School Scoliosis Screening: The Influence of Dominant Limbs and Gender



1
Human Performance Laboratory, Department of Life & Health Sciences, University of Nicosia, 46 Makedonitissas Ave., P.O. Box 24005, Nicosia 1700, Cyprus
2
School of Sciences, University of Central Lancashire, Pyla 7080, Cyprus
*
Author to whom correspondence should be addressed.
Adolescents 2024, 4(1), 62-74; https://doi.org/10.3390/adolescents4010005
Submission received: 27 November 2023
/
Revised: 19 January 2024
/
Accepted: 22 January 2024
/
Published: 24 January 2024
(This article belongs to the Section Adolescent Health and Mental Health)
Abstract
:This study aimed to examine whether (a) there is an association of the dominant hand (DH) and leg (DL) with the side of the primary angle of trunk rotation (ATR A) and (b) there are any differences between boys and girls in the degree of the angle of trunk rotation (ATR) and the dominant hand and leg. One thousand sixty-five (age: 14 ± 3 years; height: 162 ± 13 cm; weight: 56 ± 18.7 kg; BMI: 21.18 ± 5.07) secondary school children participated in this study. Of the participants, 52.5% (n = 559) were male students (age: 14 ± 2 years; height: 166 ± 16 cm; weight: 58.7 ± 22.6 kg; BMI: 21.41 ± 5.61), and 47.5% (n = 506) were female students (age: 14 ± 3 years; height: 159.5 ± 8.5 cm; weight: 53.9 ± 14.8 kg; BMI: 21.03 ± 4.38). The ATR was measured with a scoliometer. Boys were taller and heavier (p = 0.001) and had more left DLs (p = 0.039) than girls. Girls were biologically more mature (p = 0.002), also having higher measurements for the ATR A (p = 0.004) and secondary angle of trunk rotation (ATR B) (p = 0.023) degrees compared to boys. In the general sample, only in boys, there was a significant association between the DH (p = 0.012) and DL (p = 0.001) with the ATR A side. Also, within the scoliotic group, only in boys, there was a significant association between the DH (p = 0.048) and DL (p = 0.024) with the ATR A. In conclusion, girls had higher measurements for the ATR than boys, but cross laterality was found only in boys. The results suggest different progression patterns of ATR between genders during their growth. Future research should focus on examining other possible progression mechanisms.
1. Introduction
School scoliosis screening (SSS) is considered a powerful tool that aims to identify individuals with unrecognized adolescence idiopathic scoliosis (AIS) at an early stage [1]. AIS is a structural scoliosis, and it has been defined as a three-dimensional spine deformity characterized by a lateral curvature of more than 10 degrees as measured on X-rays (Cobb’s angle) [2,3] and rotation movement of the vertebrae [4]. On the other hand, functional scoliosis is characterized by the disturbance of spinal balance in orthostatism but without any anatomical deterioration of the vertebrae or intervertebral discs [4].
The etiology of functional scoliosis has been related to factors such as length differences in the lower extremities, hip dysplasia, contracture of unilateral paravertebral muscle, herniated discs, torticollis and asymmetry of the upper extremities [3,4,5,6,7]. Functional scoliosis may also further cause other asymmetries with its onset, such as abnormal postural habits, altered biomechanics, muscular imbalances, joint laxity and excessive strain on the spine’s joints, muscles, tendons and bones [8,9,10].
Laterality in children and adolescents has also been also examined to indicate a significant association of scoliosis-related attributes (curve pattern and convexity) with the direction of hand preference, the strength of the asymmetry direction or side preference consistency [11,12,13,14,15]. Yang and Li (2011) developed a theory with a three-dimensional spring model and a hypothesis for the mechanism of left–right handedness. The spine tends to flex laterally and rotate around its axis, and spine curvature coexists. The direction of this tendency is determined by the location and gravity of the heart and aorta, which could be the reason for the right convexity in AIS [16]. As a result of this tendency, most dominant right-handed people usually present curves with right convexity. It is also assumed that dominant left-handed people do not have the same tendency and that the pattern of their curve is random [16]. It was demonstrated that spine rotational patterns exist in normal, non-scoliotic human spines [17,18]. Therefore, it has been hypothesized that the onset of spinal rotation reasonably goes along with the pre-existing rotational pattern in a normal spine [17,18]. Schlösser et al. (2017) validated these theories in patients with scoliosis and situs inversus totalis and demonstrated a 94% match between organ orientation and curve convexity [19].
Several studies have examined the different parameters that may influence laterality, such as handedness, footedness, earedness and eyedness. However, studies conducted to examine the laterality of trunk asymmetry and side dominance have focused on diagnosed adolescents with AIS and on region prevalence in the spine rather than the side of the spine [11,12,13,14,15,20,21]. Arienti et al. (2019) [14] found that right-side dominance is associated with a low prevalence, whereas left dominance is associated with a high prevalence for right thoracic, right thoracolumbar and left lumbar curves [14].
There is a need for further research on the association of leg and hand dominance with the side of functional scoliosis particularly. The aims, therefore, of the present study were (a) to examine whether there is an association of the dominant hand and/or leg with the side of the primary angle of trunk rotation (ATR) in boys and girls and (b) to observe whether there are any differences between boys and girls in the dominant hand and leg and in the degrees of the ATR. It was hypothesized that there is indeed an association between the dominant hand/leg with the side of the primary ATR and that there is a different progression pattern of ATR between boys and girls during their puberty stages.
2. Materials and Methods
2.1. Participants
The participants of this study were one thousand sixty-five (n = 1065) students derived from secondary schools (age: 14 ± 3 years; height: 162 ± 13 cm; weight: 56 ± 18.7 kg; BMI: 21.18 ± 5.07). Of the participants, 52.5% (n = 559) were male students (age: 14 ± 2 years; height: 166 ± 16 cm; weight: 58.7 ± 22.6 kg; BMI: 21.41 ± 5.61), and 47.5% (n = 506) were female students (age: 14 ± 3 years; height: 159.5 ± 8.5 cm; weight: 53.9 ± 14.8 kg; BMI: 21.03 ± 4.38). All students were initially screened in school settings. All participants voluntarily participated in the study after being informed of the purpose and the potential benefits of the SSS. The study was approved by the National Bioethics Committee (ΕΕΒΚ ΕΠ 2021.01.169) and conformed to the Code of Ethics of the World Medical Association (Declaration of Helsinki) [22], and it was also under the auspices of the Ministry of Health of Cyprus. Following an explanation of the SSS methods and procedures, parental written informed consent was obtained prior to the screening. No participant had any disease or musculoskeletal injury during the study period. Nine students denied participation; therefore, none of them were forced to undertake the test.
2.2. Experimental Design
Initially, mail was sent to every private school principal in Nicosia County, including an information letter and a participation form. The targeted sample was estimated to be approximately three thousand students of the above-mentioned ages. Only seven out of the fourteen private schools agreed to participate. One thousand five hundred thirty-three envelopes were sent to parents, including the recruitment material (see below). Instructions were given to each school to voluntarily sign and return the forms either via mail or email. The information letter included the aims of the study and the potential benefits of the program. The researchers requested from the director of each school to return the signed participation form for the school and provide the following information for organizational purposes: the name of the principal and school and the number of students between the ages of 11 to 16 years old enrolled for the academic year. The targeted ages were 11 to 16 years old, as per the national SSS program of the Ministry of Health of Cyprus. All recruitment materials were prepared, and physical education teachers distributed them to the students’ parents. The recruitment materials sent to the parents were enclosed in envelopes, which included a (a) cover page, (b) parent/guardian/information letter, (c) scoliosis article, (d) parent/guardian consent form (two copies) and (e) withdrawal form (two copies). The scoliosis screening took place during physical education classes. The students of each class gathered in nursery rooms or indoor sports courts.
2.3. Anthropometrics and Biological Evaluations
The date of birth, gender, height, weight, initiation of the menstrual cycle (for girls’ maturity) and hair growth in the genital region (for boys’ maturity) were recorded. Maturity data were collected based on the answers of a questionnaire sent to parents regarding their children’s biological maturation, which, for girls, was the onset of their menstrual cycle, and for boys, was pubic hair growth [23].
2.4. Angle of Trunk Rotation Evaluation (Thoracic, Thoracolumbar and Lumbar)
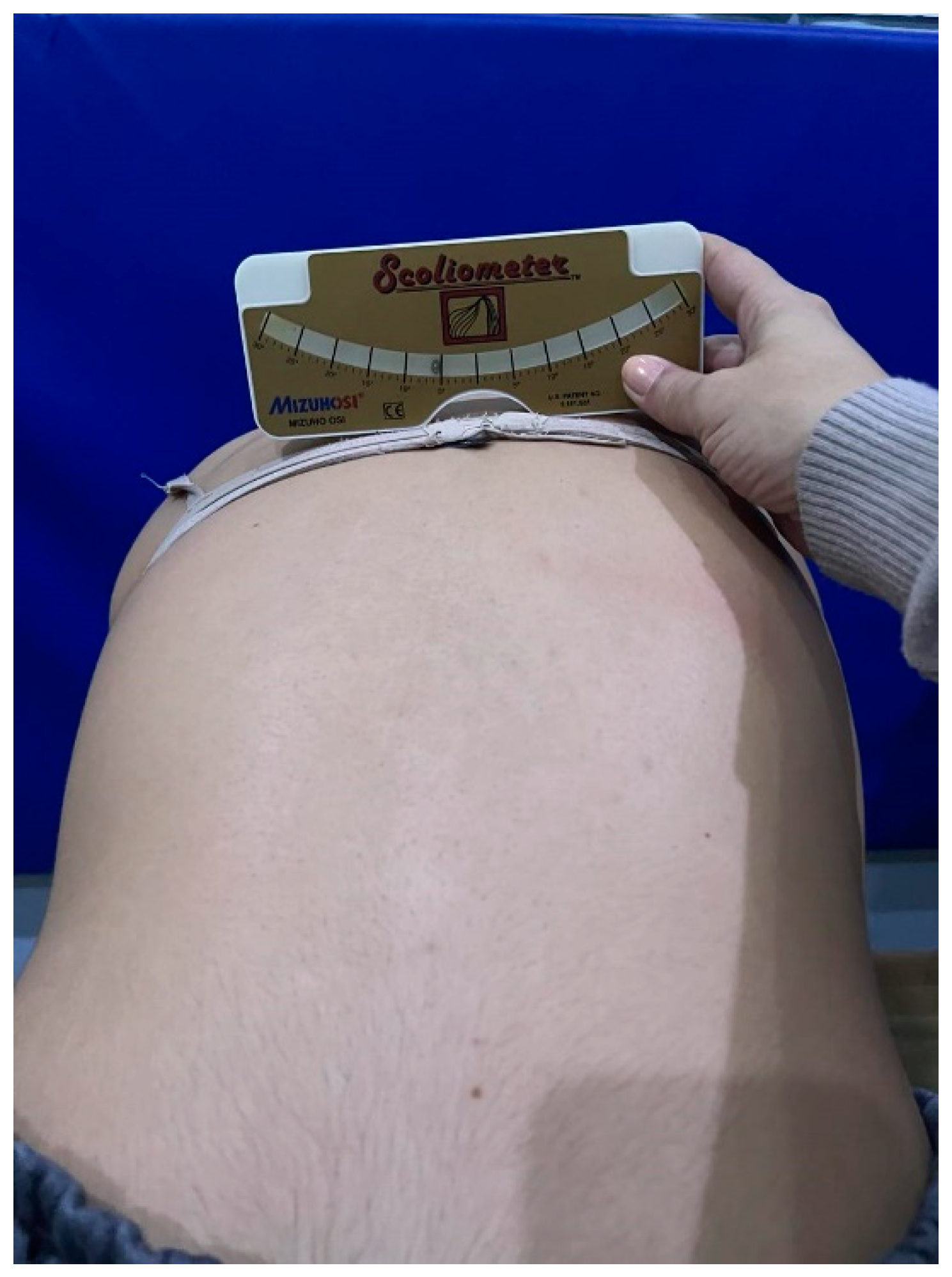
The angle of trunk rotation (ATR) was measured with a scoliometer (Mizuho Osi®, Mizuho OSI Inc., Tokyo, Japan). Initially, the participant performed Adam’s forward bend test with extended arms touching his/her knees for thoracic and thoracolumbar measurements and with his/her feet together. Afterward, the participant bent forward with extended arms pointing down for the lumbar measurements and with his/her feet together. During Adam’s forward bend test, it was observed whether there was an asymmetry at any level of the spine, and then the scoliometer was placed at that level to obtain the measurement (Figure 1 and Figure 2). The scoliometer measurement, the spine’s level and the convexity’s side of the ATR were recorded [24]. A scoliometer was chosen due to its high specificity and sensitivity. Additionally, it was chosen due to its predictive capability since it is correlated with radiographic analysis (r = 0.7 with p < 0.05) [25]. The reliability of the scoliometer was determined with a two-way random-effect intraclass correlation coefficient (ICC) with 95% confident intervals (CI) (Table 1). Two groups of ATR were created, where the primary angle of trunk rotation (ATR A) was recorded as the one with higher degrees and where the secondary angle of trunk rotation (ATR B) was the one with lower degrees. With respect to degrees, the scoliotic group was named for participants who recorded ≥6°.
2.5. Laterality
Laterality is defined as the advantage of one side of the body with respect to usability, precision and coordination [26]. Laterality progressively develops with age and is established around the age of 7 years old [26,27]. Each student reported his/her dominant hand as the one used for writing and the dominant leg as the one used to kick a ball [14].
2.6. Statistical Analysis
Following the normality of distribution test (Kolmogorov–Smirnov), all data were expressed as the median and interquartile range (IQR). Since the data violated the assumptions for parametric analysis (i.e., equality of variance and normality of distribution), a non-parametric examination was carried out. Chi-squared (χ2) was used to determine whether the variables that were measured were associated in whole groups of students and in boys and girls separately. The Mann–Whitney U test for unpaired evaluations was used to examine the differences between boys and girls. The effect sizes (ESs) for each group were estimated according to the Rosenthal (1991) equation (r = Z/√Ν) [28]. Cramer’s V value was also requested to identify the strength and the effect size of the association of the tested variables. The ESs were interpreted according to Cohen’s criteria. A Cramer’s V value equal to 0.1 is considered a small effect size, 0.3 represents a medium effect size, and 0.5 represents a large effect size [29]. Statistical significance was declared at p < 0.05. All statistical analyses were performed using SPSS software (version 28 for Windows; IBM SPSS Inc., Chicago, IL, USA).
3. Results
The reliability was determined with a two-way random-effect intraclass correlation coefficient (ICC) with 95% confidence intervals (CI) for the scoliometer. The result was ICC = 0.988 (CI = 0.981–0.993; p = 0.001).
3.1. Differences between Boys and Girls
Table 2 presents the results of the Mann Whitney U test, which revealed the differences between the boys and girls. Boys were taller and heavier when compared to girls (U = 91,733, Z = −9.915, p = 0.001, r = −0.30 and U = 112,689, Z = −5.733, p = 0.001 r = −0.18, respectively). Girls had higher measurements of ATR A and ATR B degrees when compared to boys (U = 127,203, Z = −2.877, p = 0.004, r = −0.09 and U = 134,940, Z = −2.276, p = 0.023, r = −0.07, respectively). Girls were more mature than boys (U = 130,029.5, Z = −3.119, p = 0.002, r = −0.1), and there were more left DLs in boys (U = 135,641.5, Z = −2.063, p = 0.039, r = −0.06).
No significant difference was found between the boys and girls for age, BMI and DH (p > 0.05).
3.2. Chi-Squared (χ2)—Boys and Girls
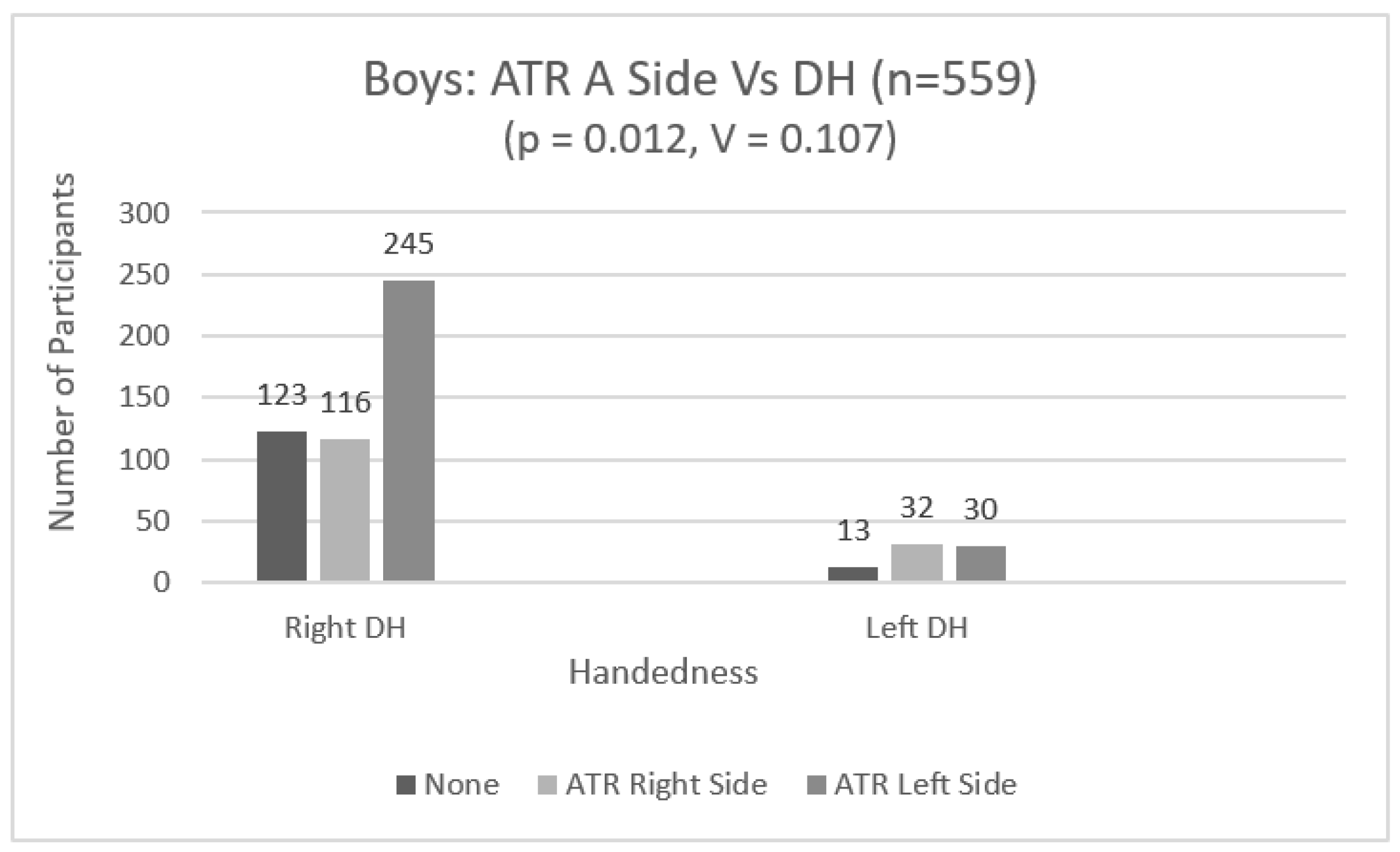
In boys, there was a significant association between the dominant hand (DH) and the ATR A side (χ2 (4) = 12.78, p = 0.012, V = 0.107) (Figure 3). The effect size, Cramer’s V, was small [29].
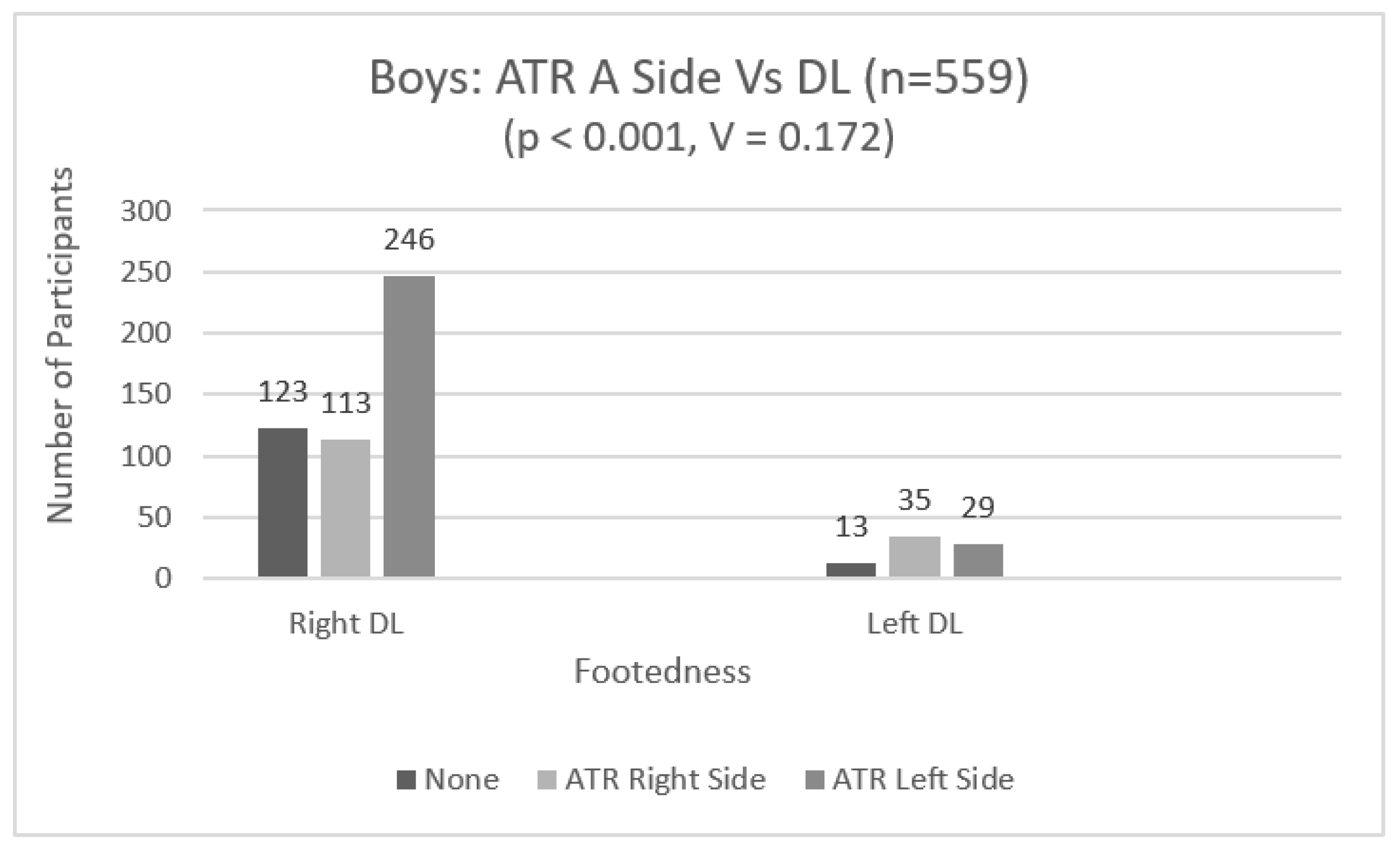
In boys, there was a significant association between the dominant leg (DL) and the ATR A side (χ2 (2) = 16.60, p < 0.001, V = 0.172) (Figure 4). The effect size, Cramer’s V, was small [29].
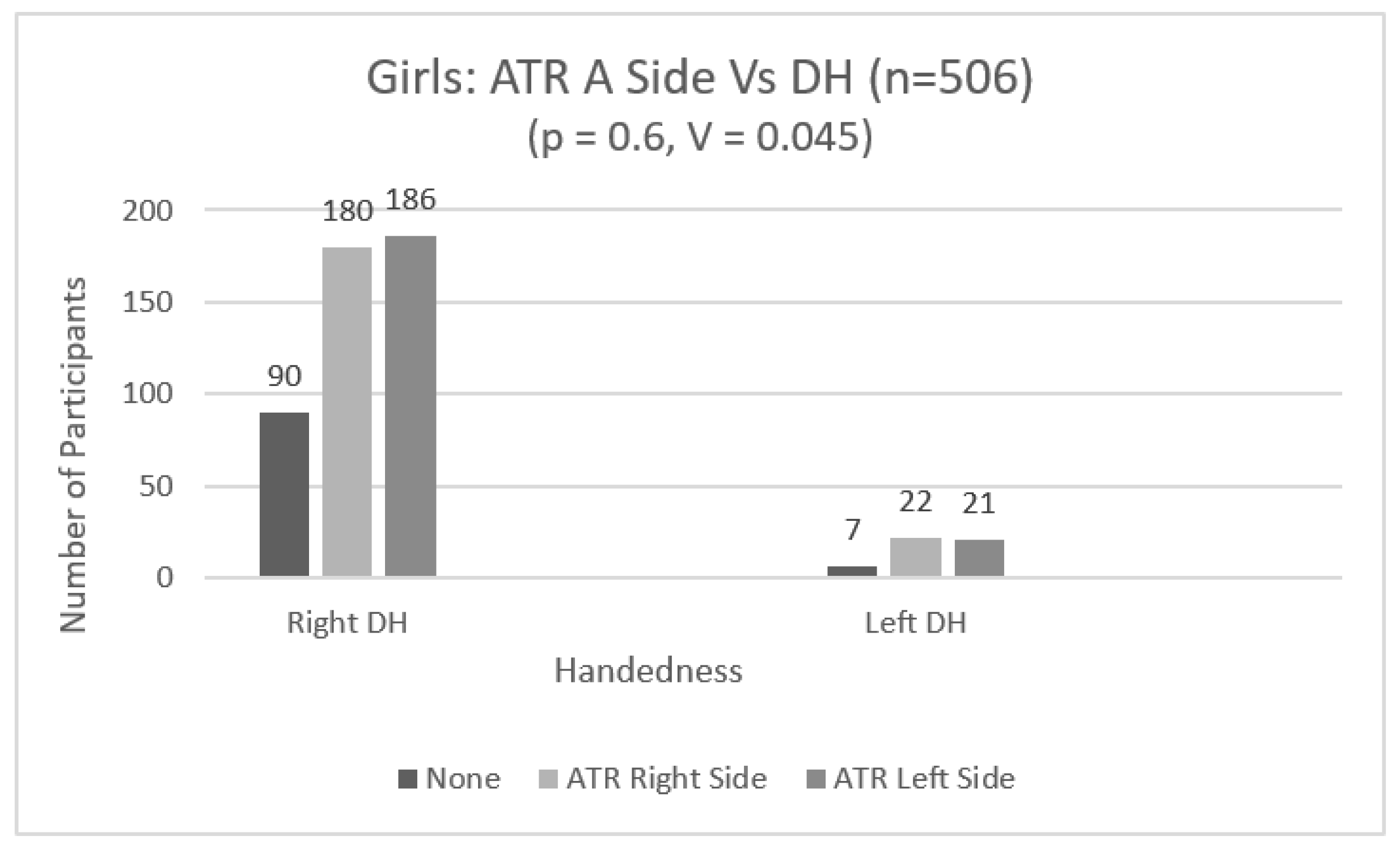
In girls, there was not a significant association between the DH and the ATR A side (χ2 (2) = 1.02, p = 0.6, V = 0.045) (Figure 5).
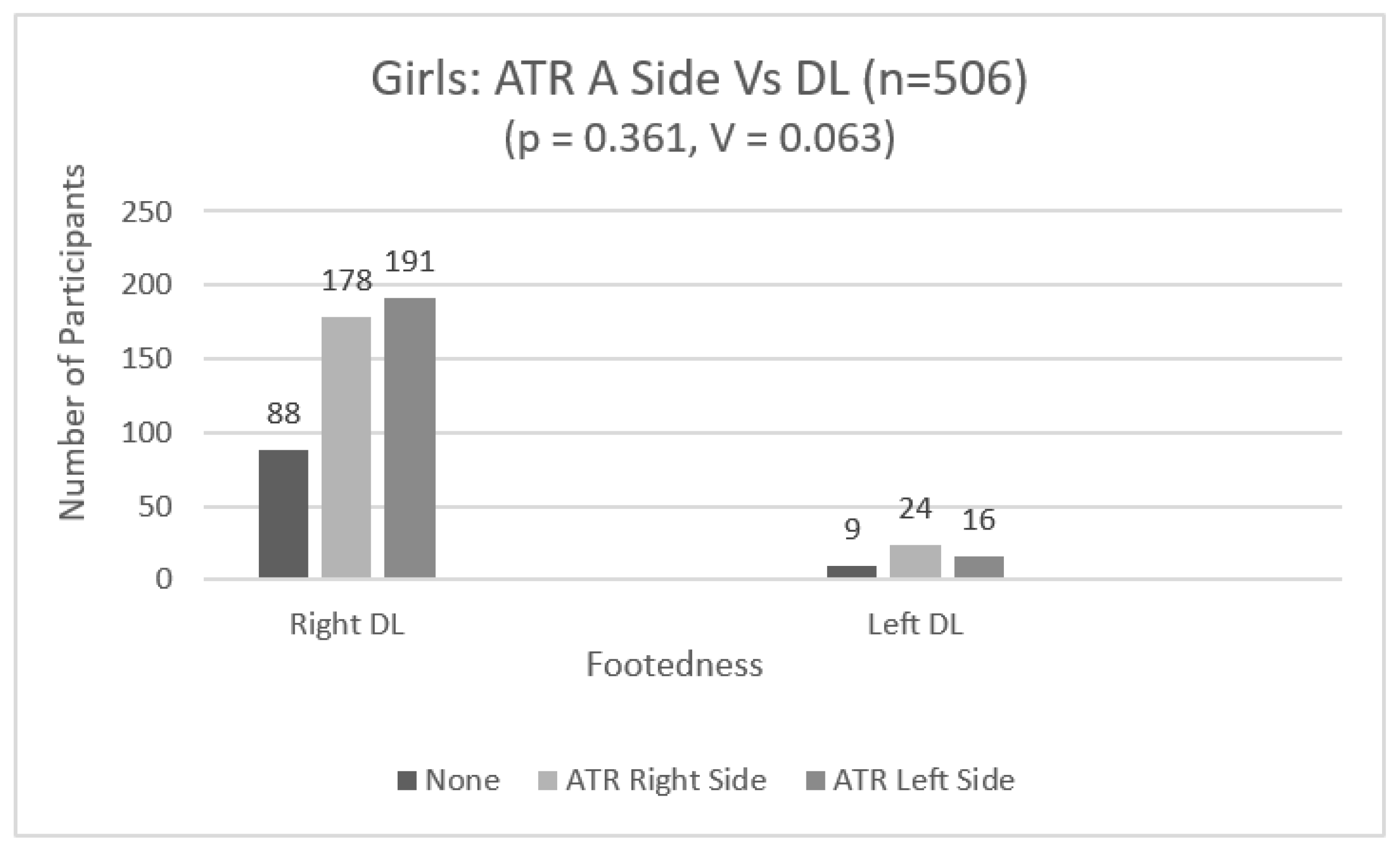
Also, in girls, there was not a significant association between the dominant leg (DL) and the ATR A side (χ2 (2) = 2.04, p = 0.361, V = 0.063) (Figure 6).
3.3. Chi-Squared (χ2)—Boys and Girls—Scoliotic Groups (≥6 Degrees)
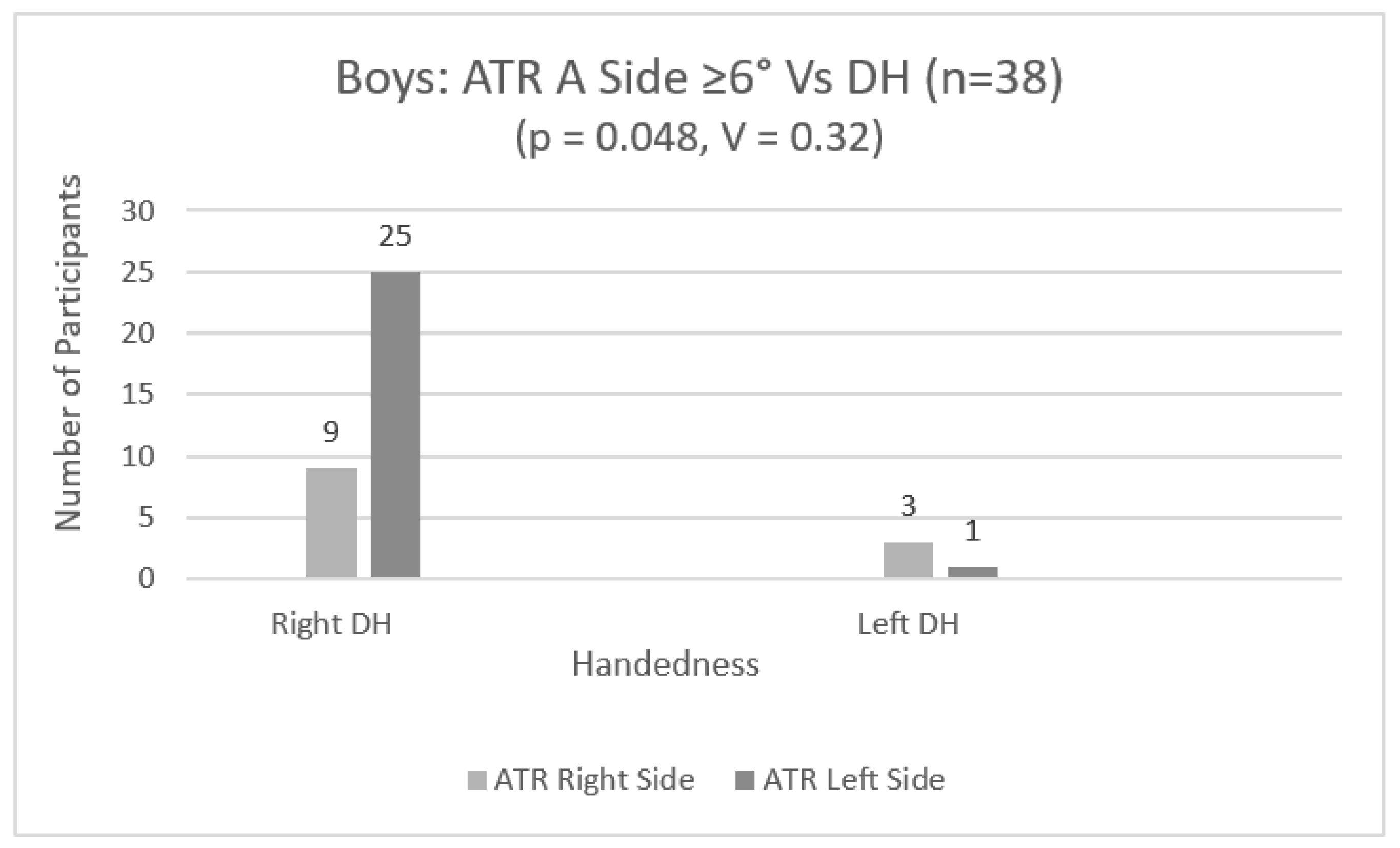
Within the scoliotic group (≥6 degrees), in boys, there was also a statistically significant association between the DH and ATR A side (χ2 (1) = 3.9, p = 0.048, V = 0.32) (Figure 7). The effect size, Cramer’s V, was medium [29].
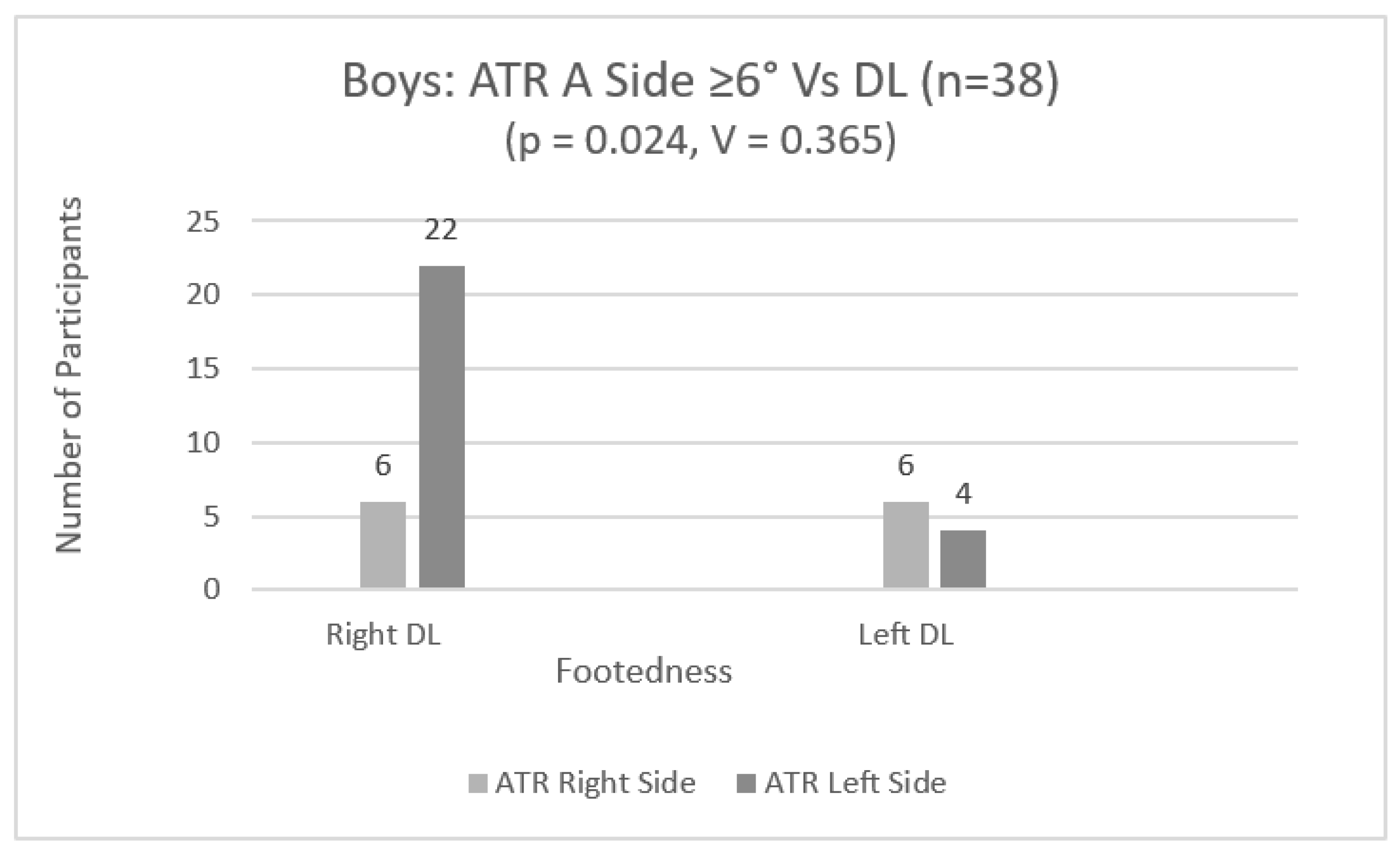
Within the scoliotic group (≥6 degrees), in boys, there were also statistically significant associations between the DL and ATR A side (χ2 (1) = 5.07, p = 0.024, V = 0.365) (Figure 8). The effect size, Cramer’s V, was medium [29].
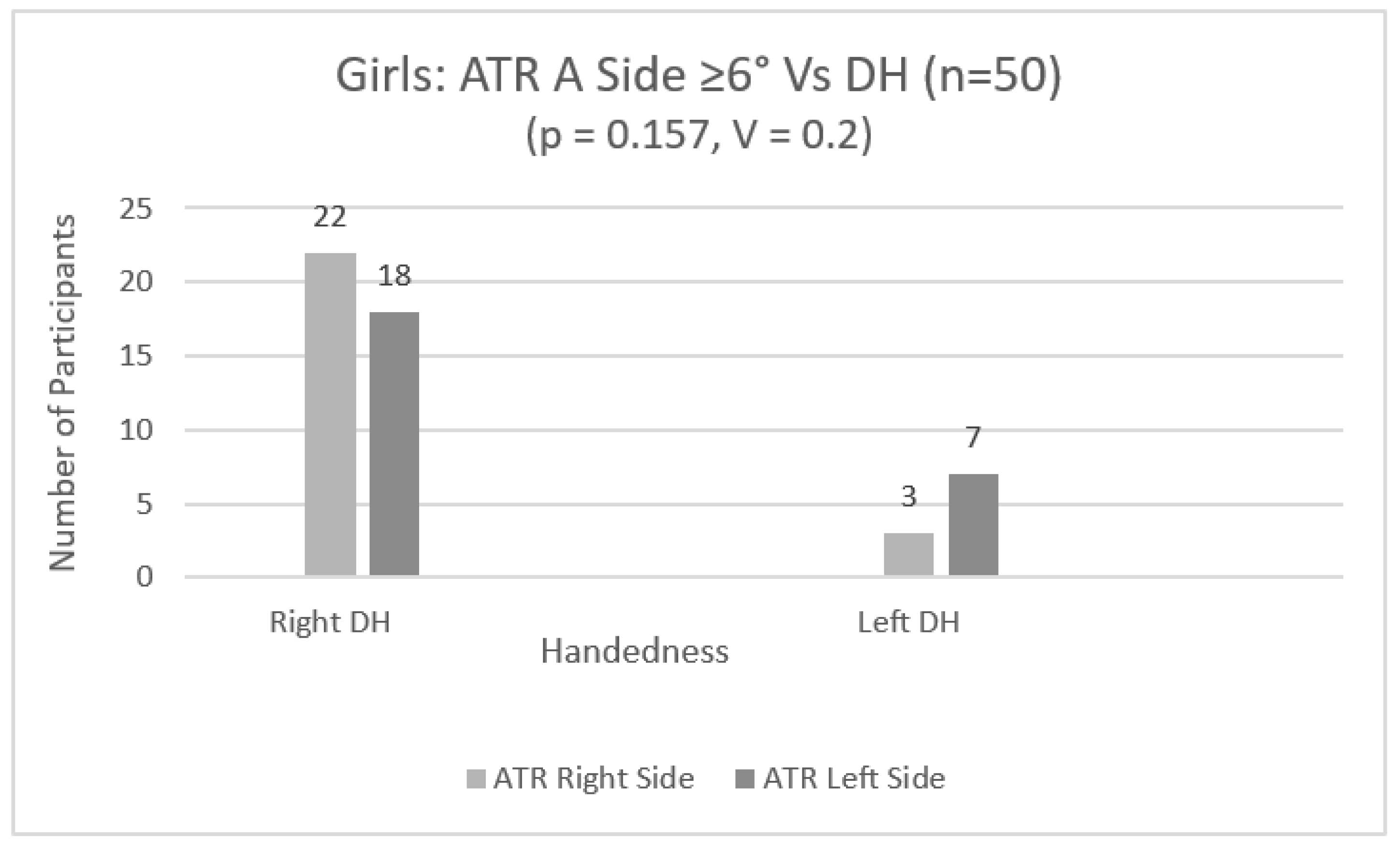
Within the scoliotic group (≥6 degrees), in girls, there was not any statistically significant association between the DH and ATR A side (χ2 (1) = 2, p = 0.157, V = 0.2) (Figure 9).
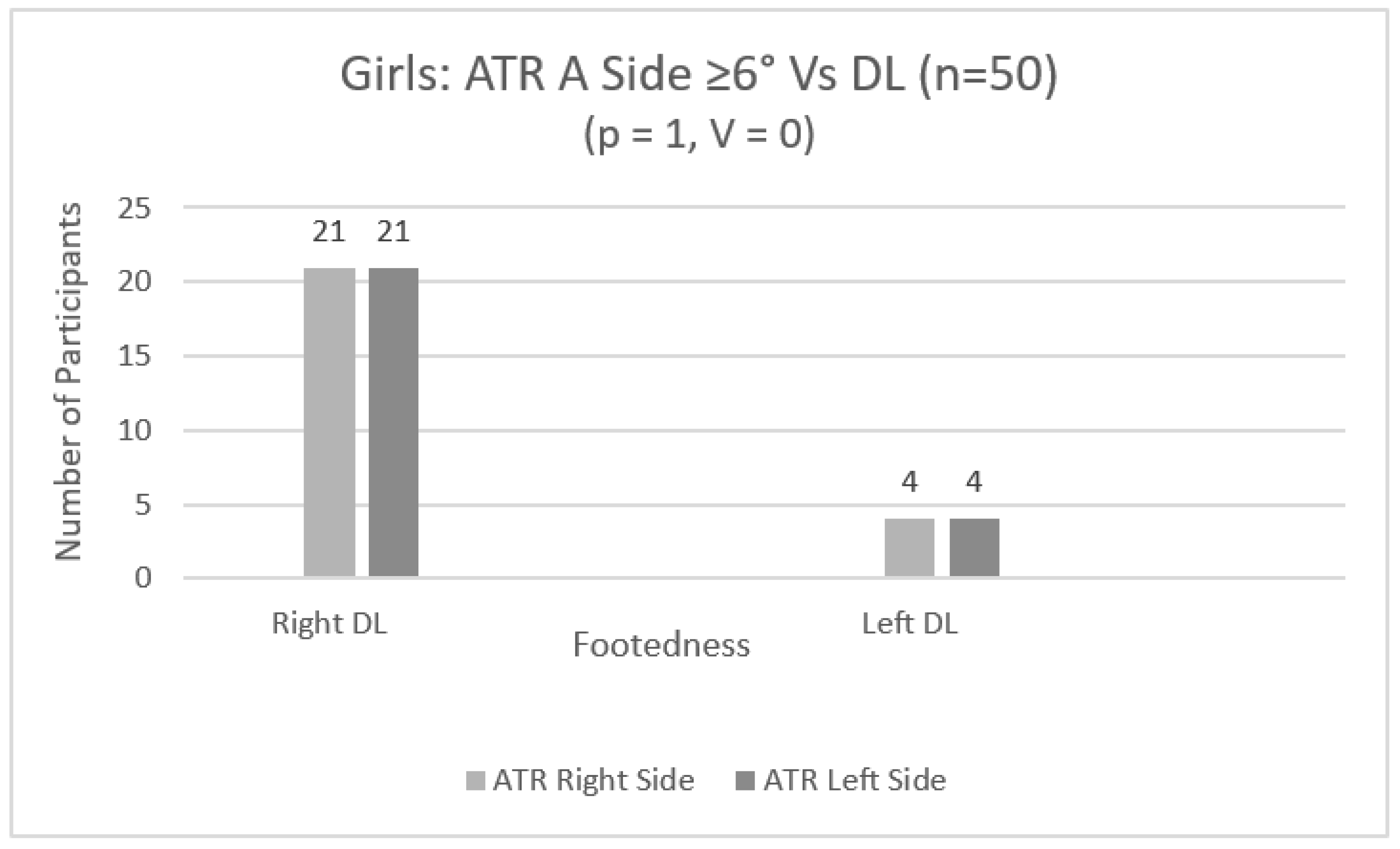
Within the scoliotic group (≥6 degrees), in girls, there was not any statistically significant association between the DL and ATR A side (χ2 (1) = 0, p = 1, V = 0) (Figure 10).
4. Discussion
The current study aimed to examine whether (a) there is an association of the dominant hand and leg with the side of the primary ATR, in boys and girls separately, and (b) there are any differences between boys and girls in the degrees of the ATR, maturity and dominant hand and leg in particular. According to the authors’ knowledge, this is the first study to examine whether there is an association of the dominant hand and/or leg with the side of the primary ATR in boys and girls. The main finding of the current study is that girls had higher measurements of ATR than those of boys, but cross laterality was found only in boys, in both the general sample and scoliotic group. These results reveal different progression patterns of ATR between boys and girls during their growth and raises the question of whether specific or perhaps different kinesiological action should be considered to eliminate ATR progression in boys and girls during their growth.
4.1. Laterality
The first aim of the current study was to examine whether there is an association between the side of ATR, handedness and footedness. Τhere were statistically significant associations between the DH and DL and the primary ATR, only in boys. Also, within the scoliotic group (≥6 degrees), the same associations were observed again only in boys. The numbers of male students of DHs and DLs were similar, and the associations with the side of the primary ATR revealed cross laterality. The right DH and DL were found to be associated with the left side of the primary ATR only in boys. The association of the left DH and DL was random in comparison to the side of ATR. Consequently, the association between these attributes is not potentially a causal effect on functional scoliosis, since scoliosis has been examined thoroughly in relation to many factors and has been characterized as multifactorial [14,30].
Most studies conducted to examine the laterality of trunk asymmetry and side dominance have focused on diagnosed adolescents with AIS and on the region that is more prevalent in the spine rather than the side of the spine [11,12,13,14,15,20,21]. However, Arienti et al. (2019) [14] found that right-side dominance was associated with a prevalence of 0.43%, 1.01% and 0.87% for right thoracic, right thoracolumbar and left lumbar curves, respectively. On the other hand, left-side dominance was associated with a prevalence of 2.72%, 2.54% and 0.65% for right thoracic, right thoracolumbar and left lumbar curves, respectively. They concluded that only the left-side dominance could be considered a predictor of trunk asymmetry in thoracic and thoracolumbar curves [14]. Similarly, in our study, there was cross laterality between the right DH and DL and the left side of the primary ATR, but only in boys.
The results of the current study do not support previous relevant studies that have observed the same laterality due to the association of pre-existing rotational patterns with body anatomy (heart and aorta) and position but not with handedness [17,18,19,30]. Our study could not make such conclusions since SSS was administered; therefore, AIS cases were not diagnosed. However, certain conclusions can be made considering that Cobb’s angle has been related to ATR due to the curve magnitude affecting Cobb’s angle [31,32]. In our sample, only boys were found to have such cross laterality. A plausible explanation for this result could be pointed out. The majority of the sample of boys practiced soccer for many years. This early participation/specialization in soccer could have contributed to developing such cross laterality in boys, only as observed in the current study. Previous studies, for example, have found that early participation in sports may cause postural malalignment in young athletes, since the development of the skeletal and muscular systems is not yet fully completed [23,33,34,35,36,37]. Early specialization may also increase the risk of developing postural asymmetries, leading progressively to acute and/or chronic injuries in both boys [34,35,37,38,39] and girls [40,41]. Furthermore, it has been suggested that, in young male and female athletes, laterality in certain sports could be related to asymmetrical bones and muscle circumference adaptations, which might also be correlated with muscle flexibility and strength [40,41,42]. However, more well-controlled studies are required to examine why cross laterality is more evident in boys than in girls.
4.2. Differences between Boys and Girls
The second aim of this study was to observe whether there are any differences between boys and girls in height, weight, BMI, degrees of the ATR, maturity and dominant hands and legs. We found that boys were taller and heavier than girls. However, girls had higher measurements of ATR A and ATR B degrees, and were more biologically mature than boys Several previous studies support these results [43,44,45,46]. Children go through two growth spurt periods: the first one occurs at a very young age during childhood, and the second one occurs with the most noticeable changes during adolescence [47]. During adolescence, postural changes occur due to hormonal effects at the beginning of puberty and musculoskeletal development. It is well documented that females grow faster and earlier than males and usually enter puberty between 8 and 14 years of age, lasting about three years [47]. Males typically enter puberty between 9.5 and 16 years of age, lasting about five years [47]. During this period, body differences become more apparent between males and females, with males mainly having a bigger skeletal size and height than females [47].
In the current study, although both sexes had no differences in chronological age, alterations were observed in biological age [47]. It is well documented that being a female is considered to be a risk factor for scoliosis progression when compared to boys [3]. Studies have reported that scoliosis is higher in females than in males across all ages [16,46,48,49]. Several factors, such as ethnicity, age, sex, maturity, BMI, genetics, socioeconomic situation, geographical latitude and screening tests used during SSS, may affect AIS prevalence [1,3,15,43,44,45,46,50]. Generally, it has been accepted that AIS prevalence is 2–3% in adolescents under 16 years old [43,44,45,46]. Du et al. (2016) reported that girls had higher prevalence (3.11%) than boys (1.96%) [48], and Yang et al. (2020) referred 5.2% of girls for radiography, a 2.2 times higher percentage than boys [16]. Furthermore, Yilmaz et al. (2020) found that AIS prevalence was higher in girls (3.1%) than in boys (1.5%). Additionally, they reported higher AIS prevalence in girls across all ages [46]. Similarly, our SSS study indicated higher prevalence in girls than in boys (boys: 6.8% (n = 38) and girls: 9.9% (n = 50)) who had six or more degrees for the primary ATR. Our study’s results could not be directly compared to other studies, though, as our evaluation method was not a definitive diagnosis of scoliosis.
4.3. Limitations
There was not an actual laterality assessment. Instead, each student reported their dominant hand as the one used for writing and the dominant leg as the one used to kick a ball. Another limitation could be the selection of children only from private schools. The main reason for this decision was that the school scoliosis screening was offered by the Ministry of Health of Cyprus only to the children of public secondary schools. However, socioeconomic backgrounds and scoliosis experiences might be different. Consequently, a study that evaluates the scoliosis incidences between public and private schools is required.
5. Conclusions
In conclusion, in the current study, girls had higher measurements of the ATR than boys, but cross laterality was found only in boys, in both the general sample and scoliotic group. These results reveal different progression patterns of ATR between boys and girls during their growth. Future studies should focus on identifying how possible factors act on ATR progression differently in the two genders but particularly in boys since such available results are limited.
Author Contributions
E.T. and M.T.: conceptualization, study design/methodology, angle of trunk rotation evaluation, data collection, formal data analysis, writing—original draft preparation, writing—reviewing and editing and project administration. M.H.: formal data analysis and writing—reviewing and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the National Bioethics Committee of Cyprus (protocol code: ΕΕΒΚ ΕΠ 2021.01.169 on 23 August 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors express their gratitude to the students for their volunteered involvement in this study, to their parents and to the P.E. staff of the private schools that participated in the study. The authors would also like to thank the former Minister of Health, Michael Hadjipantelas, and the General Director of the Ministry of Health, Christina Yiannaki, for their support of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Grivas, T.B.; Vasiliadis, E.S.; Rodopoulos, G.; Kovanis, I. School Screening as a Research Tool in Epidemiology, Natural History and Aetiology of Idiopathic Scoliosis. Stud. Health Technol. Inform. 2008, 135, 84. [Google Scholar] [PubMed]
- Bortone, I.; Piazzolla, A.; Buongiorno, D.; Bizzoca, D.; Fiore, P.; Bevilacqua, V.; Moretti, B. Influence of Clinical Features of the Spine on Gait Analysis in Adolescent with Idiopathic Scoliosis. In Proceedings of the 2020 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Bari, Italy, 1 June–1 July 2020; pp. 1–6. [Google Scholar]
- Haleem, S.; Nnadi, C. Scoliosis: A Review. Paediatr. Child Health 2018, 28, 209–217. [Google Scholar] [CrossRef]
- Ciortea, V.; Ungur, R.; Irsay, L.; Onac, I.; Popa, A.; Popa, D.; Borda, I.M. Classification of Scoliosis. Palestrica Third Millenn. Civiliz. Sport 2014, 15, 209–217. [Google Scholar]
- Ilie, E.; Orțănescu, D.; Rusu, L.; Cosma, G. The Short-Term Effect of Kinesio® Taping Applications on Muscule Tonus in Preteens with Functional Scoliosis. Discobolul-Phys. Educ. Sport Kinetotherapy J. 2017, 13, 49–54. [Google Scholar]
- Khubaib, F.; Maqsood, U.; Mahmood, T.; Arshad, H.S.; Mahmood, W. Risk Factors of Non-Structural Scoliosis in Adults with Low Back Pain. Rawal Med. J. 2019, 44, 498–501. Available online: https://www.rmj.org.pk/?mno=300142 (accessed on 27 November 2023).
- Ovadia, D. Classification of Adolescent Idiopathic Scoliosis (AIS). J. Child. Orthop. 2013, 7, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Gera, C.; Malik, M. Effect of Spinal Manipulation on Cardiopulmonary Parameters in Patients with Functional Scoliosis: A Randomised Controlled Pilot Trial. Adv. Rehabil. Rehabil. 2022, 36, 11–17. [Google Scholar] [CrossRef]
- Li, X.; Zhang, L. Sports Rehabilitation of Patients with Scoliosis Based on Intelligent Data Collection Technology under the Background of Artificial Intelligence. In Proceedings of the 2021 3rd International Conference on Artificial Intelligence and Advanced Manufacture, Manchester, UK, 23–25 October 2021; pp. 1131–1136. [Google Scholar] [CrossRef]
- Minghelli, B. Scoliosis in Adolescence—A Revision. Austin Spine 2017, 1, 1002. [Google Scholar]
- Dobies-Krześniak, B.; Werblińska, A.; Tarnacka, B. Lateralization Direction, Strength, and Consistency in Juvenile and Adolescent Idiopathic Scoliosis: A Case Control Pilot Study. Symmetry 2022, 14, 888. [Google Scholar] [CrossRef]
- Goldberg, C.J.; Moore, D.P.; Fogarty, E.E.; Dowling, F.E. Handedness and Spinal Deformity. Stud. Health Technol. Inform. 2006, 5, 442–448. [Google Scholar]
- Milenkovic, S.; Kocijancic, R.; Belojevic, G. Left Handedness and Spine Deformities in Early Adolescence. Eur. J. Epidemiol. 2004, 19, 969–972. [Google Scholar] [CrossRef] [PubMed]
- Arienti, C.; Buraschi, R.; Donzelli, S.; Zaina, F.; Pollet, J.; Negrini, S. Trunk Asymmetry Is Associated with Dominance Preference: Results from a Cross-Sectional Study of 1029 Children. Braz. J. Phys. Ther. 2019, 23, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Grivas, T.B.; Vasiliadis, E.S.; Polyzois, V.D.; Mouzakis, V. Trunk Asymmetry and Handedness in 8245 School Children. Pediatr. Rehabil. 2006, 9, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Lu, X.; Yan, B.; Huang, Y. Prevalence of Incorrect Posture among Children and Adolescents: Finding from a Large Population-Based Study in China. iScience 2020, 23, 101043. [Google Scholar] [CrossRef] [PubMed]
- Schlösser, T.P.; Vincken, K.L.; Attrach, H.; Kuijf, H.J.; Viergever, M.A.; Janssen, M.M.; Castelein, R.M. Quantitative Analysis of the Closure Pattern of the Neurocentral Junction as Related to Preexistent Rotation in the Normal Immature Spine. Spine J. 2013, 13, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.M.; Kouwenhoven, J.-W.M.; Schlösser, T.P.; Viergever, M.A.; Bartels, L.W.; Castelein, R.M.; Vincken, K.L. Analysis of Preexistent Vertebral Rotation in the Normal Infantile, Juvenile, and Adolescent Spine. Spine 2011, 36, E486–E491. [Google Scholar] [CrossRef]
- Schlösser, T.P.C.; Semple, T.; Carr, S.B.; Padley, S.; Loebinger, M.R.; Hogg, C.; Castelein, R.M. Scoliosis Convexity and Organ Anatomy Are Related. Eur. Spine J. 2017, 26, 1595–1599. [Google Scholar] [CrossRef]
- Castro, C.; Neves Silva, J.; Matos, E.; Xavier Sousa, S.; Gonçalves, D.; Azevedo, N.; Rodrigues, L.; Pacheco, G. Relationship between Handedness and the Incidence of Spinal Changes in the Frontal Plane: Evaluation Using Idiag® Spinal Mouse®. Ann. Med. 2021, 53 (Suppl. S1), S151. [Google Scholar] [CrossRef]
- Catanzariti, J.-F.; Guyot, M.-A.; Agnani, O.; Demaille, S.; Kolanowski, E.; Donze, C. Eye–Hand Laterality and Right Thoracic Idiopathic Scoliosis. Eur. Spine J. 2014, 23, 1232–1236. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Abate Daga, F.; Panzolini, M.; Allois, R.; Baseggio, L.; Agostino, S. Age-Related Differences in Hamstring Flexibility in Prepubertal Soccer Players: An Exploratory Cross-Sectional Study. Front. Psychol. 2021, 12, 741756. [Google Scholar] [CrossRef] [PubMed]
- Kotwicki, T.; Negrini, S.; Grivas, T.; Rigo, M.; Maruyama, T.; Durmala, J.; Zaina, F. Members of the International Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT): Methodology of Evaluation of Morphology of the Spine and the Trunk in Idiopathic Scoliosis and Other Spinal Deformities-6th SOSORT Consensus Paper. Scoliosis 2009, 4, 26. [Google Scholar] [CrossRef] [PubMed]
- Coelho, D.M.; Bonagamba, G.H.; Oliveira, A.S. Scoliometer Measurements of Patients with Idiopathic Scoliosis. Braz. J. Phys. Ther. 2013, 17, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Osiński, W. Antropomotoryka, 2nd ed.; AWF Poznań: Poznań, Poland, 2003. [Google Scholar]
- Bondi, D.; Prete, G.; Malatesta, G.; Robazza, C. Laterality in Children: Evidence for Task-Dependent Lateralization of Motor Functions. Int. J. Environ. Res. Public Health 2020, 17, 6705. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, R. Meta-Analytic Procedures for Social Research, 2nd ed.; Sage: Newbury Park, CA, USA, 1991. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; 12 Lawrence Erlbaum Associates Inc.: Hillsdale, MI, USA, 1988; Volume 13. [Google Scholar]
- Schlösser, T.P.; Tsirikos, A.I.; Castelein, R.M. Aetiological Process of Idiopathic Scoliosis: From a Normal Growing Spine into a Complex 3D Spinal Deformity. Orthop. Trauma 2021, 35, 321–327. [Google Scholar] [CrossRef]
- Kocahan, T.; Akınoğlu, B.; Yilmaz, A.E.; Rosemann, T.; Knechtle, B. Intra- and Inter-Rater Reliability of a Well-Used and a Less-Used IsoMed 2000 Dynamometer for Knee Flexion and Extension Peak Torque Measurements in a Concentric Test in Athletes. Appl. Sci. 2021, 11, 4951. [Google Scholar] [CrossRef]
- Kluszczyński, M.; Pilis, A.; Czaprowski, D. The Importance of the Size of the Trunk Inclination Angle in the Early Detection of Scoliosis in Children. BMC Musculoskelet. Disord. 2022, 23, 5. [Google Scholar] [CrossRef]
- Di Paolo, S.; Zaffagnini, S.; Pizza, N.; Grassi, A.; Bragonzoni, L. Poor Motor Coordination Elicits Altered Lower Limb Biomechanics in Young Football (Soccer) Players: Implications for Injury Prevention through Wearable Sensors. Sensors 2021, 21, 4371. [Google Scholar] [CrossRef]
- Mosher, A.; Till, K.; Fraser-Thomas, J.; Baker, J. Revisiting Early Sport Specialization: What’s the Problem? Sports Health Multidiscip. Approach 2022, 14, 13–19. [Google Scholar] [CrossRef]
- Puzzitiello, R.N.; Rizzo, C.F.; Garvey, K.D.; Matzkin, E.G.; Salzler, M.J. Early Sports Specialisation and the Incidence of Lower Extremity Injuries in Youth Athletes: Current Concepts. J. ISAKOS 2021, 6, 339–343. [Google Scholar] [CrossRef]
- Ribeiro, C.Z.P.; Akashi, P.M.H.; Sacco, I.d.C.N.; Pedrinelli, A. Relationship between Postural Changes and Injuries of the Locomotor System in Indoor Soccer Athletes. Rev. Bras. Med. Esporte 2003, 9, 98–103. [Google Scholar] [CrossRef]
- AMSSM Collaborative Research Network Youth Early Sport Specialization Summit; Tenforde, A.S.; Montalvo, A.M.; Nelson, V.R.; Myer, G.D.; Brenner, J.S.; DiFiori, J.P.; Jayanthi, N.A.; Marshall, S.W.; Kliethermes, S.A.; et al. Current Sport Organization Guidelines From the AMSSM 2019 Youth Early Sport Specialization Research Summit. Sports Health Multidiscip. Approach 2022, 14, 135–141. [Google Scholar] [CrossRef]
- Asadi, M.; Nourasteh, A.; Daneshmandi, H. Comparison of Spinal Column Curvatures Between Master Football Players and Their Non-Athletes Peers. IJSS 2014, 5, 338–342. [Google Scholar]
- Całka-Lizis, T.; Jankowicz-Szymańska, A.; Adamczyk, K. Body Posture in Schoolchildren Undergoing Regular Football Training Compared to Their Peers. Pol. J. Sports Med. 2008, 24, 224–230. [Google Scholar]
- Blagrove, R.C.; Bruinvels, G.; Read, P. Early Sport Specialization and Intensive Training in Adolescent Female Athletes: Risks and Recommendations. Strength Cond. J. 2017, 39, 14–23. [Google Scholar] [CrossRef]
- Hayano, T.; Plummer, H.; Oliver, G.; Andrews, J.R. Early Sport Specialization in the Adolescent Female Athlete. Ann. Jt. 2021, 6, 41. [Google Scholar] [CrossRef]
- Blanchet, M.; Guertin, P.; Pilon, F.; Gorce, P.; Prince, F. From Neural Command to Robotic Use: The Role of Symmetry/Asymmetry in Postural and Locomotor Activities. Symmetry 2021, 13, 1773. [Google Scholar] [CrossRef]
- Adamczewska, K.; Wiernicka, M.; Kamińska, E.; Małecka, J.; Dąbrowska, A.; Malchrowicz-Mośko, E. Annual Observation of Changes in the Angle of Trunk Rotation. Trunk Asymmetry Predictors. A Study from a Scoliosis Screening in School Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 1899. [Google Scholar] [CrossRef]
- Adamczewska, K.; Wiernicka, M.; Malchrowicz-Mośko, E.; Małecka, J.; Lewandowski, J. The Angle of Trunk Rotation in School Children: A Study from an Idiopathic Scoliosis Screening. Prevalence and Optimal Age Screening Value. Int. J. Environ. Res. Public Health 2019, 16, 3426. [Google Scholar] [CrossRef]
- Hresko, M.T.; Talwalkar, V.; Schwend, R. Early Detection of Idiopathic Scoliosis in Adolescents. JBJS 2016, 98, e67. [Google Scholar] [CrossRef]
- Yılmaz, H.; Zateri, C.; Ozkan, A.K.; Kayalar, G.; Berk, H. Prevalence of Adolescent Idiopathic Scoliosis in Turkey: An Epidemiological Study. Spine J. 2020, 20, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Magee, D.J. Orthopedic Physical Assessment, 6th ed.; Elservier Inc.: North York, ON, Canada, 2014. [Google Scholar]
- Du, Q.; Zhou, X.; Negrini, S.; Chen, N.; Yang, X.; Liang, J.; Sun, K. Scoliosis Epidemiology Is Not Similar All over the World: A Study from a Scoliosis School Screening on Chongming Island (China). BMC Musculoskelet. Disord. 2016, 17, 303. [Google Scholar] [CrossRef] [PubMed]
- Tisano, A.; Alito, A.; Milardi, D.; Fazio, R.; Virelli, L.; Zanella, C.; Ruggeri, C.; Filardi, V.; Bruschetta, D. Statistical Investigation about Spinal Clinical Asymmetry in a School Population. J. Orthop. 2020, 22, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Ekşi, M.Ş.; Özcan-Ekşi, E.E.; Huet, S.E.; Dinç, T.; Özmen, B.B.; Akçal, M.A. Prevalence of Thoracic Scoliosis in Adolescents in Turkey: Analysis of 1065 Chest Radiographs. World Neurosurg. 2020, 135, e527–e540. [Google Scholar] [CrossRef]
Figure 1.
Adam’s forward bend test.

Figure 2.
Obtaining measurements.

Figure 3.
Handedness results for ATR A side in boys.

Figure 4.
Footedness results for ATR A side in boys.

Figure 5.
Handedness results for ATR A side in girls.

Figure 6.
Footedness results for ATR A side in girls.

Figure 7.
Handedness results for ATR A side in scoliotic boys.

Figure 8.
Footedness results for ATR A side in scoliotic boys.

Figure 9.
Handedness results for ATR A side in scoliotic girls.

Figure 10.
Footedness results for ATR A side in scoliotic girls.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
ATR categories.
| ATR A (Degrees) | ATR B (Degrees) | |||||
|---|---|---|---|---|---|---|
| Degree Categories | Boys | Girls | All | Boys | Girls | All |
| 0–2 | 49% (n = 274) | 44.3% (n = 224) | 46.7% (n = 498) | 93.4% (n = 522) | 90.5% (n = 459) | 92.1% (n = 981) |
| 3–5 | 44.2% (n = 247) | 45.8% (n = 232) | 45.1% (n = 479) | 5.4% (n = 30) | 6.9% (n = 34) | 6% (n = 64) |
| ≥6 | 6.8% (n = 38) | 9.9% (n = 50) | 8.3% (n = 88) | 1.3% (n = 7) | 2.6% (n = 13) | 1.9% (n = 20) |
| Total | 100% (n = 559) | 100% (n = 506) | 100% (n = 1065) | 100% (n = 559) | 100% (n = 506) | 100% (n = 1065) |
ATR A = primary angle of trunk rotation, ATR B = coexisting secondary angle of trunk rotation. 0–2 = no clinical impact, 3–5 = scoliotic posture, ≥6 = scoliotic group.
Table 2.
Difference between boys and girls.
| Gender | Mean Rank | Sum of Ranks | p | ES | |
|---|---|---|---|---|---|
| Age (years) | Boys | 532.98 | 297,935 | 0.998 | 0 |
| Girls | 533.02 | 269,710 | |||
| Height (cm) | Boys | 621.9 | 347,641.5 | <0.001 * | −0.3 |
| Girls | 434.79 | 220,003.5 | |||
| Weight (kg) | Boys | 584.41 | 326,685 | <0.001 * | −0.18 |
| Girls | 476.21 | 240,960 | |||
| BMI | Boys | 545.19 | 304,759.5 | 0.174 | −0.04 |
| Girls | 519.54 | 262,885.5 | |||
| ATR A (degrees) | Boys | 507.55 | 283,723 | 0.004 * | −0.09 |
| Girls | 561.11 | 283,922 | |||
| ATR B (degrees) | Boys | 521.4 | 291,460 | 0.023 * | −0.07 |
| Girls | 545.82 | 276,185 | |||
| Maturity | Boys | 512.61 | 286,549.5 | 0.002 * | −0.1 |
| Girls | 555.52 | 281,095.5 | |||
| DH | Boys | 541.537 | 302,719 | 0.089 | −0.05 |
| Girls | 523.569 | 264,926 | |||
| DL | Boys | 543.35 | 303,732.5 | 0.039 * | −0.06 |
| Girls | 521.566 | 263,912.5 |
BMI = body mass index, DH = dominant hand, DL = dominant leg. * Statistically significant difference.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Theodorou, E.; Hadjicharalambous, M.; Tryfonidis, M. School Scoliosis Screening: The Influence of Dominant Limbs and Gender. Adolescents 2024, 4, 62-74. https://doi.org/10.3390/adolescents4010005
AMA Style
Theodorou E, Hadjicharalambous M, Tryfonidis M. School Scoliosis Screening: The Influence of Dominant Limbs and Gender. Adolescents. 2024; 4(1):62-74. https://doi.org/10.3390/adolescents4010005
Chicago/Turabian StyleTheodorou, Eleni, Marios Hadjicharalambous, and Marios Tryfonidis. 2024. "School Scoliosis Screening: The Influence of Dominant Limbs and Gender" Adolescents 4, no. 1: 62-74. https://doi.org/10.3390/adolescents4010005