
Molecular Epidemiology of Extended-Spectrum Beta-Lactamase and AmpC Producing Enterobacteriaceae among Sepsis Patients in Ethiopia: A Prospective Multicenter Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Sociodemographic Characteristics
2.2. Enterobacteriaceae: Frequencies and Distributions per Study Site
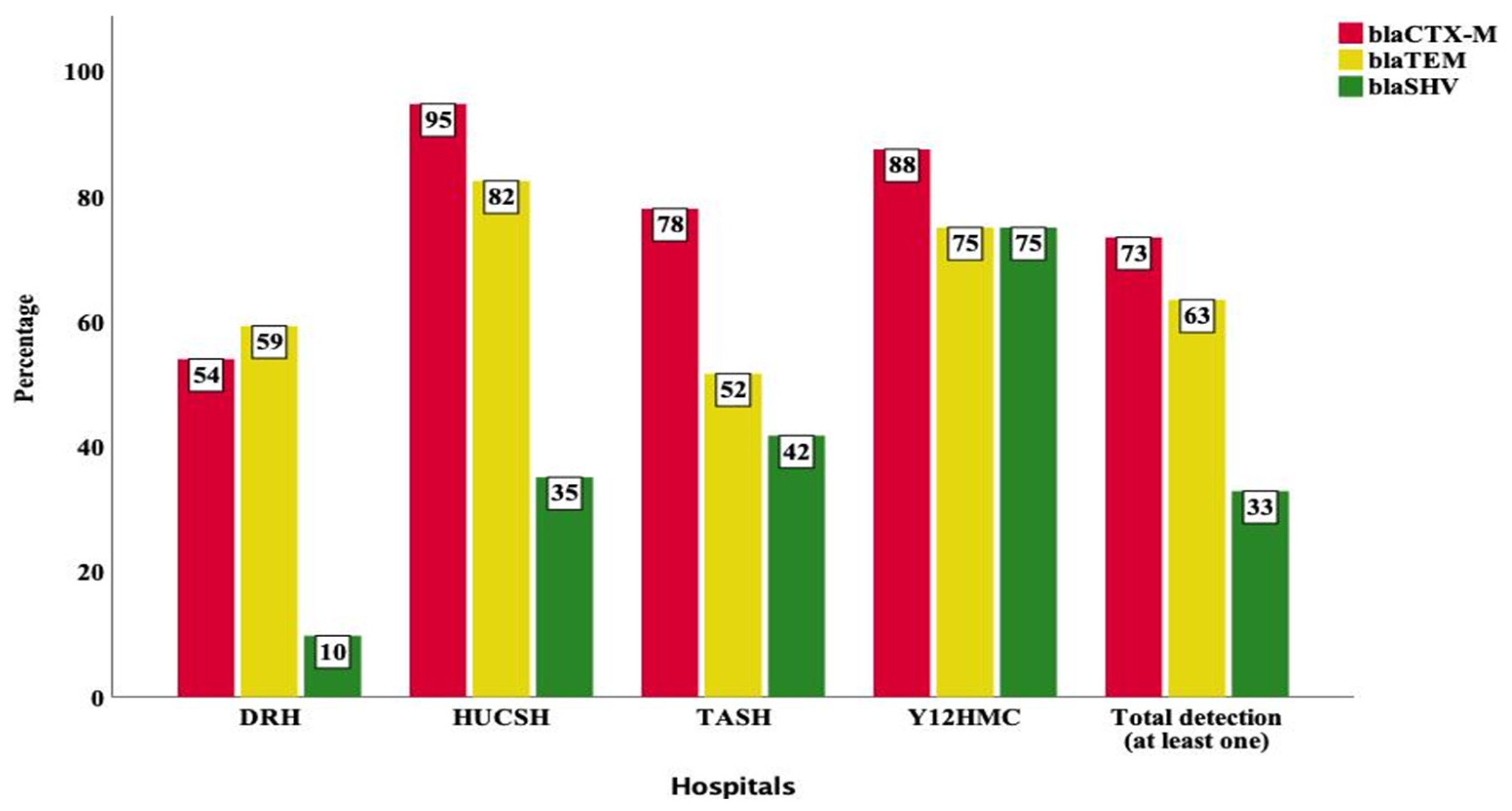
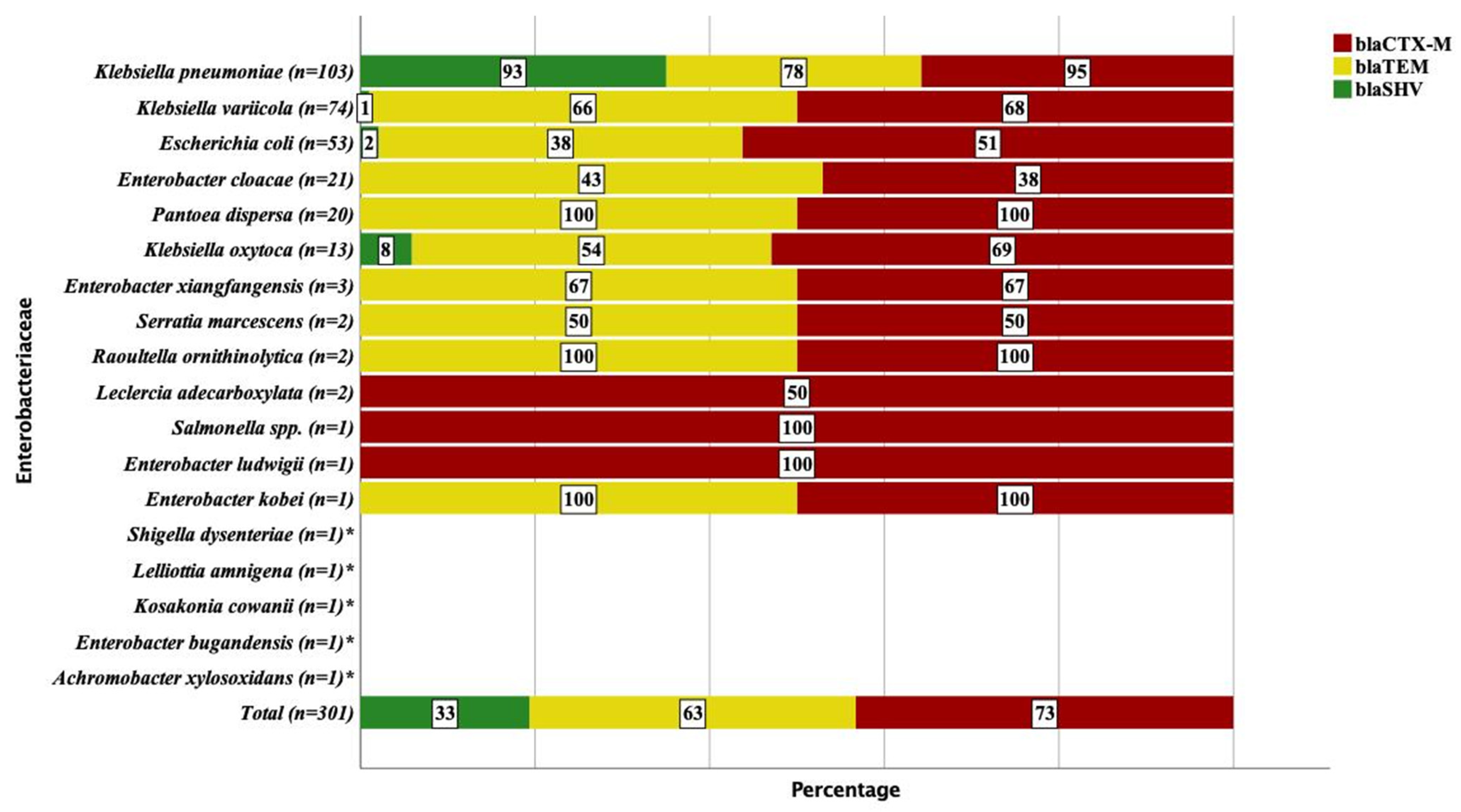
2.3. Detection of blaCTX-M, blaTEM and blaSHV Genes
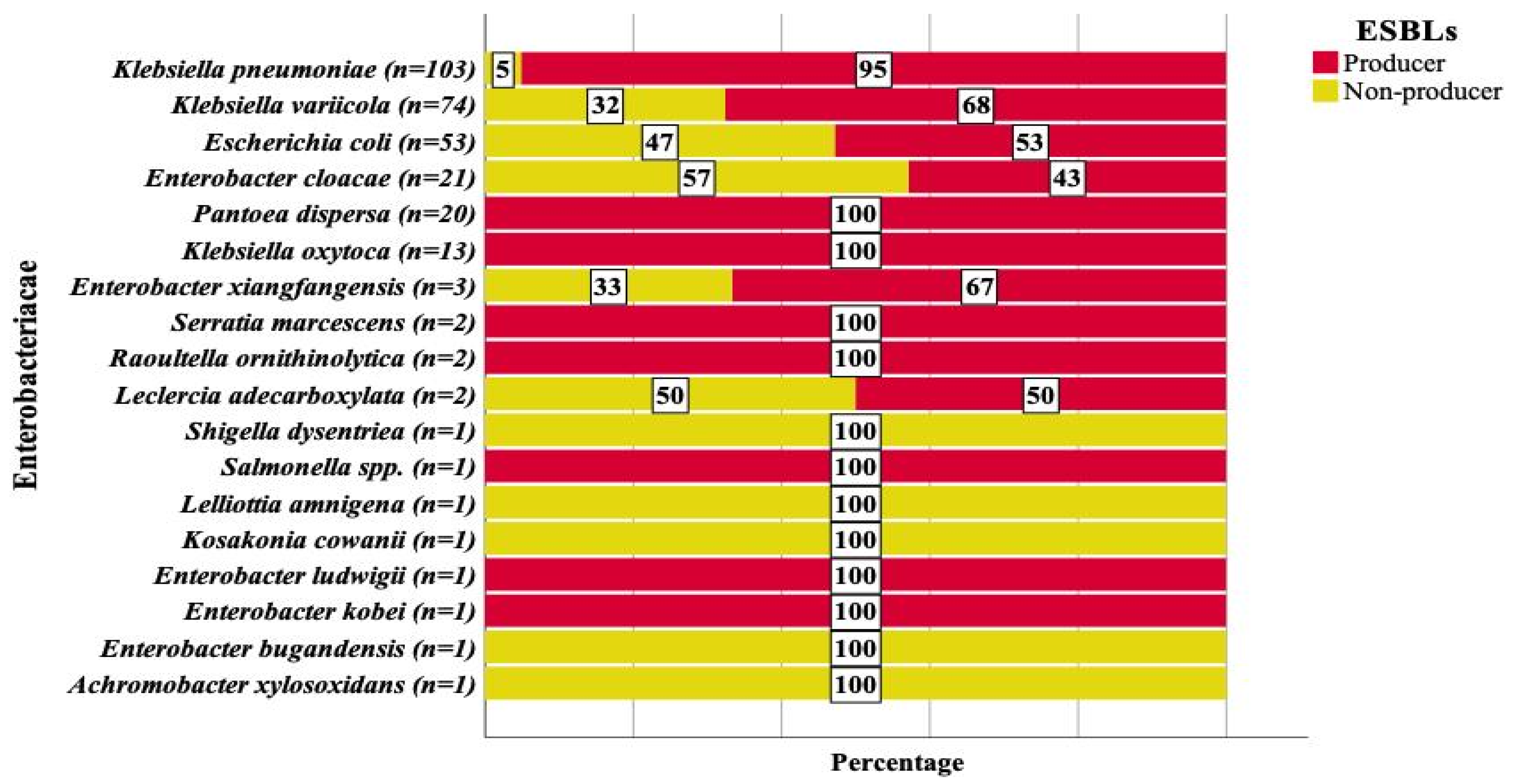
2.4. Molecular Epidemiology of ESBL Producing Enterobacteriaceae
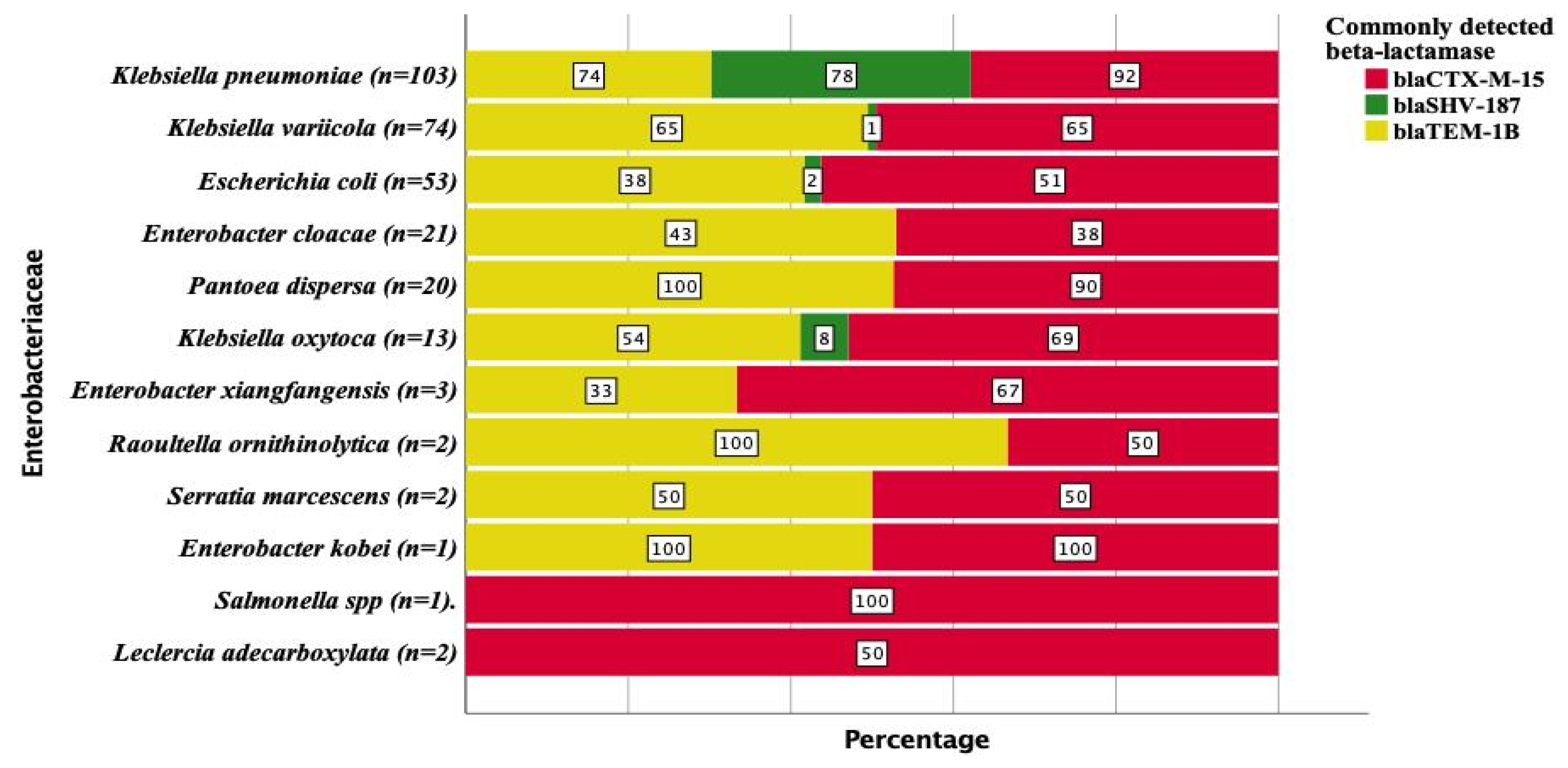
2.5. ESBL Genes
2.6. Non-ESBL β-Lactamase Variants of blaTEM and blaSHV
2.7. Co-Occurrence of Multiple ESBL Genes
2.8. Molecular Epidemiology of AmpC Producing Enterobacteriaceae
3. Discussion
4. Materials and Methods
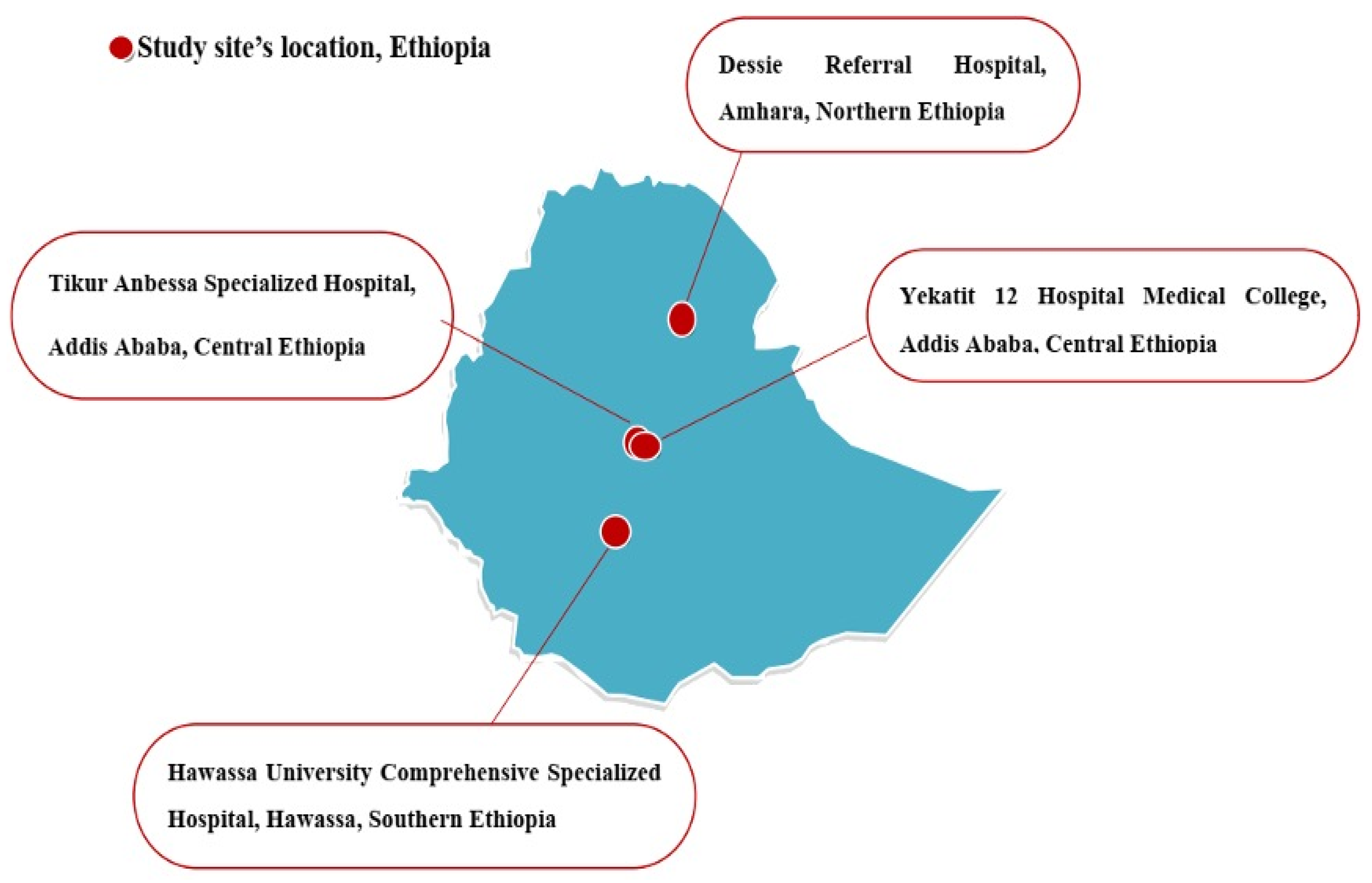
4.1. Study Design and Study Sites
4.2. Blood Culture and Enterobacteriaceae Isolation and Identification
4.3. DNA Extraction, Whole Genome Sequencing (WGS) and the Identification of Resistance Genes
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vlieghe, E.R.; Huang, T.D.; Phe, T.; Bogaerts, P.; Berhin, C.; De Smet, B.; Peetermans, W.E.; Jacobs, J.A.; Glupczynski, Y. Prevalence and distribution of beta-lactamase coding genes in third-generation cephalosporin-resistant Enterobacteriaceae from bloodstream infections in Cambodia. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Rhee, C.; Jones, T.M.; Hamad, Y.; Pande, A.; Varon, J.; O’Brien, C.; Anderson, D.J.; Warren, D.K.; Dantes, R.B.; Epstein, L.; et al. Prevalence, Underlying Causes, and Preventability of Sepsis-Associated Mortality in US Acute Care Hospitals. JAMA Netw. Open 2019, 2, e187571. [Google Scholar] [CrossRef] [PubMed]
- Sakellariou, C.; Gürntke, S.; Steinmetz, I.; Kohler, C.; Pfeifer, Y.; Gastmeier, P.; Schwab, F.; Kola, A.; Deja, M.; Leistner, R. Sepsis Caused by Extended-Spectrum Beta-Lactamase (ESBL)-Positive K. pneumoniae and E. coli: Comparison of Severity of Sepsis, Delay of Anti-Infective Therapy and ESBL Genotype. PLoS ONE 2016, 11, e0158039. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-L.; Huang, F.-Y.; Gan, L.-L.; Yu, X.; Cai, D.-J.; Fang, J.; Zhong, Z.-J.; Guo, H.-R.; Xie, Y.; Yi, J.; et al. High prevalence of blaCTX m and blaSHV among ESBL producing E. coli isolates from beef cattle in China’s Sichuan-Chongqing Circle. Sci. Rep. 2021, 11, 13725. [Google Scholar] [CrossRef]
- Ben Said, L.; Jouini, A.; Klibi, N.; Dziri, R.; Alonso, C.A.; Boudabous, A.; Ben Slama, K.; Torres, C. Detection of extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae in vegetables, soil and water of the farm environment in Tunisia. Int. J. Food Microbiol. 2015, 203, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Ejaz, H.; Younas, S.; Abosalif, K.O.A.; Junaid, K.; Alzahrani, B.; Alsrhani, A.; Abdalla, A.E.; Ullah, M.I.; Qamar, M.U.; Hamam, S.S.M. Molecular analysis of blaSHV, blaTEM, and blaCTX m in extended-spectrum β-lactamase producing Enterobacteriaceae recovered from fecal specimens of animals. PLoS ONE 2021, 16, e0245126. [Google Scholar] [CrossRef] [PubMed]
- Haghighifar, E.; Norouzi, F.; Kamali Dolatabadi, R. Molecular detection of Extended-Spectrum β-lactamases (ESBLs) and biofilm formation in uropathogen Klebsiella pneumoniae in Iran. Med. J. Islamic Repub. Iran. 2021, 35, 72. [Google Scholar] [CrossRef]
- Mosqueda-Gómez, J.L.; Montaño-Loza, A.; Rolón, A.L.; Cervantes, C.; Bobadilla-Del-Valle, J.M.; Silva-Sánchez, J.; Garza-Ramos, U.; Villasís-Keever, A.; Galindo-Fraga, A.; Palacios, G.M.R.; et al. Molecular epidemiology and risk factors of bloodstream infections caused by extended-spectrum β-lactamase-producing Klebsiella pneumoniae. Int. J. Infect. Dis. 2008, 12, 653–659. [Google Scholar] [CrossRef]
- Gürntke, S.; Kohler, C.; Steinmetz, I.; Pfeifer, Y.; Eller, C.; Gastmeier, P.; Schwab, F.; Leistner, R. Molecular epidemiology of extended-spectrum beta-lactamase (ESBL)-positive Klebsiella pneumoniae from bloodstream infections and risk factors for mortality. J. Infect. Chemother. 2014, 20, 817–819. [Google Scholar] [CrossRef]
- Hussain, H.I.; Aqib, A.I.; Seleem, M.N.; Shabbir, M.A.; Hao, H.; Iqbal, Z.; Kulyar, M.F.-E.A.; Zaheer, T.; Li, K. Genetic basis of molecular mechanisms in β-lactam resistant Gram-negative bacteria. Microb. Pathog. 2021, 158, 105040. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Sobur, M.A.; Rahman, S.; Ballah, F.M.; Ievy, S.; Siddique, M.P.; Rahman, M.; Kafi, M.A.; Rahman, M.T. Detection of blaTEM, blaCTX-M, blaCMY, and blaSHV Genes Among Extended-Spectrum Beta-Lactamase-Producing Escherichia coli Isolated from Migratory Birds Travelling to Bangladesh. Microb. Ecol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Akpaka, P.E.; Vaillant, A.; Wilson, C.; Jayaratne, P. Extended Spectrum Beta-Lactamase (ESBL) Produced by Gram-Negative Bacteria in Trinidad and Tobago. Int. J. Microbiol. 2021, 2021, 5582755. [Google Scholar] [CrossRef] [PubMed]
- Eger, E.; Heiden, S.E.; Korolew, K.; Bayingana, C.; Ndoli, J.M.; Sendegeya, A.; Gahutu, J.B.; Kurz, M.S.E.; Mockenhaupt, F.P.; Müller, J.; et al. Circulation of Extended-Spectrum Beta-Lactamase-Producing Escherichia coli of Pandemic Sequence Types 131, 648, and 410 among Hospitalized Patients, Caregivers, and the Community in Rwanda. Front. Microbiol. 2021, 12, 662575. [Google Scholar] [CrossRef] [PubMed]
- Tanır Basaranoglu, S.; Ozsurekci, Y.; Aykac, K.; Karadag Oncel, E.; Bıcakcigil, A.; Sancak, B.; Cengiz, A.B.; Kara, A.; Ceyhan, M. A comparison of blood stream infections with extended spectrum beta-lactamase-producing and non-producing Klebsiella pneumoniae in pediatric patients. Ital. J. Pediatr. 2017, 43, 79. [Google Scholar] [CrossRef]
- El Shamy, A.A.; Zakaria, Z.; Tolba, M.M.; Salah Eldin, N.; Rabea, A.-T.; Tawfick, M.M.; Nasser, H.A. AmpC β-Lactamase Variable Expression in Common Multidrug-Resistant Nosocomial Bacterial Pathogens from a Tertiary Hospital in Cairo, Egypt. Int. J. Microbiol. 2021, 2021, 6633888. [Google Scholar] [CrossRef]
- Cardoso, O.; Osorio, S.; Ramos, F.; Donato, M.M. Plasmid-Encoded AmpC and Extended-Spectrum Beta-Lactamases in Multidrug-Resistant Escherichia coli Isolated from Piglets in Portugal. Microb. Drug Resist. 2021, 27, 1742–1749. [Google Scholar] [CrossRef]
- Mahalleh, R.G.D.; Kazemi-Pour, N.; Rokhbakhsh-Zamin, F. Phenotypic and Molecular Characterization of AmpC beta-Lactamases among Escherichia coli a Prospective Study in Southeast Iran. Clin. Lab. 2021, 67. [Google Scholar] [CrossRef] [PubMed]
- Kazi, M.; Ajbani, K.; Tornheim, J.A.; Shetty, A.; Rodrigues, C. Multiplex PCR to detect pAmpC β-lactamases among Enterobacteriaceae at a tertiary care laboratory in Mumbai, India. Microbiology 2019, 165, 246–250. [Google Scholar] [CrossRef]
- Estaleva, C.E.L.; Zimba, T.F.; Sekyere, J.O.; Govinden, U.; Chenia, H.Y.; Simonsen, G.S.; Haldorsen, B.; Essack, S.Y.; Sundsfjord, A. High prevalence of multidrug resistant ESBL- and plasmid mediated AmpC-producing clinical isolates of Escherichia coli at Maputo Central Hospital, Mozambique. BMC Infect. Dis. 2021, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Cameron, A.; Mangat, R.; Mostafa, H.H.; Taffner, S.; Wang, J.; Dumyati, G.; Stanton, R.A.; Daniels, J.B.; Campbell, D.; Lutgring, J.D.; et al. Detection of CTX-M-27 β-Lactamase Genes on Two Distinct Plasmid Types in ST38 Escherichia coli from Three U.S. States. Antimicrob. Agents Chemother. 2021, 65, e0082521. [Google Scholar] [CrossRef]
- Xia, S.; Fan, X.; Huang, Z.; Xia, L.; Xiao, M.; Chen, R.; Xu, Y.; Zhuo, C. Dominance of CTX-M-Type Extended-Spectrum β-Lactamase (ESBL)-Producing Escherichia coli Isolated from Patients with Community-Onset and Hospital-Onset Infection in China. PLoS ONE 2014, 9, e100707. [Google Scholar] [CrossRef]
- Sangare, S.A.; Maiga, A.I.; Guindo, I.; Maiga, A.; Camara, N.; Savadogo, S.; Diallo, S.; Bougoudogo, F.; Armand-Lefevre, L.; Andremont, A.; et al. Prevalence of extended-spectrum beta-lactamase-producing Enterobacteriaceae isolated from blood cultures in Africa. Médecine Mal. Infect. 2015, 45, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Dirar, M.H.; Bilal, N.E.; Ibrahim, M.E.; Hamid, M.E. Prevalence of extended-spectrum beta-lactamase (ESBL) and molecular detection of blaTEM, blaSHV and blaCTX m genotypes among Enterobacteriaceae isolates from patients in Khartoum, Sudan. Pan Afr. Med. J. 2020, 37, 213. [Google Scholar] [CrossRef] [PubMed]
- Akinbami, O.R.; Olofinsae, S.; Ayeni, F.A. Prevalence of extended spectrum beta lactamase and plasmid mediated quinolone resistant genes in strains of Klebsiella pneumonia, Morganella morganii, Leclercia adecarboxylata and Citrobacter freundii isolated from poultry in South Western Nigeria. PeerJ 2018, 6, e5053. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.N.A.; Ben Zakour, N.L.; Roberts, L.W.; Wailan, A.M.; Zowawi, H.M.; Tambyah, P.A.; Lye, D.C.; Jureen, R.; Lee, T.H.; Yin, M.; et al. Whole genome analysis of cephalosporin-resistant Escherichia coli from bloodstream infections in Australia, New Zealand and Singapore: High prevalence of CMY-2 producers and ST131 carrying blaCTX-M-15 and blaCTX-M-27. J. Antimicrob. Chemother. 2018, 73, 634–642. [Google Scholar] [CrossRef]
- Paramita, R.I.; Nelwan, E.J.; Fadilah, F.; Renesteen, E.; Puspandari, N.; Erlina, L. Genome-based characterization of Escherichia coli causing bloodstream infection through next-generation sequencing. PLoS ONE 2020, 15, e0244358. [Google Scholar] [CrossRef]
- Roer, L.; Hansen, F.; Thomsen, M.C.F.; Knudsen, J.D.; Hansen, D.S.; Wang, M.; Samulioniené, J.; Justesen, U.S.; Røder, B.L.; Schumacher, H.; et al. WGS-based surveillance of third-generation cephalosporin-resistant Escherichia coli from bloodstream infections in Denmark. J. Antimicrob. Chemother. 2017, 72, 1922–1929. [Google Scholar] [CrossRef]
- Bevan, E.R.; Jones, A.M.; Hawkey, P.M. Global epidemiology of CTX m β-lactamases: Temporal and geographical shifts in genotype. J. Antimicrob. Chemother. 2017, 72, 2145–2155. [Google Scholar] [CrossRef] [PubMed]
- Ogunbosi, B.O.; Moodley, C.; Naicker, P.; Nuttall, J.; Bamford, C.; Eley, B. Colonisation with extended spectrum beta-lactamase-producing and carbapenem-resistant Enterobacterales in children admitted to a paediatric referral hospital in South Africa. PLoS ONE 2020, 15, e0241776. [Google Scholar] [CrossRef] [PubMed]
- Wyres, K.L.; Nguyen, T.N.T.; Lam, M.M.C.; Judd, L.M.; Van Vinh Chau, N.; Dance, D.A.B.; Ip, M.; Karkey, A.; Ling, C.L.; Miliya, T.; et al. Genomic surveillance for hypervirulence and multi-drug resistance in invasive Klebsiella pneumoniae from South and Southeast Asia. Genome Med. 2020, 12. [Google Scholar] [CrossRef]
- Haider, M.H.; Ain, N.U.; Abrar, S.; Riaz, S. blaOXA, blaSHV-, and blaTEM- extended-spectrum β-lactamases in Gram-negative strains from burn patients in Lahore, Pakistan. J. Infect. Dev. Ctries. 2020, 14, 1410–1417. [Google Scholar] [CrossRef] [PubMed]
- Tamma, P.D.; Smith, T.T.; Adebayo, A.; Karaba, S.M.; Jacobs, E.; Wakefield, T.; Nguyen, K.; Whitfield, N.N.; Simner, P.J. Prevalence of bla (CTX-M) Genes in Gram-Negative Bloodstream Isolates across 66 Hospitals in the United States. J. Clin. Microbiol. 2021, 59, e00127-21. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Machado, E.; Ramos, H.; Peixe, L.; Novais, Â. Expansion of ESBL-producing Klebsiella pneumoniae in hospitalized patients: A successful story of international clones (ST15, ST147, ST336) and epidemic plasmids (IncR, IncFIIK). Int. J. Med. Microbiol. 2014, 304, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Yang, G.; Li, A.; Zong, L.; Dong, Z.; Lu, J.; Zhang, K.; Cheng, C.; Chang, Q.; Wu, X.; et al. Identification and molecular characterization of Escherichia coli blaSHV genes in a Chinese teaching hospital. Gene 2017, 600, 29–35. [Google Scholar] [CrossRef] [PubMed]
- GonzáLez-LóPez, J.J.; Coelho, A.; Larrosa, M.N.; Lavilla, S.; Bartolomé, R.; Prats, G. First Detection of Plasmid-Encoded bla OXY β-Lactamase. Antimicrob. Agents Chemother. 2009, 53, 3143–3146. [Google Scholar] [CrossRef] [PubMed]
- Nijhuis, R.H.T.; Oueslati, S.; Zhou, K.; Bosboom, R.W.; Rossen, J.W.A.; Naas, T. OXY-2-15, a novel variant showing increased ceftazidime hydrolytic activity. J. Antimicrob. Chemother. 2015, 70, 1429–1433. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Xiao, W.; Xu, Q. IncN1 ST7 Epidemic Plasmid Carrying blaIMP-4 in One ST85-Type Klebsiella oxytoca Clinical Isolate with Porin Deficiency. Infect. Drug Resist. 2021, 14, 3827–3835. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, E.M.; Hickey, R.; Hsu, T.; Betancourt Román, C.M.; Chen, J.; Schwager, R.; Kline, J.; Brown, G.Z.; Halden, R.U.; Huttenhower, C.; et al. Antimicrobial Chemicals Are Associated with Elevated Antibiotic Resistance Genes in the Indoor Dust Microbiome. Environ. Sci. Technol. 2016, 50, 9807–9815. [Google Scholar] [CrossRef]
- Piazza, A.; Comandatore, F.; Romeri, F.; Pagani, C.; Mattioni Marchetti, V.; Brilli, M.; Panelli, S.; Migliavacca, R.; Ridolfo, A.; Olivieri, P.; et al. Detection of ST1702 Escherichia coli blaNDM-5 and blaCMY-42 genes positive isolates from a Northern Italian hospital. New Microbiol. 2018, 41, 230–231. [Google Scholar] [PubMed]
- Komatsu, Y.; Kasahara, K.; Inoue, T.; Lee, S.-T.; Muratani, T.; Yano, H.; Kirita, T.; Mikasa, K. Molecular epidemiology and clinical features of extended-spectrum beta-lactamase- or carbapenemase-producing Escherichia coli bacteremia in Japan. PLoS ONE 2018, 13, e0202276. [Google Scholar] [CrossRef] [PubMed]
- Silago, V.; Kovacs, D.; Samson, H.; Seni, J.; Matthews, L.; Oravcová, K.; Lupindu, A.M.; Hoza, A.S.; Mshana, S.E. Existence of Multiple ESBL Genes among Phenotypically Confirmed ESBL Producing Klebsiella pneumoniae and Escherichia coli Concurrently Isolated from Clinical, Colonization and Contamination Samples from Neonatal Units at Bugando Medical Center, Mwanza, Ta. Antibiotics 2021, 10, 476. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic Data | Number of Patients | Percentage | |
|---|---|---|---|
| Hospitals | TASH | 501 | 35.4 |
| Y12HMC | 298 | 21 | |
| DRH | 301 | 21.3 | |
| HUCSH | 316 | 22.3 | |
| Gender | Male | 783 | 55.3 |
| Female | 633 | 44.7 | |
| Age category | <29 days | 586 | 41.4 |
| ≥30 days to ≤1 year | 256 | 18.1 | |
| 1–5 years | 135 | 9.5 | |
| 5–18 years | 158 | 11.2 | |
| ≥18 years | 281 | 19.8 | |
| Ward | EOPD | 104 | 7.3 |
| ICU | 38 | 2.7 | |
| Medical ward | 148 | 10.5 | |
| NICU | 596 | 42.1 | |
| Pediatrics | 497 | 35.1 | |
| Surgical ward | 33 | 2.3 | |
| Referral patient | Yes | 722 | 51 |
| No | 694 | 49 | |
| Previous admission | Yes | 299 | 21.1 |
| No | 1117 | 78.9 | |
| Hospital stay duration | 1 week | 828 | 58.5 |
| 2 weeks | 222 | 15.7 | |
| 3 weeks | 146 | 10.3 | |
| 4 weeks and above | 220 | 15.5 | |
| Underlying diseases | Yes | 665 | 47 |
| No | 751 | 53 | |
| Previous antibiotic treatment before recruitment to the study | Yes | 440 | 31.1 |
| No | 976 | 68.9 | |
| Fever | Up to 3 days | 687 | 64.4 |
| 4–6 days | 207 | 19.4 | |
| 7 days and above | 173 | 16.2 | |
| No | 349 | 24.6 | |
| Total | 1416 | 100 | |
| Enterobacteriaceae | DRH n (%) | TASH n (%) | HUCSH n (%) | Y12HMC n (%) |
|---|---|---|---|---|
| Klebsiella pneumoniae (n = 103) | 12(11) | 39(43) | 22(39) | 30(75) |
| Klebsiella variicola (n = 74) | 44(39) | 2(2) | 28(49) | - |
| Escherichia coli (n = 53) | 17(15) | 28(31) | 4(7) | 4(10) |
| Enterobacter cloacae (n = 21) | 10(9) | 6(7) | 1(2) | 4(10) |
| Pantoea dispersa (n = 20) | 20(18) | - | - | - |
| Klebsiella oxytoca (n = 13) | 5(4) | 6(7) | 1(2) | 1(3) |
| Enterobacter xiangfangensis (n = 3) | 3(3) | - | - | - |
| Raoultella ornithinolytica (n = 2) | 1(1) | 1(1) | - | - |
| Serratia marcescens (n = 2) | - | 2(2) | - | - |
| Leclercia adecarboxylata (n = 2) | - | 2(2) | - | - |
| Achromobacter xylosoxidans (n = 1) | - | - | 1(2) | - |
| Enterobacter bugandensis (n = 1) | - | 1(1) | - | - |
| Enterobacter kobei (n = 1) | - | 1(1) | - | - |
| Enterobacter ludwigii (n = 1) | - | 1(1) | - | - |
| Kosakonia cowanii (n = 1) | 1(1) | - | - | - |
| Lelliottia amnigena (n = 1) | - | 1(1) | - | - |
| Salmonella spp. (n = 1) | - | - | - | 1(3) |
| Shigella dysenteriae (n = 1) | - | 1(1) | - | - |
| Total (n = 301) | 113 | 91 | 57 | 40 |
| Patient Characteristics | ESBL | Odds Ratio | |||||
|---|---|---|---|---|---|---|---|
| Producer n (%) | Non-Producer n (%) | COR (95% CL) | p-Value | AOR (95%CL) | p-Value | ||
| Hospital | DRH (n = 113) | 63(55.8) | 50(44.2) | 0.140(0.047–0.420) | 0.001 | 0.111(0.031–0.403) | 0.001 |
| TASH (n = 91) | 75(82) | 16(18) | 0.521(0.162–1.671) | 0.273 | |||
| HUCSH (n = 57) | 54(95) | 3(5) | 0.200(0.422–9.472) | 0.382 | |||
| Y12HMC (n = 40) | 36(90) | 4(10) | Constant | ||||
| Gender | Male (n = 174) | 128(73.6) | 46(26.4) | 0.751(0.437–1.292) | 0.301 | ||
| Female (n = 127) | 100(78.7) | 27(21.3) | Constant | ||||
| Age category | ≤29 days (n = 187) | 137(73) | 50(27) | 1.534(0.739–3.184) | 0.250 | ||
| 30 days–≤1 year (n = 32) | 30(94) | 2(6) | 8.4(1.741–40.529) | 0.008 | 4.564(0.285–73.109) | ||
| >1–≤5 year (n = 21) | 18(86) | 3(14) | 3.360(0.840–13.441) | 0.087 | |||
| >5–<18 year (n = 22) | 18(82) | 4(18) | 2.520(0.711–8.934) | 0.152 | |||
| ≥18 years (n = 39) | 25(64) | 14(36) | Constant | ||||
| Ward | EOPD (n = 12) | 9(75) | 3(25) | 3.750(0.587–23.936) | 0.162 | ||
| ICU (n = 8) | 5(63) | 3(38) | 2.083(0.298–14.549) | 0.459 | |||
| Medical ward (n = 15) | 12(80) | 3(20) | 5.000(0.806–13.457) | 0.084 | |||
| NICU (n = 189) | 139(73.5) | 50(26.5) | 3.475(0.897–13.457) | 0.071 | |||
| Paediatrics (n = 68) | 59(87) | 9(13) | 8.194(1.846–36.366) | 0.006 | 3.722(0.209–66.238) | 0.371 | |
| Surgical ward (n = 9) | 4(44) | 5(56) | Constant | ||||
| Hospital stay duration | 1 week (n = 194) | 135(69.6) | 30.4) | 0.277(0.094–0.818) | 0.020 | 0.268(0.069–1.037) | 0.056 |
| 2 weeks (n = 37) | 33(89.2) | 4(10.8) | 0.808(0.164–3.989) | 0.794 | |||
| 3 weeks (n = 23) | 20(87) | 3(13) | Constant | ||||
| ≥4 weeks (n = 47) | 40(85.1) | 7(14.9) | 0.693(0.186–2.572) | 0.583 | |||
| Underlying diseases | Yes (n = 117) | 99(84.6) | 18(15.4) | 2.363(1.306–4.278) | 0.004 | 1.197(0.308–4.652) | 0.795 |
| No (n = 184) | 129(70.1) | 55(29.9) | Constant | ||||
| Previous hospitalization | Yes (48) | 38(79.2) | 10(20.8) | 1.267(0.597–2.689) | 0.538 | ||
| No (n = 253) | 190(75.1) | 63(24.9) | Constant | ||||
| Referred patient | Yes (n = 140) | 109(77.9) | 31(22.1) | ||||
| No (n = 161) | 119(73.9) | 42(26.1) | 1.252(0.735–2.131) | 0.409 | |||
| Previous antibiotic treatment history | Yes (n = 52) | 47(90.4) | 5(9.4) | 0.283(0.108–0.742) | 0.01 | 0.639(0.179–2.281) | 0.490 |
| No (n = 249) | 181(72.7) | 68(27.3) | Constant | ||||
| ESBL Genes | Total | Hospitals | ESBL Gene Harboring Enterobacteriaceae | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DRH n (%) | HUCSH n (%) | TASH n (%) | Y12HMC n (%) | K. pneumoniae n (%) | K. variicola n (%) | E. coli n (%) | E. cloacae n (%) | P. dispersa n (%) | K. oxytoca n (%) | E. xiangfangensis n (%) | S. marcescens n (%) | R. ornithinolytica n (%) | L. adecarboxylata n (%) | Salmonella spp. n (%) | E. kobei n (%) | ||
| blaCTX-M-15 | 212(70.4) * | 57(50.4) | 53(93) | 67(73.6) | 35(87.5) | 95(92) | 48(65) | 27(51) | 8(38) | 18(90) | 9(69) | 2(67) | 1(50) | 1(50) | 1(50) | 1(100) | 1(100) |
| blaCTX-M-3 | 3(1) | 3(2.7) | - | - | - | - | 2(3) | - | - | - | - | - | - | 1(50) | - | - | - |
| blaCTX-M-9 | 1(0.3) | 1(0.9) | - | - | - | - | - | - | - | 1(5) | - | - | - | - | - | - | - |
| blaSHV-106 | 11(3.7) | 5(4.4) | 1(1.8) | 5(5.5) | - | 11(11) | - | - | - | - | - | - | - | - | - | - | - |
| blaSHV-65 | 2(0.7) | - | - | - | 2(5) | 2(2) | - | - | - | - | - | - | - | - | - | - | - |
| blaSHV-12 | 1(0.3) | - | - | 1(1.1) | - | - | - | 1(2) | - | - | - | - | - | - | - | - | - |
| blaTEM-207 | 3(1) | 1(0.9) | - | 2(2.2) | - | 2(2) | - | - | - | 1(5) | - | - | - | - | - | - | - |
| blaOXY-1-2 | 4(1.3) | (1.8) | 1(1.8) | 1(1.1) | - | - | - | - | - | - | 4(31) | - | - | - | - | - | - |
| blaOXY-1-5 | 3(1) | - | - | 2(2.2) | 1(2.5) | - | - | - | - | - | 2(15) | - | - | 1(50) | - | - | - |
| blaOXY-1-3 | 2(0.7) | 1(0.9) | - | 1(1.1) | - | - | - | - | - | - | 2(15) | - | - | - | - | - | - |
| blaOXY-2-2 | 1(0.3) | - | - | 1(1.1) | - | - | - | - | - | - | 1(8) | - | - | - | - | - | - |
| blaOXY-2-7 | 1(0.3) | - | - | 1(1.1) | - | - | - | - | - | - | 1(8) | - | - | - | - | - | - |
| blaOXY-2-8 | 1(0.3) | 1(0.9) | - | - | - | - | - | - | - | - | 1(8) | - | - | - | - | - | - |
| blaOXY-4-1 | 1(0.3) | 1(0.9) | - | - | - | - | - | - | - | - | 1(8) | - | - | - | - | - | - |
| blaOXY-5-1 | 1(0.3) | - | - | 1(1.1) | - | - | - | - | - | - | 1(8) | - | - | - | - | - | - |
| blaSRT-1 | 2(0.7) | - | - | 2(2.2) | - | - | - | - | - | - | - | - | 2(100) | - | - | - | - |
| blaCMY-42 | 1(0.3) | - | - | 1(1.1) | - | - | - | 1(2) | - | - | - | - | - | - | - | - | - |
| blaGES-11 | 1(0.3) | - | - | - | 1(2.5) | - | - | - | 1(5) | - | - | - | - | - | - | - | - |
| Total n(%) | Total Detection per Study Site | |||||
|---|---|---|---|---|---|---|
| DRH n (%) | HUCSH n (%) | TASH n (%) | Y12HMC n (%) | |||
| TEM Variants Detected | blaTEM-1B | 185(61.5) * | 65(57.5) | 46(80.7) | 45(49.5) | 29(72.5) |
| blaTEM-1A | 5(0.9) | 1(0.9) | 1(20) | 2(2.2) | 1(2.5) | |
| blaTEM-1C | 1(0.3) | 1(0.9) | - | - | - | |
| blaTEM-206 | 2(0.7) | 1(0.9) | - | 1(1.1) | - | |
| blaTEM-219 | 2(0.7) | - | 1(1.8) | 1(1.1) | - | |
| blaTEM-30 | 3(1) | 1(0.9) | - | 2(2.2) | - | |
| SHV variants detected | blaSHV-187 | 187(27.6) * | 11(9.7) | 20(35.1) | 38(41.8) | 14(35) |
| blaSHV-28 | 10(3.3) | 4(3.5) | 1(1.8) | 5(5.5) | - | |
| blaSHV-79 | 8(2.7) | - | - | - | 8(20) | |
| blaSHV-85 | 8(2.7) | - | - | - | 8(20) | |
| blaSHV-89 | 8(2.7) | - | - | - | 8(20) | |
| blaSHV-40 | 7(2.3) | - | - | - | 7(17.5) | |
| blaSHV-60 | 5(1.7) | - | - | - | 5(12.5) | |
| blaSHV-119 | 2(0.7) | - | - | 2(2.2) | - | |
| blaSHV-94 | 1(0.3) | - | - | - | 1(2.5) | |
| blaSHV-172 | 1(0.3) | - | - | - | 1(2.5) | |
| blaSHV-56 | 8(2.7) | - | - | - | 8(20) | |
| Combinations of Genes | Total n | DRH n | HUCSH n | TASH n | Y12HMC n |
|---|---|---|---|---|---|
| blaCTX-M-15 * blaTEM-1B | 166 | 53 | 45 | 39 | 29 |
| blaCTX-M-15 * blaSHV-187 | 78 | 11 | 20 | 34 | 13 |
| blaCTX-M-15 * blaSHV-106 | 10 | 5 | 1 | 4 | - |
| blaCTX-M-15 * blaOXY-1-2 | 3 | 2 | 1 | - | - |
| blaCTX-M-15 * blaTEM-207 | 1 | - | - | 1 | - |
| blaCTX-M-15 * blaOXY-1-5 | 3 | - | - | 2 | 1 |
| blaTEM-1B * blaSHV-106 | 10 | 5 | - | 5 | - |
| blaTEM-1B * blaOXY-1-2 | 2 | 2 | - | - | - |
| blaTEM-1B * blaOXY-1-5 | 3 | - | - | 2 | 1 |
| blaTEM-1B * blaTEM-207 | 3 | 1 | 0 | 2 | 1 |
| blaSHV-187 * blaSHV-106 | 11 | 5 | 1 | 5 | - |
| blaSHV-187 * blaTEM-207 | 2 | - | - | 2 | - |
| blaSHV-187 * blaTEM-207 | 2 | - | - | 2 | - |
| blaCTX-M-15 * blaTEM-1B * blaSHV-187 | 56 | 9 | 15 | 24 | 8 |
| blaCTX-M-15 * blaTEM-1B * blaSHV-106 | 9 | 5 | - | 4 | - |
| blaCTX-M-15 * blaTEM-1B * blaOXY-1-5 | 3 | - | - | 2 | - |
| blaCTX-M-15 * blaTEM-1B * blaTEM-207 | 1 | - | - | 1 | - |
| blaCTX-M-15 * blaSHV-187 * blaSHV-106 | 10 | 5 | 1 | 4 | - |
| blaCTX-M-15 * blaSHV-106 * blaTEM-207 | 1 | - | - | 1 | - |
| blaSHV-106 * blaTEM-1B * blaSHV-187 | 10 | 5 | - | 5 | - |
| blaTEM-207 * blaTEM-1B * blaSHV-187 | 2 | - | - | 2 | - |
| blaCTX-M-15 * blaTEM-1B * blaSHV-187 * blaSHV-106 | 9 | 5 | - | 4 | - |
| blaCTX-M-15 * blaTEM-1B * blaSHV-187 * blaTEM-207 | 1 | - | - | 1 | - |
| blaTEM-207 * blaTEM-1B * blaSHV-187 * blaSHV-106 | 2 | - | - | 2 | - |
| blaCTX-M-15 * blaTEM-1B * blaSHV-187 * blaTEM-207 * blaSHV-106 | 1 | - | - | 1 | - |
| AmpC Genes | Hospital | AmpC Harboring Enterobacteriaceae | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| DRH n | HUCSH n | TASH n | Y12HMC n | K. pneumoniae n | K. variicola n | E. coli n | E.cloacae n | K. oxytoca n | E. xiangfangensis n | S. marcescens n | E. ludwigii n | E. kobei n | |
| blaACT-7 (n = 9) | 5 | - | 1 | 3 | - | - | - | 6 | - | 2 | - | - | 1 |
| blaCMY-6 (n = 7) | 2 | - | 5 | - | 7 | - | - | - | - | - | - | - | - |
| blaACT-16 (n = 6) | 1 | - | 5 | - | - | - | - | 6 | - | - | - | - | - |
| blaACT-14 (n = 3) | 3 | - | 1 | - | - | - | - | 4 | - | - | - | - | - |
| blaACT-5 (n = 2) | 3 | - | - | - | - | - | - | 3 | - | - | - | - | - |
| blaDHA-1 (n = 2) | - | 5 | - | - | 2 | 2 | - | - | 1 | - | - | - | - |
| blaCMY-148 (n = 3) | - | 1 | 2 | - | - | - | 2 | - | - | - | - | 1 | - |
| blaCMY-2 (n = 2) | - | - | 2 | - | - | - | 2 | - | - | - | - | - | - |
| blaCMH-3 (n = 2) | 2 | - | - | - | - | - | - | 2 | - | - | - | - | - |
| blaSRT-1 (n = 2) | - | - | 2 | - | - | - | - | - | - | - | 2 | - | - |
| blaACT-15 (n = 1) | - | 1 | - | - | - | - | - | 1 | - | - | - | - | - |
| blaACT-4 (n = 1) | 1 | ||||||||||||
| blaCMY-42 (n = 1) | - | - | 1 | - | - | - | 1 | - | - | - | - | - | - |
| blaSRT-2 (n = 1) | - | - | 1 | - | - | - | - | - | - | - | 1 | - | - |
| Total AmpC genes detected | 17 | 7 | 20 | 3 | 9 | 2 | 5 | 22 | 1 | 2 | 1 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Legese, M.H.; Asrat, D.; Aseffa, A.; Hasan, B.; Mihret, A.; Swedberg, G. Molecular Epidemiology of Extended-Spectrum Beta-Lactamase and AmpC Producing Enterobacteriaceae among Sepsis Patients in Ethiopia: A Prospective Multicenter Study. Antibiotics 2022, 11, 131. https://doi.org/10.3390/antibiotics11020131
Legese MH, Asrat D, Aseffa A, Hasan B, Mihret A, Swedberg G. Molecular Epidemiology of Extended-Spectrum Beta-Lactamase and AmpC Producing Enterobacteriaceae among Sepsis Patients in Ethiopia: A Prospective Multicenter Study. Antibiotics. 2022; 11(2):131. https://doi.org/10.3390/antibiotics11020131
Chicago/Turabian StyleLegese, Melese Hailu, Daniel Asrat, Abraham Aseffa, Badrul Hasan, Adane Mihret, and Göte Swedberg. 2022. "Molecular Epidemiology of Extended-Spectrum Beta-Lactamase and AmpC Producing Enterobacteriaceae among Sepsis Patients in Ethiopia: A Prospective Multicenter Study" Antibiotics 11, no. 2: 131. https://doi.org/10.3390/antibiotics11020131