
Dynamics of Antibiotic Resistance of Streptococcus pneumoniae in France: A Pediatric Prospective Nasopharyngeal Carriage Study from 2001 to 2022

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Carriage and Antibiotic Resistance of S. pneumoniae
2.3. Serotype Distribution and Relation with Penicillin Non-Susceptibility
2.4. Dynamics of Predominant Serotypes during the Late PCV13 Period: Carriage and Penicillin Non-Susceptibility
2.5. Risk Factors of Antibiotic Non-Susceptible S. pneumoniae
2.6. Impact of Non-Pharmaceutical Interventions for COVID-19
3. Discussion
4. Material and Methods
4.1. Study Design
4.2. Ethics
4.3. Microbiological Investigations
4.4. Definitions
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bogaert, D.; De Groot, R.; Hermans, P.W. Streptococcus pneumoniae colonisation: The key to pneumococcal disease. Lancet Infect. Dis. 2004, 4, 144–154. [Google Scholar] [CrossRef]
- Simell, B.; Auranen, K.; Kayhty, H.; Goldblatt, D.; Dagan, R.; O’Brien, K.L.; Pneumococcal Carriage Group. The fundamental link between pneumococcal carriage and disease. Expert Rev. Vaccines 2012, 11, 841–855. [Google Scholar] [CrossRef] [PubMed]
- Kaur, R.; Morris, M.; Pichichero, M.E. Epidemiology of Acute Otitis Media in the Postpneumococcal Conjugate Vaccine Era. Pediatrics 2017, 140, e20170181. [Google Scholar] [CrossRef] [PubMed]
- Trinh, N.T.H.; Cohen, R.; Lemaitre, M.; Chahwakilian, P.; Coulthard, G.; Bruckner, T.A.; Milic, D.; Levy, C.; Chalumeau, M.; Cohen, J.F. Community antibiotic prescribing for children in France from 2015 to 2017: A cross-sectional national study. J. Antimicrob. Chemother. 2020, 75, 2344–2352. [Google Scholar] [CrossRef]
- Pichichero, M.E.; Wright, T. The use of tympanocentesis in the diagnosis and management of acute otitis media. Curr. Infect. Dis. Rep. 2006, 8, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Weinberger, D.M.; Bruden, D.T.; Grant, L.R.; Lipsitch, M.; O’Brien, K.L.; Pelton, S.I.; Sanders, E.A.M.; Feikin, D.R. Using Pneumococcal Carriage Data to Monitor Postvaccination Changes in Invasive Disease. Am. J. Epidemiol. 2013, 178, 1488–1495. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.; Done, N.; Petigara, T.; Mohanty, S.; Song, Y.; Liu, Q.; Lemus-Wirtz, E.; Signorovitch, J.; Sarpong, E.; Weiss, T. Incidence of acute otitis media in children in the United States before and after the introduction of 7- and 13-valent pneumococcal conjugate vaccines during 1998–2018. BMC Infect. Dis. 2022, 22, 294. [Google Scholar] [CrossRef]
- Ben-Shimol, S.; Givon-Lavi, N.; Greenberg, D.; Dagan, R. Pneumococcal nasopharyngeal carriage in children <5 years of age visiting the pediatric emergency room in relation to PCV7 and PCV13 introduction in southern Israel. Hum. Vaccines Immunother. 2015, 12, 268–276. [Google Scholar]
- Cohen, R.; Biscardi, S.; Levy, C. The multifaceted impact of pneumococcal conjugate vaccine implementation in children in France between 2001 to 2014. Hum. Vaccin. Immunother. 2016, 12, 277–284. [Google Scholar] [CrossRef]
- Pulcini, C.; Berger-Carbonne, A.; Coignard, B.; Salomon, J. National Antibiotic Resistance Strategy for Human Health in France. China CDC Wkly. 2022, 4, 1097–1100. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net). Available online: https://www.ecdc.europa.eu/sites/default/files/documents/ESAC-Net_AER_2021_final-rev.pdf (accessed on 4 May 2023).
- Cohen, R.; Varon, E.; Doit, C.; Schlemmer, C.; Romain, O.; Thollot, F.; Béchet, S.; Bonacorsi, S.; Levy, C. A 13-year survey of pneumococcal nasopharyngeal carriage in children with acute otitis media following PCV7 and PCV13 implementation. Vaccine 2015, 33, 5118–5126. [Google Scholar] [CrossRef] [PubMed]
- Klugman, K.P.; Rodgers, G.L. Time for a third-generation pneumococcal conjugate vaccine. Lancet Infect. Dis. 2021, 21, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.M.; Hashiguchi, T.C.O.; Cecchini, M. Impact of vaccination on carriage of and infection by antibiotic-resistant bacteria: A systematic review and meta-analysis. Clin. Exp. Vaccine Res. 2021, 10, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Sempere, J.; González-Camacho, F.; Domenech, M.; Llamosí, M.; Del Río, I.; López-Ruiz, B.; Gimeno, M.; Coronel, P.; Yuste, J. A national longitudinal study evaluating the activity of cefditoren and other antibiotics against non-susceptible Streptococcus pneumoniae strains during the period 2004–20 in Spain. J. Antimicrob. Chemother. 2022, 77, 1045–1051. [Google Scholar] [CrossRef] [PubMed]
- Santé Publique France. Données de Couverture Vaccinale Pneumocoque par Groupe D’Âge. Available online: https://www.santepubliquefrance.fr/determinants-de-sante/vaccination/articles/donnees-de-couverture-vaccinale-pneumocoque-par-groupe-d-age (accessed on 4 May 2023).
- Desmet, S.; Wouters, I.; Van Heirstraeten, L.; Beutels, P.; Van Damme, P.; Malhotra-Kumar, S.; Maes, P.; Verhaegen, J.; Peetermans, W.E.; Lagrou, K.; et al. In-depth analysis of pneumococcal serotypes in Belgian children (2015–2018): Diversity, invasive disease potential, and antimicrobial susceptibility in carriage and disease. Vaccine 2021, 39, 372–379. [Google Scholar] [CrossRef]
- DREES. La Part des Enfants de Moins de 3 ans Confiés Principalement à Une Assistante Maternelle ou Une Crèche a Presque Doublé Entre 2002 et 2021. Available online: https://drees.solidarites-sante.gouv.fr/publications-communique-de-presse/etudes-et-resultats/la-part-des-enfants-de-moins-de-3-ans-confies (accessed on 4 May 2023).
- Prins-van Ginkel, A.C.; Bruijning-Verhagen, P.C.; Uiterwaal, C.S.; van der Ent, C.K.; Smit, H.A.; de Hoog, M.L. Acute Otitis Media During Infancy: Parent-reported Incidence and Modifiable Risk Factors. Pediatr. Infect. Dis. J. 2017, 36, 245–249. [Google Scholar] [CrossRef]
- Greenberg, D.; Hoffman, S.; Leibovitz, E.; Dagan, R. Acute otitis media in children: Association with day care centers--antibacterial resistance, treatment, and prevention. Paediatr. Drugs 2008, 10, 75–83. [Google Scholar] [CrossRef]
- Dagan, R.; O’Brien, K.L. Modeling the association between pneumococcal carriage and child-care center attendance. Clin. Infect. Dis. 2005, 40, 1223–1226. [Google Scholar] [CrossRef]
- Brueggemann, A.B.; Jansen van Rensburg, M.J.; Shaw, D.; McCarthy, N.D.; Jolley, K.A.; Maiden, M.C.J.; van der Linden, M.P.G.; Amin-Chowdhury, Z.; Bennett, D.E.; Borrow, R.; et al. Changes in the incidence of invasive disease due to Streptococcus pneumoniae, Haemophilus influenzae, and Neisseria meningitidis during the COVID-19 pandemic in 26 countries and territories in the Invasive Respiratory Infection Surveillance Initiative: A prospective analysis of surveillance data. Lancet Digit. Health 2021, 3, e360–e370. [Google Scholar]
- Rybak, A.; Levy, C.; Angoulvant, F.; Auvrignon, A.; Gembara, P.; Danis, K.; Vaux, S.; Levy-Bruhl, D.; van der Werf, S.; Béchet, S.; et al. Association of Nonpharmaceutical Interventions During the COVID-19 Pandemic With Invasive Pneumococcal Disease, Pneumococcal Carriage, and Respiratory Viral Infections Among Children in France. JAMA Netw. Open 2022, 5, e2218959. [Google Scholar] [CrossRef]
- Danino, D.; Ben-Shimol, S.; Van Der Beek, B.A.; Givon-Lavi, N.; Avni, Y.S.; Greenberg, D.; Weinberger, D.M.; Dagan, R. Decline in Pneumococcal Disease in Young Children during the COVID-19 Pandemic in Israel Associated with Suppression of seasonal Respiratory Viruses, despite Persistent Pneumococcal Carriage: A Prospective Cohort Study. Clin. Infect. Dis. 2022, 1, e1154–e1164. [Google Scholar] [CrossRef]
- Ouldali, N.; Deceuninck, G.; Lefebvre, B.; Gilca, R.; Quach, C.; Brousseau, N.; Tapiero, B.; De Wals, P. Increase of invasive pneumococcal disease in children temporally associated with RSV outbreak in Quebec: A time-series analysis. Lancet Reg. Health Am. 2023, 19, 100448. [Google Scholar] [CrossRef]
- Sempere, J.; Llamosí, M.; Ruiz, B.L.; Del Río, I.; Pérez-García, C.; Lago, D.; Gimeno, M.; Coronel, P.; González-Camacho, F.; Domenech, M.; et al. Effect of pneumococcal conjugate vaccines and SARS-CoV-2 on antimicrobial resistance and the emergence of Streptococcus pneumoniae serotypes with reduced susceptibility in Spain, 2004-20: A national surveillance study. Lancet Microbe 2022, 3, e744–e752. [Google Scholar] [CrossRef]
- Santé Publique France. Consommation D’antibiotiques et Prévention de L’antibiorésistance en France en 2021: Où en Sommes-nous? Available online: https://www.santepubliquefrance.fr/les-actualites/2022/consommation-d-antibiotiques-et-prevention-de-l-antibioresistance-en-france-en-2021-ou-en-sommes-nous (accessed on 4 May 2023).
- Cohen, R.; Levy, C.; Ouldali, N.; Goldrey, M.; Béchet, S.; Bonacorsi, S.; Varon, E. Invasive Disease Potential of Pneumococcal Serotypes in Children After PCV13 Implementation. Clin. Infect. Dis. 2021, 72, 1453–1456. [Google Scholar] [CrossRef] [PubMed]
- Varon, E.; Batah, J. Rapport D’activité 2021. Available online: https://cnr-pneumo.com/docman/rapports/58-2021-epidemiologie-2020/file (accessed on 4 May 2023).
- Lo, S.W.; Mellor, K.; Cohen, R.; Alonso, A.R.; Belman, S.; Kumar, N.; Hawkins, P.A.; Gladstone, R.A.; von Gottberg, A.; Veeraraghavan, B.; et al. Emergence of a multidrug-resistant and virulent Streptococcus pneumoniae lineage mediates serotype replacement after PCV13: An international whole-genome sequencing study. Lancet Microbe 2022, 3, e735–e743. [Google Scholar] [CrossRef]
- González-Díaz, A.; Machado, M.P.; Càmara, J.; Yuste, J.; Varon, E.; Domenech, M.; Del Grosso, M.; Marimón, J.M.; Cercenado, E.; Larrosa, N.; et al. Two multi-fragment recombination events resulted in the β-lactam-resistant serotype 11A-ST6521 related to Spain9V-ST156 pneumococcal clone spreading in south-western Europe, 2008 to 2016. Eurosurveillance 2020, 25, 1900457. [Google Scholar] [CrossRef]
- Levy, C.; Vie le Sage, F.; Varon, E.; Chalumeau, M.; Grimprel, E.; Cohen, R. Pediatric Ambulatory and Hospital Networks for Surveillance and Clinical Epidemiology of Community-Acquired Infections. J. Pediatr. 2018, 194, 269–270.e2. [Google Scholar] [CrossRef] [PubMed]
- Rybak, A.; Levy, C.; Bonacorsi, S.; Béchet, S.M.; le Sage, F.V.; Elbez, A.; Varon, E.; Cohen, R. Antibiotic Resistance of Potential Otopathogens Isolated From Nasopharyngeal Flora of Children With Acute Otitis Media Before, During and After Pneumococcal Conjugate Vaccines Implementation. Pediatr. Infect. Dis. J. 2018, 37, e72–e78. [Google Scholar] [CrossRef] [PubMed]
- Paradise, J.L. On classifying otitis media as suppurative or nonsuppurative, with a suggested clinical schema. J. Pediatr. 1987, 111 Pt 1, 948–951. [Google Scholar] [CrossRef]
- Faden, H.; Duffy, L.; Wasielewski, R.; Wolf, J.; Krystofik, D.; Tung, Y.; Pediatrics, T. Relationship between Nasopharyngeal Colonization and the Development of Otitis Media in Children. Tonawanda/Williamsville Pediatrics. J. Infect. Dis. 1997, 175, 1440–1445. [Google Scholar] [CrossRef]
- Revai, K.; Mamidi, D.; Chonmaitree, T. Association of Nasopharyngeal Bacterial Colonization during Upper Respiratory Tract Infection and the Development of Acute Otitis Media. Clin. Infect. Dis. 2008, 46, e34–e37. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_13.0_Breakpoint_Tables.pdf (accessed on 4 May 2023).
- Lee, H.; Cha, J.H.; Nahm, M.H.; Burton, R.L.; Kim, K.-H. The 7-valent pneumococcal conjugate vaccine elicits cross-functional opsonophagocytic killing responses to Streptococcus pneumoniae serotype 6D in children. BMC Infect. Dis. 2013, 13, 474. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Levy, C.; Bingen, E.; Koskas, M.; Nave, I.; Varon, E. Impact of 13-valent Pneumococcal Conjugate Vaccine on Pneumococcal Nasopharyngeal Carriage in Children With Acute Otitis Media. Pediatr. Infect. Dis. J. 2012, 31, 297–301. [Google Scholar] [CrossRef] [PubMed]
- van Selm, S.; van Cann, L.M.; Kolkman, M.A.B.; van der Zeijst, B.A.M.; van Putten, J.P.M. Genetic Basis for the Structural Difference between Streptococcus pneumoniae Serotype 15B and 15C Capsular Polysaccharides. Infect. Immun. 2003, 71, 6192–6198. [Google Scholar] [CrossRef] [PubMed]
- Ouldali, N.; Varon, E.; Levy, C.; Angoulvant, F.; Georges, S.; Ploy, M.-C.; Kempf, M.; Cremniter, J.; Cohen, R.; Bruhl, D.L.; et al. Invasive pneumococcal disease incidence in children and adults in France during the pneumococcal conjugate vaccine era: An interrupted time-series analysis of data from a 17-year national prospective surveillance study. Lancet Infect. Dis. 2021, 21, 137–147. [Google Scholar] [CrossRef]
- Jandoc, R.; Burden, A.M.; Mamdani, M.; Lévesque, L.E.; Cadarette, S.M. Interrupted time series analysis in drug utilization research is increasing: Systematic review and recommendations. J. Clin. Epidemiol. 2015, 68, 950–956. [Google Scholar] [CrossRef]
- Ouldali, N.; Cohen, R.; Levy, C.; Gelbert-Baudino, N.; Seror, E.; Corrard, F.; Le Sage, F.V.; Michot, A.-S.; Romain, O.; Bechet, S.; et al. Pneumococcal susceptibility to antibiotics in carriage: A 17 year time series analysis of the adaptive evolution of non-vaccine emerging serotypes to a new selective pressure environment. J. Antimicrob. Chemother. 2019, 74, 3077–3086. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Data on Country Response Measures to COVID-19. Available online: https://www.ecdc.europa.eu/en/publications-data/download-data-response-measures-covid-19 (accessed on 4 May 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Periods | Pre-PCV7 n = 943 | Targeted PCV7 n = 2314 | PCV7 n = 3458 | Early PCV13 n = 3677 | Late PCV13 n = 6744 | Total n = 17,136 |
|---|---|---|---|---|---|---|
| Male, n (%) | 524 (55.6) | 1225 (52.9) | 1833 (53.0) | 1972 (53.6) | 3605 (53.4) | 9159 (53.4) |
| Age (months), median (IQR) | 13.1 (9.4–17.6) | 12.9 (9.3–17.5) | 12.7 (9.4–17.2) | 13.0 (9.5–17.5) | 12.6 (9.2–17.2) | 12.8 (9.3–17.3) |
| Daycare attendance, n (%) | 316 (33.5) | 764 (33.0) | 1416/3455 (41.0) | 1769 (48.1) | 3982/6741 (59.1) | 8247/17,130 (48.1) |
| Siblings, n (%) | 510 (54.1) | 1369 (59.2) | 1949/3457 (56.4) | 2057 (55.9) | 3878/6743 (57.5) | 9763/17,134 (9763) |
| Otalgia, n (%) | 811 (86.0) | 1954 (84.4) | 2565/3455 (74.2) | 2668 (72.6) | 4444/6727 (66.1) | 12,442/17,116 (72.7) |
| Fever (≥38.5 °C), n (%) | 775/775 (100.0) | 1968/1986 (99.1) | 2047/3429 (59.7) | 2041/3646 (56.0) | 3538/6646 (53.2) | 10,369/16,482 (62.9) |
| Conjunctivitis, n (%) | NA | NA | 872/3447 (25.3) | 1048 (28.5) | 1847/6740 (27.4) | 3767/13,864 (27.2) |
| Otorrhea, n (%) | 101 (10.7) | 240 (10.4) | 293/3458 (8.5) | 256 (7.0) | 498/6741 (7.4) | 1388/17,133 (8.1) |
| Bilateral AOM, n (%) | NA | NA | 482/886 (54.4) | 1844 (50.1) | 3063/6738 (45.5) | 5389/11,301 (47.7) |
| History of AOM, n (%) | NA | NA | 983/1755 (56.0) | 2209 (55.2) | 3363 (49.9) | 6375/12,176 (52.4) |
| Otitis prone children, n (%) | NA | NA | 342/1755 (19.5) | 644/3677 (17.5) | 985/6743 (14.6) | 1971/12,175 (16.2) |
| Recent use of antibiotics, n (%) | 448 (47.2) | 964 (41.7) | 1634/3455 (47.3) | 1575/3676 (42.8) | 2451/7743 (36.3) | 7069/17,131 (41.3) |
| Broad-spectrum antibiotics, n (%) | 375/442 (84.8) | 580/959 (88.6) | 1512/1629 (92.8) | 974/1571 (62.0) | 793/2433 (32.6) | 4504/7034 (64.0) |
| Periods | Pre-PCV7 n = 943 | Targeted PCV7 n = 2314 | PCV7 n = 3458 | Early PCV13 n = 3677 | Late PCV13 n = 6744 | Total n = 17,136 |
|---|---|---|---|---|---|---|
| Pneumococcal carriage | 672 (71.3) | 1418 (61.3) | 1990 (57.5) | 1984 (54.0) | 3775 (56.0) | 9839 (57.4) |
| Monthly trend (95% CI) | −0.49% (−1.22 to +0.24), p = 0.18 | −0.11% (−0.34 to +0.12), p = 0.35 | −0.03% (−0.17 to +0.11), p = 0.66 | −0.08% (−0.64 to +0.48), p = 0.78 | +0.05% (−0.04 to +0.14), p = 0.29 | |
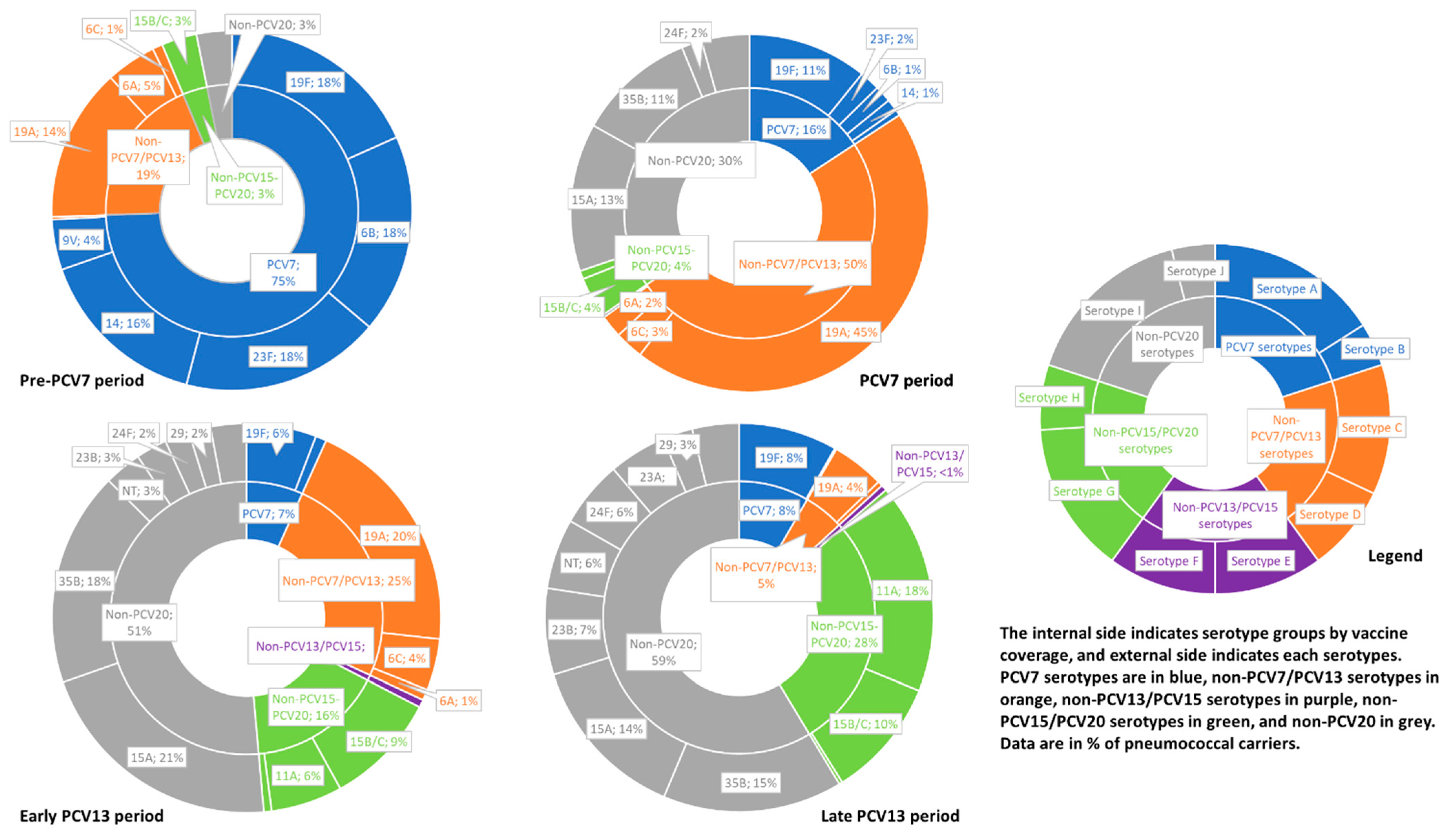
| PCV7 serotypes | 421 (44.6) | 565 (24.4) | 193 (5.6) | 64 (1.7) | 132 (2.0) | 1375 (8.0) |
| PCV13 + 6C serotypes | 585 (62.0) | 984 (42.5) | 925 (26.7) | 387 (10.5) | 306 (4.5) | 3187 (18.6) |
| 6 additional serotypes + serotype 6C | 164 (17.4) | 419 (18.1) | 732 (21.2) | 323 (8.8) | 174 (2.6) | 1812 (10.6) |
| PCV15 serotypes | 590 (87.8) | 1036 (73.1) | 985 (49.5) | 477 (24.0) | 456 (12.1) | 3544 (36.0) |
| PCV20 serotypes | 620 (92.3) | 1160 (81.8) | 1247 (62.7) | 986 (49.7) | 1565 (41.5) | 5578 (56.7) |
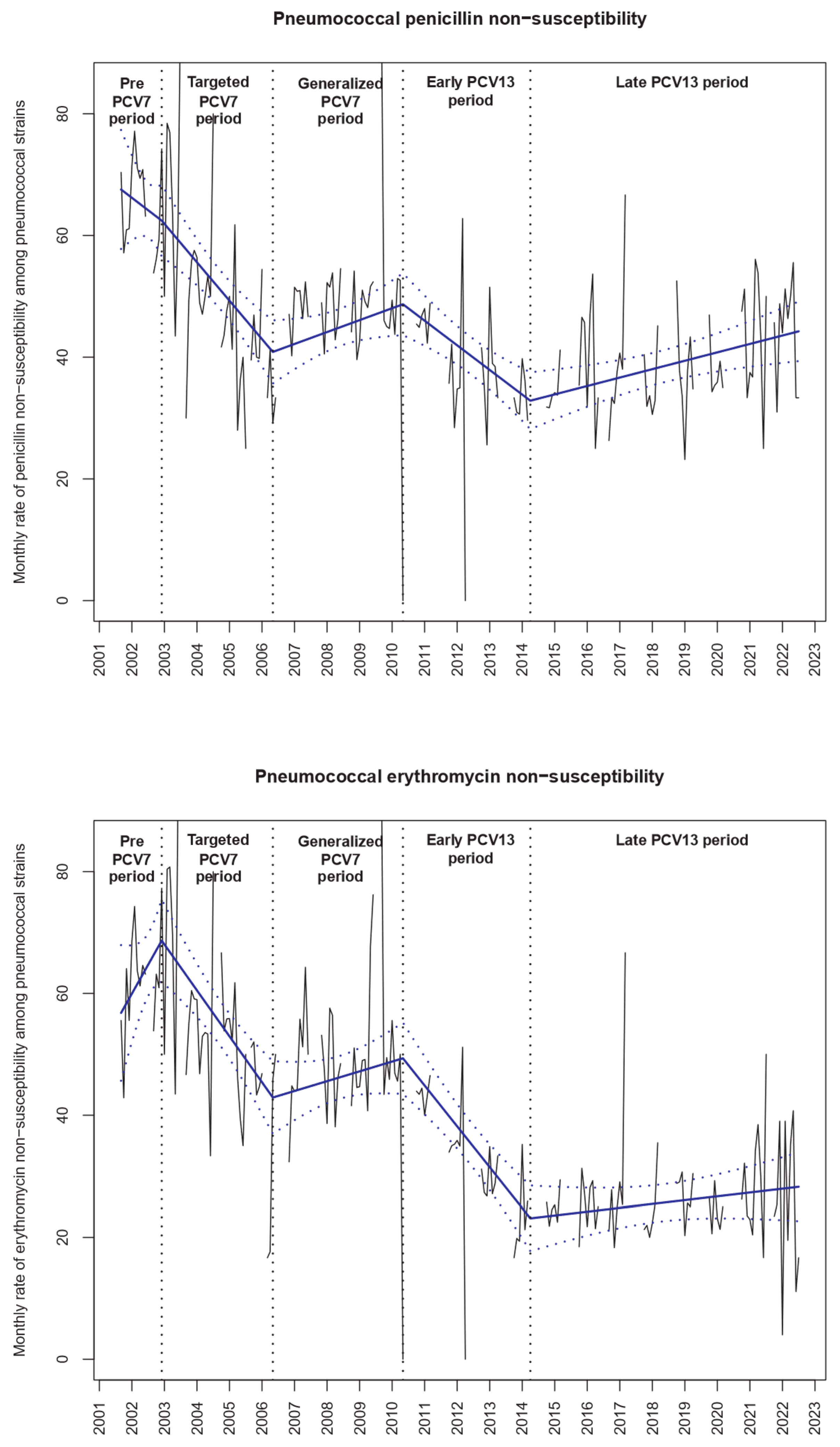
| Penicillin non-susceptible strains | 442/671 (65.9) | 687/1414 (48.6) | 944/1987 (47.5) | 774/1983 (39.0) | 1439/3776 (38.1) | 4286/9831 (43.6) |
| Monthly trend (95% CI) | −0.24% (−0.85 to +0.36), p = 0.41 | −0.31% (−1.92 to +1.31), p = 0.70 | +0.18% (+0.09 to +0.27), p < 0.001 | −0.41% (−0.66 to −0.16), p = 0.001 | +0.15% (+0.08 to 0.22), p < 0.001 | |
| Penicillin resistant strains | 8/671 (1.2) | 7/1414 (0.5) | 3/1987 (0.1) | 10/1983 (0.5) | 18/2337 (0.5) | 46/9831 (0.5) |
| Erythromycin non-susceptible strains | 423/672 (62.9) | 749/1415 (52.9) | 969/1987 (48.8) | 663/1984 (33.4) | 956/3776 (25.3) | 3760/9834 (38.2) |
| Monthly trend (95% CI) | +0.63% (−0.12 to +1.39), p = 0.09 | −0.56% (−1.00 to −0.12), p = 0.01 | +0.14% (+0.07 to +0.22), p < 0.001 | −0.78% (−1.16 to −0.39), p < 0.001 | +0.10% (+0.06 to +0.14), p < 0.001 | |
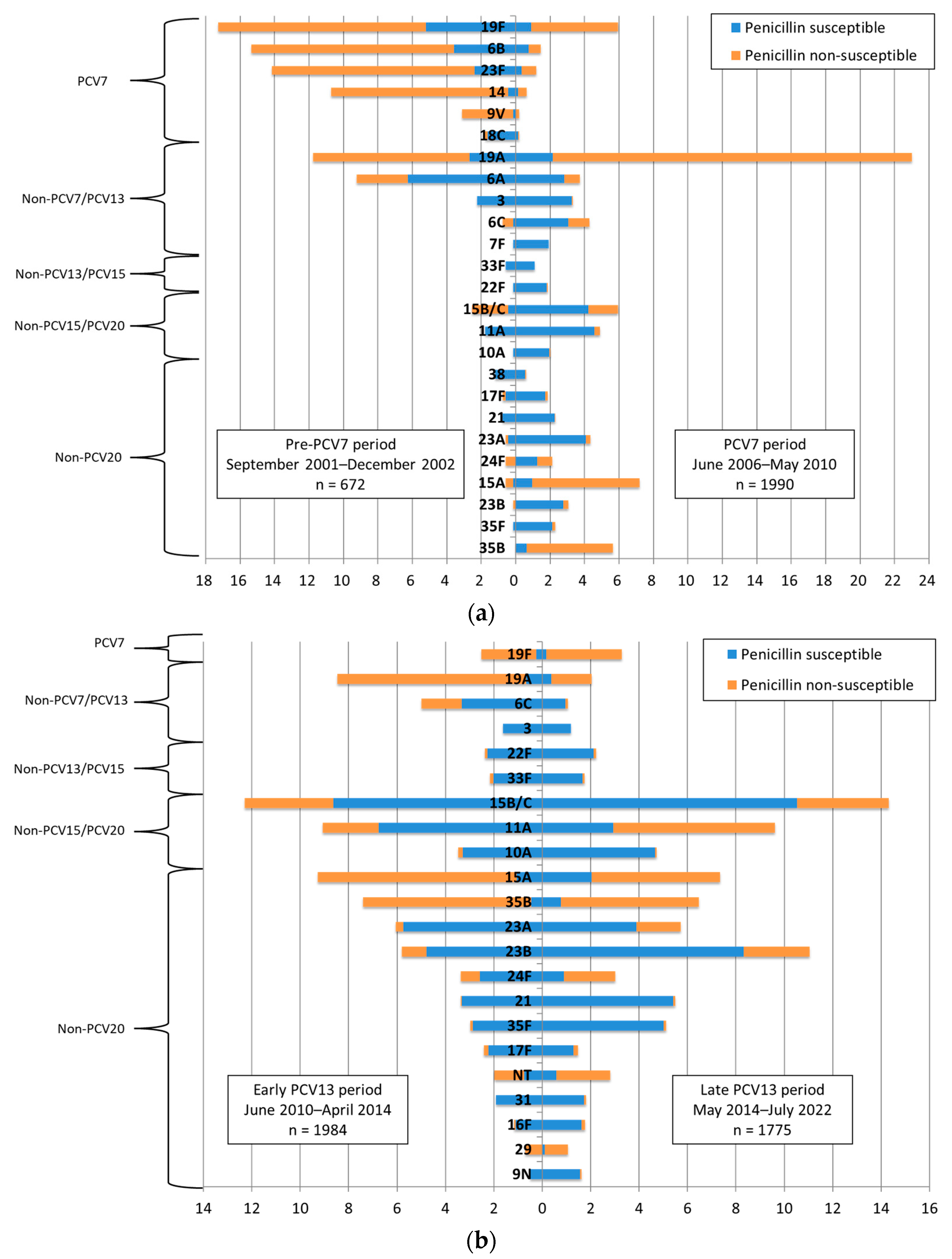
| Most frequent serotypes | 19F, 116 (17.3) | 19F, 235 (16.6) | 19A, 458 (23.0) | 15B/C, 244 (12.3) | 15B/C, 540 (14.3) | 15B/C, 978 (9.9) |
| 6B, 103 (15.3) | 19A, 190 (13.4) | 15A, 143 (7.2) | 15A, 184 (9.3) | 23B, 417 (11.0) | 19A, 973 (9.9) | |
| 23F, 95 (14.1) | 23F, 109 (7.7) | 15B/C, 118 (5.9) | 11A, 180 (9.1) | 11A, 363 (9.6) | 11A, 697 (7.1) | |
| 19A, 79 (11.8) | 6B, 108 (7.6) | 19F, 118 (5.9) | 19A, 169 (8.5) | 15A, 278 (7.4) | 19F, 643 (6.5) | |
| 14, 72 (10.7) | 3, 90 (6.3) | 35B, 112 (5.6) | 35B, 147 (7.4) | 35B, 244 (6.5) | 15A, 639 (6.5) | |
| Most frequent penicillin non-susceptible serotypes | 19F, 81 (18.3) | 19A, 172 (25.0) | 19A, 414 (43.9) | 15A, 163 (21.1) | 11A, 252 (17.5) | 19A, 865 (20.2) |
| 23F, 79 (17.9) | 19F, 162 (23.6) | 15A, 124 (13.1) | 19A, 155 (20.0) | 35B, 215 (14.9) | 15A, 515 (12.0) | |
| 6B, 79 (17.9) | 23F, 92 (13.4) | 19F, 120 (10.6) | 35B, 138 (17.8) | 15A, 200 (13.9) | 19F, 506 (11.8) | |
| 14, 69 (15.6) | 6B, 68 (9.9) | 35B, 99 (10.5) | 15B/C, 73 (9.4) | 15B/C, 143 (9.9) | 35B, 462 (10.8) | |
| 19A, 61 (13.8) | 14, 51 (7.4) | 15B/C, 34 (3.6) | 11A, 46 (5.9) | 19F, 118 (8.2) | 11A, 305 (7.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rybak, A.; Levy, C.; Ouldali, N.; Bonacorsi, S.; Béchet, S.; Delobbe, J.-F.; Batard, C.; Donikian, I.; Goldrey, M.; Assouline, J.; et al. Dynamics of Antibiotic Resistance of Streptococcus pneumoniae in France: A Pediatric Prospective Nasopharyngeal Carriage Study from 2001 to 2022. Antibiotics 2023, 12, 1020. https://doi.org/10.3390/antibiotics12061020
Rybak A, Levy C, Ouldali N, Bonacorsi S, Béchet S, Delobbe J-F, Batard C, Donikian I, Goldrey M, Assouline J, et al. Dynamics of Antibiotic Resistance of Streptococcus pneumoniae in France: A Pediatric Prospective Nasopharyngeal Carriage Study from 2001 to 2022. Antibiotics. 2023; 12(6):1020. https://doi.org/10.3390/antibiotics12061020
Chicago/Turabian StyleRybak, Alexis, Corinne Levy, Naïm Ouldali, Stéphane Bonacorsi, Stéphane Béchet, Jean-François Delobbe, Christophe Batard, Isabelle Donikian, Marie Goldrey, Jessica Assouline, and et al. 2023. "Dynamics of Antibiotic Resistance of Streptococcus pneumoniae in France: A Pediatric Prospective Nasopharyngeal Carriage Study from 2001 to 2022" Antibiotics 12, no. 6: 1020. https://doi.org/10.3390/antibiotics12061020