
Animal and Human Dirofilariasis in India and Sri Lanka: A Systematic Review and Meta-Analysis
by
 , ,
, ,
Sandani S. Thilakarathne
1,†,
Nicholas K. Y. Yuen
2,†,
Mohammad Mahmudul Hassan
2,3,
Thishan C. Yahathugoda
1 and
Swaid Abdullah
2,* 1
Department of Parasitology, Faculty of Medicine, University of Ruhuna, Galle P.O. Box 70, Sri Lanka
2
School of Veterinary Science, The University of Queensland, Gatton, QLD 4343, Australia
3
Faculty of Veterinary Medicine, Chattogram Veterinary and Animal Sciences University, Chattogram 4225, Bangladesh
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Animals 2023, 13(9), 1551; https://doi.org/10.3390/ani13091551
Submission received: 24 March 2023
/
Revised: 2 May 2023
/
Accepted: 3 May 2023
/
Published: 5 May 2023
(This article belongs to the Special Issue Zoonoses and Wildlife - One Health Approach)
Abstract
:Simple Summary
Dirofilariasis is caused by Dirofilaria spp. worm infections, transmitted by mosquitoes, and affects humans and animals worldwide. Often, infected animals show symptoms relating to the cardiopulmonary system (heart and lung) and subcutaneous tissue (eye and skin). This study assessed the current published data on the distribution and prevalence of dirofilariasis across Sri Lanka and India. This analysis found that almost all cases of human dirofilariasis reported in Sri Lanka and India are presented as subcutaneous infections, with the eye being the most commonly affected organ. Both heartworm and subcutaneous infections are found in the dog populations in India. However, only subcutaneous infections have so far been reported in Sri Lanka, and the rationale behind this geographical distribution of infection patterns of dirofilariasis remains unknown and warrants further research. There was a low infection rate in the pet and working dog populations in India and Sri Lanka, but this may change due to climate change and emerging anti-parasitic drug resistance. It was identified in this study that some regions within India and Sri Lanka have not yet been surveyed for dirofilariasis, and future studies need to target these unsurveyed areas to better understand the geographical and species distribution of dirofilariasis in these two countries.
Abstract
Dirofilariasis is an emerging vector-borne tropical disease of public health importance that mainly affects humans and dogs. Dirofilaria immitis and D. repens are the two well-documented dirofilariasis-causing filarioid helminths of both medical and veterinary concerns in India and Sri Lanka. This systematic review and meta-analysis aimed to describe and summarize the current evidence of dirofilariasis prevalence and distribution in India and Sri Lanka. Interestingly, D. repens is reported to circulate in both dogs (prevalence of 35.8% (95% CI: 11.23–60.69)) and humans (97% of published case reports) in India and Sri Lanka, but D. immitis is reported to be present in the dog populations in India (prevalence of 9.7% (95% CI: 8.5–11.0%)), and so far, it has not been reported in Sri Lanka. This peculiar distribution of D. immitis and D. repens in the two neighbouring countries could be due to the interaction between the two parasite species, which could affect the pattern of infection of the two worm species in dogs and thus influence the geographical distribution of these two filarial worms. In medical and veterinary practice, histopathology was the most commonly used diagnostic technique (31.3%; 95% CI 2.5–60.2%). The low specificity of histopathology to speciate the various Dirofilaria spp. may lead to misdiagnosis. It was identified in this study that several regions of India and Sri Lanka have not yet been surveyed for dirofilariasis. This limits our understanding of the geographical distribution and interspecies interactions of the two parasites within these countries. Parasite distribution, disease prevalence, and interspecies interactions between the vectors and the host should be targeted for future research.
1. Introduction
The dynamics of vector-borne disease transmission are often multifactorial. With climate change, unpredictable weather conditions can affect the survival and distribution of the vector populations and hence the diseases they transmit. Examples include the Dengue virus transmitted by mosquitoes [1], the Hendra virus transmitted by bats [2], and Babesia spp. transmitted by ticks [3]. Mosquito-borne diseases are arguably the most researched area in the field of vector-borne diseases. Mosquitoes can be readily transferred from one place to another by wind, air transport, or cargo ships, which then introduce and establish diseases and potential outbreaks to previously exotic/non-endemic areas. In addition, deforestation, urbanization, irrigation, and change in socio-economic circumstances have been implicated as factors contributing to the rise in mosquito-borne diseases, among other vector-borne diseases [4].
Dirofilariasis is an emerging zoonosis globally caused by infection with filarial nematodes of the genus Dirofilaria. Climate change may contribute to the changes in its temporal and spatial distribution and a possible increase in the incidence of this disease [5]. However, our understanding of this disease is limited and is often overshadowed by the more prominent mosquito-borne diseases, such as malaria, dengue, chikungunya, and West Nile fever.
Filarial worms of the genus Dirofilaria are long tubular adult worms which infect the circulatory system or connective tissues of mammalian hosts, and mature female worms produce unsheathed larvae called microfilariae, which circulate in the host blood. So far, around 34 Dirofilaria spp. have been described predominantly from carnivores and primates and allocated to two subgenera: Dirofilaria, comprising long thin worms (<0.1 mm diameter) with smooth cuticles that infect the lungs, heart, and blood vessels; Nochtiella, which are shorter stout worms (0.2–0.5 mm diameter) with cuticular ornamentations (longitudinal ridges with transverse striations) and infect subcutaneous and conjunctival tissues [6] (Table 1).
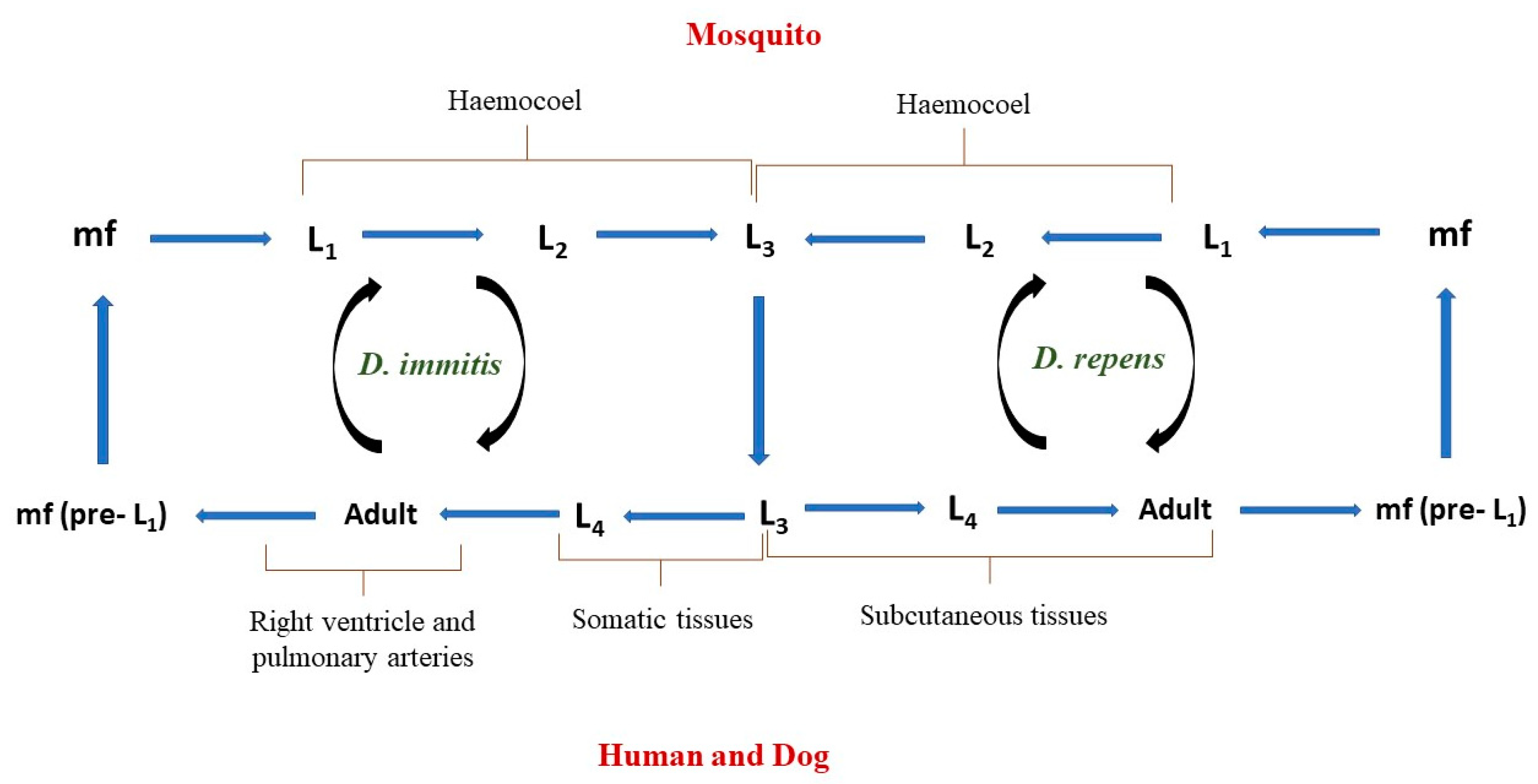
The two major species that are of both medical and veterinary concern are Dirofilaria immitis and D. repens. Infected humans and animals often share similar clinical signs, and the transmission cycles of both parasites are similar up to the point of larval migration in the host. The transmission cycle (Figure 1) begins when a competent vector (mosquito) ingests a blood meal from a Dirofilaria-infected definitive host (e.g., dogs) with microfilaria in its blood. The ingested microfilaria then matures from larval stage 1 to 3 (L1–L3) in the haemocoel of the infected mosquito vector in 2 to 3 weeks and then migrates to the mouth parts of this mosquito. The infective L3 larvae are then transmitted to a definitive host during the bite of this mosquito. Dirofilaria immitis larvae then develop from L3 to L4 in 3 to 12 days in the somatic tissues (e.g., muscles) of the mammalian host and later migrate into the bloodstream to reach the right ventricle and pulmonary arteries, where they moult from the L4 larvae to L5 immature adults, and they mature into adult heartworm in the subsequent 2–3 months. In contrast to D. immitis, D. repens L4 larvae do not migrate but moult and mature into an adult within the subcutaneous tissues. Once mature, adult worms of both species reproduce and produce microfilariae (pre-L1), which are released in the host blood vessels and taken up by a feeding mosquito [7].
While dogs and cats are well recognized as the definitive host, D. repens have, incidentally, been found in other animal species, such as racoons and monkeys, which are considered accidental hosts [8]. Many mosquito species have been identified as competent vectors, such as Armigeres spp., Mansonia spp., Culex spp., and Aedes spp. [9].
The diagnosis of infection is based on specific diagnostic tests. Commercially available veterinary serological test kits based on enzyme-linked immunosorbent assay (ELISA) and immuno-chromatographic test (ICT) can be used for antigen detection of female D. immitis in dogs, and microscopic examination of blood for microfilariae using Knott’s technique is a commonly used modality to identify a patent infection [10]. For D. repens, a blood screening using Knott’s technique is the most commonly used test [5]. In human medicine, radiographic imaging is primarily used to guide the diagnosis of D. immitis, including “coin lesions” revealed on chest X-rays and worm-like morphology on computed tomography (CT) and magnetic resonance imaging (MRI) scans, which is often followed by histological identification of larvae (often disintegrating) on nodule aspirates or excisional biopsies of the affected areas [11,12,13,14]. For D. repens, adult worms in subcutaneous or ocular nodules are extracted by excisional biopsies followed by morphological identification [15].
Treatments for adult D. immitis worm infections in dogs and cats are often complex due to potentially severe complications. One of the major concerns following adulticidal treatment is the sudden uncontrolled worm death post-treatment, which can cause a surge in cytokine release into the bloodstream leading to shock, and a high worm load can be fatal. A high amount of dirofilarial worms can also cause thrombo-embolism in the pulmonary arteries and veins, leading to vascular congestion and hypoxia. Ivermectin is mostly used as a monthly preventative to control heartworm infection in dogs, and melarsomine, in combination with doxycycline, is used as adulticide treatment in infected dogs, with a reported efficacy of 73% [16,17]. It is worth noting that the use of doxycycline (antimicrobial) is primarily to eliminate the Wolbachia bacteria, an endosymbiont of filarial worm, thereby disrupting the life cycle of filarial worms in various developmental stages [18,19]. It appears that doxycycline/ivermectin combination achieves a greater adulticidal effect, possibly by causing adult worm sterility [18,19]. Prednisolone is often used in conjunction to reduce inflammation and minimize the host immune response to the cytokine release associated with the treatment [20]. Although little information is available on the treatment of D. repens in animals, surgical removal of the nodule remains the treatment of choice in human medicine. Albendazole, diethylcarbamazine, and ivermectin are recommended to prevent their recurrence [21,22].
Published studies of D. immitis in dogs identified that dogs aged 5–6 years and male dogs are more likely to be diagnosed with heartworm infection [23,24]. While other animal species, such as domestic cats, ferrets, and wildlife (such as monkeys and wild canids), have also been implicated as susceptible hosts, the risk factors for D. immitis infection in these species are less frequently investigated [25,26,27]. Dirofilaria repens infections are more commonly reported in children and males [28]. Based on our literature search, little is known about the risk factors associated with D. repens infection in animals and D. immitis infection in humans.
While only some Dirofilaria spp. are zoonotic, it should be recognized as a public health risk, especially in parts of the world harbouring mosquito vectors and susceptible host populations. Vector-borne disease dynamics vary between geographical regions and are often driven by local geography and demography [29]. This dynamic is likely to shift unpredictably in certain areas due to climate change. Therefore, we need to widen and deepen our understanding of the distributions of dirofilariasis, particularly in the various regions of Asia, as these are arguably the most affected regions in the world [30].
The prevalence of dirofilariasis varies In different regions of the globe as vector and host distributions vary in different eco-climatic zones (Table 2). Among south Asian countries, Sri Lanka is the most affected, followed by India [6,31,32,33,34,35,36]. Thus, these two neighbouring countries, India and Sri Lanka, can be the appropriate starting point to review our current understanding of the epidemiology of dirofilariasis [6,31,32,33,34,35,36]. Interestingly, although they are neighbouring countries within the same eco-climatic zone and harbour suitable host and vector species, so far, Sri Lanka has only recorded cases of D. repens infection, while India has reported the presence of both D. repens and D. immitis. It remains unknown why these kinds of distribution variations exist between these two countries.
In this manuscript, we performed a systematic review and meta-analysis that summarizes the current understanding and prevalence of dirofilariasis in India and Sri Lanka; the review identifies and compares the prevalence of dirofilariasis between India and Sri Lanka, explores the potential reasons behind the differing prevalence in these neighbouring countries, and suggests the improvement of study designs for future investigations.
2. Materials and Methods
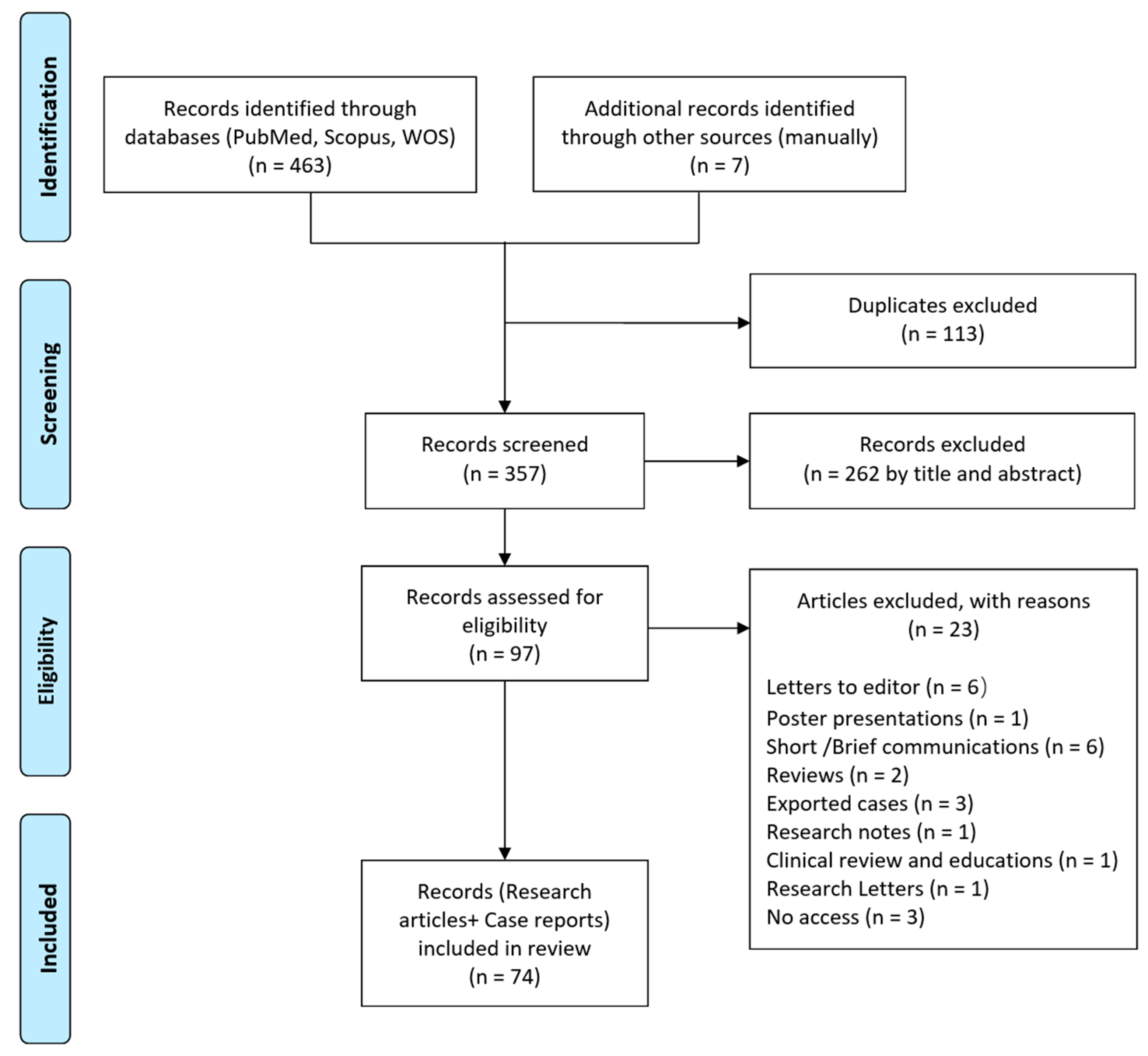
This systematic review was performed according to the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines [49] (Figure 2).
2.1. Strategy of Literature Search
A structured search of electronic databases, namely, PubMed, Scopus, and Web of Science, was performed until 22 February 2022, with no lower limit set to the date of publication. Search terms included pathogens (i.e., “Dirofilaria repens” OR “Dirofilaria immitis” OR “heartworm”) and place (i.e., “India” OR “Sri Lanka”). Bibliographies of review articles were regularly screened for potentially relevant articles and case reports that did not appear in the initial search.
2.2. Inclusion/Exclusion Criteria and Data Extraction
All article types, except original research articles, case reports, and review articles, were excluded. Published articles where the study population did not include humans or dogs were also excluded. Only peer-reviewed articles reporting the prevalence or cases of dirofilariasis in India or Sri Lanka, written in English, with full text available, were included in this manuscript. All records were first screened by titles and abstracts; then, the full text was reviewed prior to final inclusion.
Duplicate records were removed prior to data extraction. For included articles, titles, authors, publication year, type of study, country/state, species, age, sex, parasite, site of infection, the diagnostic technique, and prevalence were extracted and recorded in Microsoft Excel Spreadsheet 2019. Within the dog dataset, dog type was included and categorized into a pet, work, stray, and mixed types. The mixed dog type category included the dogs where the original publication did not specify the types of dogs in their study or did not analyse their data based on dog types.
2.3. Data Analysis
Descriptive statistics were performed and reported as percentages, with a 95% confidence interval (CI) using software package STATA/IC-13.0 (Stata Corp, 4905 Lakeway Drive, College Station, TX, USA). Meta-analysis was performed on the dog data to investigate the crude pooled estimated prevalence of parasitic cases, 95% confidence interval (CI), and the p-value. The studies’ variables were evaluated using the chi-square test on Cochran’s Q statistics (with p-value) followed by I2 statistics to determine the degree of heterogeneity. The weights were chosen to reflect the amount of information each study contains. A random-effect meta-analysis was applied using the “metan” command specifying the random effects due to the high degree of heterogeneity (I2 > 75%) [50]. The outputs were illustrated using a forest plot.
3. Results
The initial search yielded 463 records, of which 113 were duplicates. Out of 357 screened articles, 262 papers were excluded based on titles and abstracts. After screening the full text of the remaining articles, 74 records remained (Figure 2), of which there were 13 (13.6%) relating to dogs and 61 (82.4%) relating to humans. Of the 13 articles relating to dogs, 11 (84.6%) were from India, and 2 (16.4%) were from Sri Lanka (Table 3). Of the 61 articles relating to humans, 49 (80.3%) were from India, with 92 reported cases, and 12 (19.7%) were from Sri Lanka, with 138 reported cases (Table 4).
3.1. Descriptive Statistics of Human Data
The following factors were extracted from articles relating to human Dirofilaria infection: sex, affected body system, diagnostic technique, and parasite species and life cycle (Table 5). Interestingly, D. repens attributed to almost all (97.4%; 224/230) reported human cases. However, the parasitic life stage was not reported in more than 50% of cases. Overall, the incidence rates between males and females were similar, 38.3% (88/230) and 32.2% (74/230), respectively, with the eye (ocular) being the most commonly affected body system at 30.1% (98/260), followed by reproductive organs at 8.8% (23/260) and the oral region at 7.7% (20/260). In terms of diagnostic techniques (in combination or alone), 46% (182/396) of cases were diagnosed with surgical excision, followed by histopathological examination (19.2%; 76/396), and microscopy (14.9%, 59/396).
3.2. Meta-Analysis of Dog Data
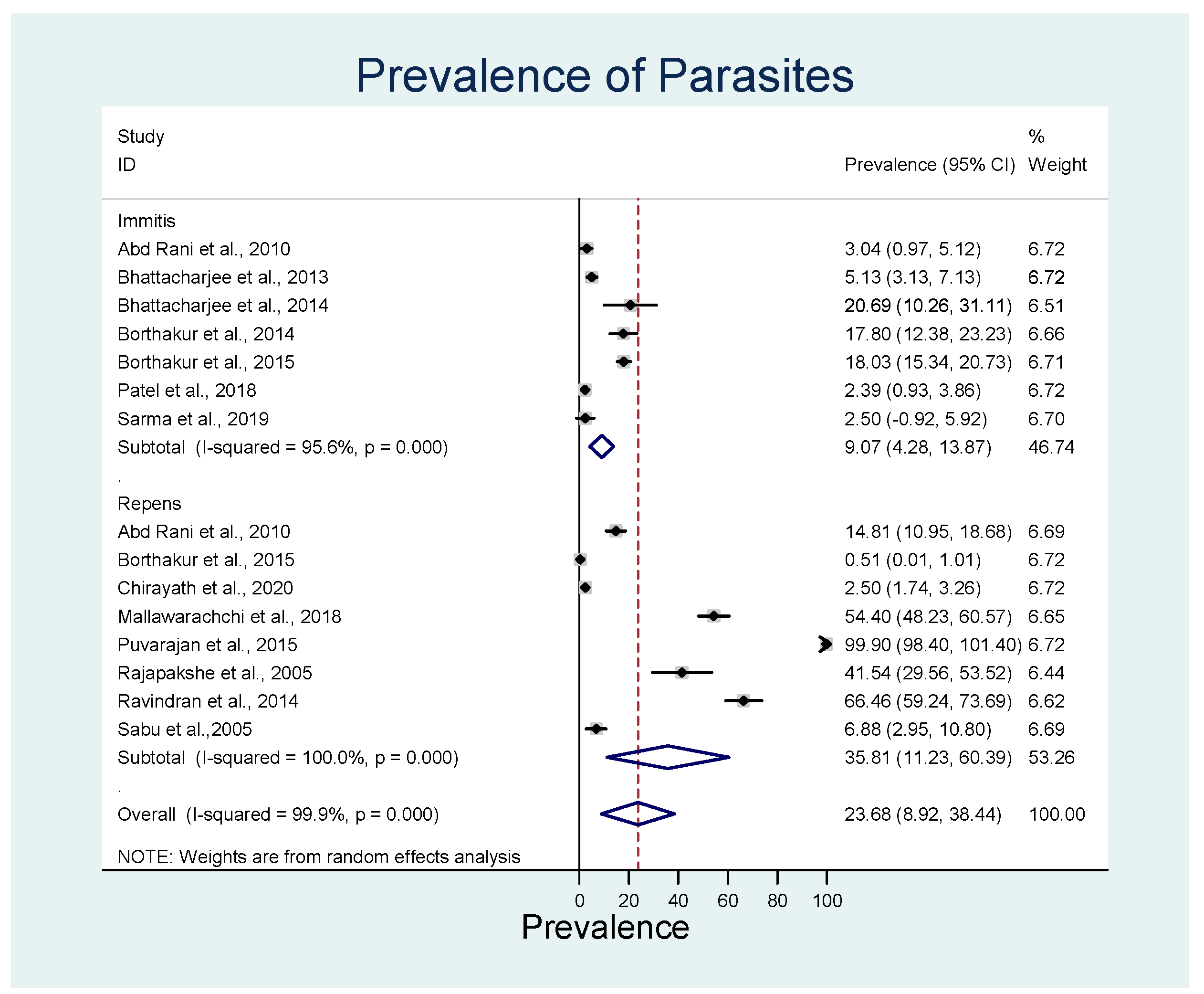
The overall estimated pooled prevalence of D. repens was 35.8% (95% CI: 11.2–60.4%, p < 0.001) with significant heterogeneity of I2 = 100% (p < 0.001), and D. immitis was 9.1% (95% CI: 4.3–13.9%; p < 0.001) with significant heterogeneity (I2 = 95.6%) (Figure 3). D. immitis data represent the prevalence in India, as no cases have been reported from Sri Lanka (Table 6).
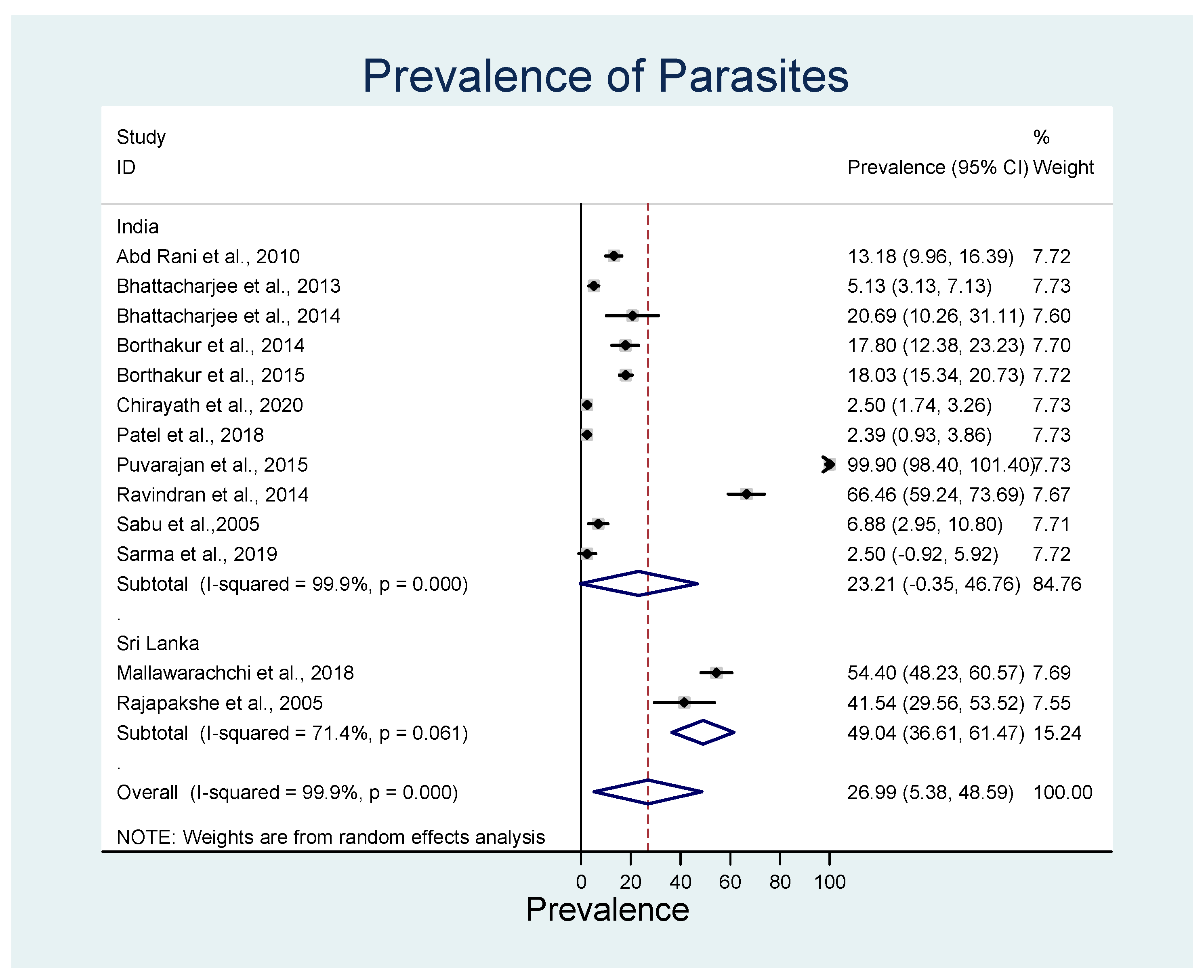
On the country level, the overall estimated pooled prevalence of both parasites in India was 23.2% (95% CI: 46.8–84.8%; p < 0.001) with significant heterogeneity (I2 = 99.9%), and in Sri Lanka, it was 49.0% (95% CI: 36.6–61.5%; p < 0.001) with significant heterogeneity (I2 = 71.4%) (Figure 4). Only D. repens, not D. immitis, has been reported in Sri Lanka.
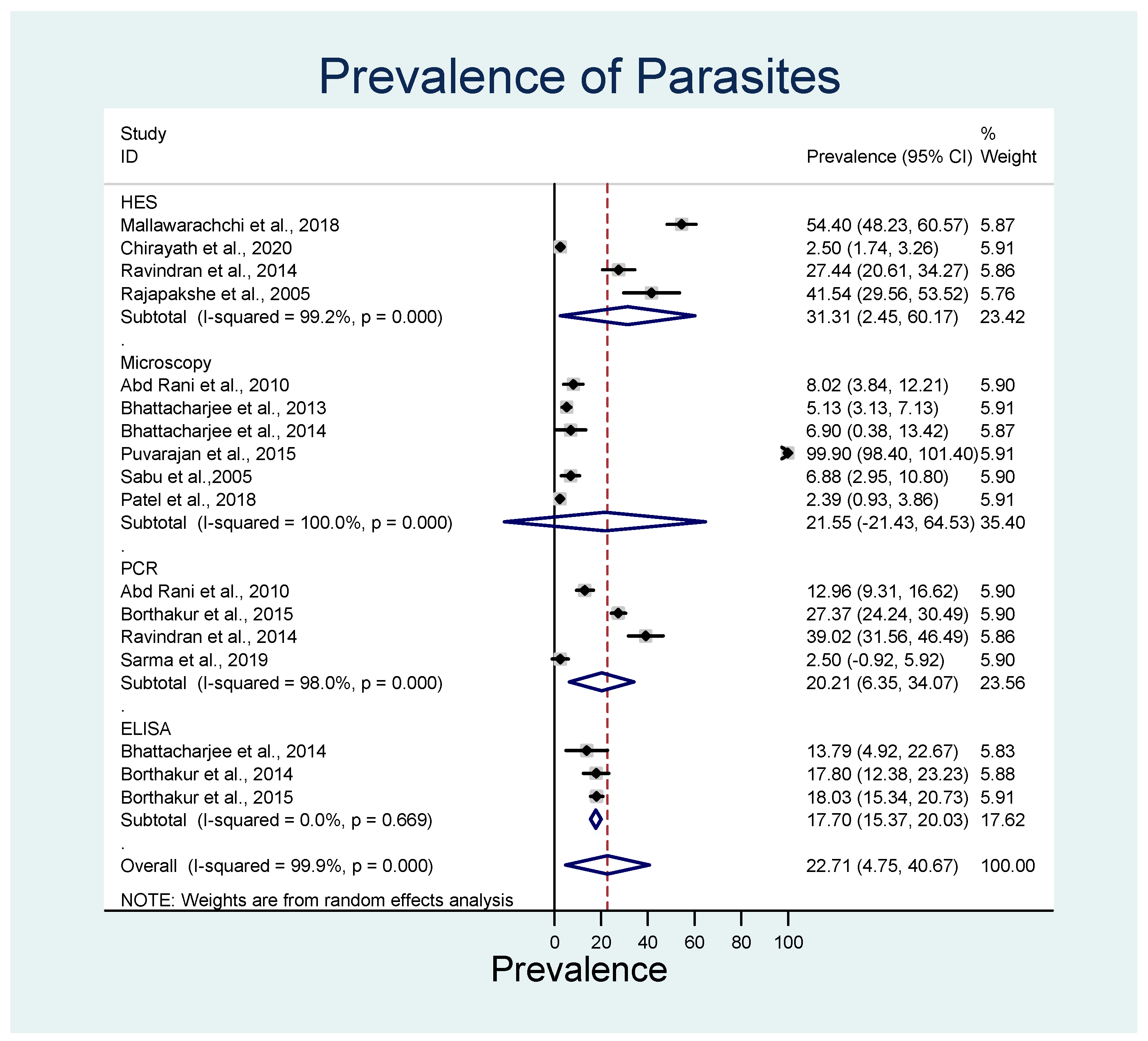
The diagnostic techniques used for the detection of infection were compared. The majority of infections with both the parasite species were identified by histopathology using hematoxylin and eosin staining (HES; 31.3%; 95% CI: 2.5–60.2%; p < 0.001; I2 = 99.2%), followed by techniques that require microscopy, such as wet film, direct smear, and Knott’s test (21.6%; 95% CI 21.4–64.5%; p < 0.001; I2 = 100), and polymerase chain reaction (PCR; 20.2%; 95% CI 6.4–34.1%; p < 0.001; I2 = 98.0) (Figure 5).
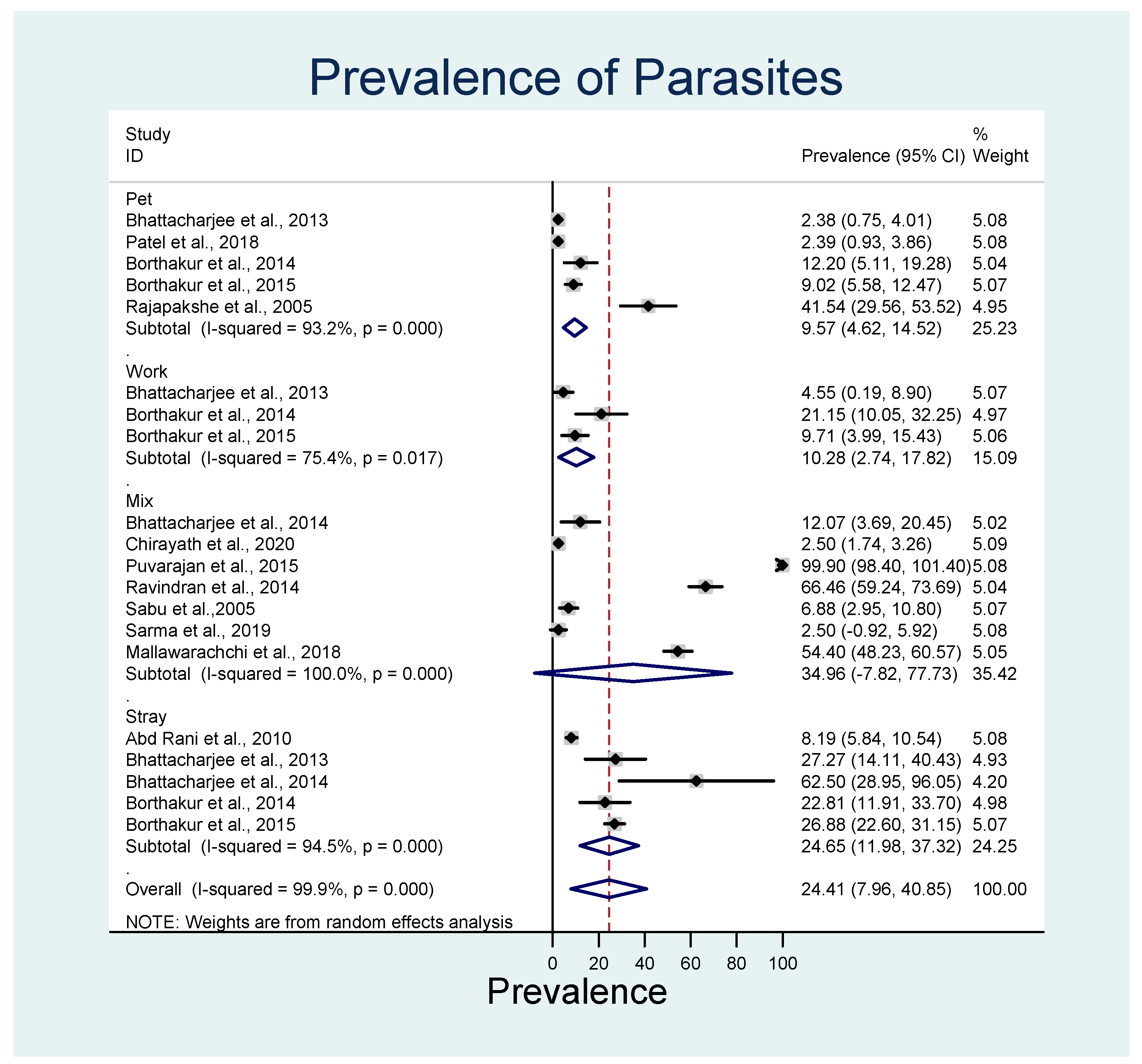
In terms of dog types (i.e., pet, work, stray, or mixed), the overall estimated pooled prevalence of both the parasite species was highest in mixed dog types (35.5%; 95% CI 7.81–77.7%; p < 0.001; I2 = 100), followed by stray dogs (24.65%; 95% CI 12.0–37.3%; p < 0.001; I2 = 94.5) and working dogs (10.3%; 95% CI 2.7–17.8%; p < 0.001; I2 = 75.5) (Figure 6).
4. Discussion
To the best of the authors’ knowledge, this systematic review and meta-analysis represent the first study that summarized the published evidence of Dirofilaria spp. infections in humans and dogs in India and Sri Lanka. The results revealed that D. repens is the dominant Dirofilaria species infecting the dog and human populations in Sri Lanka. In India, a similar prevalence of D. immitis and D. repens was observed in the dog population, and D. repens remains the dominant species being reported to affect humans. In addition, traditional microscopy was the most commonly used diagnostic method in both the counties. Surprisingly, several regions of India and Sri Lanka have not yet been surveyed for dirofilariasis.
The analysis indicates that the prevalence of dirofilariasis in dogs in Sri Lanka is more than twice that of India, with D. repens being the sole Dirofilaria spp. infecting dogs in Sri Lanka, as compared to both D. immitis and D. repens in India. A recent report from the Eastern Province of Sri Lanka confirmed our finding, where almost 60% of dog samples tested positive for D. repens, and none were found positive for D. immitis [117]. While both Dirofilaria spp. are prevalent in India, it is interesting to note that the overall prevalence of dirofilariasis in India is lower than in Sri Lanka. However, this apparent difference may be affected or misrepresented by the random/inconsistent distributions and frequencies of surveyed areas in the two countries.
Human reports of dirofilariasis in both countries were almost exclusively due to D. repens (>97%), which is possibly true given the fact that D. repens can develop to adults in humans [92,118,119] and can occasionally produce microfilariae [120]. On the other hand, humans are suboptimal hosts for D. immitis; as such, the chances of finding the microfilaria in peripheral circulation are negligible [120], which makes diagnosis more difficult. It should be noted that in human medicine, most diagnoses are determined using the histological examination of surgical excisional biopsies, which does not facilitate accurate speciation of Dirofilaria spp. Employing more sensitive molecular assays for human testing could improve the detection of D. immitis infection [121] and improve our understanding of human dirofilariasis.
Another plausible explanation for the higher prevalence of D. repens in the host populations compared to D. immitis in the two countries is that D. repens is more competent in survival and persistence in the vector and/or the host, hence causing more disease in dogs and humans than D. immitis [122]; however, the underlying mechanism remains unknown. A similar phenomenon, termed “viral interference”, has been observed and well described in flaviviral infections in mosquitoes, whereby the presence of one flavivirus suppresses the replication of other flaviviruses in the mosquito [123]. From a preliminary study in 1995 involving experimental infection in dogs, it appears that D. repens may be the dominating species over D. immitis. [122], possibly explaining the higher prevalence of D. repens in both the human and dog populations. The same study also found that re-infection of the host with the same Dirofilaria spp. within 30 days would reduce the parasite burden within the host [122].
Further studies are required to (1) determine the underlying mechanism of the interaction between D. repens and D. immitis within the host and (2) determine whether various Dirofilaria spp. compete within the vector (mosquito), as well as the outcome of such competition, if any. The authors hypothesize that interaction between multiple Dirofilaria spp., such as D. immitis and D. repens in the vector, may lead to interference in the survival and transmission of these pathogens and the resulting prevalence in dogs and humans; however, this needs further investigation.
The analysis indicates that stray dogs were more likely to be tested positive for dirofilariasis. This is likely because these animals roam unrestricted and are not on any preventatives against the parasites, which may increase the chance of these animals being bitten by an infected mosquito. Pet dogs, however, have restricted movement and are usually on parasite preventatives. It is interesting to find that the prevalence of dirofilariasis in working dogs is similar to that of pet dogs, even though the working dogs spend most of the time outdoors in mosquito-prone areas; one possible explanation for this finding is that both pet and working dogs are more likely to receive prophylactic worm treatment. In addition, mosquitoes prefer to feed on resting subjects/animals where there is minimal disruption from the environment or the host during a blood meal. The results from the mixed dog types should be interpreted with care as the proportion of the various dog types are unknown, and results may be skewed towards certain dog types.
Amongst all body systems, the ocular system was found to be the most common site of infection in humans, likely due to mosquitoes’ ease of access to the peri-orbital areas [124]. Unfortunately, due to the nature of the data extracted from the case reports, it was impossible to fit the data into a multivariant regression model for a risk factor analysis. Further, while the risk factors considered in this study are broad and generic, not all studies reported these risk factors, restricting our ability to develop a robust model. However, it is worth noting that the majority of the cases being reported were from Kerala state in India and the central province in Sri Lanka. This indicates that there is a potentially higher risk of contracting D. repens infection in these regions of India and Sri Lanka. Moreover, the possibility that under-reporting or under-diagnosis of dirofilariasis in other regions of India and Sri Lanka leads to the apparent increase in cases in Kerala in India and the Central Province of Sri Lanka cannot be excluded.
The analysis indicates that surgical excision followed by histopathology was the most common diagnostic technique for diagnosing human dirofilariasis. However, histopathology alone is less likely to clearly distinguish between D. immitis and D. repens infection without some underlying assumptions, such as the location of infection. While D. immitis is known to reside in the cardio-pulmonary system, and D. repens resides in the dermatological or subcutaneous tissues, these parasites have been found outside of these common locations. For example, D. immitis has been found in the eye [121,125], reproductive system [126], and gastrointestinal system [127,128]. This could have led to inaccurate published results, which could have affected the results presented in this review. Therefore, the authors suggest that all histopathology-positive results, such as dirofilariasis, should be further characterized by molecular assays using species-specific primers that are more sensitive, specific, and accurate. While microscopy can also provide a definitive diagnosis with confidence, one would require extensive experience to differentiate the various types of Dirofilaria spp.
High heterogeneity has been identified in the meta-analyses of the dog population. This implies that results from various studies vary widely. This could be explained by (1) the various diagnostic techniques used in different studies and (2) the locations of the survey area. Different diagnostic techniques have different sensitivity and specificity, which would affect the prevalence of disease in certain areas. Moreover, the majority of the dog data came from two states/provinces in India/Sri Lanka, namely, Kerala and Assam in India and Western and North-Western provinces in Sri Lanka. It is known that microclimates in the various regions within a country affect mosquito, host, and pathogen distribution, survival, and dispersal, hence the varying degree of disease dynamics and prevalence in different areas. This signifies the need to perform region-based surveillance to monitor dirofilariasis prevalence with standardized diagnostic protocols and techniques, especially in the less-surveyed northern regions of India and Sri Lanka. Longitudinal vector-based studies identifying the variability or similarity of mosquito species and distributions across India and Sri Lanka would provide further understanding of the vector and disease dynamics.
5. Conclusions
India and Sri Lanka, situated in the humid tropical ecoclimatic zone with monsoonal weather patterns, favour the survival of mosquitoes and, thus, the transmission of mosquito-borne diseases. With global warming, climate change, and the emergence of anthelmintic resistance, extreme weather events are likely to become more frequent. The authors hypothesize that dirofilariasis is likely to become more prevalent in India and Sri Lanka, with the potential for the emergence of unidentified Dirofilaria spp. or the introduction of exotic species, as demonstrated recently in Tamil Nadu [129]. Future studies of passive and targeted surveillance should be designed carefully to provide meaningful conclusive results to inform public health measures, facilitate the comparison of results across various studies, and support the monitoring of changes over time.
Author Contributions
Conceptualization, T.C.Y. and S.A.; methodology, S.A.; data curation, S.S.T. and N.K.Y.Y.; statistical analysis, S.S.T., N.K.Y.Y. and M.M.H.; formal analysis and investigation, S.S.T., N.K.Y.Y.; writing—original draft preparation, S.S.T. and N.K.Y.Y.; writing—review and editing, M.M.H., T.C.Y. and S.A.; supervision, S.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Messina, J.P.; Brady, O.J.; Golding, N.; Kraemer, M.U.G.; Wint, G.R.W.; Ray, S.E.; Pigott, D.M.; Shearer, F.M.; Johnson, K.; Earl, L.; et al. The current and future global distribution and population at risk of dengue. Nat. Microbiol. 2019, 4, 1508–1515. [Google Scholar] [CrossRef]
- Yuen, K.Y.; Fraser, N.S.; Henning, J.; Halpin, K.; Gibson, J.S.; Betzien, L.; Stewart, A.J. Hendra virus: Epidemiology dynamics in relation to climate change, diagnostic tests and control measures. One Health 2021, 12, 100207. [Google Scholar] [CrossRef]
- Gray, J.S.; Ogden, N.H. Ticks, human babesiosis and climate change. Pathogens 2021, 10, 1430. [Google Scholar] [CrossRef]
- Franklinos, L.H.V.; Jones, K.E.; Redding, D.W.; Abubakar, I. The effect of global change on mosquito-borne disease. Lancet Infect. Dis. 2019, 19, e302–e312. [Google Scholar] [CrossRef]
- Capelli, G.; Genchi, C.; Baneth, G.; Bourdeau, P.; Brianti, E.; Cardoso, L.; Danesi, P.; Fuehrer, H.-P.; Giannelli, A.; Ionicǎ, A.M.; et al. Recent advances on Dirofilaria repens in dogs and humans in Europe. Parasit. Vectors 2018, 11, 663. [Google Scholar] [CrossRef]
- Kini, R.G.; Leena, J.B.; Shetty, P.; Lyngdoh, R.H.; Sumanth, D.; George, L. Human dirofilariasis: An emerging zoonosis in India. J. Parasit. Dis. 2015, 39, 349–354. [Google Scholar] [CrossRef]
- Hoch, H.; Strickland, K. Canine and feline dirofilariasis: Life cycle, pathophysiology, and diagnosis. Compend. Contin. Educ. Vet. 2008, 30, 133–141. [Google Scholar]
- Dissanaike, A.S. Human infections with Dirofilaria, a filarial parasite of animals in Ceylon, with a brief review of recent cases. Ceylon Med. J. 1971, 16, 91–99. [Google Scholar]
- Dissanaike, A.S.; Abeyewickreme, W.; Wijesundera, M.D.; Weerasooriya, M.V.; Ismail, M.M. Human dirofilariasis caused by Dirofilaria (Nochtiella) repens in Sri Lanka. Parassitologia 1997, 39, 375–382. [Google Scholar]
- Sonnberger, K.; Duscher, G.G.; Fuehrer, H.P.; Leschnik, M. Current trends in canine dirofilariosis in Austria-do we face a pre-endemic status? Parasitol. Res. 2020, 119, 1001–1009. [Google Scholar] [CrossRef]
- Smitha, M.; Rajendran, V.R.; Devarajan, E.; Anitha, P.M. Case report: Orbital dirofilariasis. Indian J. Radiol. Imaging 2008, 18, 60–62. [Google Scholar] [CrossRef]
- Joseph, E.; Matthai, A.; Abraham, L.K.; Thomas, S. Subcutaneous human dirofilariasis. J. Parasit. Dis. 2011, 35, 140–143. [Google Scholar] [CrossRef]
- Kurup, S.; Veeraraghavan, R.; Jose, R.; Puthalath, U. Filariasis of the buccal mucosa: A diagnostic dilemma. Contemp. Clin. Dent. 2013, 4, 254–257. [Google Scholar] [CrossRef]
- Premakumar, P.; Nair, V.V.; Nair, B.J.; Thomas, S.; Alex, V.D.; Thomas, J.; Prasanna, R.A. Discussion of a case of dirofilariasis presenting as a nodular mass. Int. J. Occup. Environ. Health 2014, 2, 301–307. [Google Scholar]
- Diaz, J.H. Increasing risks of human dirofilariasis in travelers. J. Travel Med. 2015, 22, 116–123. [Google Scholar] [CrossRef]
- Bazzocchi, C.; Mortarino, M.; Grandi, G.; Kramer, L.H.; Genchi, C.; Bandi, C.; Genchi, M.; Sacchi, L.; McCall, J.W. Combined ivermectin and doxycycline treatment has microfilaricidal and adulticidal activity against Dirofilaria immitis in experimentally infected dogs. Int. J. Parasitol. 2008, 38, 1401–1410. [Google Scholar] [CrossRef]
- Grandi, G.; Quintavalla, C.; Mavropoulou, A.; Genchi, M.; Gnudi, G.; Bertoni, G.; Kramer, L. A combination of doxycycline and ivermectin is adulticidal in dogs with naturally acquired heartworm disease (Dirofilaria immitis). Vet. Parasitol. 2010, 169, 347–351. [Google Scholar] [CrossRef]
- McCall, J.W.; Genchi, C.; Kramer, L.; Guerrero, J.; Dzimianski, M.T.; Supakorndej, P.; Mansour, A.M.; McCall, S.D.; Supakorndej, N.; Grandi, G.; et al. Heartworm and Wolbachia: Therapeutic implications. Vet. Parasitol. 2008, 158, 204–214. [Google Scholar] [CrossRef]
- Kramer, L.; Crosara, S.; Gnudi, G.; Genchi, M.; Mangia, C.; Viglietti, A.; Quintavalla, C. Wolbachia, doxycycline and macrocyclic lactones: New prospects in the treatment of canine heartworm disease. Vet. Parasitol. 2018, 254, 95–97. [Google Scholar] [CrossRef]
- Atwell, R.; Tarish, J.H. The effect of oral, low-dose prednisolone on the extent of pulmonary pathology associated with dead Dirofilaria immitis in a canine lung model. In Proceedings of the Heartworm Symposium ’95, Auburn, AL, USA, 31 March–2 April 1995; pp. 103–111. [Google Scholar]
- Lupșe, M.; Mircean, V.; Cavasi, A.; Mihalca, A.D. Recurrent subcutaneous human dirofilariasis due to Dirofilaria repens after surgical removal of the worm and anthelmintic treatment. Parasit. Vectors 2014, 7 (Suppl 1), P3. [Google Scholar] [CrossRef]
- Peter, J.; Thomas, P.; Mathew, D.G.; George, E. Human dirofilariasis. Online J. Health Allied Sci. 2020, 19, 1–3. [Google Scholar]
- Song, K.H.; Lee, S.E.; Hayasaki, M.; Shiramizu, K.; Kim, D.H.; Cho, K.W. Seroprevalence of canine dirofilariosis in South Korea. Vet. Parasitol. 2003, 114, 231–236. [Google Scholar] [CrossRef]
- Traversa, D.; Aste, G.; Milillo, P.; Capelli, G.; Pampurini, F.; Tunesi, C.; Santori, D.; Paoletti, B.; Boari, A. Autochthonous foci of canine and feline infections by Dirofilaria immitis and Dirofilaria repens in central Italy. Vet. Parasitol. 2010, 169, 128–132. [Google Scholar] [CrossRef]
- Venco, L.; Marchesotti, F.; Manzocchi, S. Feline heartworm disease: A ‘Rubik’s-cube-like’ diagnostic and therapeutic challenge. J. Vet. Cardiol. 2015, 17, S190–S201. [Google Scholar] [CrossRef]
- Bowman, D.D.; Liu, Y.; McMahan, C.S.; Nordone, S.K.; Yabsley, M.J.; Lund, R.B. Forecasting United States heartworm Dirofilaria immitis prevalence in dogs. Parasit. Vectors 2016, 9, 1–12. [Google Scholar] [CrossRef]
- Alsarraf, M.; Dwużnik-Szarek, D.; Hildebrand, J.; Mierzejewska, E.J.; Kloch, A.; Kot, K.; Kurek, K.; Nowak, S.; Mysłajek, R.W.; Myśliwy, I.; et al. Occurrence of Dirofilaria repens in wild carnivores in Poland. Parasitol. Res. 2023, 122, 1229–1237. [Google Scholar] [CrossRef]
- Pampiglione, S.; Canestri Trotti, G.; Rivasi, F. Human dirofilariasis due to Dirofilaria (Nochtiella) repens: A review of world literature. Parassitologia 1995, 37, 149–193. [Google Scholar]
- Murdock, C.C.; Evans, M.V.; McClanahan, T.D.; Miazgowicz, K.L.; Tesla, B. Fine-scale variation in microclimate across an urban landscape shapes variation in mosquito population dynamics and the potential of Aedes albopictus to transmit arboviral disease. PLoS Negl. Trop. Dis. 2017, 11, e0005640. [Google Scholar] [CrossRef]
- Genchi, C.; Kramer, L.H. The prevalence of Dirofilaria immitis and D. repens in the Old World. Vet. Parasitol. 2020, 280, 108995. [Google Scholar] [CrossRef]
- Khyriem, A.B.; Lynrah, K.G.; Lyngdoh, W.V.; Banik, A. Subcutaneous dirofilariasis. Indian J. Med. Microbiol. 2013, 31, 403–405. [Google Scholar] [CrossRef]
- Nath, R.; Bhuyan, S.; Dutta, H.; Saikia, L. Human subcutaneous dirofilariasis in Assam. Trop. Parasitol. 2013, 3, 75–78. [Google Scholar] [CrossRef]
- Bhattacharjee, K.; Sarmah, P.C. Epidemiological aspects of Dirofilaria immitis infection in dogs from Assam of northeast India. Asian Pac. J. Trop. Dis. 2014, 4, S255–S258. [Google Scholar] [CrossRef]
- Borthakur, S.K.; Roychoudhury, P.; Bhattacharjee, K.; Islam, S.; Deka, D.K.; Sarmah, P.C. Dirofilaria repens in dogs from Assam, India. Asian Pac. J. Trop. Dis. 2015, 5, 445–447. [Google Scholar] [CrossRef]
- Ravindran, R.; Julie, B.; Swapna, S.A.; Jerin, F.; Jyothimol, G.; Lenka, D.R.; Nandakumar, S.; Sabu, S.M. Dirofilaria repens in scrotum of dogs. Trop. Biomed. 2016, 33, 842–846. [Google Scholar] [PubMed]
- Malviya, V.; Goyal, S. A case report on facial subcutaneous dirofilariasis with intraoral extension. Int. Surg. J. 2020, 7, 2755. [Google Scholar] [CrossRef]
- Simón, F.; González-Miguel, J.; Diosdado, A.; Gómez, P.J.; Morchón, R.; Kartashev, V. The complexity of zoonotic filariasis episystem and its consequences: A multidisciplinary view. Biomed. Res. Int. 2017, 2017, 6436130. [Google Scholar] [CrossRef]
- Cimpan, A.A.; Baneth, G.; Nachum-Biala, Y.; Miron, L.; Rojas, A. Dirofilaria repens predominates in shelter dogs from south Romania. Comp. Immunol. Microbiol. Infect. Dis. 2022, 84, 101793. [Google Scholar] [CrossRef]
- Miterpakova, M.; Valentova, D.; Cabanova, V.; Beresikova, L. Heartworm on the rise—New insights into Dirofilaria immitis epidemiology. Parasitol. Res. 2018, 117, 2347–2350. [Google Scholar] [CrossRef]
- Iliev, P.; Kirkova, Z.; Ivanov, A.; Prelezov, P.; Tonev, A.; Kalkanov, I. Retrospective analysis on helminthic and protozoan infections in dogs and cats in Bulgaria. Bulg. J. Vet. Med. 2017, 1477, 389–393. [Google Scholar]
- Kartashev, V.; Batashova, I.; Kartashov, S.; Ermakov, A.; Mironova, A.; Kuleshova, Y.; Ilyasov, B.; Kolodiy, I.; Klyuchnikov, A.; Ryabikina, E.; et al. Canine and human dirofilariosis in the Rostov Region (Southern Russia). Vet. Med. Int. 2010, 2011, 685713–685715. [Google Scholar] [CrossRef]
- Tumolskaya, N.I.; Pozio, E.; Rakova, V.M.; Supriaga, V.G.; Sergiev, V.P.; Morozov, E.N.; Morozova, L.F.; Rezza, G.; Litvinov, S.K. Dirofilaria immitis in a child from the Russian Federation. Parasite 2016, 23, 37. [Google Scholar] [CrossRef] [PubMed]
- Bamorovat, M.; Sharifi, I.; Fasihi Harandi, M.; Nasibi, S.; Sadeghi, B.; Khedri, J.; Mohammadi, M.A. Parasitological, serological and molecular study of Dirofilaria immitis in domestic dogs, southeastern Iran. Iran. J. Parasitol. 2017, 12, 260–266. [Google Scholar]
- Rjeibi, M.R.; Rouatbi, M.; Mabrouk, M.; Tabib, I.; Rekik, M.; Gharbi, M. Molecular study of Dirofilaria immitis and Dirofilaria repens in dogs from Tunisia. Transbound. Emerg. Dis. 2017, 64, 1505–1509. [Google Scholar] [CrossRef] [PubMed]
- Mallawarachchi, C.H.; Chandrasena, N.T.G.A.; Wickramasinghe, S.; Premaratna, R.; Gunawardane, N.Y.I.S.; Mallawarachchi, N.S.M.S.M.; de Silva, N.R. A preliminary survey of filarial parasites in dogs and cats in Sri Lanka. PLoS ONE 2018, 13, e0206633. [Google Scholar] [CrossRef] [PubMed]
- Satjawongvanit, H.; Phumee, A.; Tiawsirisup, S.; Sungpradit, S.; Brownell, N.; Siriyasatien, P.; Preativatanyou, K. Molecular analysis of canine filaria and its wolbachia endosymbionts in domestic dogs collected from two animal university hospitals in Bangkok metropolitan region, Thailand. Pathogens 2019, 8, 114. [Google Scholar] [CrossRef] [PubMed]
- Simsek, S.; Utuk, A.E.; Koroglu, E.; Rishniw, M. Serological and molecular studies on Dirofilaria immitis in dogs from Turkey. J. Helminthol. 2008, 82, 181–186. [Google Scholar] [CrossRef]
- Bailey, R.G. Ecosystem Geography From Ecoregions to Sites, 2nd ed.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Statist. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Sabu, L.; Devada, K.; Subramanian, H. Dirofilariosis in dogs and humans in Kerala. Indian J. Med. Res. 2005, 121, 691–693. [Google Scholar]
- Ravindran, R.; Varghese, S.; Nair, S.N.; Balan, V.M.; Lakshmanan, B.; Ashruf, R.M.; Kumar, S.S.; Gopalan, A.K.; Nair, A.S.; Malayil, A.; et al. Canine filarial infections in a human Brugia malayi endemic area of India. Biomed Res. Int. 2014, 2014, 630160. [Google Scholar] [CrossRef]
- Chirayath, D.; Alex, P.C.; Pillai, U.N. Molecular characterization of 5S ribosomal spacer sequences of Dirofilaria repens microfilariae in dogs in Kerala, India. J. Parasit. Dis. 2020, 44, 864–868. [Google Scholar] [CrossRef]
- Bhattacharjee, K.; Sarmah, P.C. Prevalence of haemoparasites in pet, working and stray dogs of Assam and North-East India: A hospital based study. Vet. World 2013, 6, 874–878. [Google Scholar] [CrossRef]
- Bhattacharjee, K.; Sarmah, P.C.; Barman, N.N. Seroprevalence of vector borne parasites in naturally exposed dogs of Assam, India. Vet. World 2014, 7, 87–89. [Google Scholar] [CrossRef]
- Borthakur, S.K.; Deka, D.K.; Bhattacharjee, K.; Sarmah, P.C. Seroprevalence of canine dirofilariosis, granulocytic anaplasmosis and lyme borreliosis of public health importance in dogs from India’s North East. Vet. World 2014, 7, 665–667. [Google Scholar] [CrossRef]
- Borthakur, S.K.; Deka, D.K.; Islam, S.; Sarma, D.K.; Sarmah, P.C. Prevalence and molecular epidemiological data on dirofilaria immitis in dogs from Northeastern States of India. Sci. World J. 2015, 2015, 265385. [Google Scholar] [CrossRef]
- Sarma, K.; Nachum-Biala, Y.; Kumar, M.; Baneth, G. Molecular investigation of vector-borne parasitic infections in dogs in Northeast India. Parasit. Vectors 2019, 12, 122. [Google Scholar] [CrossRef]
- Megat Abd Rani, P.A.; Irwin, P.J.; Gatne, M.; Coleman, G.T.; McInnes, L.M.; Traub, R.J. A survey of canine filarial diseases of veterinary and public health significance in India. Parasit. Vectors 2010, 3, 30. [Google Scholar] [CrossRef]
- Puvarajan, B.; Ramakrishnan, K.S.; Jeyathilakan, N.; Tamilam, T.V. Canine subcutaneous Dirofilariosis (D. repens) in Western Tamilnadu. Indian Vet. J. 2016, 93, 71–72. [Google Scholar]
- Patel, J.R.; Devi, S.; Varshney, J.P.; Jadhav, K.M. Epizootiological observations on canine microfilaremia in Gujarat state, India. Vet. World 2018, 11, 1564–1568. [Google Scholar] [CrossRef]
- Rajapakshe, R.P.; Perera, W.S.; Ihalamulla, R.L.; Weerasena, K.H.; Jayasinghe, S.; Sajeewani, H.B.; Thammitiyagodage, M.G.; Karunaweera, N.D. Study of dirofilariasis in a selected area in the Western Province. Ceylon Med. J. 2005, 50, 58–61. [Google Scholar] [CrossRef]
- Permi, H.S.; D’Souza, C.; Bhagavan, K.R.; Raju, M.; Sarda, P. Human dirofilariasis due to D. repens presenting as a chest wall swelling: A rare case report. Nitte Univ. J. Health Sci. 2012, 2, 51–53. [Google Scholar]
- Permi, H.S.; Veena, S.; Kishan Prasad, H.L.; Kumar, Y.S.; Mohan, R.; Shetty, K.J. Subcutaneous human dirofilariasis due to Dirofilaria repens: Report of two cases. J. Glob. Infect. Dis. 2011, 3, 199–201. [Google Scholar] [CrossRef]
- Achappa, B.; Madi, D.; Mahalingam, S. An interesting case of a subcutaneous nodule. J. Clin. Diagn. Res. 2013, 7, 364–365. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, T.N.; Lakshmi, K.P.; Shaji, P.C.; Rajalakshmi, P.C. Periorbital dirofilariasis-clinical and imaging findings: Live worm on ultrasound. Indian J. Ophthalmol. 2013, 61, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Rai, R.; Karnaker, V.K.; Naik, J. An unanticipated cause of intramuscular mass—A case report. Nitte Univ. J. Health Sci. 2014, 4, 118–119. [Google Scholar] [CrossRef]
- Janardhanan, M.; Rakesh, S.; Savithri, V. Oral dirofilariasis. Indian J. Dent. Res. 2014, 25, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Yaranal, P.J.; Priyadarshini, M.M.; Purushotham, B. Human subcutaneous dirofilariasis of forearm an unusual presentation. Indian J. Dermatol. 2015, 60, 103. [Google Scholar] [CrossRef]
- Guptha, S.S.; Ranjakumar, T.C.; Sundaram, L.; Ashraf, R.M.; Adil, S.; Hisha, M. Beware of foreign body sensation” this live worm can swim through your eye!—A case series on increasing prevalence of ocular dirofilariasis in tropical India: A disease of travel to foreign lands. Int. J. Recent Surg. Med. Sci. 2015, 1, 26–30. [Google Scholar]
- Manuel, S.; Surej Kumar, L.K.; Khalam, S.A. Oral dirofilariasis: Report of a case arising in the buccal vestibular region. J. Oral Maxillofac. Surg. Med. Pathol. 2015, 27, 418–421. [Google Scholar] [CrossRef]
- Nazar, N.; Lakshmanan, B.; Jayavardhanan, K.K. Molecular characterization of human Dirofilaria isolates from Kerala. Indian J. Med. Res. 2017, 146, 528–533. [Google Scholar] [CrossRef]
- Seema, K.M. A case of pediatric ocular dirofilariasis. Kerala J. Ophthalmol. 2017, 29, 136–138. [Google Scholar] [CrossRef]
- Nambiara, A.; Manappallilb, R.; Nambiarc, H.; Shamsudeenda, Z. Pericardial effusion: An untold presentation of human dirofilariasis. IHJ Cardiovasc. Case Rep. 2018, 2, 79–81. [Google Scholar] [CrossRef]
- Rajan, R.P.; Jena, S.; Ramachandran, N.O.; Kohli, P. Rare cause of floaters: A motile live worm in vitreous cavity. Indian J. Ophthalmol. 2019, 67, 1490–1492. [Google Scholar] [CrossRef] [PubMed]
- Mani, A.; Khan, M.A.; Kumar, V.P. Subcutaneous dirofilariasis of the eyelid. Med. J. Armed Forces India 2019, 75, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Aswathi, T.V.; Sreelesh, L.S.; Rajan, T.M.S.; Geethu, G.N. A case of human subcutaneous dirofilariasis presenting as urticaria. Indian J. Surg. 2021, 83, 931–933. [Google Scholar] [CrossRef]
- Sanjeev, H.; Rajini, M.; Prasad, S.R. Human dirofilariasis: An uncommon case of subcutaneous infection with Dirofilaria repens with a brief review of literature. Nitte Univ. J. Health Sci. 2011, 1, 60–62. [Google Scholar]
- Nadgir, S.; Tallur, S.S.; Mangoli, V.; Halesh, L.H.; Krishna, B.V. Subconjunctival dirofilariasis in India. Southeast Asian J. Trop. Med. Public Health 2001, 32, 244–246. [Google Scholar]
- Shenoi, S.D.; Kumar, P.; Johnston, S.P.; Khadilkar, U.N. Cutaneous dirofilariasis presenting as an eyelid swelling. Trop. Doct. 2009, 39, 189–190. [Google Scholar] [CrossRef]
- Shenoi, S.D.; Kumar, P.; Khadilkar, U.; Johnston, S. Crusted papule on forehead due to Dirofilaria repens. Trop. Doct. 2005, 35, 181–182. [Google Scholar] [CrossRef]
- Singh, R.; Shwetha, J.V.; Samantaray, J.C.; Bando, G. Dirofilariasis: A rare case report. Indian J. Med. Microbiol. 2010, 28, 75–77. [Google Scholar] [CrossRef]
- Acharya, D.; Chatra, P.S.; Padmaraj, S.R.; Ahamed, A. Subcutaneous dirofilariasis. Singapore Med. J. 2012, 53, e184–e185. [Google Scholar] [PubMed]
- Srinivasamurthy, V.; Rao, M.; Thejaswini, M. Human subcutaneous dirofilariasis. Ann. Trop. Med. Public Health 2012, 5, 349–351. [Google Scholar] [CrossRef]
- Kotigadde, S.; Ramesh, S.A.; Medappa, K.T. Human dirofilariasis due to Dirofilaria repens in southern India. Trop. Parasitol. 2012, 2, 67–68. [Google Scholar] [CrossRef] [PubMed]
- Bhat, K.S.; Kotigadde, S.; Vishwanatha Bhat, K.; Pare, P. Subconjunctival dirofilariasis: Case studies with review of literature. Trop. Parasitol. 2014, 4, 119–121. [Google Scholar] [CrossRef]
- Shankar, M.K.; Shet, S.; Gupta, P.; Nadgir, S.D. Sac over the sac—A rare case of subcutaneous dirofilariasis over the lacrimal sac area. Nepal. J. Ophthalmol. 2014, 6, 224–226. [Google Scholar] [CrossRef]
- Bhat, S.; Saldanha, M.; Mendonca, N. Periocular dirofilariasis: A case series. Orbit 2016, 35, 100–102. [Google Scholar] [CrossRef]
- Nagaraja, H.R.; Deshmukh, A.; Shivanna, Y.; Thungappa, K.S.; Rohit, S. Ocular parasitosis: A report of two contrasting cases. Arch. Clin. Microbiol. 2017, 8, 3–5. [Google Scholar]
- Murthy, N.; Gopi, A.; Bele-Kenge, P. Subcutaneous dirofilariasis of the cheek with microfilaremia. Ann. Trop. Med. Public Health 2018, 11, 95–99. [Google Scholar] [CrossRef]
- Shambhu, S.K.; Murthy, P.R.; D’Souza P, E.; Hanumappa, D.; Vikram, H.R.; Janardhana, G.C.; Matada, R. Subconjunctival dirofilariasis presenting as orbital cellulitis. Ophthalmic Plast. Reconstr. Surg. 2019, 35, e97–e99. [Google Scholar] [CrossRef]
- Damle, A.S.; Iravane Bajaj, J.A.; Khaparkhuntikar, M.N.; Maher, G.T.; Patil, R.V. Microfilaria in human subcutaneous dirofilariasis: A case report. J. Clin. Diagn. Res. 2014, 8, 113–114. [Google Scholar] [CrossRef]
- Desai, R.S.; Pai, N.; Nehete, A.P.; Singh, J.S. Oral dirofilariasis. Indian J. Med. Microbiol. 2015, 33, 593–594. [Google Scholar] [CrossRef]
- Kombade, S.P.; Mantri, R.S.; Ambhore, N.A.; Karyakarte, R.P. Subcutaneous human Dirofilariasis in Vidarbha. Indian J. Pathol. Microbiol. 2015, 58, 387–388. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, S.; Kulkarni, V. Periorbital dirofilariasis: A rare case from western India. J. Clin. Diagn. Res. 2016, 10, Od12–Od14. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Agrawal, R.; Shastri, J. Ocular Dirofilariasis: A rare case from Mumbai, India. J. Clin. Diagn. Res. 2017, 11, Dd09–dd10. [Google Scholar] [CrossRef] [PubMed]
- Behl, S.S.; Fasahtay, A. Subconjunctival dirofilariasis after cataract surgery. JCRS Online Case Rep. 2017, 5, 52–53. [Google Scholar] [CrossRef]
- Gandham, N.; Mirza, S.; Das, N.; Misra, R. A rare case of subcutaneous dirofilariasis from a tertiary care hospital in Western Maharashtra. Med. J. Dr. D.Y. Patil Vidyapeeth 2021, 14, 80–83. [Google Scholar] [CrossRef]
- Nath, R.; Gogoi, R.; Bordoloi, N.; Gogoi, T. Ocular dirofilariasis. Indian J. Pathol. Microbiol. 2010, 53, 157–159. [Google Scholar] [CrossRef]
- Das, D.; Das, K.; Islam, S.; Bhattacharjee, K.; Bhattacharjee, H.; Das, S.M.; Deka, A. A rare case of anterior chamber dirofilariasis. Oman J. Ophthalmol. 2015, 8, 50–53. [Google Scholar] [CrossRef]
- Sathyan, P.; Manikandan, P.; Bhaskar, M.; Padma, S.; Singh, G.; Appalaraju, B. Subtenons infection by Dirofilaria repens. Indian J. Med. Microbiol. 2006, 24, 61–62. [Google Scholar] [CrossRef]
- Jacob, S.; Parameswaran, A.; Santosham, R.; Santosham, R. Human pulmonary dirofilariasis masquerading as a mass. Asian Cardiovasc. Thorac. Ann. 2016, 24, 722–725. [Google Scholar] [CrossRef]
- Chopra, R.; Bhatti, S.M.; Mohan, S.; Taneja, N. Dirofilaria in the anterior chamber: A rare occurrence. Middle East Afr. J. Ophthalmol. 2012, 19, 349–351. [Google Scholar] [CrossRef]
- Agrawal, S.; Modaboyina, S.; Raj, N.; Das, D.; Bajaj, M.S. Eyelid Dirofilaria during COVID-19 Pandemic: A telemedicine diagnosis. Cureus 2021, 13, e15525. [Google Scholar] [CrossRef] [PubMed]
- Spadigam, A.; Dhupar, A.; Syed, S.; Sawant, P.R. Human oral dirofilariasis. Trop. Parasitol. 2018, 8, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Ratnatunga, N.; Wijesundera, M.S. Histopathological diagnosis of subcutaneous Dirofilaria repens infection in humans. Southeast Asian J. Trop. Med. Public Health 1999, 30, 375–378. [Google Scholar] [PubMed]
- Tilakaratne, W.M.; Pitakotuwage, T.N. Intra-oral Dirofilaria repens infection: Report of seven cases. J. Oral Pathol. Med. 2003, 32, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Iddawela, D.; Ehambaram, K.; Wickramasinghe, S. Human ocular dirofilariasis due to Dirofilaria repens in Sri Lanka. Asian Pac. J. Trop. Med. 2015, 8, 1022–1026. [Google Scholar] [CrossRef] [PubMed]
- Jayasinghe, R.D.; Gunawardane, S.R.; Sitheeque, M.A.; Wickramasinghe, S. A case report on oral subcutaneous dirofilariasis. Case Rep. Infect. Dis. 2015, 2015, 648278. [Google Scholar] [CrossRef]
- Gunathilaka, N.; Siriwardana, S.; Wijesooriya, L.; Gunaratne, G.; Perera, N. Subcutaneous dirofilariasis caused by Dirofilaria (Nochtiella) repens in Sri Lanka: A potential risk of transmitting human dirofilariasis. SAGE Open Med. Case Rep. 2017, 5, 2050313X17701373. [Google Scholar] [CrossRef]
- Ratnavale, W.D.; Dissanaike, A.S. On the second case of human infection with Dirofilaria (Nochtiella) repens from Ceylon. J. Helminthol. 1964, 38, 287–290. [Google Scholar] [CrossRef]
- Senanayake, M.P.; Infaq, M.L.; Adikaram, S.G.; Udagama, P.V. Ocular and subcutaneous dirofilariasis in a Sri Lankan infant: An environmental hazard caused by dogs and mosquitoes. Paediatr. Int. Child Health 2013, 33, 111–112. [Google Scholar] [CrossRef]
- Sinhabahu, V.P.; Hettiarachchi, J.; Gamage, M.; Beneragama, D.H. A child with an unusual lump in the cheek. Sri Lanka J. Child Health 2018, 47, 89–90. [Google Scholar] [CrossRef]
- Chandrasena, T.G.A.N.; Premaratna, R.; Mallawaarachchi, C.H.; Gunawardena, N.K.; Gunathilaka, P.A.D.H.N.; Abeyewickrama, W.Y.; Silva, N.R.d. The diversity of human dirofilariasis in Western Sri Lanka. Biomed. Res. Int. 2019, 2019, 9209240–9209247. [Google Scholar] [CrossRef] [PubMed]
- Weerasekera, C.J.; Hapuachchige, C.; Wijeratne, Y.M.T.Y.; Goonesinghe, R.; Wickremasinghe, D.R.; Yahathugoda, T.C.; Ranasinghe, S. Omental dirofilariasis caused by Dirofilaria repens; visceralisation in a patient with diabetes mellitus. J. Ceylon Coll. Physicians 2021, 52, 105. [Google Scholar] [CrossRef]
- de Silva, G.P.U.P.; Udugampola, D.S.; Ekanayake, E.M.I.B.; Fonseka, K.V.S.; Karunadasa, M.S.E. An underrated differential diagnosis for subcutaneous lumps: 26 cases of subcutaneous Dirofilariasis. Sri Lanka J. Surg. 2021, 39, 31. [Google Scholar] [CrossRef]
- Dasanayake, R.; Balendran, T.; Atapattu, D.; Iddawela, D. A study on canine dirofilariasis in selected areas of Sri Lanka. BMC Res. Notes 2022, 15, 137. [Google Scholar] [CrossRef]
- Kramer, L.H.; Kartashev, V.V.; Grandi, G.; Morchón, R.; Nagornii, S.A.; Karanis, P.; Simón, F. Human subcutaneous dirofilariasis, Russia. Emerg. Infect. Dis. 2007, 13, 150–152. [Google Scholar] [CrossRef]
- Poppert, S.; Hodapp, M.; Krueger, A.; Hegasy, G.; Niesen, W.D.; Kern, W.V.; Tannich, E. Dirofilaria repens infection and concomitant meningoencephalitis. Emerg. Infect. Dis. 2009, 15, 1844–1846. [Google Scholar] [CrossRef]
- Simón, F.; Siles-Lucas, M.; Morchón, R.; González-Miguel, J.; Mellado, I.; Carretón, E.; Montoya-Alonso, J.A. Human and animal dirofilariasis: The emergence of a zoonotic mosaic. Clin. Microbiol. Rev. 2012, 25, 507–544. [Google Scholar] [CrossRef]
- Rossi, A.; Peix, Á.; Pavlikovskaya, T.; Sagach, O.; Nikolaenko, S.; Chizh, N.; Kartashev, V.; Simón, F.; Siles-Lucas, M. Genetic diversity of Dirofilaria spp. isolated from subcutaneous and ocular lesions of human patients in Ukraine. Acta Trop. 2015, 142, 1–4. [Google Scholar] [CrossRef]
- Genchi, C.; Solari Bansano, F.; Bandi, C.; Di Sacco, B.; Venco, L.; Vezzoni, A.; Cancrini, G. Interaction between Dirofilaria immitis and Dirofilaria repens; American Heartworm Society: Holly Springs, NC, USA, 1995; pp. 65–71. [Google Scholar]
- Salas-Benito, J.S.; De Nova-Ocampo, M. Viral interference and persistence in mosquito-borne flaviviruses. J. Immunol. Res. 2015, 2015, 873404. [Google Scholar] [CrossRef]
- Kalogeropoulos, C.D.; Stefaniotou, M.I.; Gorgoli, K.E.; Papadopoulou, C.V.; Pappa, C.N.; Paschidis, C.A. Ocular dirofilariasis: A case series of 8 patients. Middle East Afr. J. Ophthalmol. 2014, 21, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Moorhouse, D.E. Dirofilaria immitis: A cause of human intra-ocular infection. Infection 1978, 6, 192–193. [Google Scholar] [CrossRef] [PubMed]
- Theis, J.H.; Gilson, A.; Simon, G.E.; Bradshaw, B.; Clark, D. Case report: Unusual location of Dirofilaria immitis in a 28-year-old man necessitates orchiectomy. Am. J. Trop. Med. Hyg. 2001, 64, 317–322. [Google Scholar] [CrossRef] [PubMed]
- Tada, I.; Sakaguchi, Y.; Eto, K. Dirofilaria in the abdominal cavity of a man in Japan. Am. J. Trop. Med. Hyg. 1979, 28, 988–990. [Google Scholar] [CrossRef]
- Kim, M.K.; Kim, C.H.; Yeom, B.W.; Park, S.H.; Choi, S.Y.; Choi, J.S. The first human case of hepatic dirofilariasis. J. Korean Med. Sci. 2002, 17, 686–690. [Google Scholar] [CrossRef]
- Gowrishankar, S.; Aravind, M.; Sastya, S.; Latha, B.R.; Azhahianambi, P.; Vairamuthu, S.; Jayanthy, C. Dirofilaria hongkongensis—A first report of potential zoonotic dirofilariosis infection in dogs from Tamil Nadu. Vet. Parasitol. Reg. Stud. Rep. 2019, 18, 100326. [Google Scholar] [CrossRef]
Figure 1.
Life cycles of D. immitis and D. repens.

Figure 2.
PRISMA flow diagram of the study selection process.

Figure 3.
Forest plot of the pooled estimated prevalence of D. repens and D. immitis. The central square represents point estimates, whereas the square size represents the weight of each study in the meta-analysis. Diamonds represent the overall or summary effect for the respective category. Immitis = D. immitis; Repens = D. repens [45,51,52,53,54,55,56,57,58,59,60,61,62].
Figure 3.
Forest plot of the pooled estimated prevalence of D. repens and D. immitis. The central square represents point estimates, whereas the square size represents the weight of each study in the meta-analysis. Diamonds represent the overall or summary effect for the respective category. Immitis = D. immitis; Repens = D. repens [45,51,52,53,54,55,56,57,58,59,60,61,62].

Figure 4.
Forest plot of the pooled estimated prevalence of D. repens and D. immitis in India and Sri Lanka. The central square represents point estimates, whereas the square size represents the weight of each study in the meta-analysis. Diamonds represent the overall or summary effect for the respective category [45,51,52,53,54,55,56,57,58,59,60,61,62].
Figure 4.
Forest plot of the pooled estimated prevalence of D. repens and D. immitis in India and Sri Lanka. The central square represents point estimates, whereas the square size represents the weight of each study in the meta-analysis. Diamonds represent the overall or summary effect for the respective category [45,51,52,53,54,55,56,57,58,59,60,61,62].

Figure 5.
Forest plot of the pooled estimated prevalence of D. repens and D. immitis identified using different diagnostic techniques. The central square represents point estimates, whereas the square size represents the weight of each study in the meta-analysis. Diamonds represent the overall or summary effect for the respective category [45,51,52,53,54,55,56,57,58,59,60,61,62].
Figure 5.
Forest plot of the pooled estimated prevalence of D. repens and D. immitis identified using different diagnostic techniques. The central square represents point estimates, whereas the square size represents the weight of each study in the meta-analysis. Diamonds represent the overall or summary effect for the respective category [45,51,52,53,54,55,56,57,58,59,60,61,62].

Figure 6.
Forest plot of the pooled estimated prevalence of D. repens and D. immitis identified in different dog types. The central square represents point estimates, whereas the square size represents the weight of each study in the meta-analysis. Diamonds represent the overall or summary effect for the respective category [45,51,52,53,54,55,56,57,58,59,60,61,62].
Figure 6.
Forest plot of the pooled estimated prevalence of D. repens and D. immitis identified in different dog types. The central square represents point estimates, whereas the square size represents the weight of each study in the meta-analysis. Diamonds represent the overall or summary effect for the respective category [45,51,52,53,54,55,56,57,58,59,60,61,62].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Predilection sites of selected Dirofilaria spp. mainly found in India and Sri Lanka.
| Parasite | Subgenus | Definitive/Incidental Host | Primary Site of Infection | Zoonosis | Distribution |
|---|---|---|---|---|---|
| D. immitis | Dirofilaria | Canid, felid, humans 1 | Cardiovascular, Pulmonary | Yes | Americas, Europe, Indochina, Asia, Australia |
| D. repens | Nochtiella | Canid, felid, humans 1 | Subcutaneous, subconjunctival, intermuscular tissues | Yes | Eurasia, Africa |
| D. indica | Dirofilaria | Dog | Heart | No | India |
| D. linstowi | Nochtiella | Primates | Subcutaneous tissues | No | Sri Lanka |
| D. macae | Nochtiella | Primates | Subcutaneous tissues | No | Indochina |
| D. pagumae | Nochtiella | Viverrid | Subcutaneous tissues | No | Indochina |
| D. hongkongnesis | Nochtiella | Canids, humans | Subcutaneous tissues | Yes | India, Hong Kong |
1 Many definitive/incidental hosts (list not exhaustive), including wildlife.
Table 2.
Prevalence (last reported) summary of D. immitis and D. repens in various countries.
| Countries | Regions/Areas Reported | Continent | Eco-Climatic Zone 1 | Parasites | Last Reported Prevalence 2 | Reference |
|---|---|---|---|---|---|---|
| Mediterranean countries | Canary Islands | Europe | Dry | D. immitis | 22–40% | [37] |
| Romania | Southern | Europe | Dry/Humid temperate | D. immitis | 5% | [38] |
| D. repens | 12% | |||||
| Slovakia | Trnava region | Central Europe | Humid temperate | D. immitis | 64% | [39] |
| Bulgaria | N.A. | Central Europe | Humid temperate | D. immitis | 34% | [40] |
| D. repens | 6% | |||||
| Russia | Southern and central areas | North Asia | Polar | D. immitis | 36–55% | [41,42] |
| Iran | Kerman, southeastern | South Asia | Dry | D. immitis | 5% | [43] |
| Tunisia | Northern and Central | Africa | Dry/Humid-temperate | D. immitis | 15% | [44] |
| D. repens | 3% | |||||
| India | Assam | Southeast Asia | Humid tropical | D. immitis | 30% | [34] |
| Sri Lanka | Western and North-western | Southeast Asia | Humid tropical | D. repens | 69% | [45] |
| Thailand | Bangkok metropolitan region | Southeast Asia | Humid tropical | D. immitis | 58% | [46] |
| Turkey | Sakarya, Kocaeli, Ankara, Elazig, and Mersin provinces | Western Asia | Dry/Humid-temperate | D. immitis | 0–18% | [47] |
N.A. = Not applicable. 1 Four ecoclimatic zones of the earth [48]. 2 Methodologies to determine prevalence of various parasites were different in different studies.
Table 3.
Geographical distribution of dog data.
| Countries | State/Province 1 | % (95%CI) | References |
|---|---|---|---|
| India (n = 454) | Kerala (n = 160) | 35.24 (30.85–39.83) | [51,52,53] |
| Assam (n = 157) | 34.58 (30.21–39.16) | [54,55,56,57] | |
| Mizoram (n = 54) | 11.89 (9.06–15.23) | [57,58] | |
| Maharashtra (n = 40) | 8.81 (6.37–11.80) | [59] | |
| Tamil Nadu (n = 17) | 3.74 (2.20–5.93) | [60] | |
| Delhi (n = 15) | 3.30 (1.86–5.39) | [59] | |
| Goa (n = 10) | 2.20 (1.06–4.01) | [61] | |
| Sikkim (n = 1) | 0.22 (0.01–1.22) | [59] | |
| Sri Lanka (n = 163) | Western Province (n = 114) | 69.93 (62.27–76.86) | [45,62] |
| Northwestern Province (n = 49) | 30.06 (23.13–37.72) | [45] |
1 State for India; Provinces for Sri Lanka.
Table 4.
Geographical distribution of human data.
| Countries | State/Province 1 | % (95%CI) | References |
|---|---|---|---|
| India (n = 92) | Kerala (n = 51) | 55.43 (44.70–65.81) | [11,12,13,14,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78] |
| Karnataka (n = 18) | 19.57 (12.03–29.15) | [79,80,81,82,83,84,85,86,87,88,89,90,91] | |
| Maharashtra (n = 9) | 9.78 (4.57–17.76) | [92,93,94,95,96,97,98] | |
| Assam (n = 7) | 7.61 (3.11–15.05) | [32,99,100] | |
| Thamil Nadu (n = 3) | 3.26 (0.68–9.23) | [101,102] | |
| Bihar (n = 1) | 1.09 (0.03–5.91) | [103] | |
| Delhi (n = 1) | 1.09 (0.03–5.91) | [104] | |
| Goa (n = 1) | 1.09 (0.03–5.91) | [105] | |
| Orissa (n = 1) | 1.09 (0.03–5.91) | [82] | |
| Sri Lanka (n = 138) | Central Province (n = 63) | 45.65 (37.15–54.34) | [9,106,107,108,109,110] |
| Western Province (n = 32) | 23.18 (16.43–31.12) | [9,110,111,112,113,114,115] | |
| Uva Province (n = 26) | 18.84 (12.69–26.37) | [116] | |
| Southern Province (n = 10) | 7.24 (3.52–12.92) | [9] | |
| Sabaragamuwa Province (n = 3) | 2.17 (0.45–6.22) | [9] | |
| Northwestern Province (n = 2) | 1.44 (0.17–5.13) | [9] | |
| Eastern Province (n = 1) | 0.72 (0.01–3.97) | [9] | |
| North Province (n = 1) | 0.72 (0.01–3.97) | [9] |
1 State for India; Provinces for Sri Lanka
Table 5.
Descriptive summary of human data on dirofilariasis in India and Sri Lanka.
| Variables | Characteristics | % (95%CI) |
|---|---|---|
| Sex (n = 230) | Male (n = 88) | 38.26 (31.95–44.87) |
| Female (n = 74) | 32.17 (26.18–38.63) | |
| N.A. (n = 68) | 29.56 (23.74–35.91) | |
| Diagnostic technique (n = 396) | Surgical excision (n = 182) | 45.95 (40.97–51.00) |
| Histopathological examination (n = 76) | 19.19 (15.42–23.42) | |
| Microscopy (n = 59) | 14.89 (11.53–18.79) | |
| Ultrasound (n = 38) | 9.59 (6.88–12.93) | |
| Ophthalmic examination (n = 18) | 4.54 (2.71–7.08) | |
| PCR (n = 11) | 2.77 (1.39–4.91) | |
| Imaging (n = 6) | 1.51 (0.55–3.26) | |
| FNA (n = 3) | 0.75 (0.15–2.19) | |
| Self-emerged (n = 3) | 0.75 (0.15–2.19) | |
| Parasite species (n = 230) | D. repens (n = 224) | 97.39 (94.41–99.04) |
| D. immitis (n = 5) | 2.17 (0.71–4.99) | |
| Dirofilaria spp. (n = 1) | 0.43 (0.01–2.39) | |
| Body system (n = 260) | Eye (n = 98) | 30.05 (31.77–43.88) |
| Repro (n = 23) | 8.84 (5.69–12.97) | |
| Oral (n = 20) | 7.69 (4.76–11.63) | |
| Hand (n = 18) | 6.92 (4.15–10.72) | |
| Chest/Breast (n = 14) | 5.38 (2.97–8.86) | |
| Abdomen (n = 13) | 5.00 (2.68–8.39) | |
| Cheek/Face (n = 11) | 4.23 (2.13–7.44) | |
| Neck (n = 11) | 4.23 (2.13–7.44) | |
| Leg (n = 9) | 3.46 (1.59–6.46) | |
| Head (n = 4) | 1.53 (0.04–3.89) | |
| Respiratory (n = 2) | 0.07 (0.09–2.75) | |
| Buttock (n = 1) | 0.03 (0.09–2.12) | |
| Cardiovascular (n = 1) | 0.03 (0.09–2.12) | |
| Digestive (n = 1) | 0.03 (0.09–2.12) | |
| N.A. (n = 34) | 13.07 (9.22–17.79) | |
| Parasite life stage (n = 230) | Female (n = 39) | 16.95 (12.34–22.44) |
| Female adult (n = 14) | 6.08 (3.36–10.00) | |
| Female immature (n = 10) | 4.34 (2.10–7.85) | |
| Dead (n = 10) | 4.34 (2.10–7.85) | |
| Male (n = 8) | 3.47 (1.51–6.73) | |
| Live (n = 4) | 1.73 (0.47–4.39) | |
| Degenerated (n = 3) | 1.30 (0.26–3.76) | |
| Female gravid (n = 2) | 0.86 (0.11–3.11) | |
| Female gravid with microfilaria (n = 1) | 0.43 (0.01–2.39) | |
| Female dead (n = 1) | 0.43 (0.01–2.39) | |
| Infertile (n = 1) | 0.43 (0.01–2.39) | |
| Male adult (n = 1) | 0.43 (0.01–2.39) | |
| Male immature (n = 1) | 0.43 (0.01–2.39) | |
| Mature adult (n = 1) | 0.43 (0.01–2.39) | |
| Microfilaria (n = 1) | 0.43 (0.01–2.39) | |
| Worm fragmented (n = 1) | 0.43 (0.01–2.39) | |
| N.A. (n = 132) | 57.39 (50.72–63.86) |
N.A. = Not applicable.
Table 6.
The overall prevalence of D. immitis and D. repens is categorized by country.
| India Prevalence (95% CI; Positive/Total) | Sri Lanka Prevalence (95% CI; Positive/Total) | |
|---|---|---|
| D. immitis | 9.7% (8.5–11.0%; 225/2318) | Nil |
| D. repens | 8.1% (7.2–9.2%; 229/2814) | 51.7% (46.1–57.4%; 163/315) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Thilakarathne, S.S.; Yuen, N.K.Y.; Hassan, M.M.; Yahathugoda, T.C.; Abdullah, S. Animal and Human Dirofilariasis in India and Sri Lanka: A Systematic Review and Meta-Analysis. Animals 2023, 13, 1551. https://doi.org/10.3390/ani13091551
AMA Style
Thilakarathne SS, Yuen NKY, Hassan MM, Yahathugoda TC, Abdullah S. Animal and Human Dirofilariasis in India and Sri Lanka: A Systematic Review and Meta-Analysis. Animals. 2023; 13(9):1551. https://doi.org/10.3390/ani13091551
Chicago/Turabian StyleThilakarathne, Sandani S., Nicholas K. Y. Yuen, Mohammad Mahmudul Hassan, Thishan C. Yahathugoda, and Swaid Abdullah. 2023. "Animal and Human Dirofilariasis in India and Sri Lanka: A Systematic Review and Meta-Analysis" Animals 13, no. 9: 1551. https://doi.org/10.3390/ani13091551
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.