
Clinical Outcomes and Safety of Meropenem–Colistin versus Meropenem–Tigecycline in Patients with Carbapenem-Resistant Acinetobacter baumannii Pneumonia

Abstract
:1. Introduction
2. Results
2.1. Patients and Clinical Characteristics
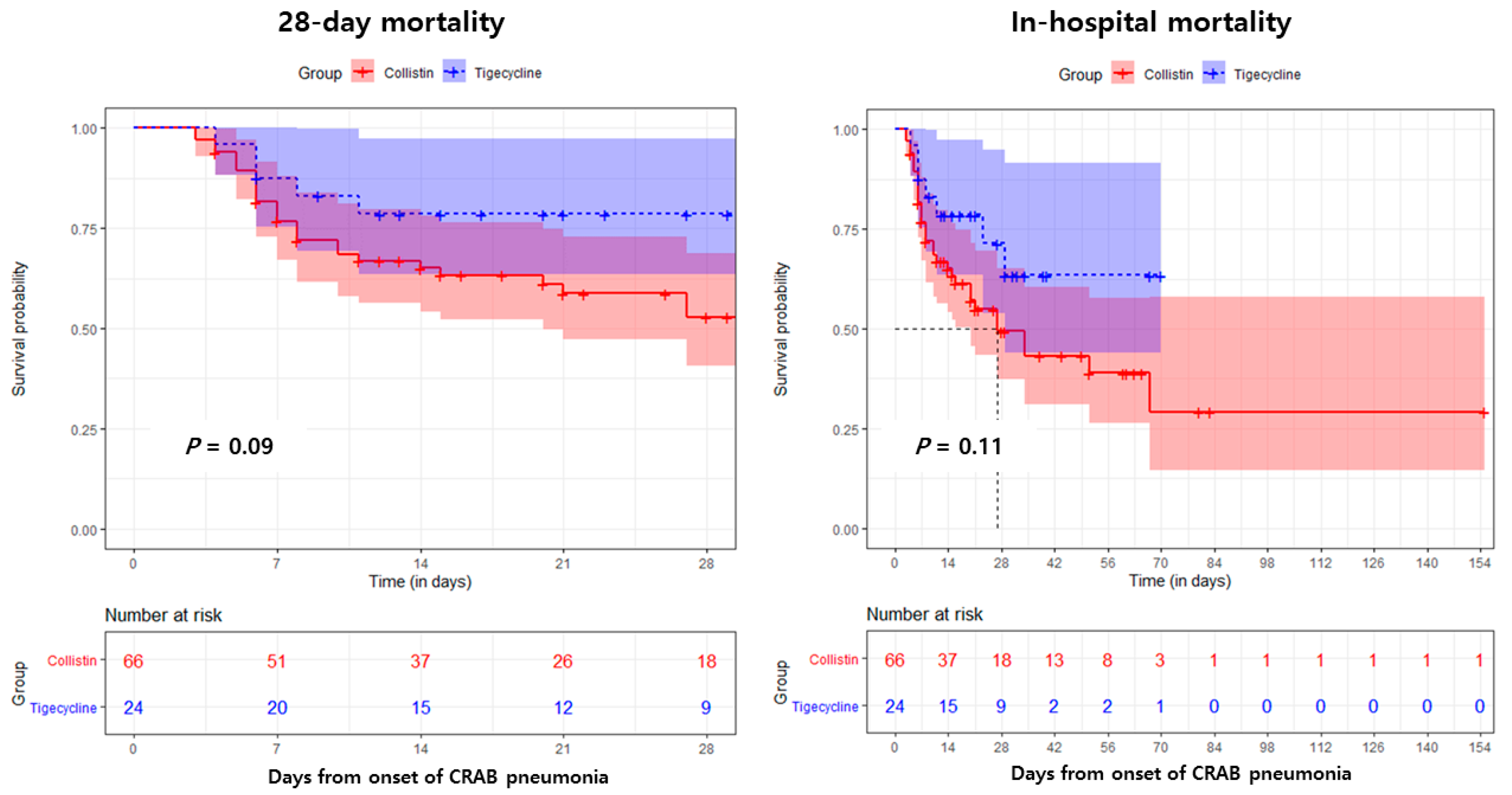
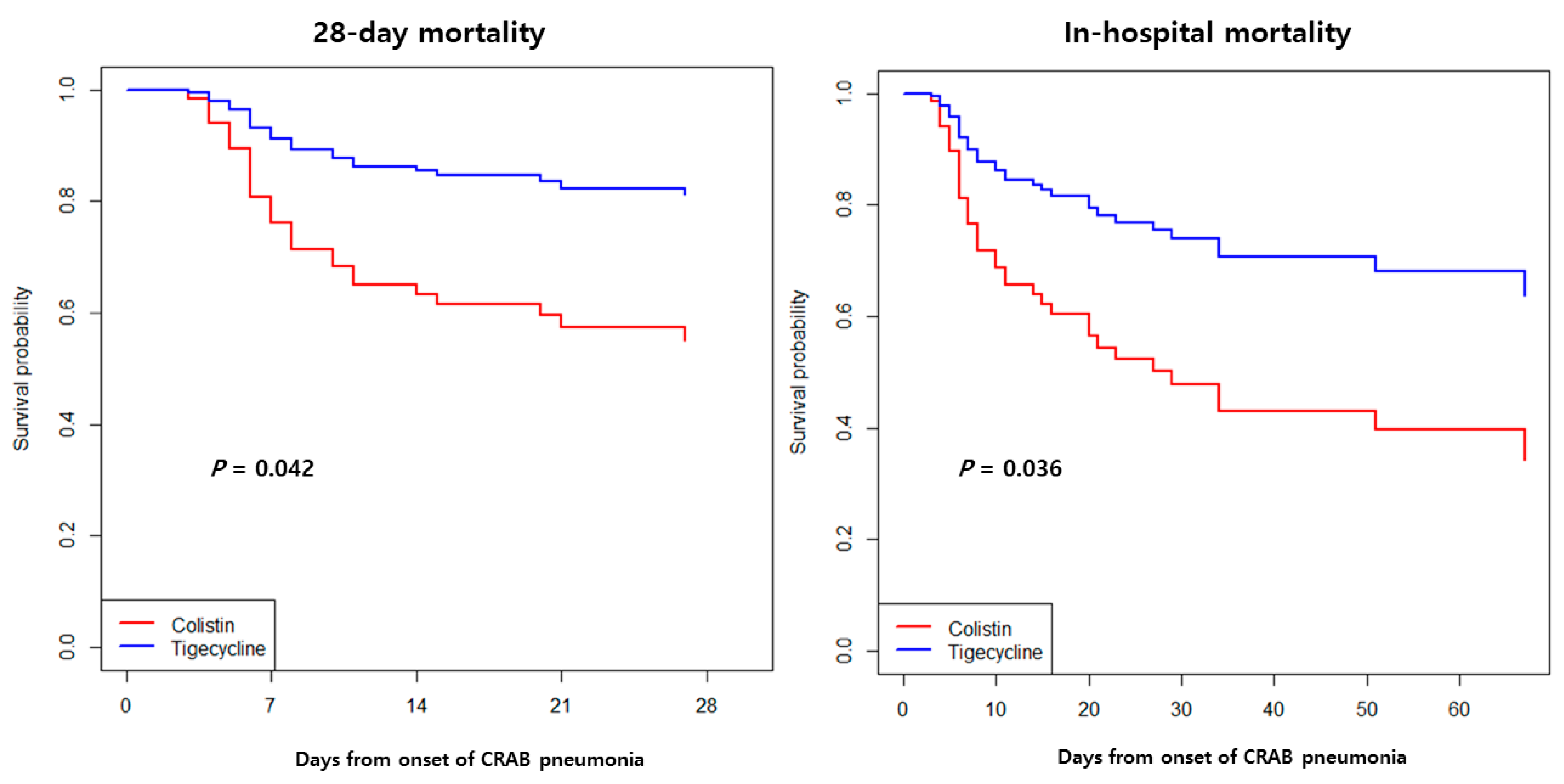
2.2. Treatment Outcomes
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Variables and Definitions
4.3. Microbiological Tests
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of New Antibiotics. 2017. Available online: http://www.who.int/medicines/publications/WHO-PPL-Short_Summary_25Feb-ET_NM_WHO.pdf (accessed on 18 April 2021).
- World Health Organization. Central Asian and Eastern European Surveillance of Antimicrobial Resistance [Annual Report]. World Health Organization Regional Office for Europe, Copenhagen, Denmark. 2017. Available online: http://www.euro.who.int/__data/assets/pdf_file/0005/354434/WHO_CAESAR_AnnualReport_2017.pdf?ua=1 (accessed on 18 April 2021).
- Kim, D.; Ahn, J.Y.; Lee, C.H.; Jang, S.J.; Lee, H.; Yong, D.; Jeong, S.H.; Lee, K. Increasing Resistance to Extended-Spectrum Cephalosporins, Fluoroquinolone, and Carbapenem in Gram-Negative Bacilli and the Emergence of Carbapenem Non-Susceptibility in Klebsiella pneumoniae: Analysis of Korean Antimicrobial Resistance Monitoring System (KARMS) Data From 2013 to 2015. Ann. Lab. Med. 2017, 37, 231–239. [Google Scholar]
- Chung, D.R.; Song, J.H.; Kim, S.H.; Thamlikitkul, V.; Huang, S.G.; Wang, H.; So, T.M.; Yasin, R.M.; Hsueh, P.R.; Carlos, C.C.; et al. High Prevalence of Multidrug-Resistant Nonfermenters in Hospital-Acquired Pneumonia in Asia. Am. J. Respir. Crit. Care Med. 2011, 184, 1409–1417. [Google Scholar] [CrossRef]
- Bouchillon, S.K.; Hoban, D.J.; Johnson, B.M.; Johnson, J.L.; Hsiung, A.; Dowzicky, M.J.; Tigecycline Evaluation and Surveillance Trial (TEST) Group. In Vitro Activity of Tigecycline Against 3989 Gram-Negative and Gram-Positive Clinical Isolates from the United States Tigecycline Evaluation and Surveillance Trial (TEST Program; 2004). Diagn. Microbiol. Infect. Dis. 2005, 52, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Crandon, J.L.; Kim, A.; Nicolau, D.P. Comparison of Tigecycline Penetration into the Epithelial Lining Fluid of Infected and Uninfected Murine Lungs. J. Antimicrob. Chemother. 2009, 64, 837–839. [Google Scholar] [CrossRef] [Green Version]
- Zha, L.; Pan, L.; Guo, J.; French, N.; Villanueva, E.V.; Tefsen, B. Effectiveness and Safety of High Dose Tigecycline for the Treatment of Severe Infections: A Systematic Review and Meta-Analysis. Adv. Ther. 2020, 37, 1049–1064. [Google Scholar] [CrossRef] [PubMed]
- Freire, A.T.; Melnyk, V.; Kim, M.J.; Datsenko, O.; Dzyublik, O.; Glumcher, F.; Chuang, Y.C.; Maroko, R.T.; Dukart, G.; Cooper, C.A.; et al. Comparison of Tigecycline with Imipenem/Cilastatin for the Treatment of Hospital-Acquired Pneumonia. Diagn. Microbiol. Infect. Dis. 2010, 68, 140–151. [Google Scholar] [CrossRef] [PubMed]
- FDA Drug Safety Communication. Increased Risk of Death with Tygacil (Tigecycline) Compared to Other Antibiotics Used to Treat Similar Infections. Available online: http://www.fda.gov/Drugs/DrugSafety/ucm224370.htm (accessed on 18 April 2021).
- Nation, R.L.; Garonzik, S.M.; Thamlikitkul, V.; Giamarellos-Bourboulis, E.J.; Forrest, A.; Paterson, D.L.; Li, J.; Silveira, F.P. Dosing Guidance for Intravenous Colistin in Critically Ill Patients. Clin. Infect. Dis. 2017, 64, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Gurjar, M. Colistin for lLung Infection: An Update. J. Intensive Care 2015, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Akajagbor, D.S.; Wilson, S.L.; Shere-Wolfe, K.D.; Dakum, P.; Charurat, M.E.; Gilliam, B.L. Higher Incidence of Acute Kidney Injury with Intravenous Colistimethate Sodium Compared With Polymyxin B in Critically Ill Patients at a Tertiary Care Medical Center. Clin. Infect. Dis. 2013, 57, 1300–1303. [Google Scholar] [CrossRef] [Green Version]
- Phe, K.; Lee, Y.; McDaneld, P.M.; Prasad, N.; Yin, T.; Figueroa, D.A.; Musick, W.L.; Cottreau, J.M.; Hu, M.; Tam, V.H. In Vitro Assessment and Multicenter Cohort Study of Comparative Nephrotoxicity Rates Associated with Colistimethate Versus Polymyxin B Therapy. Antimicrob. Agents Chemother. 2014, 58, 2740–2746. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Rayner, C.R.; Nation, R.L.; Owen, R.J.; Spelman, D.; Tan, K.E.; Liolios, L. Heteroresistance to Colistin in Multidrug-Resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2006, 50, 2946–2950. [Google Scholar] [CrossRef] [Green Version]
- Ni, W.; Han, Y.; Zhao, J.; Wei, C.; Cui, J.; Wang, R.; Liu, Y. Tigecycline Treatment Experience Against Multidrug-Resistant Acinetobacter baumannii Infections: A Systematic Review and Meta-Analysis. Int. J. Antimicrob. Agents. 2016, 47, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.C.; Cheng, C.Y.; Sheng, W.H.; Sun, H.Y.; Wang, J.T.; Chen, Y.C.; Chang, S.C. Effectiveness of Tigecycline-Based Versus Colistin- Based Therapy for Treatment of Pneumonia Caused by Multidrug-Resistant Acinetobacter baumannii in a Critical Setting: A Matched Cohort Analysis. BMC Infect. Dis. 2014, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.A.; Lin, Y.C.; Lu, P.L.; Chen, H.C.; Chang, H.L.; Sheu, C.C. Antibiotic Strategies and Clinical Outcomes in Critically Ill Patients with Pneumonia Caused by Carbapenem-Resistant Acinetobacter baumannii. Clin. Microbiol. Infect. 2018, 24, 908.e1–908.e7. [Google Scholar] [CrossRef] [Green Version]
- Ye, J.J.; Lin, H.S.; Kuo, A.J.; Leu, H.S.; Chiang, P.C.; Huang, C.T.; Lee, M.H. The Clinical Implication and Prognostic Predictors of Tigecycline Treatment for Pneumonia Involving Multidrug-Resistant Acinetobacter baumannii. J. Infectol. 2011, 63, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.Y.; Moon, J.Y.; Huh, J.W.; Choi, S.H.; Lim, C.M.; Koh, Y.; Chong, Y.P.; Hong, S.B. Comparable Efficacy of Tigecycline Versus Colistin Therapy for Multidrug-Resistant and Extensively Drug-Resistant Acinetobacter baumannii Pneumonia in Critically Ill Patients. PLoS ONE 2016, 11, e0150642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Chen, X.; Xu, P.; Zhu, Y.; Wang, K.; Xiang, D.; Wang, F.; Banh, H.L. Clinical Experience with Tigecycline in the Treatment of Hospital-Acquired Pneumonia Caused by Multidrug Resistant Acinetobacter baumannii. BMC Pharmacol. Toxicol. 2019, 20, 19. [Google Scholar] [CrossRef]
- Liu, B.; Li, S.; Li, H.T.; Wang, X.; Tan, H.Y.; Liu, S.; Pan, P.H.; Li, X.G.; Li, X.M. Outcomes and Prognostic Factors of Tigecycline Treatment for Hospital-Acquired Pneumonia Involving Multidrug-Resistant Acinetobacter baumannii. J. Int. Med. Res. 2020, 48. [Google Scholar] [CrossRef]
- Stein, G.E.; Craig, W.A. Tigecycline: A Critical Analysis. Clin. Infect. Dis. 2006, 43, 518–524. [Google Scholar] [CrossRef]
- Karageorgopoulos, D.E.; Kelesidis, T.; Kelesidis, I.; Falagas, M.E. Tigecycline for the Treatment of Multidrug-Resistant (Including Carbapenem-Resistant) Acinetobacter Infections: A Review of the Scientific Evidence. J. Antimicrob. Chemother. 2008, 62, 45–55. [Google Scholar] [CrossRef] [Green Version]
- De Pascale, G.; Montini, L.; Pennisi, M.; Bernini, V.; Maviglia, R.; Bello, G.; Spanu, T.; Tumbarello, M.; Antonelli, M. High Dose Tigecycline in Critically Ill Patients with Severe Infections Due to Multidrug-Resistant Bacteria. Crit. Care 2014, 18, R90. [Google Scholar] [CrossRef] [Green Version]
- De Pascale, G.; Lisi, L.; Ciotti, G.M.P.; Vallecoccia, M.S.; Cutuli, S.L.; Cascarano, L.; Gelormini, C.; Bello, G.; Montini, L.; Carelli, S.; et al. Pharmacokinetics of High-Dose Tigecycline in Critically Ill Patients with Severe Infections. Ann. Intensive Care 2020, 10, 94. [Google Scholar] [CrossRef]
- Pongpech, P.; Amornnopparattanakul, S.; Panapakdee, S.; Fungwithaya, S.; Nannha, P.; Dhiraputra, C.; Leelarasamee, A. Antibacterial Activity of Carbapenem-Based Combinations Against Multidrug-Resistant Acinetobacter baumannii. J. Med. Assoc. Thai. 2010, 93, 161–171. [Google Scholar]
- Jiang, Z.; He, X.; Li, J. Synergy Effect of Meropenem-Based Combinations Against Acinetobacter baumannii: A Systematic Review and Meta-Analysis. Infect. Drug Resist. 2018, 11, 1083–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zusman, O.; Avni, T.; Leibovici, L.; Adler, A.; Friberg, L.; Stergiopoulou, T.; Carmeli, Y.; Paul, M. Systematic Review and Meta-Analysis of In Vitro Synergy of Polymyxins and Carbapenems. Antimicrob. Agents Chemother. 2013, 57, 5104–5111. [Google Scholar] [CrossRef] [Green Version]
- Daikos, G.L.; Tsaousi, S.; Tzouvelekis, L.S.; Anyfantis, I.; Psichogiou, M.; Argyropoulou, A.; Stefanou, I.; Sypsa, V.; Miriagou, V.; Nepka, M.; et al. Carbapenemase-Producing Klebsiella pneumoniae Bloodstream Infections: Lowering Mortality by Antibiotic Combination Schemes and the Role of Carbapenems. Antimicrob. Agents Chemother. 2014, 58, 2322–2328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, D.N.; Moellering, R.C., Jr.; Eliopoulos, G.M. The Sanford Guide to Antimicrobial Therapy 2018, 48th ed; Antimicrobial Therapy: Sperryville, VA, USA, 2018. [Google Scholar]
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the Management of Adults with Hospital-Acquired, Ventilator-Associated, and Healthcare-Associated Pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef] [PubMed]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. Twenty-Eight Informational Supplement; CLSI Document M100; CLSI: Annapolis Junction, MD, USA, 2010; ISBN 1-56238-839-8. [Google Scholar]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a Combined Comorbidity Index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total (n = 90) | Colistin-Based (n = 66) | Tigecycline-Based (n = 24) | p-Value |
|---|---|---|---|---|
| Demographic variable | ||||
| Median age, years (IQR) | 70 (62–80) | 68 (61–76) | 79 (67–85) | 0.003 |
| Male sex, n (%) | 59 (65.6) | 46 (69.7) | 13 (54.2) | 0.170 |
| Variables from current admission | ||||
| Median length of hospital stay before CRAB pneumonia diagnosis (IQR), days | 15 (10–33) | 14 (9–27) | 23 (15–46) | 0.013 |
| BMI ≥ 25 kg/m2 | 19 (23.8) | 17 (28.3) | 2 (10.0) | 0.132 |
| Ventilator–associated pneumonia | 28 (31.1) | 25 (37.9) | 3 (12.5) | 0.021 |
| Comorbidities, n (%) | ||||
| Cardiovascular disease | 49 (54.4) | 35 (53.0) | 14 (58.3) | 0.655 |
| Neurologic disease | 35 (38.9) | 25 (37.9) | 10 (41.7) | 0.744 |
| Malignant disease | 22 (24.4) | 20 (30.3) | 2 (8.3) | 0.032 |
| Trauma | 8 (8.9) | 5 (7.6) | 3 (12.5) | 0.435 |
| Renal disease | 11 (2.2) | 9 (13.6) | 2 (8.3) | 0.721 |
| Hepatic disease | 6 (6.7) | 6 (9.1) | 0 | 0.187 |
| Pulmonary disease | 6 (6.7) | 6 (9.1) | 0 | 0.187 |
| Metabolic disease | 36 (40.0) | 28 (42.4) | 8 (33.3) | 0.436 |
| Median Charlson comorbidity score (IQR) | 2 (1–3) | 2 (1–4) | 2 (1–2) | 0.253 |
| Antimicrobial susceptibility, n (%) | ||||
| Meropenem MIC = 8 µg/mL | 18 (20.0) | 12 (18.2) | 6 (25.0) | 0.554 |
| Tigecycline MIC ≤ 2 µg/mL | 73 (81.1) | 54 (81.8) | 19 (79.2) | 0.767 |
| Clinical severity, n (%) | ||||
| CRAB bacteremia | 12 (13.3) | 11 (16.7) | 1 (4.2) | 0.710 |
| ICU admission | 88 (97.8) | 65 (98.5) | 23 (95.8) | 0.464 |
| Septic shock | 68 (75.6) | 50 (75.8) | 18 (75.0) | 0.941 |
| Mechanical ventilator | 80 (88.9) | 61 (92.4) | 19 (79.2) | 0.123 |
| Hemodialysis | 28 (31.1) | 24 (36.4) | 4 (16.7) | 0.074 |
| ECMO | 7 (7.8) | 6 (9.1) | 1 (4.2) | 0.670 |
| Laboratory findings at time of CRAB pneumonia diagnosis, n (%) | ||||
| Hemoglobin ≤ 10 mg/dL | 86 (95.6) | 63 (95.5) | 23 (95.8) | 1.000 |
| Platelet ≤ 100,000/mm3 | 61 (67.8) | 46 (69.7) | 15 (62.5) | 0.518 |
| Bilirubin ≥ 3 mg/dL | 23 (25.6) | 18 (27.3) | 5 (20.8) | 0.536 |
| Albumin ≤ 3 mg/dL | 87 (96.7) | 63 (95.5) | 24 (100.0) | 0.562 |
| C-reactive protein ≥ 100 mg/L | 79 (87.8) | 59 (89.4) | 20 (83.3) | 0.475 |
| Procalcitonin ≥ 1 ng/mL | 54 (66.7) | 38 (65.5) | 16 (69.6) | 0.727 |
| Characteristics | Total (n = 90) | Colistin-Based (n = 66) | Tigecycline-Based (n = 24) | p-Value |
|---|---|---|---|---|
| Adverse events during treatment, n (%) | ||||
| Nephrotoxicity | 37 (41.1) | 34 (51.5) | 3 (12.5) | 0.001 |
| Hepatotoxicity | 35 (38.9) | 28 (42.4) | 7 (29.2) | 0.254 |
| Nausea | 9 (10.0) | 6 (9.1) | 3 (12.5) | 0.696 |
| Change of initial antibiotic therapy, n (%) | ||||
| Antibiotic change | 15 (16.7) | 12 (18.2) | 3 (12.5) | 0.751 |
| Median time before change of initial antibiotics (IQR), days | 9 (6–12) | 8 (6–11) | 11 (7–13) | 0.033 |
| Clinical outcomes, n (%) | ||||
| In-hospital mortality | 40 (44.4) | 33 (50.0) | 7 (29.2) | 0.079 |
| 14-day hospital mortality | 26 (28.9) | 21 (31.8) | 5 (20.8) | 0.309 |
| 28-day hospital mortality | 32 (35.6) | 27 (40.9) | 5 (20.8) | 0.078 |
| Median length of hospital stay after CRAB pneumonia diagnosis (IQR), days | 16 (7–31) | 16 (7–30) | 21 (10–32) | 0.398 |
| Median length of hospital stay (IQR), days | 39 (25–64) | 34 (24–61) | 47 (31–82) | 0.080 |
| Characteristics | Total (n = 90) | Survivors (n = 50) | Non-Survivors (n = 40) | p-Value |
|---|---|---|---|---|
| Demographic variable | ||||
| Median age, years (IQR) | 70 (62–80) | 70 (61–80) | 71 (62–79) | 0.855 |
| Male sex, n (%) | 59 (65.6) | 31 (62.0) | 28 (70.0) | 0.427 |
| Variables from current admission | ||||
| Median length of hospital stay before CRAB pneumonia diagnosis (IQR), days | 15 (10–33) | 15 (9–27) | 17 (11–37) | 0.134 |
| BMI ≥ 25 kg/m2 | 19 (23.8) | 9 (20.5) | 10 (27.8) | 0.444 |
| Ventilator-associated pneumonia | 28 (31.1) | 15 (30.0) | 13 (32.5) | 0.799 |
| Comorbidities, n (%) | ||||
| Cardiovascular disease | 49 (54.4) | 26 (52.0) | 23 (57.5) | 0.603 |
| Neurologic disease | 35 (38.9) | 23 (46.0) | 12 (30.0) | 0.122 |
| Malignant disease | 22 (24.4) | 6 (12.0) | 16 (40.0) | 0.002 |
| Trauma | 8 (8.9) | 6 (12.0) | 2 (5.0) | 0.292 |
| Renal disease | 11 (12.2) | 6 (12.0) | 5 (12.5) | 1.000 |
| Hepatic disease | 6 (6.7) | 2 (4.0) | 4 (10.0) | 0.400 |
| Pulmonary disease | 6 (6.7) | 4 (8.0) | 2 (5.0) | 0.689 |
| Metabolic disease | 36 (40.0) | 17 (34.0) | 19 (47.5) | 0.194 |
| Median Charlson comorbidity score (IQR) | 2 (1–3) | 1.5 (1–3) | 2 (1–4) | 0.060 |
| Antimicrobial susceptibility, n (%) | ||||
| Meropenem MIC = 8 µg/mL | 18 (20.0) | 9 (18.0) | 9 (22.5) | 0.596 |
| Tigecycline MIC ≤ 2 µg/mL | 73 (81.1) | 43 (86.0) | 30 (75.0) | 0.185 |
| Antimicrobial regimen for CRAB pneumonia, n (%) | ||||
| Colistin-based regimen | 66 (73.3) | 33 (66.0) | 33 (82.5) | 0.079 |
| Tigecycline-based regimen | 24 (26.7) | 17 (34.0) | 7 (17.5) | 0.079 |
| Clinical severity, n (%) | ||||
| CRAB bacteremia | 12 (13.3) | 6 (12.0) | 6 (15.0) | 0.677 |
| ICU admission | 88 (97.8) | 49 (98.0) | 39 (97.5) | 1.000 |
| Septic shock | 68 (75.6) | 31 (62.0) | 37 (92.5) | 0.001 |
| Mechanical ventilator | 80 (88.9) | 43 (86.0) | 37 (92.5) | 0.502 |
| Hemodialysis | 28 (31.1) | 12 (24.0) | 16 (40.0) | 0.103 |
| ECMO | 7 (7.8) | 1 (2.0) | 6 (15.0) | 0.042 |
| Laboratory findings at time of CRAB pneumonia diagnosis, n (%) | ||||
| Hemoglobin ≤ 10 mg/dL | 86 (95.6) | 47 (94.0) | 39 (97.5) | 0.626 |
| Platelet ≤ 100,000/mm3 | 61 (67.8) | 29 (58.0) | 32 (80.0) | 0.026 |
| Bilirubin ≥ 3 mg/dL | 23 (25.6) | 9 (18.0) | 14 (35.0) | 0.066 |
| Albumin ≤ 3 mg/dL | 87 (96.7) | 47 (94.0) | 40 (100.0) | 0.251 |
| C-reactive protein ≥ 100 mg/L | 79 (87.8) | 42 (84.0) | 37 (92.5) | 0.334 |
| Procalcitonin ≥ 1 ng/mL | 54 (66.7) | 24 (53.3) | 30 (83.3) | 0.004 |
| Clinical outcomes, n (%) | ||||
| Nephrotoxicity | 37 (41.1) | 14 (28.0) | 23 (57.5) | 0.005 |
| Hepatotoxicity | 35 (38.9) | 10 (20.0) | 25 (62.5) | <0.001 |
| Median total length of hospital stay (IQR), days | 39 (25–64) | 48 (27–71) | 32 (19–56) | 0.041 |
| Independent Variables | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Meropenem–colistin combination therapy | 2.58 | 1.07–6.23 | 0.036 |
| Procalcitonin≥ 1 ng/mL | 3.39 | 1.40–8.19 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.-M.; Yang, K.-S.; Chung, Y.-S.; Lee, K.-B.; Kim, J.-Y.; Kim, S.-B.; Sohn, J.-W.; Yoon, Y.-K. Clinical Outcomes and Safety of Meropenem–Colistin versus Meropenem–Tigecycline in Patients with Carbapenem-Resistant Acinetobacter baumannii Pneumonia. Antibiotics 2021, 10, 903. https://doi.org/10.3390/antibiotics10080903
Park J-M, Yang K-S, Chung Y-S, Lee K-B, Kim J-Y, Kim S-B, Sohn J-W, Yoon Y-K. Clinical Outcomes and Safety of Meropenem–Colistin versus Meropenem–Tigecycline in Patients with Carbapenem-Resistant Acinetobacter baumannii Pneumonia. Antibiotics. 2021; 10(8):903. https://doi.org/10.3390/antibiotics10080903
Chicago/Turabian StylePark, Jae-Min, Kyung-Sook Yang, You-Seung Chung, Ki-Byung Lee, Jeong-Yeon Kim, Sun-Bean Kim, Jang-Wook Sohn, and Young-Kyung Yoon. 2021. "Clinical Outcomes and Safety of Meropenem–Colistin versus Meropenem–Tigecycline in Patients with Carbapenem-Resistant Acinetobacter baumannii Pneumonia" Antibiotics 10, no. 8: 903. https://doi.org/10.3390/antibiotics10080903