automated Hand Hygiene Monitoring System |
| AI | Artificial Intelligence |
| AMSS | Antimicrobial Surveillance and Stewardship |
| ASP | Antimicrobial Stewardship Program |
| ATP | Adenosine Triphosphate |
| ATS | American Thoracic Society |
| CDC | Centers for Disease Control and Prevention |
| EHHMS | Electronic Hand Hygiene Monitoring System |
| ESBL | Extended-Spectrum β-Lactamase |
| GNB | Gram-Negative Bacteria |
| HAC | Healthcare-Acquired Colonization |
| HAI | Healthcare-Associated Infection |
| HCP | Healthcare Personnel |
| HEH | Healthcare Environmental Hygiene |
| HEPA | High-Efficiency Particulate Absorption |
| ICU | Intensive Care Unit |
| IDSA | Infectious Diseases Society of America |
| MD | Model |
| MDR | Multidrug-Resistant |
| MDRO | Multidrug-Resistant Organism |
| MRSA | Methicillin-Resistant Staphylococcus aureus |
| NICU | Neonatal Intensive Care Unit |
| PPE | Personal Protective Equipment |
| SHEA | Society for Healthcare Epidemiology of America |
| UV | Ultraviolet |
| VRE | Vancomycin-Resistant enterococci |
| WHO | World Health Organization |
References
- Han, Y.; Zhang, J.; Zhang, H.Z.; Zhang, X.Y.; Wang, Y.M. Multidrug-resistant organisms in intensive care units and logistic analysis of risk factors. World J. Clin. Cases 2022, 10, 1795–1805. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Johani, K.; Gosbell, I.B.; Jacombs, A.S.; Almatroudi, A.; Whiteley, G.S.; Deva, A.; Jensen, S.; Vickery, K. Intensive care unit environmental surfaces are contaminated by multidrug-resistant bacteria in biofilms: Combined results of conventional culture, pyrosequencing, scanning electron microscopy, and confocal laser microscopy. J. Hosp. Infect. 2015, 91, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Strich, J.R.; Palmore, T.N. Preventing Transmission of Multidrug-Resistant Pathogens in the Intensive Care Unit. Infect. Dis. Clin. N. Am. 2017, 31, 535–550. [Google Scholar] [CrossRef] [PubMed]
- Kernéis, S.; Lucet, J.C. Controlling the Diffusion of Multidrug-Resistant Organisms in Intensive Care Units. Semin. Respir. Crit. Care Med. 2019, 40, 558–568. [Google Scholar] [CrossRef]
- De Groote, P.; Blot, K.; Conoscenti, E.; Labeau, S.; Blot, S. Mobile phones as a vector for Healthcare-Associated Infection: A systematic review. Intensive Crit. Care Nurs. 2022, 72, 103266. [Google Scholar] [CrossRef]
- Galvin, S.; Dolan, A.; Cahill, O.; Daniels, S.; Humphreys, H. Microbial monitoring of the hospital environment: Why and how? J. Hosp. Infect. 2012, 82, 143–151. [Google Scholar] [CrossRef]
- Weber, D.J.; Rutala, W.A.; Miller, M.B.; Huslage, K.; Sickbert-Bennett, E. Role of hospital surfaces in the transmission of emerging health care-associated pathogens: Norovirus, Clostridium difficile, and Acinetobacter species. Am. J. Infect. Control 2010, 38, S25–S33. [Google Scholar] [CrossRef] [PubMed]
- Levin, P.D.; Shatz, O.; Sviri, S.; Moriah, D.; Or-Barbash, A.; Sprung, C.L.; Moses, A.E.; Block, C. Contamination of portable radiograph equipment with resistant bacteria in the ICU. Chest 2009, 136, 426–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulger, F.; Esen, S.; Dilek, A.; Yanik, K.; Gunaydin, M.; Leblebicioglu, H. Are we aware how contaminated our mobile phones with nosocomial pathogens? Ann. Clin. Microbiol. Antimicrob. 2009, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Agodi, A.; Barchitta, M.; Cipresso, R.; Giaquinta, L.; Romeo, M.A.; Denaro, C. Pseudomonas aeruginosa carriage, colonization, and infection in ICU patients. Intensive Care Med. 2007, 33, 1155–1161. [Google Scholar] [CrossRef]
- Boyce, J.M. Modern technologies for improving cleaning and disinfection of environmental surfaces in hospitals. Antimicrob. Resist. Infect. Control 2016, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brêda Mascarenhas, L.A.; Machado, B.A.S.; Rodrigues, L.A.P.; Saraiva Hodel, K.V.; Bandeira Santos, A.; Freitas Neves, P.R.; da Silva Andrade, L.P.C.; Soares, M.B.; de Andrade, J.B.; Badaró, R. Potential application of novel technology developed for instant decontamination of personal protective equipment before the doffing step. PLoS ONE 2021, 16, e0250854. [Google Scholar] [CrossRef] [PubMed]
- Elbehiry, A.; Marzouk, E.; Abalkhail, A.; El-Garawany, Y.; Anagreyyah, S.; Alnafea, Y.; Almuzaini, A.M.; Alwarhi, W.; Rawway, M.; Draz, A. The Development of Technology to Prevent, Diagnose, and Manage Antimicrobial Resistance in Healthcare-Associated Infections. Vaccines 2022, 10, 2100. [Google Scholar] [CrossRef] [PubMed]
- Lanckohr, C.; Boeing, C.; De Waele, J.J.; de Lange, D.W.; Schouten, J.; Prins, M.; Nijsten, M.; Povoa, P.; Morris, A.C.; Bracht, H. Antimicrobial stewardship, therapeutic drug monitoring and infection management in the ICU: Results from the international A—TEAMICU survey. Ann. Intensive Care 2021, 11, 131. [Google Scholar] [CrossRef] [PubMed]
- Jamin, C.; De Koster, S.; van Koeveringe, S.; De Coninck, D.; Mensaert, K.; De Bruyne, K.; Selva, N.P.; Lammens, C.; Goossens, H.; Hoebe, C.; et al. Harmonization of whole-genome sequencing for outbreak surveillance of Enterobacteriaceae and Enterococci. Microb. Genom. 2021, 7, 000567. [Google Scholar] [CrossRef]
- Montero, J.G.; Lerma, F.; Galleymore, P.R.; Martínez, M.P.; Rocha, L.; Gaite, F.B.; Rodríguez, J.Á.; González, M.C.; Moreno, I.F.; Baño, J.R.; et al. Combatting resistance in intensive care: The multimodal approach of the Spanish ICU “Zero Resistance” program. Crit. Care 2015, 19, 114. [Google Scholar] [CrossRef] [Green Version]
- Rohr, U.; Kaminski, A.; Wilhelm, M.; Jurzik, L.; Gatermann, S.; Muhr, G. Colonization of patients and contamination of the patients’ environment by MRSA under conditions of single-room isolation. Int. J. Hyg. Environ. Health 2009, 212, 209–215. [Google Scholar] [CrossRef]
- Pittet, D.; Dharan, S.; Touveneau, S.; Sauvan, V.; Perneger, T.V. Bacterial contamination of the hands of hospital staff during routine patient care. Arch. Intern. Med. 1999, 159, 821–826. [Google Scholar] [CrossRef]
- Montoya, A.; Schildhouse, R.; Goyal, A.; Mann, J.D.; Snyder, A.; Chopra, V.; Mody, L. How often are health care personnel hands colonized with multidrug- resistant organisms? A systematic review and meta-analysis. Am. J. Infect. Control 2019, 47, 693–703. [Google Scholar] [CrossRef] [Green Version]
- Sax, H.; Allegranzi, B.; Uçkay, I.; Larson, E.; Boyce, J.; Pittet, D. ‘My five moments for hand hygiene’: A user-centred design approach to understand, train, monitor and report hand hygiene. J. Hosp. Infect. 2007, 67, 9–21. [Google Scholar] [CrossRef]
- Hayden, M.K.; Blom, D.W.; Lyle, E.A.; Moore, C.G.; Weinstein, R.A. Risk of hand or glove contamination after contact with patients colonized with vancomycin-resistant enterococcus or the colonized patients’ environment. Infect. Control Hosp. Epidemiol. 2008, 29, 149–154. [Google Scholar] [CrossRef]
- Bonten, M.J.; Hayden, M.K.; Nathan, C.; van Voorhis, J.; Matushek, M.; Slaughter, S.; Rice, T.; Weinstein, R.A. Epidemiology of colonisation of patients and environment with vancomycin-resistant enterococci. Lancet 1996, 348, 1615–1619. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.P.; Smyth, D.; Moore, G.; Singleton, J.; Jackson, R.; Gant, V.; Jeanes, A.; Shaw, S.; James, E.; Cooper, B.; et al. The impact of enhanced cleaning within the intensive care unit on contamination of the near-patient environment with hospital pathogens: A randomized crossover study in critical care units in two hospitals. Crit. Care Med. 2011, 39, 651–658. [Google Scholar] [CrossRef]
- Albert, N.M.; Hancock, K.; Murray, T.; Karafa, M.; Runner, J.C.; Fowler, S.B.; Nadeau, C.A.; Rice, K.L.; Krajewski, S. Cleaned, ready-to-use, reusable electrocardiographic lead wires as a source of pathogenic microorganisms. Am. J. Crit. Care 2010, 19, e73–e80. [Google Scholar] [CrossRef] [PubMed]
- Lestari, T.; Ryll, S.; Kramer, A. Microbial contamination of manually reprocessed, ready to use ECG lead wire in intensive care units. GMS Hyg. Infect. Control 2013, 8, Doc07. [Google Scholar] [PubMed]
- Whittington, A.M.; Whitlow, G.; Hewson, D.; Thomas, C.; Brett, S.J. Bacterial contamination of stethoscopes on the intensive care unit. Anaesthesia 2009, 64, 620–624. [Google Scholar] [CrossRef]
- Sui, Y.S.; Wan, G.H.; Chen, Y.W.; Ku, H.L.; Li, L.P.; Liu, C.H.; Mau, H.S. Effectiveness of bacterial disinfectants on surfaces of mechanical ventilator systems. Respir. Care 2012, 57, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shokoohi, H.; Armstrong, P.; Tansek, R. Emergency department ultrasound probe infection control: Challenges and solutions. Open Access Emerg. Med. 2015, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Frazee, B.W.; Fahimi, J.; Lambert, L.; Nagdev, A. Emergency department ultrasonographic probe contamination and experimental model of probe disinfection. Ann. Emerg. Med. 2011, 58, 56–63. [Google Scholar] [CrossRef]
- Muradali, D.; Gold, W.L.; Phillips, A.; Wilson, S. Can ultrasound probes and coupling gel be a source of nosocomial infection in patients undergoing sonography? An in vivo and in vitro study. Am. J. Roentgenol. 1995, 164, 1521–1524. [Google Scholar] [CrossRef] [PubMed]
- Bures, S.; Fishbain, J.T.; Uyehara, C.F.; Parker, J.M.; Berg, B.W. Computer keyboards and faucet handles as reservoirs of nosocomial pathogens in the intensive care unit. Am. J. Infect. Control 2000, 28, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Teng, S.O.; Lee, W.S.; Ou, T.Y.; Hsieh, Y.C.; Lee, W.C.; Lin, Y.C. Bacterial contamination of patients’ medical charts in a surgical ward and the intensive care unit: Impact on nosocomial infections. J. Microbiol. Immunol. Infect. 2009, 42, 86–91. [Google Scholar] [PubMed]
- Panhotra, B.R.; Saxena, A.K.; Al-Mulhim, A.S. Contamination of patients’ files in intensive care units: An indication of strict handwashing after entering case notes. Am. J. Infect. Control 2005, 33, 398–401. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.H.; Chen, L.R.; Wang, Y.K. Contamination of medical charts: An important source of potential infection in hospitals. PLoS ONE 2014, 9, e78512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brady, R.R.; Verran, J.; Damani, N.N.; Gibb, A.P. Review of mobile communication devices as potential reservoirs of nosocomial pathogens. J. Hosp. Infect. 2009, 71, 295–300. [Google Scholar] [CrossRef]
- Kramer, A.; Assadian, O. Survival of Microorganisms on Inanimate Surfaces. In Use of Biocidal Surfaces for Reduction of Healthcare Acquired Infections; Borkow, G., Ed.; Springer International Publishing: Cham, Switzerland, 2014; pp. 7–26. [Google Scholar]
- Glowicz, J.B.; Landon, E.; Sickbert-Bennett, E.E.; Aiello, A.E.; Dekay, K.; Hoffmann, K.K.; Maragakis, L.; Olmsted, R.N.; Polgreen, P.M.; Trexler, P.A.; et al. SHEA/IDSA/APIC Practice Recommendation: Strategies to prevent healthcare-associated infections through hand hygiene: 2022 Update. Infect. Control Hosp. Epidemiol. 2023, 44, 355–376. [Google Scholar] [CrossRef]
- Chou, D.T.; Achan, P.; Ramachandran, M. The World Health Organization ‘5 moments of hand hygiene’: The scientific foundation. J. Bone Jt. Surg. Br. 2012, 94, 441–445. [Google Scholar] [CrossRef]
- Gestrich, S.A.; Jencson, A.L.; Cadnum, J.L.; Livingston, S.H.; Wilson, B.M.; Donskey, C.J. A multicenter investigation to characterize the risk for pathogen transmission from healthcare facility sinks. Infect. Control Hosp. Epidemiol. 2018, 39, 1467–1469. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, J.; Qiao, F.; Feng, B.; Hu, F.; Xi, Z.-A.; Wu, W.; Ni, Z.-L.; Liu, L.; Yuan, Y. Compared hand hygiene compliance among healthcare providers before and after the COVID-19 pandemic: A rapid review and meta-analysis. Am. J. Infect. Control 2022, 50, 563–571. [Google Scholar] [CrossRef]
- Ali, A.S.; Cherel, O.; Brehaut, P.; Garrait, V.; Lombardin, C.; Schortgen, F.; Constan, A.; Lanceleur, F.; El-Assali, A.; Poullain, S.; et al. Impact of COVID-19 pandemic waves on health-care worker hand hygiene activity in department of medicine and ICU as measured by an automated monitoring system. Infect. Dis. Health 2023, 28, 95–101. [Google Scholar] [CrossRef]
- Hess, O.C.R.; Armstrong-Novak, J.D.; Doll, M.; Cooper, K.; Bailey, P.; Godbout, E.; Stevens, M.P.; Bearman, G. The impact of coronavirus disease 2019 (COVID-19) on provider use of electronic hand hygiene monitoring technology. Infect. Control Hosp. Epidemiol. 2021, 42, 1007–1009. [Google Scholar] [CrossRef]
- Doll, M.E.; Pierce, J.W. Electronic hand hygiene monitoring systems: Not worth the costs. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, e126. [Google Scholar] [CrossRef] [PubMed]
- Schaffzin, J.K. Electronic hand hygiene monitoring systems are the wave of the future. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, e89. [Google Scholar] [CrossRef] [PubMed]
- Anforderungen an die Hygiene bei der Reinigung und Desinfektion von Flächen. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2022, 65, 1074–1115. [CrossRef] [PubMed]
- Siddharth, V.; Singh, A.R.; Sharma, D.K.; Satpathy, S.; Kaushal, V.K.; Lathwal, A.; Sain, A.; Misra, S.; Kausar, M.; Garg, R. National guidelines for sanitation services: Addressing the unmet need of standardizing cleaning practices in tertiary care public health facilities of a developing country. J. Fam. Med. Prim. Care 2021, 10, 3475–3480. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.; Schmid, M.N.; Parneix, P.; Lebowitz, D.; de Kraker, M.; Sauser, J.; Zingg, W.; Pittet, D. Impact of environmental hygiene interventions on healthcare-associated infections and patient colonization: A systematic review. Antimicrob. Resist. Infect. Control 2022, 11, 38. [Google Scholar] [CrossRef]
- Lowbury, E.J.; Babb, J.R.; Ford, P.M. Protective isolation in a burns unit: The use of plastic isolators and air curtains. J. Hyg. 1971, 69, 529–546. [Google Scholar] [CrossRef]
- Casini, B.; Tuvo, B.; Scarpaci, M.; Totaro, M.; Badalucco, F.; Briani, S.; Luchini, G.; Costa, A.L.; Baggiani, A. Implementation of an Environmental Cleaning Protocol in Hospital Critical Areas Using a UV-C Disinfection Robot. Int. J. Environ. Res. Public Health 2023, 20, 4284. [Google Scholar] [CrossRef]
- Özen, M.; Yılmaz, G.; Coşkun, B.; Topçuoğlu, P.; Öztürk, B.; Gündüz, M.; Atilla, E.; Arslan, Ö.; Özcan, M.; Demirer, T.; et al. A Quasi-Experimental Study Analyzing the Effectiveness of Portable High-Efficiency Particulate Absorption Filters in Preventing Infections in Hematology Patients during Construction. Turk. J. Haematol. 2016, 33, 41–47. [Google Scholar] [CrossRef]
- Amini Tapouk, F.; Nabizadeh, R.; Mirzaei, N.; Hosseini Jazani, N.; Yousefi, M.; Valizade Hasanloei, M.A. Comparative efficacy of hospital disinfectants against nosocomial infection pathogens. Antimicrob. Resist. Infect. Control 2020, 9, 115. [Google Scholar] [CrossRef]
- Otter, J.A.; Yezli, S.; Perl, T.M.; Barbut, F.; French, G.L. The role of ‘no-touch’ automated room disinfection systems in infection prevention and control. J. Hosp. Infect. 2013, 83, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Birkett, M.; Dover, L.; Cherian Lukose, C.; Wasy Zia, A.; Tambuwala, M.M.; Serrano-Aroca, Á. Recent Advances in Metal-Based Antimicrobial Coatings for High-Touch Surfaces. Int. J. Mol. Sci. 2022, 23, 1162. [Google Scholar] [CrossRef] [PubMed]
- Salgado, C.D.; Sepkowitz, K.A.; John, J.F.; Cantey, J.R.; Attaway, H.H.; Freeman, K.D.; Sharpe, P.A.; Michels, H.T.; Schmidt, M.G. Copper surfaces reduce the rate of healthcare-acquired infections in the intensive care unit. Infect. Control Hosp. Epidemiol. 2013, 34, 479–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blehm, C.J.; Monteiro, M.S.G.; Bessa, M.C.; Leyser, M.; Dias, A.S.; Sumienski, J.; Gallo, S.W.; da Silva, A.B.; Barros, A.; Marco, R.; et al. Copper-coated hospital surfaces: Reduction of total bacterial loads and resistant Acinetobacter spp. AMB Express 2022, 12, 146. [Google Scholar] [CrossRef]
- Masse, J.; Elkalioubie, A.; Blazejewski, C.; LeDoux, G.; Wallet, F.; Poissy, J.; Preau, S.; Nseir, S. Colonization pressure as a risk factor of ICU-acquired multidrug resistant bacteria: A prospective observational study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 797–805. [Google Scholar] [CrossRef]
- Nseir, S.; Grailles, G.; Soury-Lavergne, A.; Minacori, F.; Alves, I.; Durocher, A. Accuracy of American Thoracic Society/Infectious Diseases Society of America criteria in predicting infection or colonization with multidrug-resistant bacteria at intensive-care unit admission. Clin. Microbiol. Infect. 2010, 16, 902–908. [Google Scholar] [CrossRef] [Green Version]
- Xie, J.; Ma, X.; Huang, Y.; Mo, M.; Guo, F.; Yang, Y.; Qiu, H. Value of American Thoracic Society guidelines in predicting infection or colonization with multidrug-resistant organisms in critically ill patients. PLoS ONE 2014, 9, e89687. [Google Scholar] [CrossRef]
- Mietchen, M.S.; Short, C.T.; Samore, M.; Lofgren, E.T. Examining the impact of ICU population interaction structure on modeled colonization dynamics of Staphylococcus aureus. PLoS Comput. Biol. 2022, 18, e1010352. [Google Scholar] [CrossRef]
- Majumder, A.A.; Rahman, S.; Cohall, D.; Bharatha, A.; Singh, K.; Haque, M.; Hilaire, M.G.-S. Antimicrobial Stewardship: Fighting Antimicrobial Resistance and Protecting Global Public Health. Infect. Drug Resist. 2020, 13, 4713–4738. [Google Scholar] [CrossRef]
- Spernovasilis, N.; Kritsotakis, E.I.; Mathioudaki, A.; Vouidaski, A.; Markaki, I.; Psaroudaki, D.; Ioannou, P.; Kofteridis, D.P. Antimicrobial Prescribing before and after the Implementation of a Carbapenem-Focused Antimicrobial Stewardship Program in a Greek Tertiary Hospital during the COVID-19 Pandemic. Antibiotics 2022, 12, 39. [Google Scholar] [CrossRef]
- Spernovasilis, N.; Kritsotakis, E.I.; Mathioudaki, A.; Vouidaski, A.; Spanias, C.; Petrodaskalaki, M.; Ioannou, P.; Chamilos, G.; Kofteridis, D.P. A carbapenem-focused antimicrobial stewardship programme implemented during the COVID-19 pandemic in a setting of high endemicity for multidrug-resistant Gram-negative bacteria. J. Antimicrob. Chemother. 2023, 78, 1000–1008. [Google Scholar] [CrossRef]
- Huang, J.; Cui, C.; Zhou, S.; Chen, M.; Wu, H.; Jin, R.; Chen, X. Impact of multicenter unified enhanced environmental cleaning and disinfection measures on nosocomial infections among patients in intensive care units. J. Int. Med. Res. 2020, 48, 300060520949766. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Huang, H.M.; Lin, P.Y.; Shi, Z.Y. Comparing visual inspection and performance observation for evaluation of hospital cleanliness. Am. J. Infect. Control 2021, 49, 1511–1514. [Google Scholar] [CrossRef] [PubMed]
- Spernovasilis, N.; Ierodiakonou, D.; Spanias, C.; Mathioudaki, A.; Ioannou, P.; Petrakis, E.C.; Kofteridis, D.P. Doctors’ Perceptions, Attitudes and Practices towards the Management of Multidrug-Resistant Organism Infections after the Implementation of an Antimicrobial Stewardship Programme during the COVID-19 Pandemic. Trop. Med. Infect. Dis. 2021, 6, 20. [Google Scholar] [CrossRef]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C. What is antimicrobial stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ture, Z.; Güner, R.; Alp, E. Antimicrobial stewardship in the intensive care unit. J. Intensive Med. 2023, 3, 244–253. [Google Scholar] [CrossRef]
- Mokrani, D.; Chommeloux, J.; Pineton de Chambrun, M.; Hékimian, G.; Luyt, C.E. Antibiotic stewardship in the ICU: Time to shift into overdrive. Ann. Intensive Care 2023, 13, 39. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, P.J.; Rohailla, S.; Taggart, L.R.; Lightfoot, D.; Havey, T.; Daneman, N.; Lowe, C.; Muller, M.P. Antimicrobial Stewardship and Intensive Care Unit Mortality: A Systematic Review. Clin. Infect. Dis. 2019, 68, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Mandelli, G.; Dore, F.; Langer, M.; Garbero, E.; Alagna, L.; Bianchin, A.; Ciceri, R.; Di Paolo, A.; Giani, T.; Giugni, A.; et al. Effectiveness of a Multifaced Antibiotic Stewardship Program: A Pre-Post Study in Seven Italian ICUs. J. Clin. Med. 2022, 11, 4409. [Google Scholar] [CrossRef]
- Davari, M.; Khorasani, E.; Tigabu, B.M. Factors Influencing Prescribing Decisions of Physicians: A Review. Ethiop. J. Health Sci. 2018, 28, 795–804. [Google Scholar] [CrossRef]
- Evans, R.S.; Pestotnik, S.L.; Classen, D.C.; Clemmer, T.P.; Weaver, L.K.; Orme, J.F.; Lloyd, J.F., Jr.; Burke, J.P. A computer-assisted management program for antibiotics and other antiinfective agents. N. Engl. J. Med. 1998, 338, 232–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buising, K.L.; Thursky, K.A.; Robertson, M.B.; Black, J.F.; Street, A.C.; Richards, M.J.; Brown, G.V. Electronic antibiotic stewardship-reduced consumption of broad-spectrum antibiotics using a computerized antimicrobial approval system in a hospital setting. J. Antimicrob. Chemother. 2008, 62, 608–616. [Google Scholar] [CrossRef] [Green Version]
- Cavallaro, M.; Moran, E.; Collyer, B.; McCarthy, N.D.; Green, C.; Keeling, M.J. Informing antimicrobial stewardship with explainable AI. PLoS Digit. Health 2023, 2, e0000162. [Google Scholar] [CrossRef] [PubMed]
- Spernovasilis, N.; Ierodiakonou, D.; Milioni, A.; Markaki, L.; Kofteridis, D.P.; Tsioutis, C. Assessing the knowledge, attitudes and perceptions of junior doctors on antimicrobial use and antimicrobial resistance in Greece. J. Glob. Antimicrob. Resist. 2020, 21, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Seidelman, J.L.; Turner, N.A.; Wrenn, R.H.; Sarubbi, C.; Anderson, D.J.; Sexton, D.J.; Moehring, R.W. Impact of Antibiotic Stewardship Rounds in the Intensive Care Setting: A Prospective Cluster-Randomized Crossover Study. Clin. Infect. Dis. 2022, 74, 1986–1992. [Google Scholar] [CrossRef]
- Ya, K.Z.; Win, P.T.N.; Bielicki, J.; Lambiris, M.; Fink, G. Association between Antimicrobial Stewardship Programs and Antibiotic Use Globally: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2023, 6, e2253806. [Google Scholar]
- Haque, M.; McKimm, J.; Sartelli, M.; Dhingra, S.; Labricciosa, F.M.; Islam, S.; Jahan, D.; Nusrat, T.; Chowdhury, T.S.; Coccolini, F.; et al. Strategies to Prevent Healthcare-Associated Infections: A Narrative Overview. Risk Manag. Healthc. Policy 2020, 13, 1765–1780. [Google Scholar] [CrossRef]
- Teerawattanapong, N.; Kengkla, K.; Dilokthornsakul, P.; Saokaew, S.; Apisarnthanarak, A.; Chaiyakunapruk, N. Prevention and Control of Multidrug-Resistant Gram-Negative Bacteria in Adult Intensive Care Units: A Systematic Review and Network Meta-analysis. Clin. Infect. Dis. 2017, 64, S51–S60. [Google Scholar] [CrossRef]
- Saporito, L.; Graziano, G.; Mescolo, F.; Amodio, E.; Insinga, V.; Rinaudo, G.; Aleo, A.; Bonura, C.; Vitaliti, M.; Corsello, G.; et al. Efficacy of a coordinated strategy for containment of multidrug-resistant Gram-negative bacteria carriage in a Neonatal Intensive Care Unit in the context of an active surveillance program. Antimicrob. Resist. Infect. Control 2021, 10, 30. [Google Scholar] [CrossRef]
- Peters, A.; Schmid, M.N.; Kraker, M.E.A.; Parneix, P.; Pittet, D. Results of an international pilot survey on health care environmental hygiene at the facility level. Am. J. Infect. Control 2022, 50, 1302–1310. [Google Scholar] [CrossRef]
- Peters, A.; Parneix, P.; Kiernan, M.; Severin, J.A.; Gauci, T.; Pittet, D. New frontiers in healthcare environmental hygiene: Thoughts from the 2022 healthcare cleaning forum. Antimicrob. Resist. Infect. Control 2023, 12, 7. [Google Scholar] [CrossRef] [PubMed]
- Çaǧlayan, Ç.; Barnes, S.L.; Pineles, L.L.; Harris, A.D.; Klein, E.Y. A Data-Driven Framework for Identifying Intensive Care Unit Admissions Colonized with Multidrug-Resistant Organisms. Front. Public Health 2022, 10, 853757. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xiao, Y.; Yang, Q.; Wang, F.; Wang, Y.; Yuan, C. Clinical prediction models for multidrug-resistant organism colonisation or infection in critically ill patients: A systematic review protocol. BMJ Open 2022, 12, e064566. [Google Scholar] [CrossRef]
- Paramythiotou, E.; Routsi, C. Association between infections caused by multidrug-resistant gram-negative bacteria and mortality in critically ill patients. World J. Crit. Care Med. 2016, 5, 111–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakbar, I.; Medam, S.; Ronflé, R.; Cassir, N.; Delamarre, L.; Hammad, E.; Lopez, A.; Lepape, A.; Machut, A.; Boucekine, M.; et al. Association between mortality and highly antimicrobial-resistant bacteria in intensive care unit-acquired pneumonia. Sci. Rep. 2021, 11, 16497. [Google Scholar] [CrossRef]
- Denis, J.B.; Lehingue, S.; Pauly, V.; Cassir, N.; Gainnier, M.; Léone, M.; Daviet, F.; Coiffard, B.; Baron, S.; Guervilly, C.; et al. Multidrug-resistant Pseudomonas aeruginosa and mortality in mechanically ventilated ICU patients. Am. J. Infect. Control 2019, 47, 1059–1064. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| 1. Disinfect frequently touched surfaces or surfaces close to patients (basic hygiene), such as patient rooms, doctor’s offices, and rescue vehicles. Ensure that the disinfectant used is bactericidal and yeasticidal and allows for an appropriate exposure time before use. Clean these surfaces daily or upon patient changes (without previous isolation). |
| 2. For infrequently touched surfaces or surfaces distant from patients, such as clean work surfaces, medication tables, and dressing trolleys, ensure that the disinfectant used is bactericidal and yeasticidal. Clean these surfaces only when necessary, such as when they are visibly dirty, immediately before use, or in situations of increased risk of contamination. Base the exposure time on the allowed exposure time for a specific disinfectant. |
| 3. Disinfect floor surfaces daily to ensure a clean and hygienic environment, thus minimizing the risk of infection spreading within the ICU. |
| 4. Pay attention to clean work areas/rooms and ensure the proper disinfection of surfaces before performing aseptic tasks. |
| 5. Compliance with other area-specific cleaning regulations (e.g., blood banks, hospital pharmacies, doctor’s offices) is critical for maintaining a safe environment in the ICU. |
| 6. After the discharge of a patient from the ICU, perform a final disinfection of all surfaces to prepare for the next patient and reduce the risk of cross-contamination. |
| 1. Frequency of cleaning: clean high-risk areas such as ICUs once every two hours, with spot cleaning as required. |
| 2. Level of cleaning/disinfection: perform both cleaning and intermediate-level disinfection in high-risk areas. Soap and detergent are used for cleaning, followed by disinfection with alcohol and aldehydes. |
| 3. Method of cleaning/disinfection: use a combination of soap and detergent for cleaning surfaces, followed by the application of disinfectants containing alcohol and aldehyde compounds to achieve intermediate-level disinfection. |
| 4. Evaluation/auditing frequency: conduct weekly evaluations and audits of the cleaning and disinfection practices in high-risk areas. This should be done by the officer in charge of the Sanitation and Infection Control Team. |
| 5. Staffing: in the ICU, one Sanitary Attendant is allocated up to six ICU beds in each shift. |
| 6. Induction training: provide 24 h of intensive training on general cleaning and infection control to all cleaning staff involved in high-risk areas. This training should be followed by seven days of supervised duties. |
| 7. Refresher training/on-the-job training: conduct 4 h of training every month to refresh the knowledge and skills of the cleaning staff in high-risk areas. |
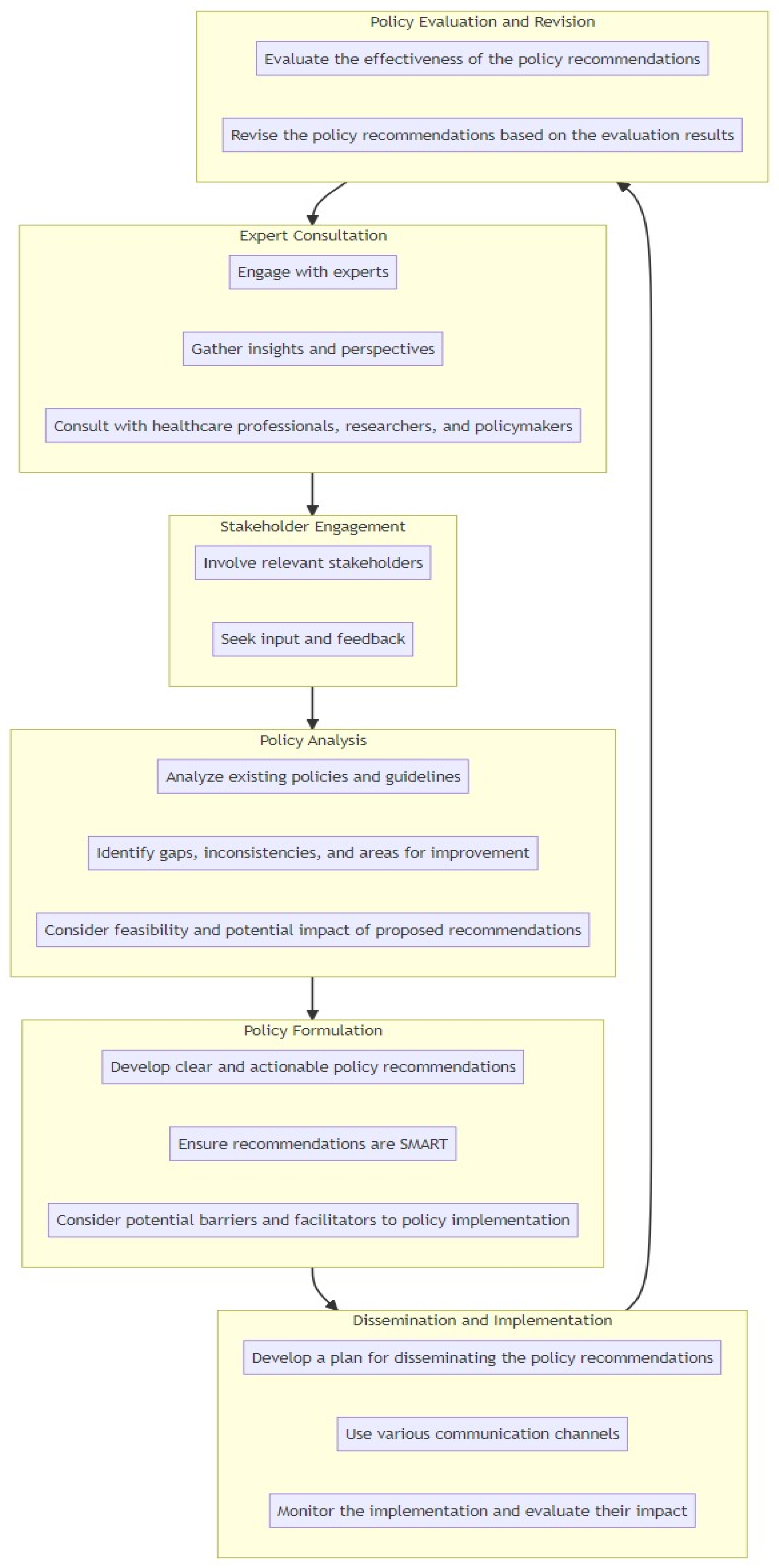
| Expert Consultation for Policy Development: Engage with experts in the field of infection control, healthcare policy, and ICU management to gather insights and perspectives on the topic. Consultations with healthcare professionals, researchers, and policymakers can provide valuable input for developing policy recommendations. |
| Stakeholder Engagement in Policy Formulation: Involve relevant stakeholders, including healthcare administrators, infection control specialists, ICU staff, and patient representatives in the policy development process. Seek their input and feedback to ensure that the recommendations are practical, feasible, and aligned with the needs and realities of the ICU. |
| Policy Analysis: Identifying Gaps and Opportunities: Analyze existing policies and guidelines related to infection control in ICUs at local, national, and international levels. Identify gaps, inconsistencies, and areas for improvement in current policies. Consider the feasibility and potential impact of proposed policy recommendations in the context of existing regulations and healthcare systems. |
| Formulating SMART Policy Recommendations: Based on the evidence from the literature review, expert consultation, stakeholder engagement, and policy analysis, develop clear and actionable policy recommendations. Ensure that the recommendations are specific, measurable, achievable, relevant, and time-bound (SMART). Consider the potential barriers and facilitators of policy implementation and develop strategies to address them. |
| Dissemination and Implementation of Policy Recommendations: Develop a plan for disseminating policy recommendations to relevant stakeholders, including healthcare facilities, professional organizations, and government agencies. Consider the use of various communication channels such as policy briefs, guidelines, workshops, and conferences to raise awareness and promote the adoption of recommendations. Monitor the implementation of the policy recommendations and evaluate their impact on MDR bacterial transmission in the ICU. |
| Policy Evaluation and Revision: A continuous process: Regularly evaluate the effectiveness of policy recommendations in reducing multidrug-resistant bacterial transmission in the ICU. Collect data on key indicators, such as infection rates, hand hygiene compliance, and environmental cleanliness, to assess the impact of the policy. Revise and update policy recommendations based on new evidence, emerging technologies, and changing healthcare practices. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schinas, G.; Polyzou, E.; Spernovasilis, N.; Gogos, C.; Dimopoulos, G.; Akinosoglou, K. Preventing Multidrug-Resistant Bacterial Transmission in the Intensive Care Unit with a Comprehensive Approach: A Policymaking Manual. Antibiotics 2023, 12, 1255. https://doi.org/10.3390/antibiotics12081255
Schinas G, Polyzou E, Spernovasilis N, Gogos C, Dimopoulos G, Akinosoglou K. Preventing Multidrug-Resistant Bacterial Transmission in the Intensive Care Unit with a Comprehensive Approach: A Policymaking Manual. Antibiotics. 2023; 12(8):1255. https://doi.org/10.3390/antibiotics12081255
Chicago/Turabian StyleSchinas, Georgios, Elena Polyzou, Nikolaos Spernovasilis, Charalambos Gogos, George Dimopoulos, and Karolina Akinosoglou. 2023. "Preventing Multidrug-Resistant Bacterial Transmission in the Intensive Care Unit with a Comprehensive Approach: A Policymaking Manual" Antibiotics 12, no. 8: 1255. https://doi.org/10.3390/antibiotics12081255