Changing rates but persisting seasons: patterns of enterovirus infections in hospitalizations and outpatient visits in Denmark 2015-2022
 Caroline Klint Johannesen1*
Caroline Klint Johannesen1*  Amanda Marie Egeskov-Cavling1 Micha Phill Grønholm Jepsen2 Theis Lange3
Amanda Marie Egeskov-Cavling1 Micha Phill Grønholm Jepsen2 Theis Lange3  Tyra Grove Krause4 Ulrikka Nygaard5
Tyra Grove Krause4 Ulrikka Nygaard5  Thea K. Fischer1,6
Thea K. Fischer1,6- 1Department of Clinical Research, North Zealand University Hospital, Hillerød, Capital Region, Denmark
- 2Department of Infective and Pulmonary Diseases, North Zealand University Hospital, Hillerød, Capital Region, Denmark
- 3Section of Biostatistics, Department of Public Health, University of Copenhagen, Copenhagen, Denmark
- 4Epidemiological Infection Preparedness, Statens Serum Institut, Copenhagen, Capital Region, Denmark
- 5Department of Paediatrics and Adolescent Medicine, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
- 6Department of Public Health, Section of Global Health, University of Copenhagen, Copenhagen, Denmark
Background: Enteroviruses (EV) constitute a diverse group of viruses manifesting a broad spectrum of clinical presentations in humans ranging from mild skin manifestations to more severe central nervous system (CNS) infection. Severe infections are reported with increased frequency globally, albeit the burden of diseases and the evolution of circulating viruses is largely unknown. We aimed to systematically explore contemporary trends in hospitalizations attributed to EV infections using national hospitalization discharge data.
Methods: We utilized the Danish National Patient Register which holds information on all contacts to Danish hospitals. We covered eight full years (2015-2022). Length-of-stay and administrative procedure codes were used to distinguish hospital admissions from outpatient visits. We utilized burden of disease estimates and distribution statistics.
Results: We identified 1029 hospitalizations and 1970 outpatient visits due to EV infections. The hospital admissions were primarily associated with CNS-infections (n=570, 55.4%) and skin (n=252, 24.5%), with variation over the studied period. The admitted patients were predominately children (43.8%) though patients were identified in all ages. The clinical manifestation was associated with age, with CNS infections dominating in the neonates and adults, and skin infections dominating in children 1-2 years (17.2%). Outpatient visits were predominantly observed among children 1-2 years (55.0%), presenting with skin symptoms (77.9%). We show a seasonal pattern of EV infections with summer/fall peaks and markedly impact on the EV hospitalization burden related to COVID-19 mitigation measures including national lockdown periods. 25% of hospital admissions occurred during 2020-2022.
Conclusion: EV infections caused both hospital admissions and outpatient visits in the period studied, predominately among children aged 1-2 years. Overall, skin infections dominated the outpatient visits, while the majority of hospital admissions were due to CNS infections. The pandemic period did not change the seasonal pattern of EV infections but notably lowered the number of admissions to hospital with CNS infection and raised the number of outpatient admissions with skin infection.
1 Introduction
Human enteroviruses (EV) are common viruses, with over 300 EV types characterized genetically by phylogenetic clustering to this date. EV belongs to the genus Enterovirus of the Picornaviridae family, consisting of single-stranded RNA viruses. EV are classified into four species (Enterovirus A- Enterovirus D) and three rhinovirus species (Rhinovirus A – Rhinovirus C) (1–3). Five additional animal species (Enterovirus E- Enterovirus J) exist as well. Most EV infections are asymptomatic or cause mild upper respiratory or gastrointestinal infections but EV can cause severe infections, in particular in young infants with central nervous system (CNS) involvement and potential long-term impairment (1, 4, 5). EV have been the cause of major epidemics, with severe clinical manifestation such as poliomyelitis (6). A European review of EV laboratory data through national reference laboratories between 2015-2017 reported that 66% of infections documented were in children younger than 5 years and that 45% of cases presented with neurological symptoms (7).
Recently, EV have been linked with acute flaccid myelitis (AFM), in particular types EV-D68 and EV-A71 have been recognized as causal agents of flaccid paralysis similar to poliomyelitis in children (8–10). In Denmark, the first case of AFM caused by EV-D68 was reported in 2020, and the circulation is monitored closely by the national public health institute, Statens Serum Institute (SSI) (11, 12). Commencing with the onset of the COVID-19 pandemic, there has been a surge in reports detailing EV infections attributed to Echovirus-11 in newborns with severe clinical impact and mortality higher than usual (13–16).
With the recent trends of more severe EV infections emerging and re-emerging, attention should be given to documenting the impact of these infections, including a more detailed description of the disease burden caused by the viruses. A study of EV-positive samples showed a steady number of between 215-315 positive per year from 2010-2013 (17). Studies of EV infections in Denmark based on reviews of medical journals have shown higher number of EV meningitis in adults in 2017/2018 compared to the years before, but with a decline again in 2019 (18, 19). There is no systematic information on severe EV infections in children or in adults without CNS involvement available from Denmark, and it is the aim of this study to provide information on all severe EV infections. This is needed to guide public health decisions on surveillance and interventions.
We explored the Danish national health registries to assess the burden of documented hospital admissions associated with EV infection regardless of clinical presentation in the Danish population during an 8-year period.
2 Materials and methods
We conducted an observational study of patients admitted to hospitals in Denmark from January 1, 2015, to December 31, 2022, utilizing data from the Danish National Patient Register (NPR) (20), the Medical Birth Register (MFR) (21), and the Cause of Death Register (DAR) (22) to gain information on demographics, outcomes, and risk factors. The NPR serves as a comprehensive research register founded on the entirety of administrative registrations documenting hospital contacts throughout Denmark. Each contact within this register is assigned a primary diagnosis using the International Classification of Disease no. 10 (ICD-10), and the inclusion of optional and unlimited secondary diagnoses enhances the depth of clinical information (20). The MFR holds detailed records of Danish births, with clinical information on mother, child, and delivery. Additionally, the repository contains administrative information outlining the procedures involved in each birth (21). The Cause of Death Registry (DAR) compiles information concerning all Danish residents who have deceased within the borders of Denmark. The causes of death are listed in the registry as they are declared on the death certificate of the diseased person (22).
Contacts to hospital with EV diagnosis was extracted from the NPR, where only the ICD-10 diagnosis is available. The registry holds no specific clinical information and no information on patient samples, though we assume that patients with EV specific diagnosis have had confirmative testing leading to the specific diagnosis. Diagnostic testing primarily occurred based on clinical indication. All samples positive for EV were shipped to the SSI reference laboratory for confirmation tests and subtyping of samples as part of the WHO polio surveillance framework (5, 17). EV are typically identified with polymerase chain reaction (PCR) tests on samples (cerebrospinal fluid (CSF), sputum, saliva, blood, skin, fecal) from patients with suspected EV infection. During the study period emergency departments and departments of infectious medicine invested in small point-of-care-test (POCT) PCR (POCT-PCR) machines, for syndromic testing. With this, most EV testing is conducted as real-time PCR tests at Departments of Clinical Microbiology (KMA) or the national reference laboratory at SSI, using in-house assays PCR-testing (17) or at hospitals using POCT with commercial syndromic assays PCR for CNS-, respiratory- or gastrointestinal infections (multiple manufacturers).
EV infections were defined by the ICD-10 codes and divided into groups based on diagnosis. Diagnostic groups were distinguished using ICD-10 codes. We divided the diagnosis into main groups after organ system and frequency, combining diseases in organ systems with few instances of registration into the group ‘Other’. In organ system group central nervous system (CNS), infections with symptoms involving the CNS are included. In the group skin infections, infections with presentations predominantly in the skin, such as rashes, blisters, or ulcers, are included. The specific diagnoses are presented in Table 1. Contacts to hospital were included in the study if patients were given at least one EV diagnosis, primary or secondary, during admission. Patients with contacts starting on or between 1. January 2015 and 31. December 2022 were included in the study. Information on discharge and deaths were obtained on 13. July 2023. Contacts with no discharge date at the end of study were excluded. Contacts due to accidents and planned recurrent visits (i.e., for follow-up treatment or examination) were excluded using administrative procedure codes. Contacts shorter than 12 hours were considered outpatient visits and contacts with a minimum of 12 hours of hospitalization were considered a hospital admission. Two concurrent admissions were treated as one admission if the time between discharge and next admission were 7 days or less. Recurrent admission with EV diagnosis within 90 days of discharge was investigated individually to establish if the second admission was a part of the first registered admission or a new infection causing hospital admission.
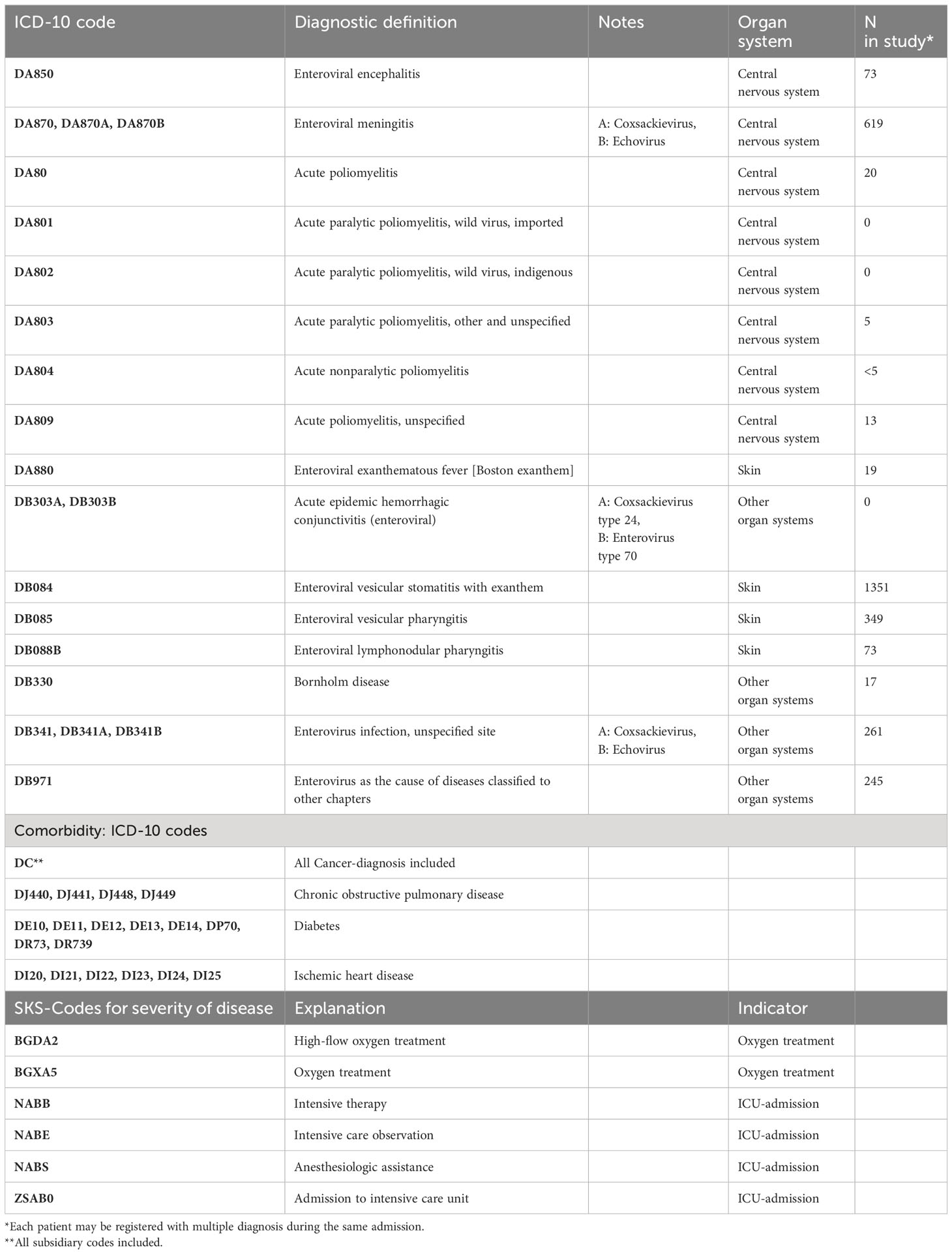
Table 1 ICD-10 codes and SKS-codes used to identify admissions with EV infection, severe outcomes, and comorbidities in adults.
We classified the patients into the following age groups by the age at admission: <1 month (30 days or less), 1-2 months (31 days -12 weeks), 3-5 months (13-24 weeks), 6-11 months (25-52 weeks), 1-2 years, 3-5 years, 6-17 years, 18-25 years, 26-45 years, 46-65 years, 66+ years.
We calculated length-of-stay (LOS) from the start of first registered admission, until last timestamp of the admission. If patients were transferred between departments or hospitals, the admissions were considered connected and counted as one admission.
Severe outcomes of the EV infection were defined as registered need for oxygen treatment, admission to the intensive care unit (ICU) or death. Patients who received oxygen treatment and/or admission to ICU were identified through procedure codes in NPR. Deaths during admission or within 30 days of discharge were identified in DAR.
Expected risk factors in the patients were identified through NPR and MFR. For children we investigated the distribution of preterm birth, low birth weight, and maternal smoking during pregnancy. In adults, we investigated the distribution of cancer, diabetes, ischemic heart disease, and chronic obstructive pulmonary disease (COPD).
We conducted descriptive analysis; frequency distributions and incidence rates pr. 100,000 person years, in age groups where appropriate. Population estimates were gathered from Statistics Denmark (23). We calculated medians and interquartile ranges (IQR) for continuous variables age and LOS. All analysis were performed using R version 4.3.1 (24).
3 Results
3.1 Hospital admissions
We identified 1029 patients admitted to hospitals with EV infections, and found they consisted of 1024 unique individuals based on the Danish civil registration system. 5 patients had multiple admissions with EV infection. 55.8% of patients were male, with male domination in all age groups except from 18-25 years (45% male) and 66+ years (36% male) (Table 2).
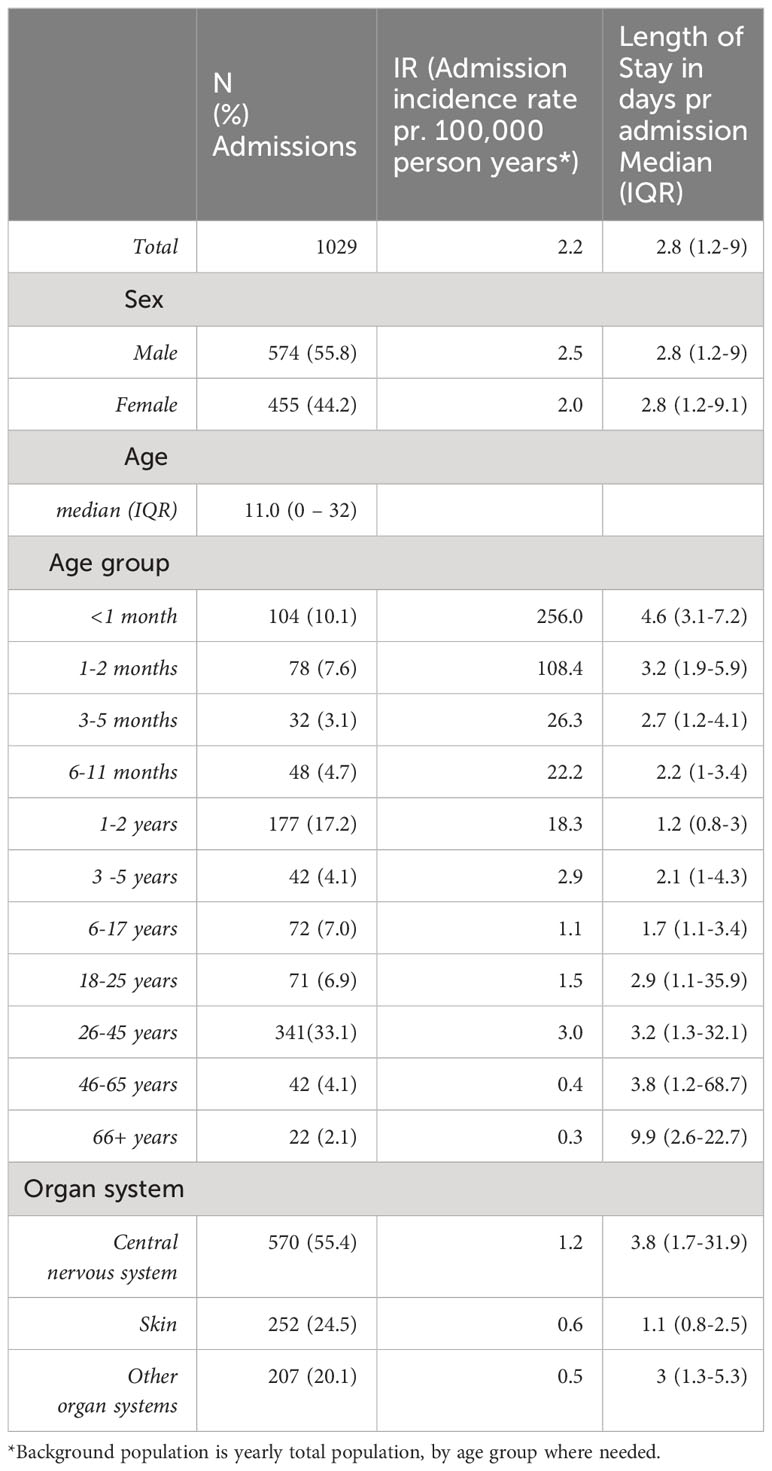
Table 2 Hospital admissions with enterovirus infection.
Patients younger than 3 years represented 42.7% (n=379) of all admissions and 262 admissions (25.5%) were in children younger than 1 year. The highest incidence rate of admission was found in the neonates (256 admissions pr. 100,000 children <1 month) (Table 2). Adults aged 26-45 years had the highest admission incidence rate (2.96 per 100,000), and this age group accounted for 33.1% of all patients admitted. Across all patients, the median length of stay (LOS) was 2.8 days (IQR: 1.2-9.0). Adults 66+ years had the longest median LOS, with 9.9 days (IQR: 2.6-22.7). In the adult age groups admissions with more than 30 bed days were not uncommon (26-45 years, median 3.8 (IQR: 1.2-68.7)) (Table 2). Among the youngest children (<1 month) the median LOS was 4.6 days (IQR: 3.1-7.2) (Table 2).
Our study covered eight full calendar years with a fluctuating number of admissions per year, reaching a maximum in 2018 (228 admissions, 22.2%) and a minimum in 2020 (52 admissions, 5.1%) (Table 3). Admissions by month followed a seasonal pattern, with few during the winter months of January to March, admissions increasing during the summer months of June and July, peaking either in the late summer months of August and September or in fall months October or November (Figure 1). During the COVID-19 pandemic period (2020–2022), the seasonal pattern continued but the number of cases was lower. The distribution between age groups changed during the study period, with a smaller portion of admissions occurring in adults during the pandemic period compared to the years 2017-2019 (Figure 2). A larger proportion of children (<18 years) admitted in the pandemic period were older than 6 months, while the proportion of children <1 month was not markedly different in this period (Figure 2).

Table 3 Yearly distributions for enterovirus admissions n (%).
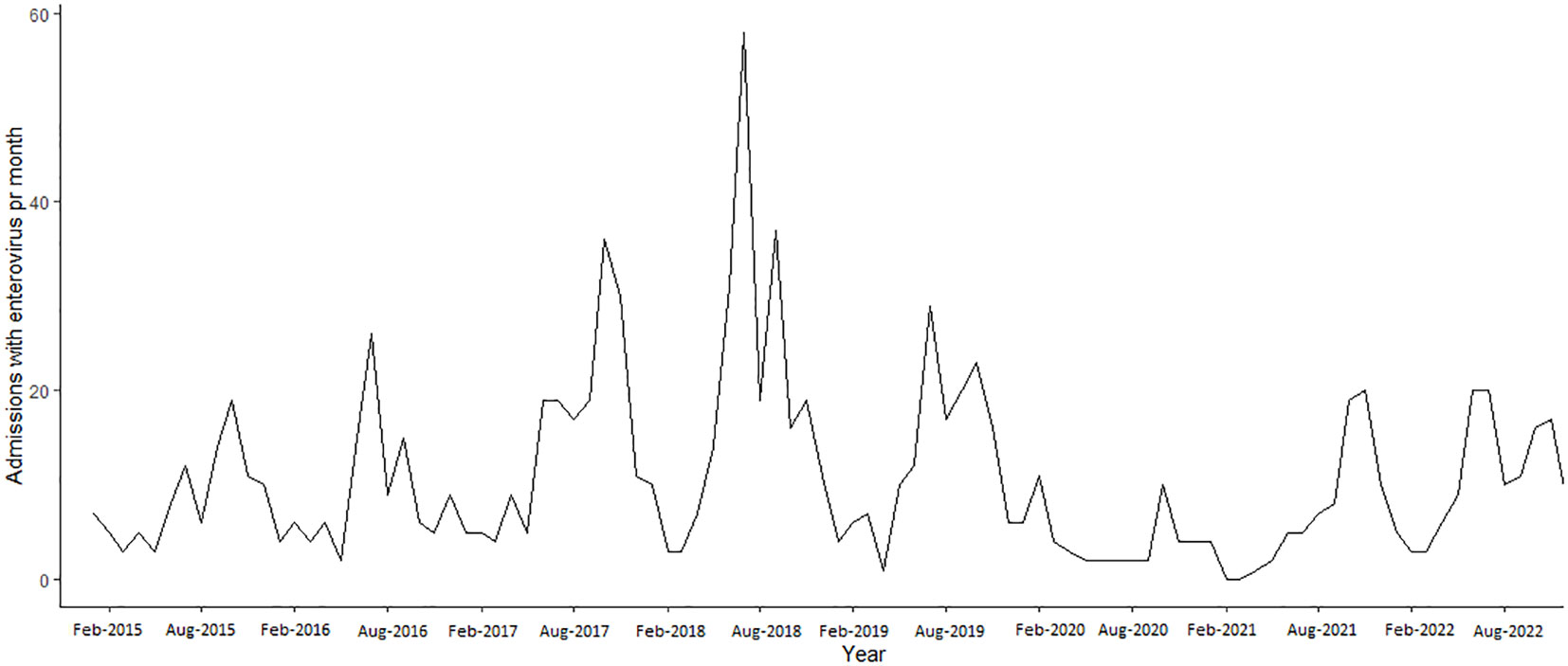
Figure 1 Enterovirus admissions per month 2015-2022.
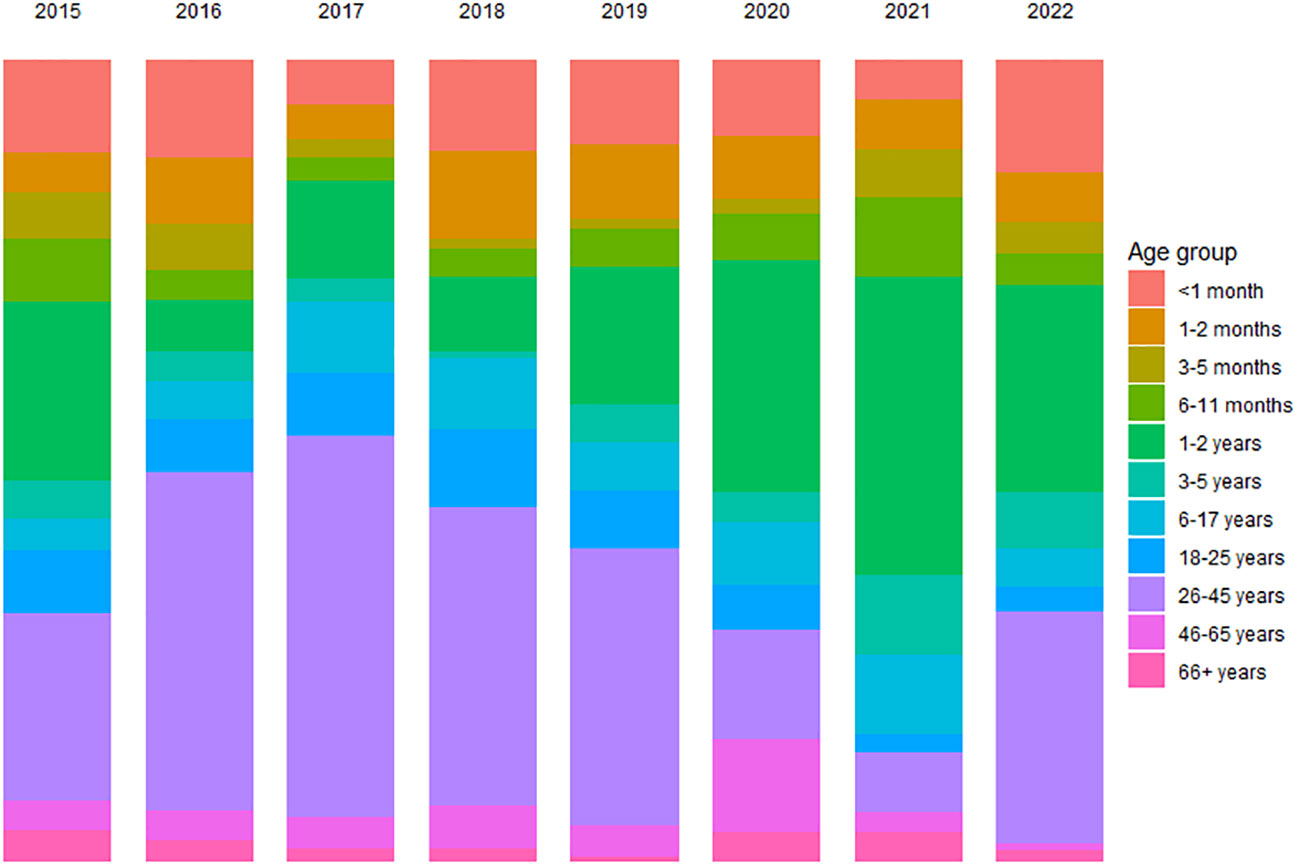
Figure 2 Age distribution in hospital admissions by year.
The patients were predominately admitted to hospital due to EV infection in two major organ systems: the CNS (55.4%) or the skin (24.5%), though other organ systems were affected in 20.1% of the admissions (see Table 1 for included diagnosis, Table 2). The disease pattern varied with age as children were more prone to be admitted with skin infections and adults more often admitted due to CNS infections (Figure 3).
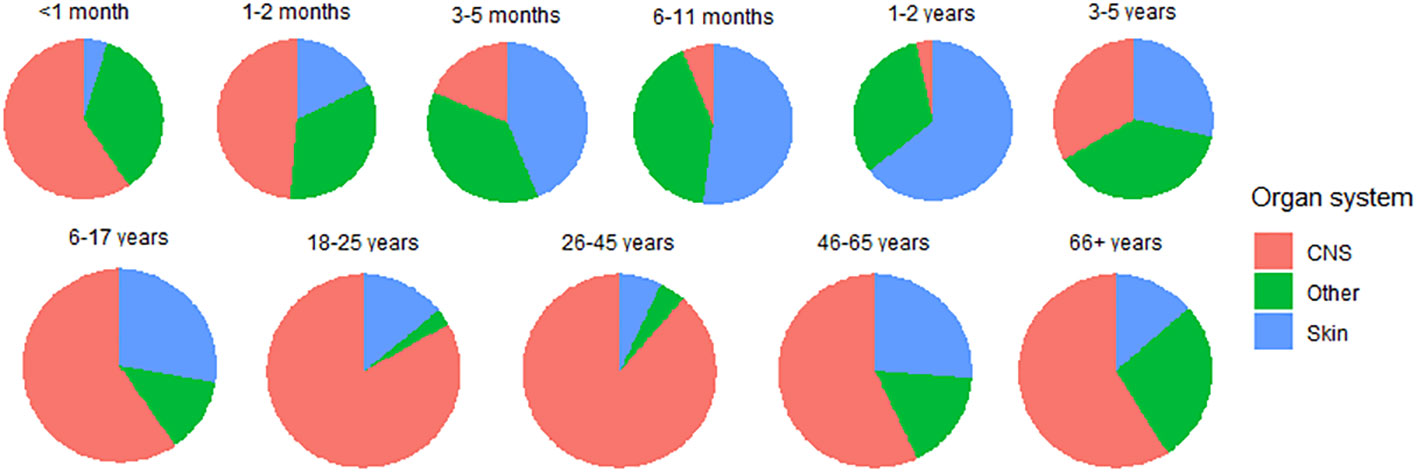
Figure 3 Distribution of infected organ systems in age groups.
The seasonal pattern differed by which organ system was infected (Figure 4). CNS-infections had clear seasonal peaks, while the seasonal variation was less pronounced for skin-infections and other infections. Skin- and other infections with EV occurred throughout the year, with small peaks at the same time as the CNS-infections, either in summer months around August or the fall month of October. During the COVID-19 pandemic period (2020-2022), the number of admissions with CNS-infections fell to exceptionally low levels and the expected peaks did not occur in 2020 and 2021, while admissions with skin and other infections did not change their seasonal pattern in this period.
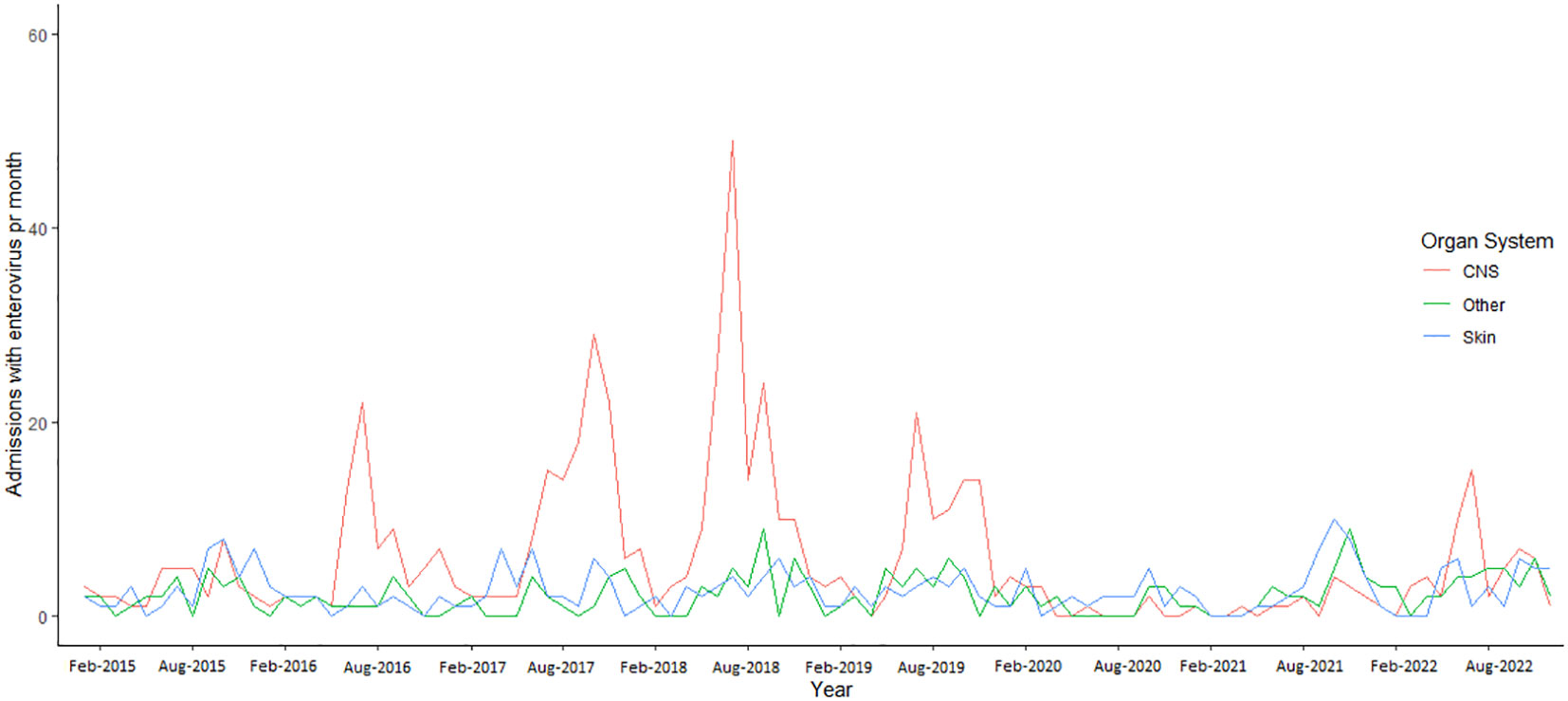
Figure 4 Enterovirus hospital admission by organ system affected 2015-2022.
When looking at severity of EV infections among the admitted patients, we found that 0.9% were admitted to the intensive care unit (ICU). Oxygen was required as a part of the treatment in 9.7% of admissions (n=100). Oxygen treatments were used in all age groups. In patients <1 month 5.8% received oxygen treatment, and children, the proportions receiving oxygen treatments varied between 2.6% (1-2 months) and 9.5% (3-5 years). In the age group 26-45 years 21.1% required oxygen treatment, which was the highest proportion among adults. Oxygen treatments were administered in 7% of CNS admissions, 2.6% of skin admissions and 1.1% of other admissions. Throughout the study period, there were 2 fatal cases within 30 days of EV-admission, all in adults above 45 years. There were no fatalities with EV-infection as registered cause of death (Data not shown).
We found that a possible risk factor in children admitted with EV was being born prematurely and with low birth weight (4.6% and 4.3% respectively in children <18 years, and in children younger than 1 year, 4.9% and 4.6% respectively) while 1.2% had low birth weight for their gestational age. Maternal tobacco usage during pregnancy occurred in 12.3% of admissions among children <18 years and 10.3% in children <1 year (Table 4).
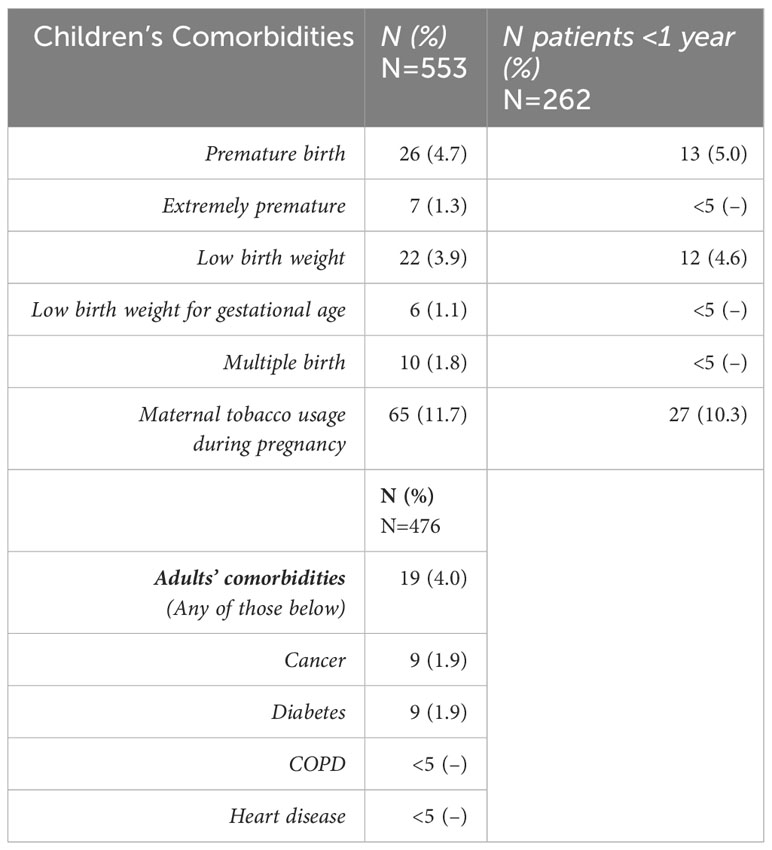
Table 4 Risk factor distributions in admissions in children <18 and <1 years and adults.
For adults, we investigated the distribution of diagnoses of cancer, diabetes, heart disease, and chronic obstructive pulmonary disease (COPD) (Table 4). In 3.9% of adults admitted with EV, the patient had a diagnosis of at least one of these comorbidities within 5 years before admission.
3.2 Outpatient visits
We identified 1970 outpatient visits (i.e., hospital stays shorter than 12 hours and not a planned control) with EV infections, where 59.0% of patients were male. The incidence rate per 100,000 person years was 4.3 visits (Table 5). Children aged 1-2 years accounted for 55.8% of the outpatient visits (IR: 113.8) while children <1 month had almost no outpatient visits (6, 0.3%). Among outpatients, skin infections were most prevalent, with 77.9% of all visits. CNS-infections constituted 7.0% of outpatient visits (Table 5). Over time, the number of outpatient visits per month increased, and in 2019-2022 a seasonal pattern emerged, which remained unchanged during the pandemic period (2020-2022) (Figure 5).
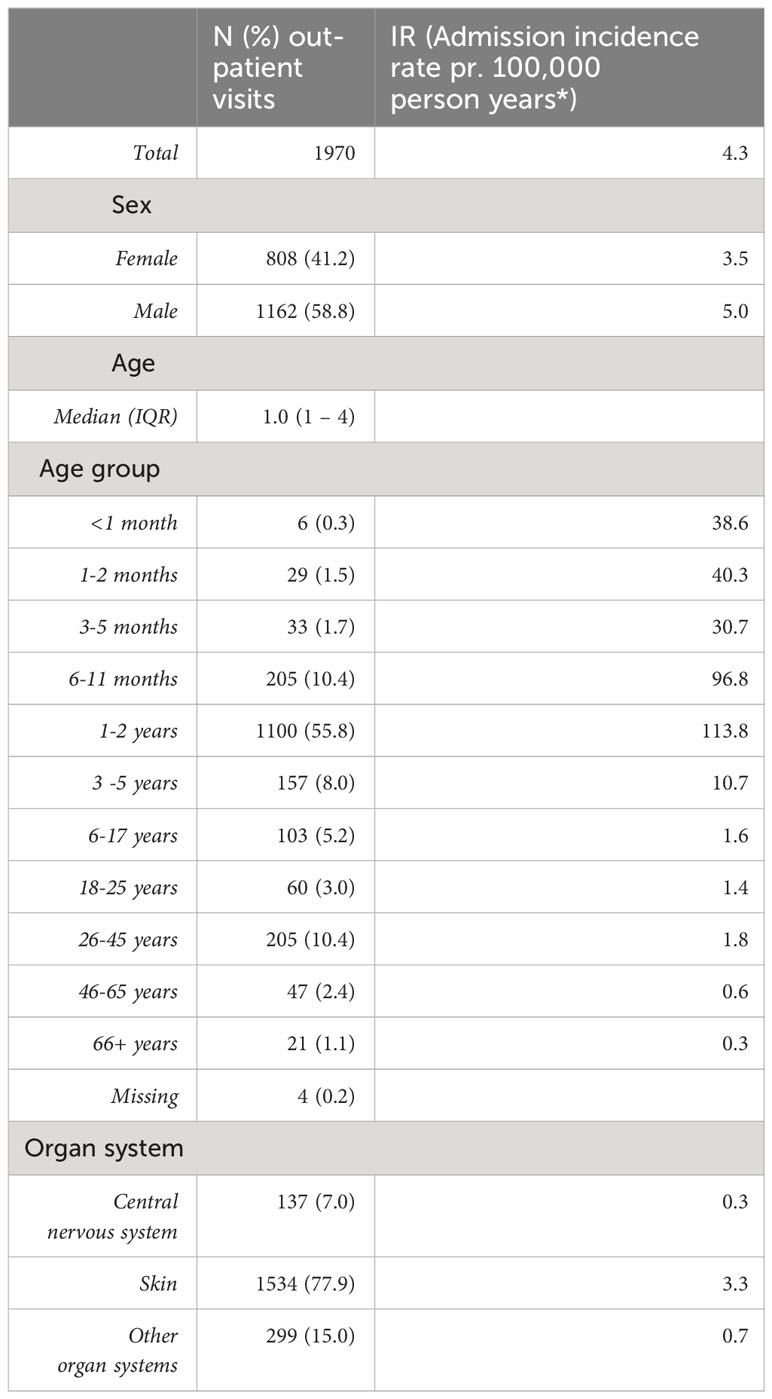
Table 5 Descriptive statistics for enterovirus outpatient visits.
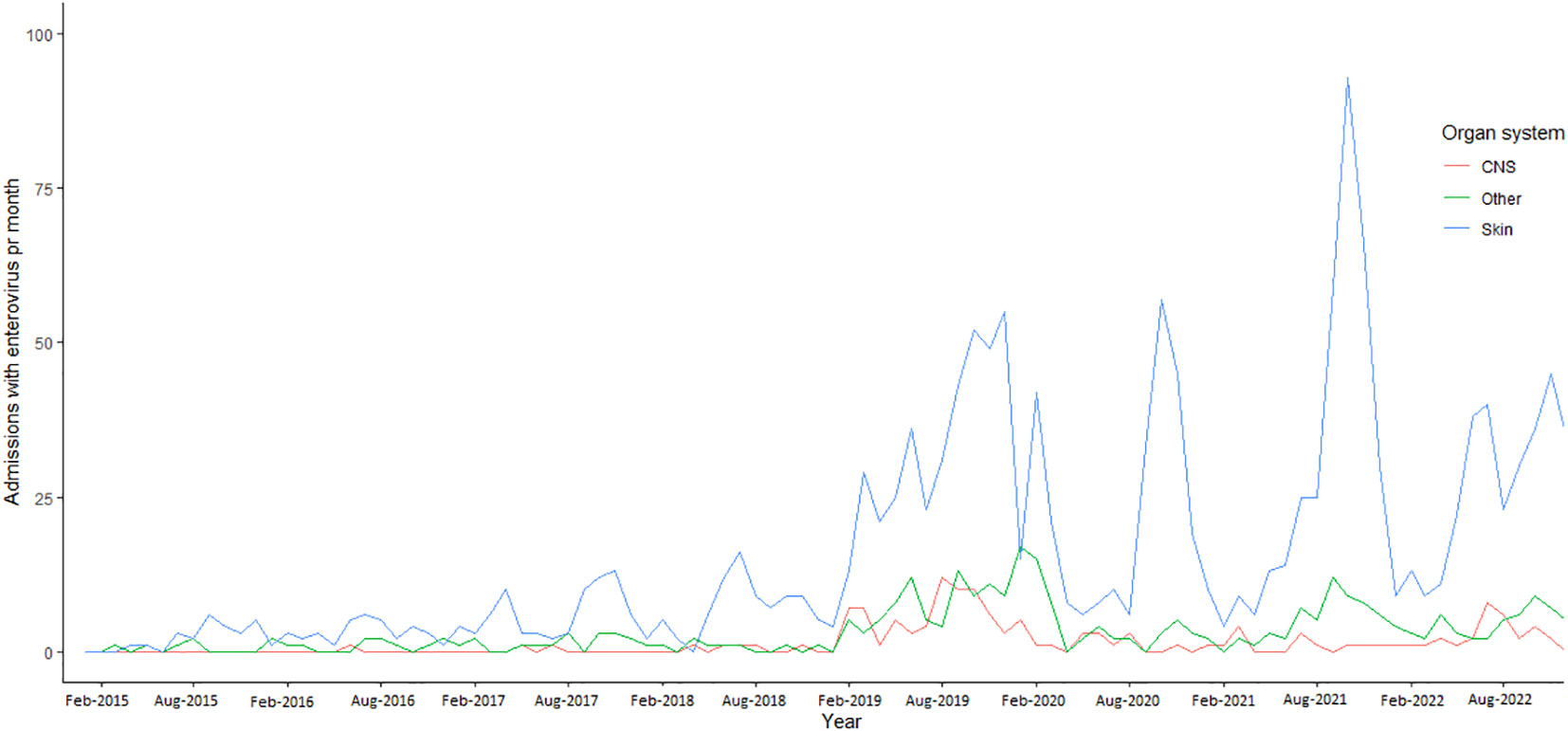
Figure 5 Enterovirus outpatient visits by organ system per month 2015-2022.
4 Discussion
In this study we documented the number of patients diagnosed and admitted with EV infections in Danish hospitals over an 8-year period. This is the largest full-national systematic documentation of severe EV infections in a European country to this date. Utilizing the National Danish health care registers, we were able to identify all registered EV infections causing either admission to hospital or outpatient visits. The proportion of EV admissions caused by CNS-infections was highest among in-patients, whereas skin-infections were most common among patients seen as out-patients. EV infections were predominantly registered among young children. CNS-infections constituted the majority of hospital admissions. However, it was notable that this trend deviated among the youngest infants aged 3-5 months up to 3-5 years. Hospitalizations among these young children were mainly caused by EV-associated skin infections (dominating diagnose of Hand-Foot-and Mouth disease (HFMD)). Also notably, among children in the age group of 3- 5 years, the distribution of hospital admissions reached parity among skin, CNS and other EV-infections (Figure 3). Among the hospital admissions, LOS differed between age groups, with longer stays in neonates, which could possibly be explained by hospital admissions for EV occurring simultaneously with their birth, as well as neonates being at higher risk of admission due to their venerability. In adults aged above 66 years, the LOS was the highest, which may be explained by EV infections occurring simultaneously with other severe diseases or chronic conditions worsening with the infections.
We observed a seasonal pattern characterized by peak infection rates in either the months of August and September or October and November. A trend that was less pronounced in hospital admissions during the pandemic period. This shift in pattern was attributed to a change in the prevalence of CNS infections, while skin infections and other infections maintained relatively low occurrences.
In 2018, hospital admissions with EV were at the highest during the study period. This peak can be explained by an echo 11 epidemic, as described by Broberg 2018 (25) The low number of hospitalizations in 2020 was explained by the COVID-19 pandemic control measurements such as lock downs and restrictions on public activities (13, 26).
The number of outpatient visits exhibited an increasing trend from 2019 onwards, with skin infections predominantly contributing to the rise in numbers. Notably, outpatient skin infections demonstrated a seasonal pattern since 2017, which became more distinct during this period marked by an increase in infections. In other locations such as Brazil, India, and China, changes to the seasonality of HFMD have been reported since the onset of the pandemic. China experienced a decrease in cases, while Brazil and India witnessed increases in HFMD cases (27–29). To our knowledge no European studies have been published on the latest trends in HFMD. We found an equal number of monthly outpatient visits and inpatient hospital admissions in 2017-2018, but the increased trend of outpatient visits from 2019 onwards shifted this distribution. Overall, there were 1970 outpatient visits versus 1029 inpatient hospitalizations. When considering the pathogen specific diagnosis, a positive test for EV is expected for a diagnosis of a disease with CNS-involvement, where skin lesions from EV infections can be differentiated from other skin infections by a trained physician. This difference may affect the number of outpatients presenting with CNS-symptoms correctly diagnosed with EV infections.
We observed that severe adverse outcomes such as ICU admissions or death were infrequent in our study, and we have not extended our follow-up information to include potential late presentations of severe sequelae including impaired motor functions or other disabilities. A longitudinal study conducted in Denmark revealed that across all age groups, individuals with EV infections exhibited a 10-fold higher 1-year mortality rate, with no discernible variation in subsequent years (5). Another Danish study focused on adults with EV meningitis and found that 20% of patients experienced outcomes ranging from moderate disability to death within 30 days of discharge (18).
A comprehensive Danish clinical database dedicated to collecting information on infections in the CNS has systematically compiled data on adult EV meningitis from all hospitals in Denmark (19). Given that this data collection is prioritized by clinicians, we anticipate a near-complete representation of EV meningitis cases among hospital admissions. From 2015 to 2019, a total of 419 cases of adult EV meningitis were documented, a slightly lower figure than the overall number of adult admissions (476) disregarding the affected organ system or specific diagnoses over an extended study period.
This observed discrepancy is likely attributable to underreporting of EV specific ICD-10 diagnosis in the healthcare registries, which primarily serve as administrative tools for the planning and financing of Denmark’s health care system. Similar deficiencies in ICD-10 codes within administrative registries of infectious diseases have been previously demonstrated in other settings when compared to clinical datasets of confirmed positive cases (30).
Beyond the variations in preferences for specific ICD-10 codes, our observations suggest that limited awareness of EV in general, may contribute to divergent practices in testing and diagnosis outpatient visits, where the seasonal trends of EV infections only became evident after 2018, coinciding with the increased adoption of point-of-care testing.
This discrepancy was most pronounced in outpatient visits, where the seasonal trends of EV infections only became evident after 2018, coinciding with the increased adoption of point-of-care testing polymerase chain reaction (POCT-PCR) in emergency departments across Denmark. In the case of young children, the rarity of pathogen diagnosis in CNS-infections coupled with low C-reactive protein (CRP) counts, often leads pediatricians to refrain from performing lumbar puncture procedures. Consequently, in the absence of a confirmed infective pathogen, hospital admissions are less likely to be assigned EV-specific ICD-10 codes. While our work has documented registered EV infections in Denmark from 2015 to 2022, the challenges associated with ICD-10 coding may have led to an underestimation of the true burden of EV infections.
We advocate for the adoption of prospective study designs, akin to those implemented in the Danish clinical database for adults with infections in the brain, and the surveillance pilots proposed by the European non-polio enterovirus network (19, 31). These approaches, encompassing all age groups and considering diverse clinical presentations, will be instrumental in detecting EV infections more comprehensively. By further investigating EV infections and systematically collecting information on symptoms, outcomes, diagnoses, and treatments, we can enhance our understanding of the intricate landscape of EV infections.
5 Conclusion
In this retrospective national study of EV-associated hospitalizations, CNS-infections were most prevalent among hospitalized patients across all ages, while skin-infections and HFMD was most common among pediatric outpatient visits. The affected organ system leading to hospital admission exhibited age-related variations, with CNS infections prevailing in the youngest children and in adults. Interestingly, the seasonal pattern of CNS-infections causing admissions showed a diminished prominence during the pandemic period. In contrast, the seasonality observed in skin infections prompting outpatient visits remained unaffected. This intriguing divergence in the impact of the pandemic on the seasonal dynamics of different EV-infection types warrants further investigation and consideration in public health strategies.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The datasets presented in this article are not readily available due to Danish data protection legislation. All register data in Denmark are accessible for researchers with approval for use from the relevant authorities. Requests to access the datasets should be directed to Sundhedsdatastyrelsen (The Danish Health Data Authority). Requests to access these datasets should be directed to e-sundhed.dk.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
CJ: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review and editing. AE: Data curation, Writing – review and editing. MJ: Supervision, Writing – review and editing. TL: Supervision, Writing – review and editing. TK: Supervision, Writing – review and editing. UN: Supervision, Writing – review and editing. TF: Conceptualization, Funding acquisition, Supervision, Writing – review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The work presented in this manuscript was funded by Nordsjaellands Hospitals Forskningspulje (The research pool), on a grant awarded in 2023.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nikonov OS, Chernykh ES, Garber MB, Nikonova E. Enteroviruses: Classification, diseases they cause, and approaches to development of antiviral drugs. Biochem Biokhimiia. (2017) 82:1615–31. doi: 10.1134/S0006297917130041
2. Zell R, Delwart E, Gorbalenya AE, Hovi T, King AMQ, Knowles NJ, et al. ICTV virus taxonomy profile: picornaviridae. J Gen Virol. (2017) 98:2421–2. doi: 10.1099/jgv.0.000911
3. Simmonds P, Gorbalenya AE, Harvala H, Hovi T, Knowles NJ, Lindberg AM, et al. Recommendations for the nomenclature of enteroviruses and rhinoviruses. Arch Virol. (2020) 165:793–7. doi: 10.1007/s00705-019-04520-6
4. Harvala H, Broberg E, Benschop K, Berginc N, Ladhani S, Susi P, et al. Recommendations for enterovirus diagnostics and characterisation within and beyond Europe. J Clin Virol Off Publ Pan Am Soc Clin Virol. (2018) 101:11–7. doi: 10.1016/j.jcv.2018.01.008
5. Omland LH, Holm-Hansen C, Lebech AM, Dessau RB, Bodilsen J, Andersen NS, et al. Long-term survival, health, social functioning, and education in patients with an enterovirus central nervous system infection, Denmark, 1997-2016. J Infect Dis. (2020) 222:619–27. doi: 10.1093/infdis/jiaa151
6. Minor PD. An introduction to poliovirus: pathogenesis, vaccination, and the endgame for global eradication. In: Martín J, editor. Poliovirus: Methods and Protocols. Springer, New York, NY (2016). p. 1–10. doi: 10.1007/978-1-4939-3292-4_1
7. Bubba L, Broberg EK, Jasir A, Simmonds P, Harvala H, Redlberger-Fritz M, et al. Circulation of non-polio enteroviruses in 24 EU and EEA countries between 2015 and 2017: a retrospective surveillance study. Lancet Infect Dis. (2020) 20:350–61. doi: 10.1016/S1473-3099(19)30566-3
8. Knoester M, Helfferich J, Poelman R, Van Leer-Buter C, Brouwer OF, Niesters HGM. Twenty-nine cases of enterovirus-D68–associated acute flaccid myelitis in Europe 2016. Pediatr Infect Dis J. (2019) 38:16–21. doi: 10.1097/INF.0000000000002188
9. Holm-Hansen CC, Midgley SE, Fischer TK. Global emergence of enterovirus D68: a systematic review. Lancet Infect Dis. (2016) 16:e64–75. doi: 10.1016/S1473-3099(15)00543-5
10. Fischer TK, Nielsen AY, Sydenham TV, Andersen PH, Andersen B, Midgley SE. Emergence of enterovirus 71 C4a in Denmark, 2009 to 2013. Euro Surveill Bull Eur Sur Mal Transm Eur Commun Dis Bull. (2014) 19:20911. doi: 10.2807/1560-7917.ES2014.19.38.20911
11. Hartling UB, Linnet KM, Thomsen MK, Midgley SE, Holm M. Akut slap parese associeret med enterovirus D68 hos et barn. Copenhagen, Denmark: Ugeskrift for læger (2020) 182(22):V10190616. Available at: https://ugeskriftet.dk/videnskab/akut-slap-parese-associeret-med-enterovirus-d68-hos-et-barn.
12. Midgley SE, Christiansen CB, Poulsen MW, Hansen CH, Fischer TK. Emergence of enterovirus D68 in Denmark, June 2014 to February 2015. Euro Surveill Bull Eur Sur Mal Transm Eur Commun Dis Bull. (2015) 20:21105. doi: 10.2807/1560-7917.ES2015.20.17.21105
13. Lee BR, Sasidharan A, Harrison CJ, Selvarangan R. Disruption of seasonal enterovirus and parechovirus detections in the CSF and plasma of children during the COVID-19 pandemic. J Clin Virol Off Publ Pan Am Soc Clin Virol. (2023) 160:105381. doi: 10.1016/j.jcv.2023.105381
14. Grapin M, Mirand A, Pinquier D, Basset A, Bendavid M, Bisseux M, et al. Severe and fatal neonatal infections linked to a new variant of echovirus 11, France, July 2022 to April 2023. Eurosurveillance. (2023) 28:2300253. doi: 10.2807/1560-7917.ES.2023.28.22.2300253
15. Wise J. Myocarditis: Unusual cluster of cases in babies is identified in Wales. BMJ. (2023) 381:1151. doi: 10.1136/bmj.p1151
16. Piralla A, Borghesi A, Di Comite A, Giardina F, Ferrari G, Zanette S, et al. Fulminant echovirus 11 hepatitis in male non-identical twins in northern Italy, April 2023. Euro Surveill Bull Eur Sur Mal Transm Eur Commun Dis Bull. (2023) 28:2300289. doi: 10.2807/1560-7917.ES.2023.28.24.2300289
17. Condell O, Midgley S, Christiansen CB, Chen M, Chen Nielsen X, Ellermann-Eriksen S, et al. Evaluation of the enterovirus laboratory surveillance system in Denmark, 2010 to 2013. Euro Surveill Bull Eur Sur Mal Transm Eur Commun Dis Bull. (2016) 21. doi: 10.2807/1560-7917.ES.2016.21.18.30218
18. Petersen PT, Bodilsen J, Jepsen MPG, Larsen L, Storgaard M, Hansen BR, et al. Clinical features and prognostic factors in adults with viral meningitis. Brain. (2023) 146:3816–25. doi: 10.1093/brain/awad089
19. Bodilsen J, Mens H, Midgley S, Brandt CT, Petersen PT, Larsen L, et al. Enterovirus meningitis in adults: A prospective nationwide population-based cohort study. Neurology. (2021) 97:e454–63. doi: 10.1212/WNL.0000000000012294
20. Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register(2011). Available online at: https://journals-sagepub-com.ep.fjernadgang.kb.dk/doi/abs/10.1177/1403494811401482.
21. The Danish Medical Birth Register on JSTOR. Available online at: https://www-jstor-org.ep.fjernadgang.kb.dk/stable/44849605?sid=primo.
22. Helweg-Larsen K. The Danish Register of Causes of Death(2011). Available online at: https://journals-sagepub-com.ep.fjernadgang.kb.dk/doi/abs/10.1177/1403494811399958.
23. StatBank Denmark. Population of Denmark. Available online at: https://www.statistikbanken.dk/statbank5a/default.asp?w=1920.
24. R Core Team. R: A Language and Environment for Statistical Computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing (2023). Available at: https://www.R-project.org/.
25. Broberg EK, Simone B, Jansa J. EU/EEA Member State contributors. Upsurge in echovirus 30 detections in five EU/EEA countries, April to September, 2018. Euro Surveill Bull Eur Sur Mal Transm Eur Commun Dis Bull. (2018) 23:1800537. doi: 10.2807/1560-7917.ES.2018.23.44.1800537
26. Rankin DA, Spieker AJ, Perez A, Stahl AL, Rahman HK, Stewart LS, et al. Circulation of rhinoviruses and/or enteroviruses in pediatric patients with acute respiratory illness before and during the COVID-19 pandemic in the US. JAMA Netw Open. (2023) 6:e2254909. doi: 10.1001/jamanetworkopen.2022.54909
27. Carmona RCC, MaChado BC, Reis FC, Jorge AMV, Cilli A, Dias AMN, et al. Hand, foot, and mouth disease outbreak by Coxsackievirus A6 during COVID-19 pandemic in 2021, São Paulo, Brazil. J Clin Virol Off Publ Pan Am Soc Clin Virol. (2022) 154:105245. doi: 10.1016/j.jcv.2022.105245
28. Farahat RA, Shaheen N, Kundu M, Shaheen A, Abdelaal A. The resurfacing of hand, foot, and mouth disease: Are we on the verge of another epidemic? Ann Med Surg. (2022) 81:104419. doi: 10.1016/j.amsu.2022.104419
29. Wu H, Xue M, Wu C, Lu Q, Ding Z, Wang X, et al. Trend of hand, foot, and mouth disease from 2010 to 2021 and estimation of the reduction in enterovirus 71 infection after vaccine use in Zhejiang Province, China. PloS One. (2022) 17:e0274421. doi: 10.1371/journal.pone.0274421
30. Pfister T, Rennert-May E, Ellison J, Bush K, Leal J. Clostridioides difficile infections in Alberta: The validity of administrative data using ICD-10 diagnostic codes for CDI surveillance versus clinical infection surveillance. Am J Infect Control. (2020) 48:1431–6. doi: 10.1016/j.ajic.2020.08.016
Keywords: enterovirus, epidemiology, cohort study, seasonality, meningitis, childhood infection, clinical presentation
Citation: Johannesen CK, Egeskov-Cavling AM, Jepsen MPG, Lange T, Krause TG, Nygaard U and Fischer TK (2024) Changing rates but persisting seasons: patterns of enterovirus infections in hospitalizations and outpatient visits in Denmark 2015-2022. Front. Virol. 4:1346352. doi: 10.3389/fviro.2024.1346352
Received: 29 November 2023; Accepted: 13 February 2024;
Published: 29 February 2024.
Edited by:
Susan Prockop, Boston Children’s Hospital and Harvard Medical School, United StatesReviewed by:
Carmen Baur Vieira, Fluminense Federal University, BrazilOmkar Indari, St. Jude Children’s Research Hospital, United States
Copyright © 2024 Johannesen, Egeskov-Cavling, Jepsen, Lange, Krause, Nygaard and Fischer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caroline Klint Johannesen, caroline.klint.johannesen@regionh.dk