Case report: Is bilateral renal dioctophymosis and severe uremia in a dog synonymous of euthanasia? Not today
 Pâmela Caye1*
Pâmela Caye1*  Jean Carlos Gasparotto1
Jean Carlos Gasparotto1  Anna Vitória Hörbe2 Letícia Rodrigues Leitao Andrade3 Rainer da Silva Reinstein1 Luiza Tonietto Mangini1 Daniel Curvello de Mendonça Müller4 Maurício Veloso Brun4,5
Anna Vitória Hörbe2 Letícia Rodrigues Leitao Andrade3 Rainer da Silva Reinstein1 Luiza Tonietto Mangini1 Daniel Curvello de Mendonça Müller4 Maurício Veloso Brun4,5- 1Postgraduate Program in Veterinary Medicine, Center for Rural Sciences, Federal University of Santa Maria, Santa Maria, Brazil
- 2Residency Program in Veterinary Medicine, University Veterinary Hospital, Federal University of Santa Maria, Santa Maria, Brazil
- 3Degree in Veterinary Medicine, Center for Rural Sciences, Federal University of Santa Maria, Santa Maria, Brazil
- 4Department of Small Animal Clinic, Rural Science Center, Federal University of Santa Maria, Santa Maria, Brazil
- 5Brazilian National Council for Scientific and Technological Development (CNPq) Research Productivity Scholarship-Level 1C (3304353/2021-3), Brazil
A dog with bilateral renal dioctophymosis presented with stage 5 acute kidney injury, weight loss, vomiting, apathy, and hematuria. Laboratory tests showed creatinine of 17.2 mg/dL and Dioctophyme renale eggs in the urine. It underwent a 30-min session of hyperbaric oxygen preconditioning at a pressure of 2 ATA. Subsequently, bilateral nephroscopy was performed, without warm ischemia, using Amplatz-type renal dilators. Five parasites were removed, three females from the right kidney, one female from the left kidney, and one male from the abdominal cavity. After surgery, the patient continued doing daily hyperbaric oxygen therapy (HBOT) sessions and clinical therapy. Postoperative care consisted of analgesics, antimicrobials, antioxidants, gastric protector and fluid therapy. Ultrasound monitoring showed a reduction in the area of renal dilation and the hematological and biochemical tests showed rapid recovery from acute kidney injury. There was no bacterial growth in the urine sample collected directly from the kidneys. The patient had an excellent clinical progression and was discharged from hospital 7 days postoperatively, with creatinine values of 2.9 mg/dL. This is the first report of the use of nephroscopy in the treatment of dioctophymosis and indicates excellent chances of cure even in severe cases of bilateral parasitosis. HBOT was shown to be an ally in the clinical therapy of patients with D. renale by helping with stabilization and postoperative recovery.
Introduction
Dioctophymosis in dogs occurs due to parasitism by Dioctophyme renale, a cosmopolitan nematode with worldwide distribution and common in southern Brazil (1–4). The parasite usually affects the hosts' right kidney, leading to chronic and irreversible destruction of the renal parenchyma (3, 5–8). Although rare, there are reports of bilateral renal dioctophymosis in dogs (9, 10) and humans (11), with most cases associated with patient death. Treatment is surgical and usually involves nephrectomy of the parasitized kidney (8). In general, nephron-sparing surgery is recommended, especially when there is major impairment of renal function and some renal viability. There are reports of laparoscopic nephrotomy to remove parasites in dogs with unilateral dioctophymosis (12). To the authors' knowledge, there are no reports of nephroscopy for the treatment of parasitosis. This report describes the first bilateral nephroscopy for the treatment of a dog with D. renale presenting with severe acute kidney injury (AKI).
Case description
A greyhound female dog, estimated to be 5 years old, was treated at a veterinary hospital after being referred by another professional. Six days before, it had been diagnosed with bilateral renal dioctophymosis due to D. renale. The owner reported that, at the time of diagnosis, it had been losing weight and appetite, showing apathy and its urine was red. On what was established as Day 1, the veterinarian responsible for the referral ordered hematological tests, which showed no abnormalities, and renal biomarkers, which indicated severe azotemia (Table 1). Urinalysis showed leukocyturia, hematuria, proteinuria, and D. renale eggs. It is noteworthy that creatinine had been measured 15 days previously and was slightly elevated (1.78 mg/dL).
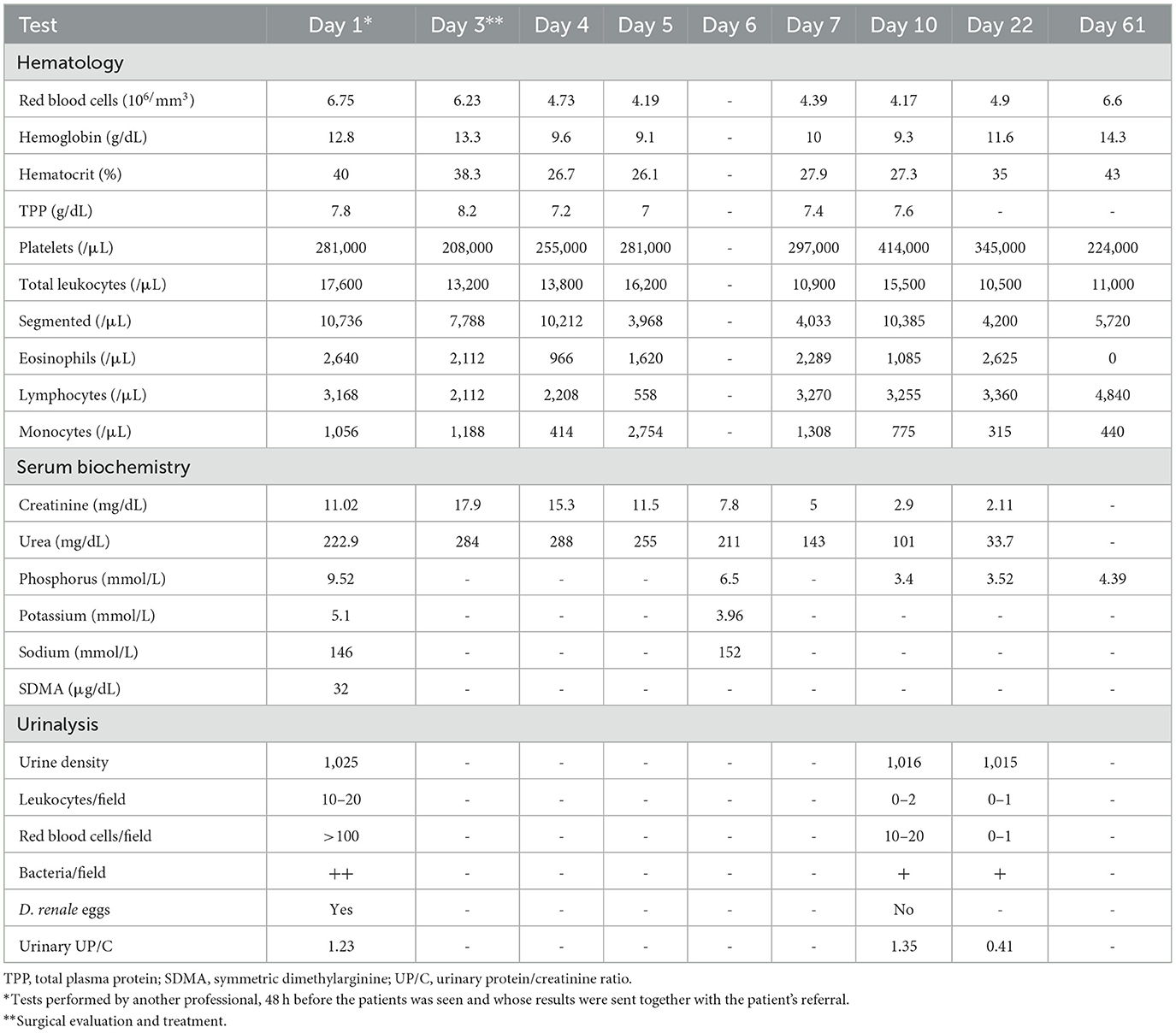
Table 1. Laboratory tests performed before and after nephroscopy and hyperbaric oxygen therapy in a dog with bilateral Dioctophyme renale.
At the time of its visit to the University Veterinary Hospital from Federal University of Santa Maria on Day 3, the patient had been suffering from anorexia for 4 days, increased fluid intake, nausea, vomiting, pasty stools, hematochezia, and hematuria. The following was described on clinical examination: weight of 22.6 kg, body score of 2/5, dehydration of 6%, abdominal rigidity, pain on palpation, capillary refill time of 3 s. Hematological and biochemical tests and ultrasound were repeated. The results are presented in Table 1. Worsening of biomarkers of renal function was observed, characterizing the clinical picture as uremic syndrome and classifying it as non-oliguric stage 5 AKI, according to IRIS (13).
Abdominal ultrasound confirmed the bilateral presence of parasites (Figures 1A, B). The right kidney measured 80 mm and had multiple cylindrical structures with hyperechoic edges and hypoechoic center. Minimal renal parenchyma was visualized. The area corresponding to the pelvis and the site where the parasites were found measured 66 mm. The left kidney was hypertrophic (104.4 mm) and had the same structures, although restricted to the internal medulla and renal pelvis (63.7 mm). The parenchyma appeared intact, with reduced corticomedullary definition and a diffuse increase in echogenicity. There was retroperitoneal reactivity adjacent to the renal contours.
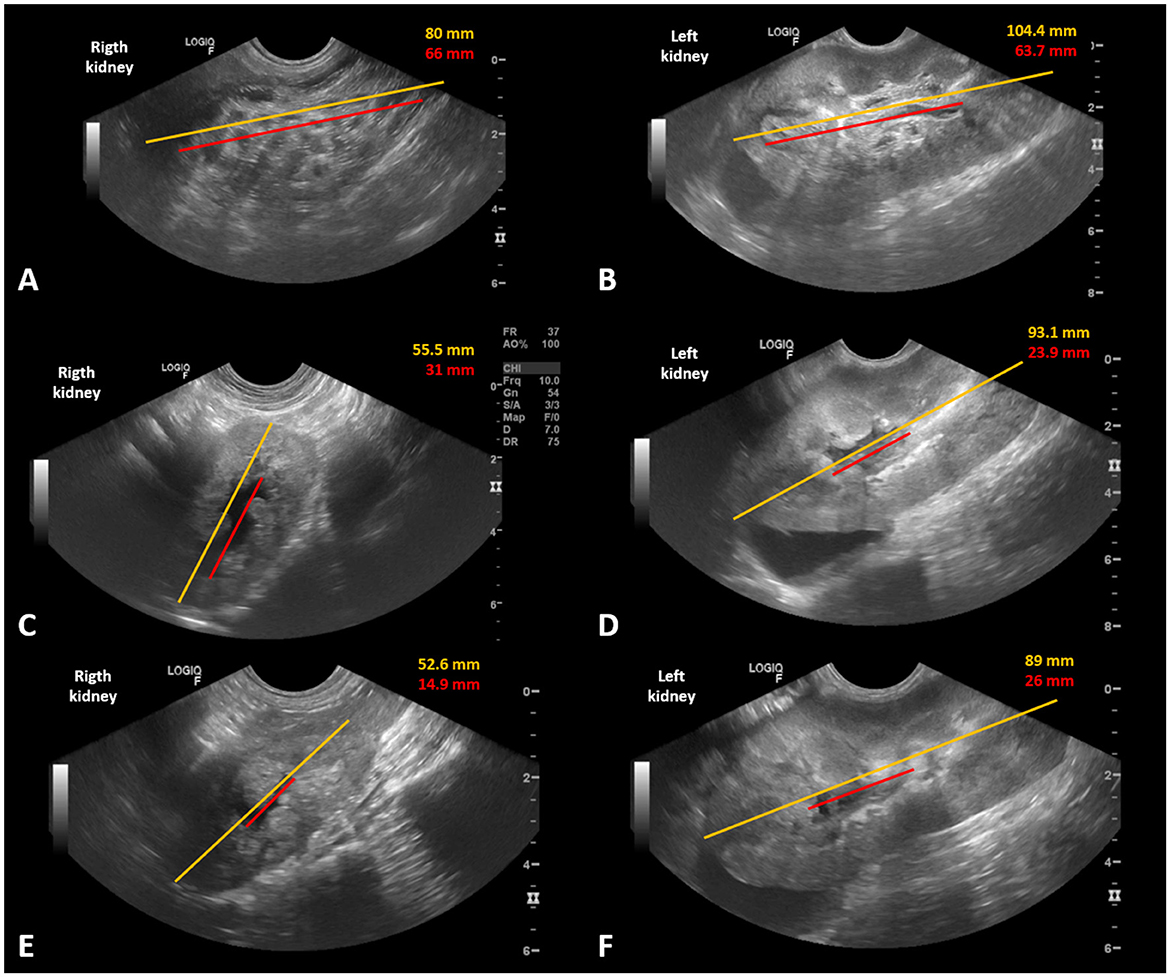
Figure 1. Ultrasound images of a dog with bilateral Dioctophyme renale, before and after bilateral nephroscopy to remove the parasites. (A) Preoperative appearance of the right kidney full of tubular structures with hyperechoic borders and a hypoechoic center. (B) Preoperative appearance of the left kidney, with the same structures, restricted to the internal medullary region and renal pelvis. (C, D) Appearance 48 h after the surgical procedure to remove the kidney parasites, with a significant reduction in the length and dilation of the bilateral pelvis. (E, F) Appearance 7 days after the surgical procedure, with a reduction in the hyperechogenicity of the parenchyma and inflammation, as well as a reduction in the dilation of both pelvises. Yellow line—approximate measurement of kidney length in a longitudinal section. Red line—approximate measurement of the area where the parasites were located and dilation of the pelvis.
The patient immediately began treatment with fluid therapy with Ringer's lactate (4 ml/kg/h) to correct dehydration, analgesia with dipyrone (25 mg/kg, IV) and methadone (0.2 mg/kg, SC), and antibiotic therapy with cephalothin (30 mg/kg, IV). After administration of the medications, the patient underwent the first session of hyperbaric oxygen therapy (HBOT; Figure 2A). The therapy was carried out in a veterinary monoplace chamber (HVM™), pressurized with 100% oxygen at a pressure of 2 ATA (atmosphere absolute). The dog remained inside the chamber for 60 min, including 15 min of pressurization, 30 min of therapy, and 15 min of depressurization. It made a slight rapid head movement, suggesting ear discomfort, and urinated inside the chamber. It did not show any other type of discomfort during the session and remained lying down and calm.
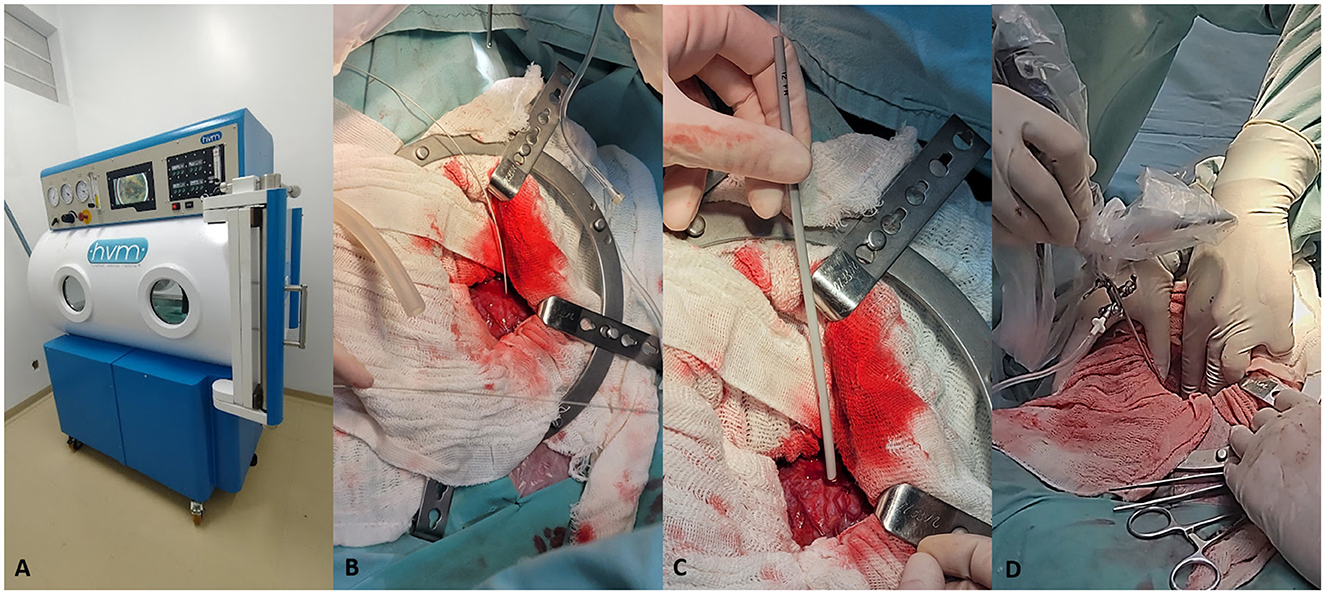
Figure 2. Hyperbaric oxygen therapy and bilateral nephroscopy performed in a dog with bilateral Dioctophyme renale. (A) Monoplace hyperbaric chamber (HVM™) during therapy at 2 ATA pressure. (B) Left kidney with guidewire positioned inside the kidney, after puncture with a 14G catheter. (C) Dilation of the orifice with an Amplatz-type 12 Fr renal dilator. (D) Nephroscopy with a 9.6 Fr rigid cystoscope and irrigation of the renal pelvis with sterile solution.
It then underwent a bilateral nephroscopy surgical procedure. Anesthesia induction was performed using ketamine (1 mg/kg), fentanyl (3 μg/kg), and propofol (5 mg/kg), IV. After orotracheal intubation and stabilization of the anesthetic plane, epidural anesthesia was performed with 0.5% bupivacaine (0.33 ml/kg) associated with morphine (0.1 mg/kg) and fentanyl (2 μg/kg). Ketamine (0.6 mg/kg/h) and dexmedetomidine (0.5 mg/kg/h) were administered in continuous infusion to reduce the minimum alveolar concentration (MAC) of the halogenated anesthetic (isoflurane) and provide analgesia. The patient was positioned in the supine position and the surgical site was prepared aseptically. Pre-umbilical celiotomy was performed and a wound retractor ring was placed. Diffuse reactivity was detected in the omentum, as well as the presence of a free 20-cm male parasite, close to the left kidney.
The left kidney showed hypertrophy and increased vascular pattern. It was punctured in the medial region with a 14 Fr catheter, until urine was obtained, and a hydrophilic guidewire was inserted (Figure 2B). Then, Amplatz-type renal dilators 10, 12, 14, and 16 Fr were used progressively (Figure 2C). Renal artery hemostasis was not performed and there was no relevant hemorrhage. Nephroscopy was performed with a 30-degree and 1.9–2.2 mm diameter telescope (Karl Storz™) positioned in a 9.6 Fr cystoscopy sheath. After the infusion of saline solution, a parasite was visualized that completely obstructed the ureter (Figure 2D). Cystoscopy grasping forceps and DeBakey atraumatic forceps were not sufficient for traction, and 5-mm laparoscopic Kelly forceps were used to remove a 33-cm female parasite (Figures 3A, B). The renal pelvis was inspected and cleaned. The 16 Fr hole (Figure 3C) was closed with a 3-0 polydioxanone suture in a horizontal mattress pattern.
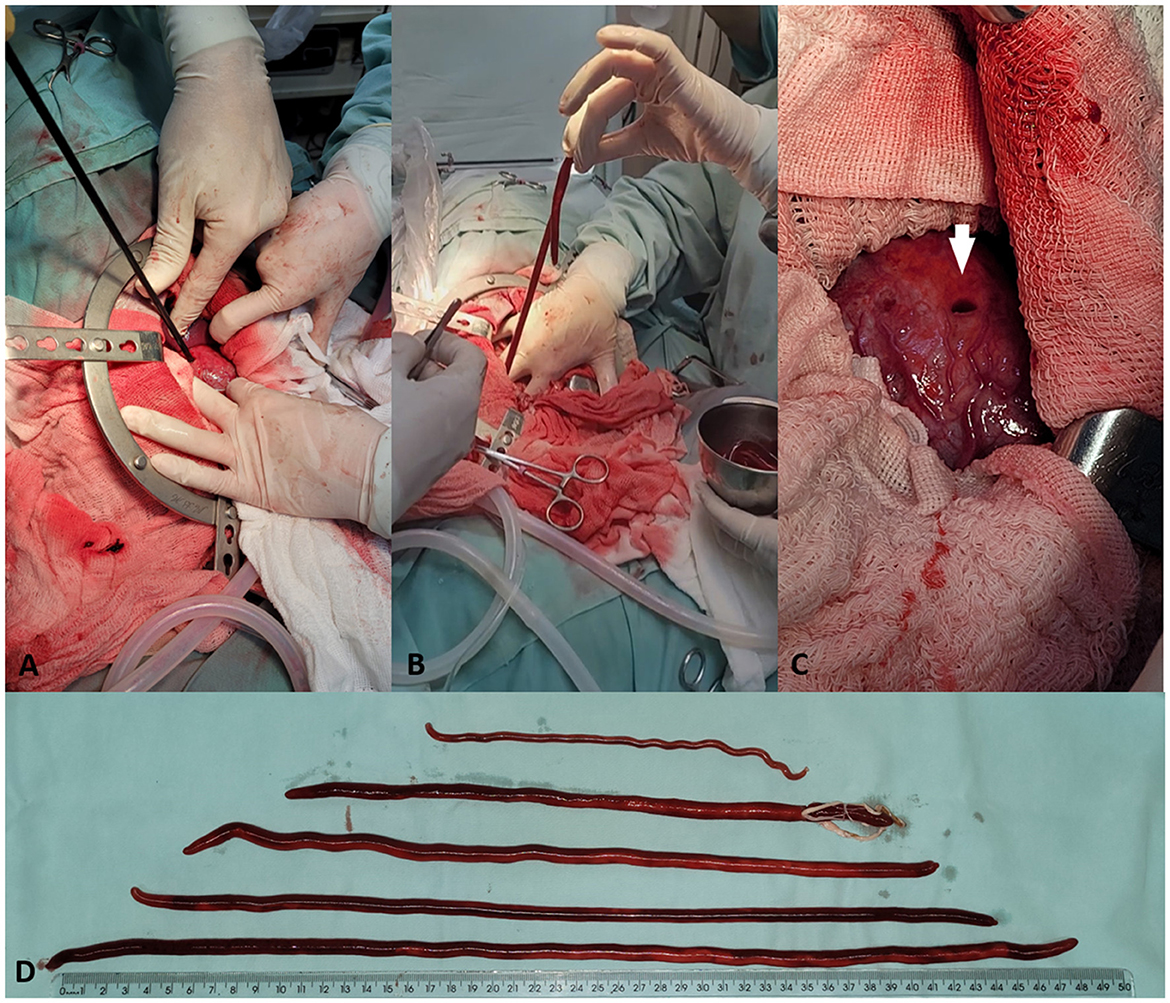
Figure 3. Bilateral nephroscopy to remove Dioctophyme renale in a dog. (A) Insertion of 5-mm laparoscopic Kelly forceps to capture the parasite. (B) Extraction of a female parasite removed from the inside of the right kidney. (C) Final appearance of the 16 Fr orifice (white arrow) through which the parasites were removed from the kidney interior. (D) One male (above) and five females of D. renale removed from a parasitized dog.
The right kidney had an altered conformation, smaller than the left kidney. The same access technique was used but there was difficulty in capturing the parasites because they were in the pelvic recesses. The same kind of laparoscopy forceps were used and one parasite was removed. On palpation it was suspected that there were more parasites, but the forceps did not reach any more. Reinspection and washing with a cystoscope advanced toward the cranial renal pole allowed more specimens to be found and two more females were removed. In total, the right kidney had three female parasites measuring 38, 42, and 50 cm (Figure 3D). Reinspection confirmed a parasite-free renal interior, which was irrigated with saline solution and sutured with the same technique used in the contralateral kidney.
On first inspection, the left kidney did not present the same interior image as the right kidney. Therefore, to ensure the removal of all parasites, the first renal suture was undone. The kidney was reevaluated to confirm the absence of parasites and sutured again. The abdominal cavity was irrigated with sterile solution and the two renal access points were omentalized. Routine three-layer closure of the incision was performed. Next, an esophageal feeding tube was placed.
Postoperative care consisted of analgesics, antimicrobials, antioxidants, gastric protector, and other medications to aid the patient's recovery. The medications used were as follows: methadone 0.3 mg/kg SC q6h for 24 h, followed by 0.2 mg/kg SC q6h for the following 24 h; tramadol 4 mg/kg IV q8h, started after methadone suspension and used for 3 days; dipyrone 25 mg/kg IV q8h for 7 days; cephalothin 30 mg/kg IV q8h for 5 days; maropitant citrate 1 mg/kg IV q24h for 4 days; omeprazole 1 mg/kg IV q12h for 4 days, later replaced by oral omeprazole, same dose, administered every 24 h for another 3 days; aluminum hydroxide 20 mg/kg, PO q12h for 7 days; probiotic paste 4 g/VO q24h; ferrous sulfate 120 mg/animal PO q24h for 7 days and omega-3 1,000 mg/animal PO q24h in continuous use.
Eighteen hours after the end of the surgical procedure, the HBOT sessions were resumed, using the protocol described previously, at 24-h intervals, totaling four postoperative sessions. Fluid therapy was performed with Ringer's lactate at a dose of 4 ml/kg/h during the first 24 h after surgery, during which time urine production was 2.8 ml/kg/h. Then, because the patient also received hydration via an esophageal tube, fluid therapy was reduced to a rate of 2 ml/kg/h and kept for 3 days. The animal was fed through an esophageal tube until it gradually started eating spontaneously, approximately on the fifth postoperative day.
Hematological and biochemical tests were performed daily and confirmed the rapid and satisfactory recovery from AKI. Serial abdominal ultrasounds confirmed the removal of all parasites and renal recovery. Figures 1A–F shows kidney size and the proportion of pelvic dilation in both kidneys. The measurements obtained were subjective because the kidney size exceeded the capacity of the ultrasound device to capture each organ in its entirety. A gradual bilateral reduction in the size and dilation of the renal pelvis was observed.
The severely parasitized right kidney measured 52.6 mm 7 days postoperatively, with loss of corticomedullary definition, irregular contours, and hyperechogenic heterogeneous parenchyma. There was slight dilation of the renal pelvis due to anechoic content (14.9 mm). The left kidney measured 82.6 mm, showed decreased corticomedullary definition due to diffuse increase in renal echogenicity and some hyperechogenic cortical striations, with preserved vascular flow in color Doppler mode. There was also slight dilation of the renal pelvis due to anechoic content (26 mm).
The patient presented normal physiological parameters for the species during the recovery period. With recovery, the medications and fluid therapy were reduced or discontinued. There was no bacterial growth in the urine sample collected directly from the kidneys. Clinical improvement was accompanied by normalization of behavior, including spontaneous water and food intake and active demeanor. The patient was discharged from hospital 7 days postoperatively, without an esophageal tube, with a prescription for kidney diet food, omega-3, and aluminum hydroxide. At this time, its condition was classified as stage 3 chronic kidney disease with proteinuria and prehypertension, according to IRIS (14).
The owner lives in a city far from the veterinary hospital (~290 km) where the animal was treated. Patient monitoring is carried out by a local nephrologist and by telephone. Reassessment 19 days postoperatively indicated mild anemia and increased creatinine. The patient continued to receive kidney food and omega-3 and was in excellent clinical condition 183 days after the surgical intervention.
Discussion
Here we describe the therapeutic success of the first nephroscopy performed for the treatment of bilateral dioctophymosis in a dog. Minimally invasive surgical procedures have several benefits in dogs. However, they are also associated with ischemia/reperfusion (I/R) injuries caused by pneumoperitoneum and longer surgical times (15). Conventional incisional nephrotomy can temporarily reduce 25–50% of renal function (16). The traditional abdominal surgical approach was chosen by the surgeons considering the severity of the case, the presence of bilateral disease, and the need for reduced surgical time. Nevertheless, nephron-sparing techniques were used, with minimal kidney damage. Petrovsky et al. (17) described the use of nephroscopy for nephrolithotomy in a very similar way, which also made it possible to inspect the renal pelvis and confirm its complete emptying (17).
The use of dilators to access the renal pelvis, instead of the nephrotomy incision, significantly reduced intraoperative bleeding. Therefore, warm ischemia (WI) was not used in both kidneys. Studies have described the performance of partial nephrectomy without WI, which reduces the deterioration of the glomerular filtration rate (18). Raheem et al. indicated that renal WI longer than 30 min was not associated with long-term chronic kidney disease in human patients with two kidneys (19). However, WI is associated with renal I/R injury (20, 21) and the patient in the present case had severe bilateral renal involvement and grade 5 AKI. This explains the choice of faster and less harmful methods.
On the other hand, the limited access resulted in difficulty in inspecting the renal pelvis. Also, there are no descriptions of images from similar nephroscopy procedures to show the appearance after removing the parasites. Therefore, the first suture on the left kidney was removed to allow for a reevaluation of the organ, due to concerns about residual parasites. This could have been avoided with the use of intraoperative imaging tests, such as ultrasound, which was not available.
HBOT is a therapy that consists of delivering 100% oxygen in a pressurized environment. It is associated with improved healing response, synergy with antibiotics, reduction of vasogenic edema and treatment of gas embolism (22). It is well-tolerated by dogs and cats and has been applied for various purposes (23–25). At the renal level, both preconditioning and hyperbaric therapies after I/R injury showed induction of renal tissue protection. There was an improvement in the glomerular filtration rate and a reduction in urea and creatinine levels in rats (20, 26–28). HBOT has already been used in dogs with D. renale and the results were promising (29). Although there are no experimental studies with dogs, from the authors' experience, the patient's rapid improvement was a result of the hyperbaric preconditioning process and treatment continuation, associated with the appropriate postoperative clinical management.
Unilateral parasitosis is not usually associated with surgical emergencies, as shown in a study with 52 nephrectomy procedures in dogs with D. renale (8). However, this was a case of extremely severe dioctophymosis in a dog. The rapid and sudden progression of kidney injury is of note, with a 10-fold increase in creatinine within 20 days. The authors believe the severe progression of the disease was partly caused by unilateral ureteral obstruction caused by the left kidney parasite, which was resolved with removal of the worm. The patient's treatment was delayed, as there was a 6-day interval between diagnosis and surgery, as a result of the distance between the city of origin and the veterinary hospital that was capable of performing a procedure of this complexity. This interval also explains the serious progression of AKI. There is no doubt that without proper intervention, the patient would have quickly died.
There is still no drug therapy proven to be effective in curing dioctophymosis. Even if there were, the parasite causes pressure atrophy and necrosis of the renal parenchyma, which are accompanied by tissue inflammation (30). Therefore, killing the parasite without removing it would not prevent further kidney damage. The authors highlight here the importance of rapid surgical intervention to remove the parasites.
The most similar case in the literature is described by Borrelli (10), in which a dog underwent right nephrectomy and left nephrotomy using a conventional surgical technique. The current literature does not provide reports of similar cases for comparison of postoperative ultrasound images. However, the authors consider the imaging evolution of both kidneys very positive. Comparative serial measurements between total renal size and areas of pelvic dilation showed a progressive increase in the parenchyma/pelvis proportion. Kidney size reduction, hydronephrosis, and inflammatory appearance, associated with the increase in the proportion of renal parenchyma subjectively indicates renal function improvement.
The results presented here in allow us to conclude that bilateral nephroscopy, not associated with warm ischemia, leads to the cure of bilateral renal dioctophymosis when part of the renal parenchyma is viable. HBOT plays an important role in protecting renal function against parasitic, surgical, and inflammatory injury. This report offers a new perspective on the treatment of bilateral renal parasitosis in dogs, thus dispelling the idea that the disease inevitably leads to the death of severely parasitized patients.
The procedures performed in this case were part of the necessary emergency clinical treatment for the patient. Therefore, approval from the Institutional Animal Care and Use Committee was not required. Written informed consent was obtained from the owners for the participation of their animals in this study.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Author contributions
PC: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. JG: Data curation, Investigation, Methodology, Writing – original draft. AH: Data curation, Investigation, Methodology, Writing – original draft. LA: Data curation, Formal analysis, Writing – original draft. RR: Visualization, Writing – original draft. LM: Data curation, Investigation, Methodology, Writing – original draft. DM: Funding acquisition, Project administration, Resources, Writing – review & editing. MB: Investigation, Resources, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was funded by Foundation for Support to Research of the State of Rio Grande do Sul (FAPERGS—Edital 07/2021 PqG), as well Brazilian National Council for Scientific and Technological Development (CNPq), Coordination for the Improvement of Higher Education Personnel (CAPES), and Hyperbaric Veterinary Medicine (HVM™).
Acknowledgments
The authors thank the Foundation for Support to Research of the State of Rio Grande do Sul (FAPERGS), National Council for Scientific and Technological Development (CNPq), the Coordination for the Improvement of Higher Education Personnel (CAPES), and the team at the University Veterinary Hospital of the Federal University of Santa Maria (HVU—UFSM). Also, the authors wish to thank HVM—Brasil for supporting this work through the concession of the veterinary hyperbaric chamber.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Caye P, Novo TST, Cavalcanti GAdO, Rappeti JCDS. Prevalência de Dioctophyme renale (Goeze, 1782) em cães de uma organização não governamental do sul do Rio Grande do Sul—Brasil. Arch Vet Sci. (2020) 25:46–55. doi: 10.5380/avs.v25i2.67468
2. Caye P, Aguiar ESVd, Andrades JdL, Neves KRd, Rondelli MCH, Braga FdVA, et al. Report of rare case of intense parasitism by 34 specimens of Dioctophyme renale in a dog. Rev Bras Parasitol Vet. (2020) 29:1–6. doi: 10.1590/s1984-29612020080
4. Pedrassani D, Nascimento AAd, André MR, Machado RZ. Dioctophyme renale: prevalence and risk factors of parasitism in dogs of São Cristóvão district, Três Barras county, Santa Catarina State, Brazil. Rev Bras Parasitol Vet. (2017) 26:39–46. doi: 10.1590/s1984-29612017004
5. Rahal SC, Mamprim MJ, Oliveira HS, Mosque LR, Faria LG, Takahira RK, et al. Ultrasonographic, computed tomographic, and operative findings in dogs infested with giant kidney worms (Dioctophyme renale). J Am Vet Med Assoc. (2014) 244:555–8. doi: 10.2460/javma.244.5.555
6. Sapin CDF, Silva-Mariano LC, Piovesan AD, Fernandes CG, Rappeti JCdS, Braga FDVA, et al. Anatomopathologic study of kidneys parasitized by Dioctophyme renale in dogs. Acta Vet Sci. (2017) 45:7. doi: 10.22456/1679-9216.79788
7. Eiras J, Zhu XQ, Yurlova N, Pedrassani D, Yoshikawa M, Nawa Y. Dioctophyme renale (Goeze, 1782) (Nematoda, Dioctophymidae) parasitic in mammals other than humans: a comprehensive review. Parasitol Int. (2021) 81:102269. doi: 10.1016/j.parint.2020.102269
8. Caye P, Rappeti JCdS, Perera SC, Segat HJ, Vives PS, Braga FdVA, et al. Nephrectomy in 52 dogs for the treatment of dioctophyme renal infection—knowing the enemy to win. Top Companion Anim Med. (2024) 58:100828. doi: 10.1016/j.tcam.2023.100828
9. Sapin CF, Silva-Mariano LC, Grecco-Correa L, Rappeti JCdS, Durante LH, Perera SC, et al. Bilateral and disseminated renal dioctophymatosis in dog. Pesq Vet Bras. (2017) 37:1499–504. doi: 10.1590/s0100-736x2017001200022
10. Borrelli S. Bilateral renal dioctophimosis—presentation of a clinical case. Veterinaria Cuyana. (2018) 13:39–46.
11. Li G, Liu C, Li F, Zhou M, Liu X, Niu Y. Fatal bilateral Dioctophymatosis. J Parasitol. (2010) 96:1152–4. doi: 10.1645/GE-2132.1
12. Milech V, Caye P, Nascimento Antunes B, Rappeti JCds, Carra Perera S, Gehrcke MI, et al. Laparoscopic nephron-sparing surgery for the treatment of canine dioctophymosis. J Vet Med Sci. (2022) 84:618. doi: 10.1292/jvms.21-0097
13. International Renal Interest Society. IRIS Grading of Acute Kidney Injury. (2023). Available online at: http://www.iris-kidney.com/guidelines/grading.html (accessed January 8, 2024).
14. International Renal Interest Society. IRIS Staging of CKD. (2023). Available online at: http://www.iris-kidney.com/guidelines/staging.html (accessed January 8, 2024).
15. Oliveira MT. Alterações inflamatórias na videocirurgia. In:Brun MV, , editor. Videocirurgia em Pequenos Animais. Rio de Janeiro: Roca (2015). p. 68–71.
17. Petrovsky B, Berent AC, Weisse CW, Branter E, Bagley DH, Lamb KE. Endoscopic nephrolithotomy for the removal of complicated nephroliths in dogs and cats: 16 kidneys in 12 patients (2005-2017). J Am Vet Med Assoc. (2019) 255:352–65. doi: 10.2460/javma.255.3.352
18. Mina-Riascos SH, Vitagliano G, García-Perdomo HA. Effectiveness and safety of partial nephrectomy-no ischemia vs. warm ischemia: systematic review and meta-analysis. Investig Clin Urol. (2020) 61:464–74. doi: 10.4111/icu.20190313
19. Raheem AA, Alowidah I, Capitanio U, Montorsi F, Larcher A, Derweesh I, et al. Warm ischemia time length during on-clamp partial nephrectomy: does it really matter? Minerva Urol Nephrol. (2022) 74:194–202. doi: 10.23736/S2724-6051.21.04466-9
20. Hentia C, Rizzato A, Camporesi E, Yang Z, Muntean DM, Săndesc D, et al. An overview of protective strategies against ischemia/reperfusion injury: the role of hyperbaric oxygen preconditioning. Brain Behav. (2018) 8:1–14. doi: 10.1002/brb3.959
21. He X, Xu X, Fan M, Chen X, Sun X, Luo G, et al. Preconditioning with hyperbaric oxygen induces tolerance against renal ischemia-reperfusion injury via increased expression of heme oxygenase-1. J Surg Res. (2011) 170:e271–7. doi: 10.1016/j.jss.2011.06.008
23. Birnie GL, Fry DR, Best MP. Safety and tolerability of hyperbaric oxygen therapy in cats and dogs. J Am Anim Hosp Assoc. (2018) 54:188–94. doi: 10.5326/JAAHA-MS-6548
24. Simpson AC, Wiener DJ. Positive effects of hyperbaric oxygen therapy in a cat with cutaneous nocardiosis. Vet Dermatol. (2021) 32:392–e112. doi: 10.1111/vde.12978
25. Latimer CR, Lux CN, Roberts S, Drum MG, Braswell C, Sula MJM. Effects of hyperbaric oxygen therapy on uncomplicated incisional and open wound healing in dogs. Vet Surg. (2018) 47:827–36. doi: 10.1111/vsu.12931
26. Solmazgul E, Uzun G, Cermik H, Atasoyu EM, Aydinoz S, Yildiz S. Hyperbaric oxygen therapy attenuates renal ischemia/reperfusion injury in rats. Urol Int. (2007) 78:82–5. doi: 10.1159/000096941
27. Ramalho RJ, de Oliveira PS, Cavaglieri RC, Silva C, Medeiros PR, Filho DM, et al. Hyperbaric oxygen therapy induces kidney protection in an ischemia/reperfusion model in rats. Transplant Proc. (2012) 44:2333–6. doi: 10.1016/j.transproceed.2012.07.020
28. Ilhan H, Eroglu M, Inal V, Eyi YE, Arziman I, Yildirim AO, et al. Hyperbaric oxygen therapy alleviates oxidative stress and tissue injury in renal ischemia/reperfusion injury in rats. Ren Fail. (2012) 34:1305–8. doi: 10.3109/0886022X.2012.723776
29. Caye P, Gasparotto JC, Antunes BN, Plentz ID, Hasan JA, Muller DCDM, et al. Hyperbaric oxygen therapy in bitches with dioctophymosis. Acta Vet Sci. (2023) 51:909. Available online at: https://seer.ufrgs.br/index.php/ActaScientiaeVeterinariae/article/view/131110
Keywords: dioctophymosis, Dioctophyme renale, giant kidney worm, nephroscopy, hyperbaric oxygen therapy
Citation: Caye P, Gasparotto JC, Hörbe AV, Andrade LRL, Reinstein RS, Mangini LT, Müller DCM and Brun MV (2024) Case report: Is bilateral renal dioctophymosis and severe uremia in a dog synonymous of euthanasia? Not today. Front. Vet. Sci. 11:1396467. doi: 10.3389/fvets.2024.1396467
Received: 05 March 2024; Accepted: 29 April 2024;
Published: 22 May 2024.
Edited by:
Hasan Tarık Atmaca, Balıkesir University, TürkiyeReviewed by:
Ankit Prajapati, Kamdhenu University, IndiaRicardo Lucena, Federal University of Paraíba, Brazil
Copyright © 2024 Caye, Gasparotto, Hörbe, Andrade, Reinstein, Mangini, Müller and Brun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pâmela Caye, pamiscaye@gmail.com