Comparison of radiological and clinical outcomes of 3D-printed artificial vertebral body with Titanium mesh cage in single-level anterior cervical corpectomy and fusion: A meta-analysis
 Haiyang Cheng1,2,†
Haiyang Cheng1,2,†  Gan Luo1,2,†
Gan Luo1,2,†  Dan Xu1
Dan Xu1  Yuqiao Li1,2 Ziqi Wang2,3 Houzhi Yang1,2 Yang Liu2 Yutao Jia2
Yuqiao Li1,2 Ziqi Wang2,3 Houzhi Yang1,2 Yang Liu2 Yutao Jia2  Tianwei Sun1,2*
Tianwei Sun1,2*
- 1Graduate School of Tianjin Medical University, Tianjin, China
- 2Department of Spinal Surgery, Tianjin Union Medical Center, Tianjin, China
- 3School of Medicine, Nankai University, Tianjin, China
Propose: This meta-analysis aimed to determine whether 3D-printed artificial vertebral body have superior clinical and radiographic outcome than Titanium Mesh Cage(TMC) in single-level anterior cervical corpectomy and fusion.
Methods: A comprehensive search of the PubMed, Embase, Cochrane Library, Web of Science, and CNKI (China National Knowledge Infrastructure) databases was conducted to find randomized control trials (RCTs) or cohort studies that compared 3D-printed artificial vertebral body with conventional Titanium Mesh Cage (TMC) in single-level anterior cervical corpectomy and fusion (SL-ACCF). Operation time; intraoperative blood loss; subsidence of vertebral body; preoperative, and final follow-up C2–C7 Cobb angle, Japanese Orthopedic Association (JOA) scores, and Visual Analog Scale(VAS) scores were collected from eligible studies for meta-analysis.
Results: We included 6 cohort studies with 341 patients. The results of the meta-analysis showed that the 3D group has a shorter operation time than the traditional TMC group(p = 0.04) and the TMC group had more severe subsidence(≥3 mm) of vertebral body than the 3D group(p < 0.0001). And the cervical C2–C7 Cobb angle in the 3D group was larger than that in the TMC group at the final follow-up.
Conclusion: This meta-analysis demonstrates that 3D-printed artificial vertebral body is superior to traditional TMC in reducing the operation time and maintaining the postoperative vertebral height and restoring sagittal balance to the cervical spine in single-level anterior cervical corpectomy and fusion.
Introduction
Recently, the incidence of cervical spondylotic myelopathy (CSM) is increasing (1, 2). Anterior Cervical Corpectomy and Fusion (ACCF) possesses the advantages of complete exposure and sufficient decompression, so it is extensively used in the treatment of a variety of cervical-related diseases (3–7). Autogenous iliac crest, fibula, allogeneic bone, and interbody fusion cages are often implanted in the cervical vertebral body to restore the stability of the anterior column. Autologous bone transplantation will not only extend the operation time, but also cause certain injury and complications (8–11). Titanium Mesh Cage(TMC) with autologous bone or hydroxyapatite artificial bone block has gradually become the most commonly used in ACCF implant materials (12), but TMC, while avoids donor site injury and complication, however, has some disadvantages, such as no close contact between bone and material interface and displacement and subsidence of the prosthesis (9, 13–15). Lu (16) et al. reported 3D-printed adaptive titanium mesh cage for the treatment of CSM and Ossification of the Posterior Longitudinal Ligament (OPLL), showing that 3D-printed artificial vertebral body has good clinical and imaging results in single-level anterior cervical corpectomy and fusion (SL-ACCF). However, due to the short clinical time of D-printed artificial vertebral body, there is a lack of high evidence-based medical evidence on efficacy and safety. This meta-analysis was designed to assess the clinical and radiographic outcomes of 3D-printed artificial vertebral body compared to Titanium Mesh Cage in single-level anterior cervical corpectomy and fusion.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (17) was used as guidance for our systematic review and meta-analysis.
Search strategy and study selection
Two investigators independently searched the following databases (inception to Oct 2022): PubMed, Embase, Cochrane Library, Web of Science, and CNKI (China National Knowledge Infrastructure) databases. The electronic search strategy used the following keywords: “Printing, Three-Dimensional”, “Titanium Mesh Cage”, and “anterior cervical corpectomy and fusion”. The search terms were adjusted according to the characteristics of each database, and we also examined the reference lists of the screened full-text studies to identify additional trials that might be eligible. And a third reviewer was consulted when the two reviewers could not reach a consensus.
Selection strategy
The inclusion and exclusion criteria for this study followed the PICOS principle. (1) Participants: Patients with Cervical Spondylotic Myelopathy (CSM) or Ossification of the Posterior Longitudinal Ligament (OPLL) or other cervical spondylosis, who need to be treated with single-level anterior cervical corpectomy and fusion (SL-ACCF). (2) Intervention and Comparison: In the operation procedure, the implant is the Titanium Mesh Cage (TMC) or the 3D-printed artificial vertebral body, and no implants other than Titanium Mesh Cage (TMC) or 3D-printed artificial vertebral body and titanium plates were used during the procedure. (3) Outcomes: The study should include at least one of the following data: Operation time, intraoperative blood loss, subsidence of vertebral body; preoperative, and final follow-up C2–C7 Cobb angle, Japanese Orthopedic Association (JOA) scores, or Visual Analog Scale (VAS) scores. (4) Study design: Observational studies and randomized control trials were eligible. Surgery with more than one level, case reports, case series, commentaries, practice guidelines, systematic reviews and meta-analysis were excluded. In addition, duplicate studies with the same cohort or studies considered by consensus to be of low quality were excluded.
Data extraction
Data were extracted from the included studies as follows: (1) study design: first author, publication region, publication time, and study type; (2) sample demographics: number of patients, age, sex, and disease diagnosis; (3) surgery details: Type of implants and their details, operation time, intraoperative blood loss; (4) analysis variables: Severe subsidence of vertebral body; operation time, intraoperative blood loss, preoperative, and final follow-up C2–C7 Cobb Angle, Japanese Orthopedic Association (JOA) scores, and Visual Analog Scale(VAS) scores.
Assessment of risk of bias
Two reviewers evaluated bias risk in the cohort studies using the Newcastle-Ottawa scale (18). Sensitivity analysis was performed by excluding a single study of each study in turn and reanalyzing the data. Publication bias was analyzed qualitatively by funnel plot.
Statistical analysis
The continuous variables were estimated by weighted mean difference (WMD), and dichotomous variables were estimated by using odds ratios (ORs) with 95% confidence intervals (CIs). The statistical heterogeneity of the pooled results was determined using the I² statistic. For this meta-analysis, we used the fixed-effect model when I² was greater than 50%, and if I²was less than 50%, a random-effect model was applied. The meta-analysis results were considered statistically significant when the p value < 0.05. The meta-analysis was performed using Review Manager 5.4 (Revman, The Cochrane Collaboration, Oxford, The UK).
Results
Search results
A total of 129 articles from PubMed, Web of science, the Cochrane Library, and CNKI were initially identified. The exact number of articles identified in each database is as follows: PubMed (n = 59), Web of Science (n = 39), the Cochrane library (n = 7), CNKI (n = 14). 48 articles were excluded because of duplication, and 73 studies were excluded by screening the titles and abstracts for: irrelevant studies, case reports, non-comparative studies and review articles. Leaving 7 articles that underwent a comprehensive full-text analysis. Finally, 6 studies (19–24) were included in the final meta-analysis. The flow chart used for the new systematic review according to PRISMA 2020 is shown in Figure 1.
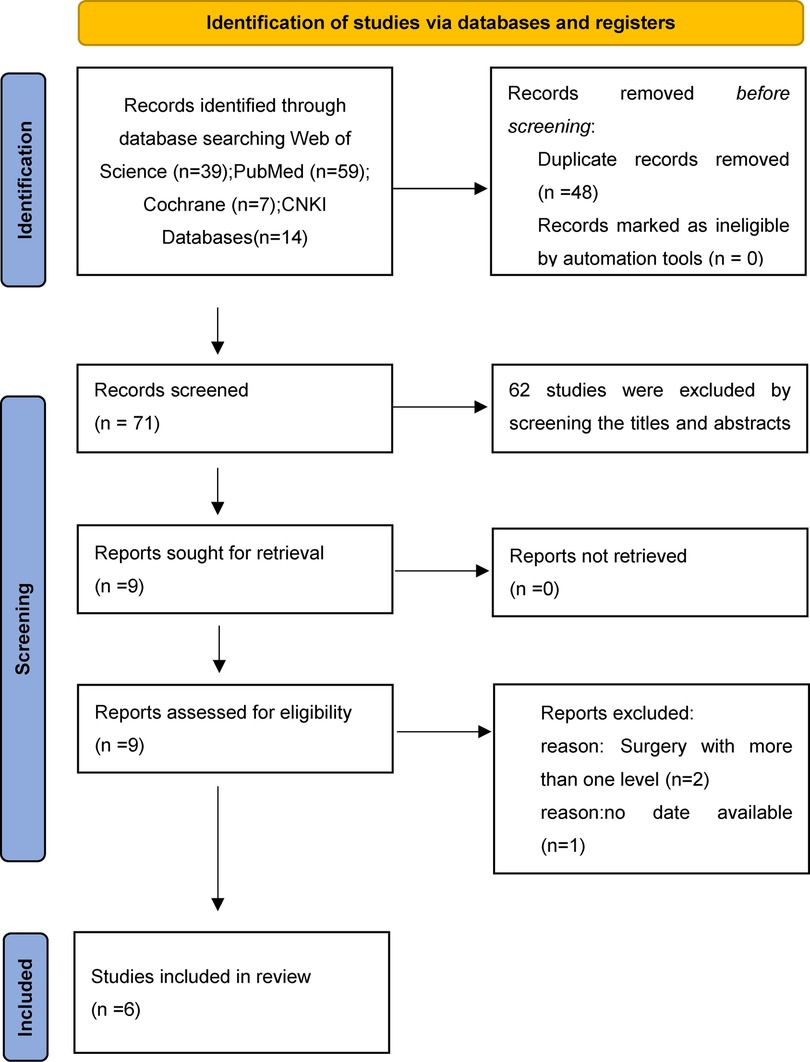
Figure 1. PRISMA flowchart.
Study characteristics and risk of bias
A total of 341 patients were enrolled in the 6 studies. The 3D-printed artificial vertebral body included 150 patients, and the TMC group included 164 patients. The characteristics of the included studies are presented in Table 1. The quality of included studies was evaluated according to the Newcastle-Ottawa scale, with scores above 7 (including 7) of high quality, and the evaluation results are shown in Table 2.
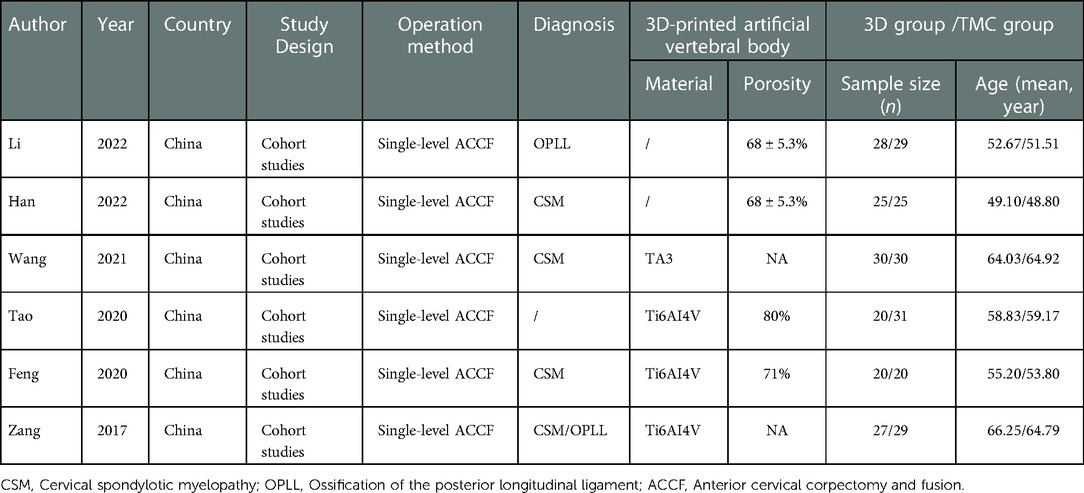
Table 1. Demographics and characteristics of included studies.
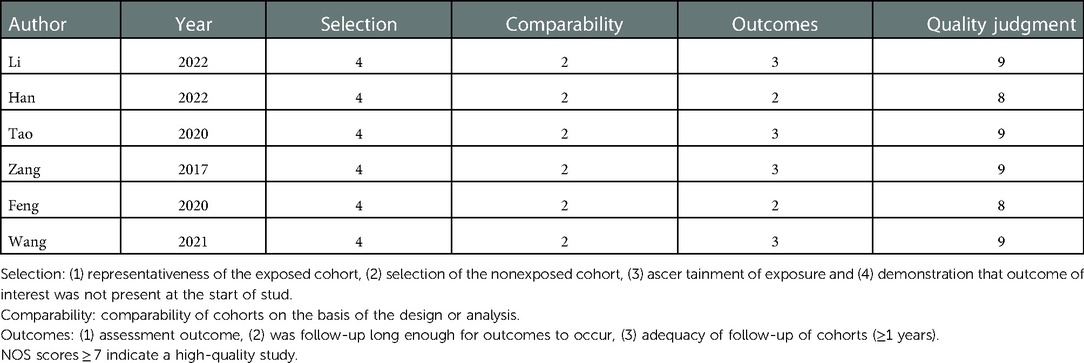
Table 2. Newcastle-Ottawa scale for observational studies.
Meta-Analysis results
Preoperative cervical C2–C7 Cobb angle, VAS scores and JOA scores
Preoperative evaluation indicators indicate the baseline level of patients before surgery, three studies (n = 141 patients; 65 in the 3D group and 76 in the TMC group) provided the preoperative cervical C2–C7 Cobb angle, three studies (n = 161 patients; 75 in the 3D group and 86 in the TMC group) offered Visual Analog Scale(VAS) scores and six studies(n = 314 patients; 150 in the 3D group and 164 in the TMC group) reported the preoperative Japanese Orthopedic Association (JOA) scores. No statistically significant difference was observed in the above indicators between the 3D group and TMC group, Combined effect value and heterogeneity test results: Preoperative cervical C2–C7 Cobb angle: P = 0.80, WMD −0.21 [−1.78, 1.36], Heterogeneity: Chi² = 0.75, df = 2 (P = 0.69); I² = 0%; Preoperative Visual Analog Scale(VAS) scores: P = 0.33, WMD −0.18 [−0.55, 0.18], Heterogeneity: Chi² = 0.86, df = 2 (P = 0.62); I² = 0%; and preoperative Japanese Orthopedic Association (JOA) scores: P = 0.95, WMD 0.01 [−0.32, 0.34], Heterogeneity: Chi² = 5.22, df = 5 (P = 0.39); I² = 4% [Figure 2]. which indicated that the included studies did not differ significantly between the 3D group and TMC group at baseline and that the observations were comparable.
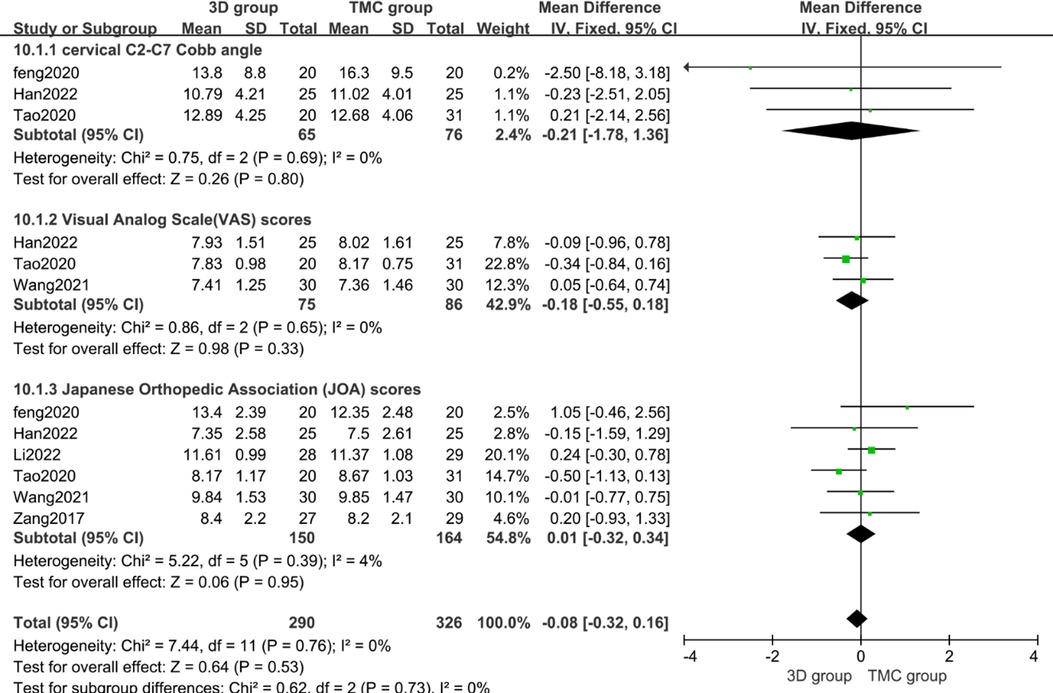
Figure 2. Weighted mean difference of preoperative cervical C2–C7 Cobb angle, Visual Analog Scale (VAS) scores, Japanese Orthopedic Association (JOA) scores between the 3D group and the TMC group. SD standard deviation, CI confidence interval, IV inverse variance.
Operation time and intraoperative blood loss
Operation time and intraoperative blood loss were used for evaluating the surgical trauma. Five studies (n = 274 patients; 130 in the 3D group and 144 in the TMC group) provided operation time and four studies (n = 223 patients; 110 in the 3D group and 113 in the TMC group) provided intraoperative blood loss. No statistically significant difference exists in intraoperative blood loss between the two groups (P = 0.65, WMD −0.59 [−3.10, 1.92], Heterogeneity: Tau² = 1.63; Chi² = 3.96, df = 3 (P = 0.27); I² = 24%) [Figure 3]. In contrary, the 3D group showed significantly shorter operation time compared with TMC group (p = 0.04, WMD −6.77 [−13.15, −0.40], Heterogeneity: Tau² = 44.12; Chi² = 39.94, df = 4 (P < 0.00001); I² = 90%) [Figure 4], It may indicate that 3D-printed artificial vertebral body can shorten the operation time compared with conventional Titanium Mesh Cage(TMC), but there is no significant difference in the amount of blood loss during surgery.

Figure 3. Weighted mean difference of intraoperative blood loss between the 3D group and the TMC group. SD standard deviation, CI confidence interval, IV inverse variance.
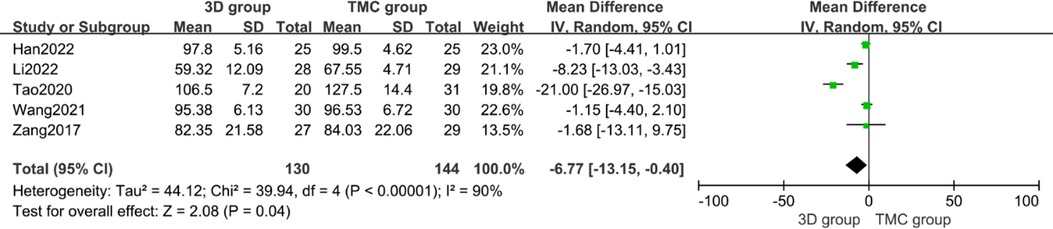
Figure 4. Weighted mean difference of operation time between the 3D group and the TMC group. SD standard deviation, CI confidence interval, IV inverse variance.
Severe subsidence of vertebral body
Vertebral subsidence was used to assess the ability of the implant to maintain vertebral height. All included articles defined severe subsidence as a decrease of more than 3 mm in the height of the fused segment during the follow-up period after surgery compared with that immediately after surgery (25, 26). A total of 5 studies reported the severe subsidence of vertebral body (n = 254 patients; 120 in the 3D group and 134 in the TMC group). Statistically significant difference was observed in 3D group and TMC group (p < 0.0001, OR = 0.12 [0.05, 0.32], Heterogeneity: Chi² = 1.59, df = 4 (P = 0.81); I² = 0%) [Figure 5]. The incidence of severe subsidence of vertebral body in the 3D group was significantly lower than that in the TMC group, indicating that 3D-printed artificial vertebral body performed significantly better than traditional TMC in maintaining vertebral body height after operation.
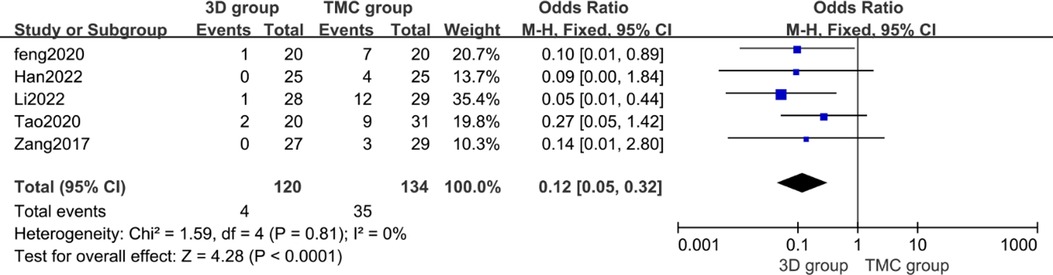
Figure 5. Odds ratio of severe subsidence of vertebral body between the 3D group and the TMC group. CI confidence interval, M-H Mantel-Haenszel.
Final follow-up VAS scores and JOA scores
The last follow-up time was defined as 1 year after surgery for all included studies. There studies (n = 161 patients; 75 in the 3D group and 86 in the TMC group) provided final follow-up VAS scores and four studies (n = 274 patients; 130 in the 3D group and 144 in the TMC group) reported the final follow-up JOA scores. There was no statistically significant difference between the two groups regarding final follow-up VAS scores (P = 0.98, WMD = −0.42 [−0.91, 0.06], Heterogeneity: Tau² = 0.10; Chi² = 4.71, df = 2 (P = 0.09); I² = 58%) [Figure 6] and final follow-up JOA scores (P = 0.16, WMD = 0.64 [−0.25, 1.54], Heterogeneity: Tau² = 0.84; Chi² = 30.11, df = 4 (P < 0.00001); I² = 87%) [Figure 7]. Although Japanese Orthopedic Association (JOA) scores and Visual Analog Scale (VAS) scores improved in the last follow-up in each study compared with preoperative assessment, there was no significant difference in the improvement between the two groups.

Figure 6. Weighted mean difference of final follow-up Visual Analog Scale (VAS) scores between the 3D group and the TMC group. SD standard deviation, CI confidence interval, IV inverse variance.
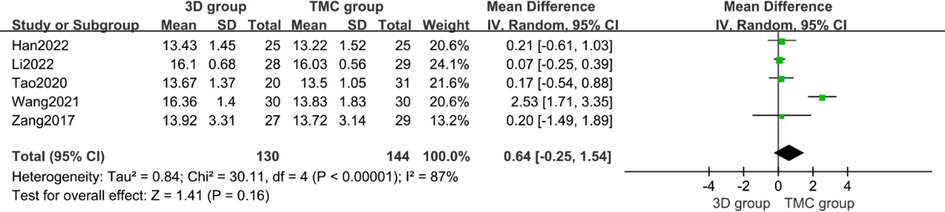
Figure 7. Weighted mean difference of final follow-up Japanese Orthopedic Association (JOA) scores between the 3D group and the TMC group. SD standard deviation, CI confidence interval, IV inverse variance.
Final follow-up cervical C2–C7 Cobb angle
Similarly, the last follow-up time in the included studies was 1 year after surgery. Two studies (n = 101 patients; 45 in the 3D group and 56 in the TMC group) provided the final follow-up cervical C2–C7 Cobb angle. There was statistically significant difference in cervical C2–C7 Cobb angle between the 3D group and TMC group at final follow-up cervical C2–C7 Cobb angle (P < 0.0001,WMD 5.88 [3.04, 8.73], Heterogeneity: Tau² = 2.93; Chi² = 3.10, df = 1 (P = 0.08); I² = 68%) [Figure 8], The results showed that the cervical C2–C7 Cobb angle in the 3D group was larger than that in the TMC group at the final follow-up.

Figure 8. Weighted mean difference of final follow-up cervical C2–C7 Cobb angle between the 3D group and the TMC group. SD standard deviation, CI confidence interval, IV inverse variance.
Heterogeneity and sensitivity analysis
The results of this analysis showed that the heterogeneity of the operation time, final follow-up VAS scores, JOA scores and cervical C2–C7 Cobb angle was high. A random-effect model was used to partially eliminate the effect of heterogeneity, but the results showed that the heterogeneity was still high. After removing one of the included studies for each index (final follow-up VAS scores, JOA scores and cervical C2–C7 Cobb angle), we found that heterogeneity did not decrease significantly, but it did not affect the results, this shows that the results of this meta-analysis are relatively reliable. When it comes to operation time, when we removed each included article separately, the combined effect value shows a significant change or even no significance. Therefore, the conclusion that the 3D group had a shorter operation time than the TMC group is not reliable, and the large heterogeneity may come from the technical level of the surgeons.
Bias analysis
Funnel plots were constructed to assess publication bias, and the results were largely symmetrical, indicating acceptable publication bias in our analysis. However, the distribution of JOA scores was significantly asymmetric at the last follow-up, suggesting that publication bias is likely (Figures 9–15).
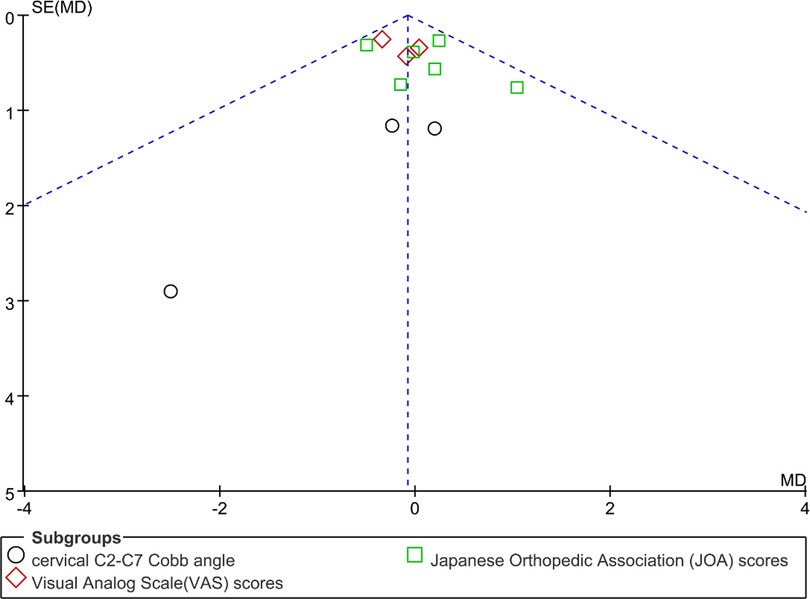
Figure 9. Funnel plot of preoperative cervical C2–C7 Cobb angle, Visual Analog Scale (VAS) scores, Japanese Orthopedic Association (JOA) scores.
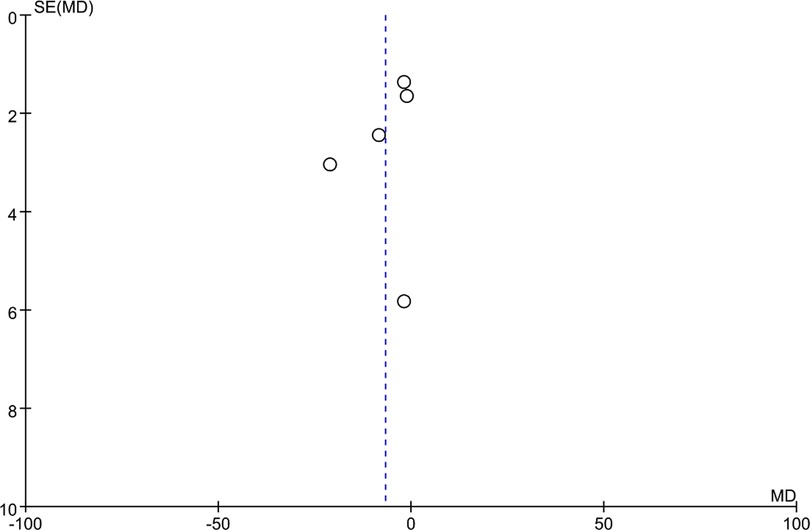
Figure 10. Funnel plot of operation time.
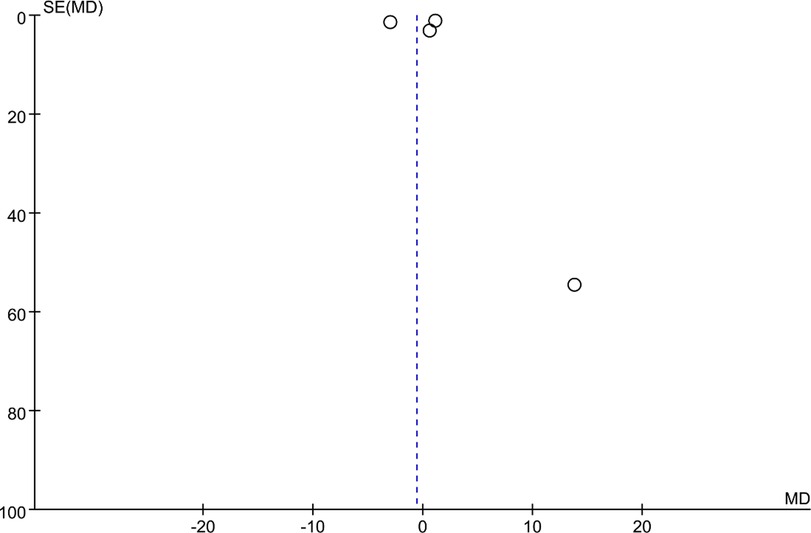
Figure 11. Funnel plot of intraoperative blood loss.
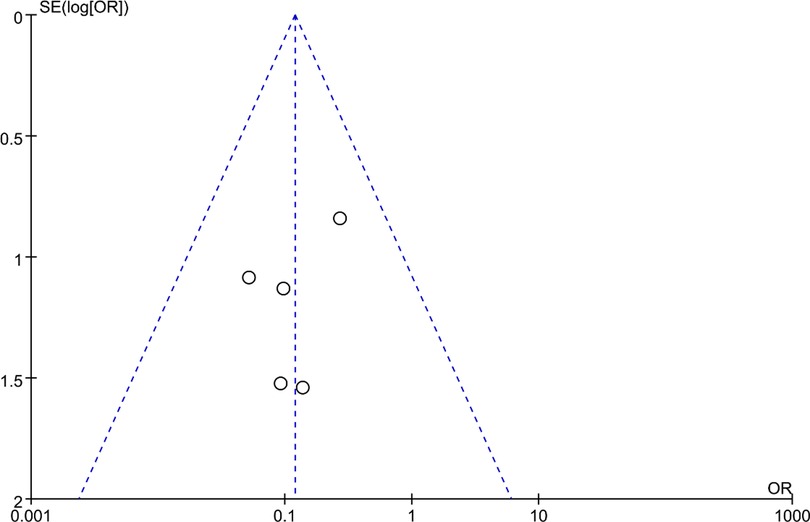
Figure 12. Funnel plot of severe subsidence of vertebral body.
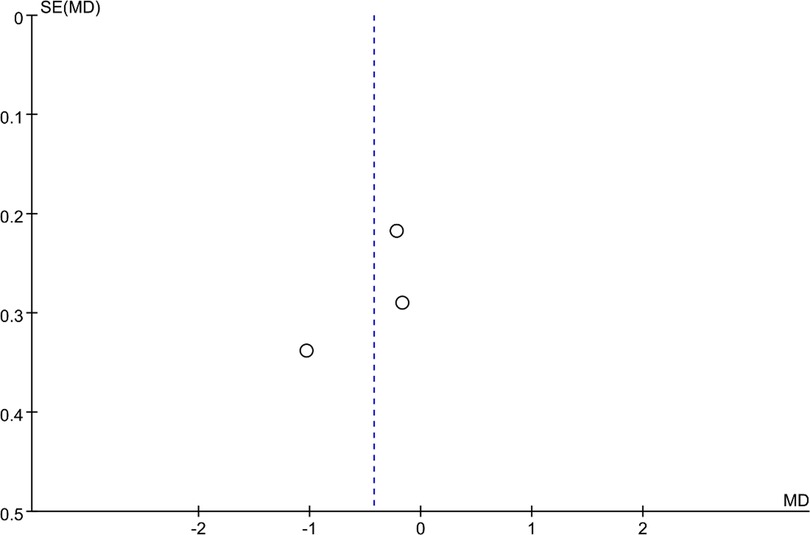
Figure 13. Funnel plot of final follow-up Visual Analog Scale (VAS) scores.
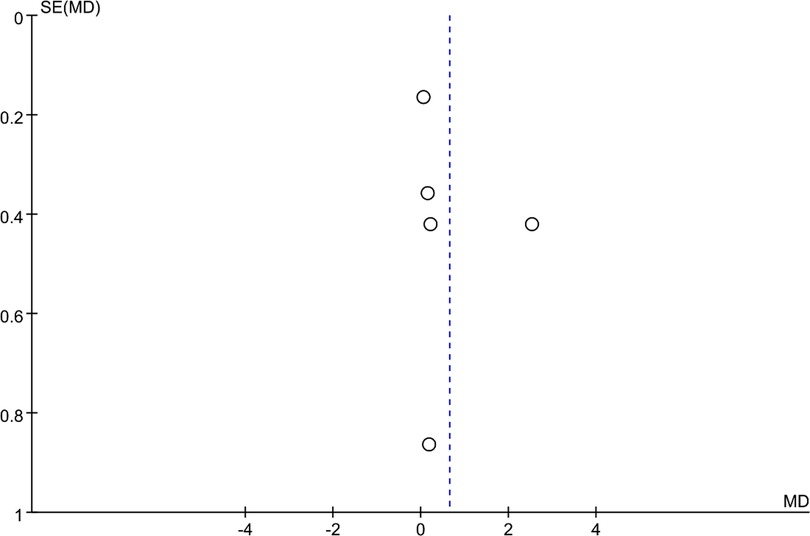
Figure 14. Funnel plot of final follow-up Japanese Orthopedic Association (JOA) scores.
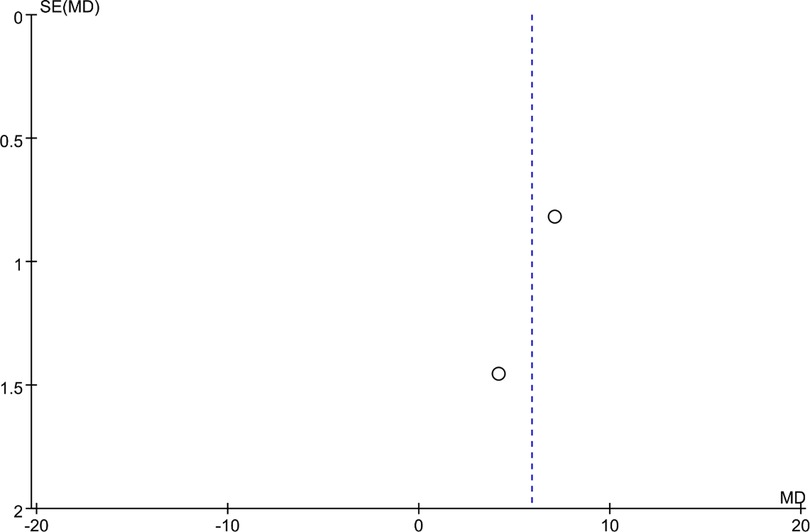
Figure 15. Funnel plot of final follow-up cervical C2–C7 Cobb angle.
Discussion
Anterior cervical corpectomy and fusion(ACCF) is a common surgical method to treat cervical-related diseases (5, 10), Spinal surgeons are always looking for a more efficient and more secure implants and Titanium Mesh Cage(TMC) has gradually replaced autologous bone graft and become mainstream (15, 27, 28), the emergence of Three-dimensional printing technology provides a brand-new choice of fusion implant (29), However, at present, there is no large-scale research to prove whether 3D printed artificial vertebral body is more safe and effective than traditional TMC. In this paper, six cohort studies were included to analyze the efficacy and safety of 3D-printed artificial vertebral body in single-level anterior cervical corpectomy and fusion(SL-ACCF), and the results show that 3D printing artificial vertebral body is superior to traditional TMC in shortening the operation time, reducing the occurrence of Severe subsidence of vertebral body and restoring C2–C7 Cobb Angle, but there is no significant difference in Japanese Orthopedic Association (JOA) scores, Visual Analog Scale (VAS) scores and reducing intraoperative blood loss.
During the traditional operation, the operator repeatedly tried to select a suitable interbody fusion cage, it increases the risk of fracture of steel plate that is too large, and loosening and displacement are easy to occur when it is too small, thus increasing the operation time (30). While the 3D-printed artificial vertebral body has been modeled by the CT or MRI spiral scanner of the whole vertebral body, and the final height of the vertebral body of the fusion cage is almost the same as the anatomical height of the patient, thus avoiding the repeated selection of the appropriate interbody fusion cage and shortening the operation time (31).
After the surgery, vertebral body height and cervical sagittal balance has always been the focus of clinical doctors, traditional TMC is easy to decrease the height of vertebral body after operation, especially when TMC subsides, it is easy to decrease the height of intervertebral foramen and the number of wrinkles of posterior longitudinal ligament, which leads to the symptoms of nerve and spinal cord compression (9, 32, 33). The main reason for these situations is that the elastic modulus of the TMC is inconsistent with that of normal human bones, resulting in stress shielding. The 3D-printed artificial vertebral body with upper dome structure and lower inclination Angle designed by Lu (16) et al. can increase the contact area with the upper and lower vertebral bodies, reducing the concentrated stress and the drop of vertebral body height. Studies have shown that the porosity of the implant should be controlled between 60% and 80% to balance the elastic modulus and compression strength of the prosthesis. Rapuano (34) et al. confirmed that cells spread well on the surface of porous titanium alloy, and the micro-rough structure was beneficial to the aggregation and growth of bone cells in vitro and Olivares-Navarrete (35) et al. also found that the design of porous rough titanium alloy can create an osteogenic environment containing bone morphogenetic protein 2(BMP2), BMP4 and BMP7, promote the differentiation and maturation of osteoblasts (36), and facilitate the earlier completion of osseous fusion and the stability of implants (19). Cervical C2–C7 Cobb Angle is an important metric to measure the sagittal balance of the cervical spine. Also, due to the rational structure of the upper and lower ends of the 3D-printed artificial vertebral body, reasonable porous design, elastic modulus to that of normal bone, and providing a microenvironment for the growth of bone cells, the cervical C2–C7 Cobb Angle outperforms better than that of the titanium cage. This study also confirmed the advantages of 3D-printed vertebral body in reconstruction of the anterior column and restoring the sagittal balance of the cervical spine.
Limitations
First of all, there were no randomized controlled trials in all the included studies, but no serious bias was found in the published bias test [Figures 9–15]. Second, there are differences in the 3D printed implants used in most studies, such as porosity, upper and lower structures, etc. There is a high degree of heterogeneity among the various studies, such as the operation time, but after excluding each study sequentially, the recalculated pooled results did not significantly change, indicating that there was no outlying study that significantly influenced the overall results. All the articles included are from China, and most of the samples are Asian, so they are not well represented. Only 6 articles were included, and the sample size is small, so a large number of randomized controlled trials with long follow-up times are needed to complement the conclusions.
Conclusion
This meta-analysis demonstrated that 3D-printed artificial vertebral body is superior to traditional TMC in reducing the operation time and maintaining the postoperative vertebral height and restoring sagittal balance of cervical spine in single-level anterior cervical corpectomy and fusion.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
HYC and TWS conducted research design and data collection. HYC and GL conducted data analysis. DX and ZQW interpreted the results. The first draft of the manuscript was written by HYC, and GL reviewed and corrected the manuscript. All authors read and approved the final manuscript. All authors contributed to the article and approved the submitted version.
Funding
This research was funded by Tianjin Key Medical Discipline(Specialty) Construction Project, grant number TJYXZDXK-064B; Tianjin Health Research Project, grant number TJWJ2022MS018; Tianjin municipal Health Commission, grant number 2021180.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fernandez-Moure J, Moore CA, Kim K, Karim A, Smith K, Barbosa Z, et al. Novel therapeutic strategies for degenerative disc disease: review of cell biology and intervertebral disc cell therapy. SAGE Open Med. (2018) 6:2050312118761674. doi: 10.1177/2050312118761674
2. McCormick JR, Sama AJ, Schiller NC, Butler AJ, Donnally CJ 3rd. Cervical spondylotic myelopathy: a guide to diagnosis and management. J Am Board Fam Med. (2020) 33:303–13. doi: 10.3122/jabfm.2020.02.190195
3. Iwasaki M, Okuda S, Miyauchi A, Sakaura H, Mukai Y, Yonenobu K, et al. Surgical strategy for cervical myelopathy due to ossification of the posterior longitudinal ligament: part 2: advantages of anterior decompression and fusion over laminoplasty. Spine (Phila Pa 1976). (2007) 32:654–60. doi: 10.1097/01.brs.0000257566.91177.cb
4. Majd ME, Vadhva M, Holt RT. Anterior cervical reconstruction using titanium cages with anterior plating. Spine (Phila Pa 1976). (1999) 24:1604–10. doi: 10.1097/00007632-199908010-00016
5. Odate S, Shikata J, Kimura H, Yamamura S. Anterior corpectomy with fusion in combination with an anterior cervical plate in the management of ossification of the posterior longitudinal ligament. J Spinal Disord Tech. (2012) 25:133–7. doi: 10.1097/BSD.0b013e318211fc35
6. Qiu X, Zhao B, He X, Zhao C, Leng Z. Interface fixation using absorbable screws versus plate fixation in anterior cervical corpectomy and fusion for two-level cervical spondylotic myelopathy. Med Sci Monit. (2020) 26:e921507. doi: 10.12659/MSM.921507
7. Zhang Y, Liu H, Yang H, Pi B. Anterior cervical corpectomy and fusion versus discectomy and fusion for the treatment of two-level cervical spondylotic myelopathy: analysis of sagittal balance and axial symptoms. Int Orthop. (2018) 42:1877–82. doi: 10.1007/s00264-018-3804-3
8. Malloy KM, Hilibrand AS. Autograft versus allograft in degenerative cervical disease. Clin Orthop Relat Res. (2002) 394:27–38. doi: 10.1097/00003086-200201000-00004
9. Fengbin Y, Jinhao M, Xinyuan L, Xinwei W, Yu C, Deyu C. Evaluation of a new type of titanium mesh cage versus the traditional titanium mesh cage for single-level, anterior cervical corpectomy and fusion. Eur Spine J. (2013) 22:2891–6. doi: 10.1007/s00586-013-2976-1
10. Wen Z, Lu T, Wang Y, Liang H, Gao Z, He X. Anterior cervical corpectomy and fusion and anterior cervical discectomy and fusion using titanium mesh cages for treatment of degenerative cervical pathologies: a literature review. Med Sci Monit. (2018) 24:6398–404. doi: 10.12659/MSM.910269
11. Emery SE, Bohlman HH, Bolesta MJ, Jones PK. Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy. Two to seventeen-year follow-up. J Bone Joint Surg Am. (1998) 80:941–51. doi: 10.2106/00004623-199807000-00002
12. Zeng J, Duan Y, Yang Y, Wang B, Hong Y, Lou J, et al. Anterior corpectomy and reconstruction using dynamic cervical plate and titanium mesh cage for cervical spondylotic myelopathy: a minimum 5-year follow-up study. Medicine (Baltimore). (2018) 97:e9724. doi: 10.1097/MD.0000000000009724
13. Mohammad-Shahi MH, Nikolaou VS, Giannitsios D, Ouellet J, Jarzem PF. The effect of angular mismatch between vertebral endplate and vertebral body replacement endplate on implant subsidence. J Spinal Disord Tech. (2013) 26:268–73. doi: 10.1097/BSD.0b013e3182425eab
14. Li Z, Guo Z, Hou S, Zhao Y, Zhong H, Yu S, et al. Segmental anterior cervical corpectomy and fusion with preservation of middle vertebrae in the surgical management of 4-level cervical spondylotic myelopathy. Eur Spine J. (2014) 23:1472–9. doi: 10.1007/s00586-014-3208-z
15. Ji C, Yu S, Yan N, Wang J, Hou F, Hou T, et al. Risk factors for subsidence of titanium mesh cage following single-level anterior cervical corpectomy and fusion. BMC Musculoskelet Disord. (2020) 21:32. doi: 10.1186/s12891-019-3036-8
16. Lu T, Liu C, Yang B, Liu J, Zhang F, Wang D, et al. Single-level anterior cervical corpectomy and fusion using a new 3D-printed anatomy-adaptive Titanium mesh cage for treatment of cervical spondylotic myelopathy and ossification of the posterior longitudinal ligament: a retrospective case series study. Med Sci Monit. (2017) 23:3105–14. doi: 10.12659/msm.901993
17. Parums DV. Editorial: review articles, systematic reviews, meta-analysis, and the updated preferred reporting items for systematic reviews and meta-analyses (PRISMA) 2020 guidelines. Med Sci Monit. (2021) 27:e934475. doi: 10.12659/MSM.934475
18. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–5. doi: 10.1007/s10654-010-9491-z
19. Fang T, Zhang M, Yan J, Zhao J, Pan W, Wang X, et al. Comparative analysis of 3D-printed artificial vertebral body versus Titanium mesh cage in repairing bone defects following single-level anterior cervical corpectomy and fusion. Med Sci Monit. (2021) 27:e928022. doi: 10.12659/MSM.928022
20. Wei F, Xu N, Li Z, Cai H, Zhou F, Yang J, et al. A prospective randomized cohort study on 3D-printed artificial vertebral body in single-level anterior cervical corpectomy for cervical spondylotic myelopathy. Ann Transl Med. (2020) 8:1070. doi: 10.21037/atm-19-4719
21. Yuwei L, Haijiao W, Wei C, Bingtao H, Fan L, Tiantian Y. Clinical efficacy of 3D printed microporous titanium artificial vertebral body intreatment of ossification of cervical posterior longitudinal ligament. J Army Med Univ. (2022) 44:1542–8. doi: 10.16016/j.2097-0927.202112124
22. Shuhong H, Jiahua W, He S. Comparative study on the effects of 3D-printed artificial vertebral body and titanium cage in anterior cervical corpectomy and fusion surgery. Chin J Spine Spinal Cord. (2022) 32:426–33. doi: 10.3969/j.issn.1004-406X.2022.05.07
23. Quan-jin Z, Teng L, Hui L, Wen-long Y, Ping-lin Y, Hao-peng L, et al. Comparative study of a new 3D anatomical titanium cage and traditional titanium cage in anterior cervical corpectomy and fixation. Chin J Bone Joint Inj. (2017) 32:673–6. doi: 10.7531/j.issn.1672-9935.2017.07.001
24. Jiahua W, Di W, He S, Yilong Z, Lili X, Renzan Z. The effect of 3D printing artificial vertebral body assisted anterior cervical corpectomy and fusion on prosthesis sedimentation rate and stress response in patients with cervical spondylotic myelopathy. Chin J Gerontol. (2021) 41:5561–4. doi: 10.3969/j.issn.1005-9202.2021.24.025
25. Chen Y, Chen D, Guo Y, Wang X, Lu X, He Z, et al. Subsidence of titanium mesh cage: a study based on 300 cases. J Spinal Disord Tech. (2008) 21:489–92. doi: 10.1097/BSD.0b013e318158de22
26. van Jonbergen HP, Spruit M, Anderson PG, Pavlov PW. Anterior cervical interbody fusion with a titanium box cage: early radiological assessment of fusion and subsidence. Spine J. (2005) 5:645–9. discussion 649. doi: 10.1016/j.spinee.2005.07.007
27. Zhong W, Liang X, Tang K, Luo X, Quan Z, Jiang D. Nanohydroxyapatite/polyamide 66 strut subsidence after one-level corpectomy: underlying mechanism and effect on cervical neurological function. Sci Rep. (2018) 8:12098. doi: 10.1038/s41598-018-30678-1
28. Burkett CJ, Baaj AA, Dakwar E, Uribe JS. Use of titanium expandable vertebral cages in cervical corpectomy. J Clin Neurosci. (2012) 19:402–5. doi: 10.1016/j.jocn.2011.07.030
29. Li S, Huan Y, Zhu B, Chen H, Tang M, Yan Y, et al. Research progress on the biological modifications of implant materials in 3D printed intervertebral fusion cages. J Mater Sci. (2021) 33:2. doi: 10.1007/s10856-021-06609-4
30. Zhou E, Huang H, Zhao Y, Wang L, Fan Y. The effects of titanium mesh cage size on the biomechanical responses of cervical spine after anterior cervical corpectomy and fusion: a finite element study. Clin Biomechan. (2022) 91:105547. doi: 10.1016/j.clinbiomech.2021.105547
31. Jin YZ, Zhao B, Lu XD, Zhao YB, Zhao XF, Wang XN, et al. Mid- and long-term follow-up efficacy analysis of 3D-printed interbody fusion cages for anterior cervical discectomy and fusion. Orthop Surg. (2021) 13:1969–78. doi: 10.1111/os.13005
32. Kabir SM, Alabi J, Rezajooi K, Casey AT. Anterior cervical corpectomy: review and comparison of results using titanium mesh cages and carbon fibre reinforced polymer cages. Br J Neurosurg. (2010) 24:542–6. doi: 10.3109/02688697.2010.503819
33. Zhou J, Li X, Zhou X, Lin H, Dong J. Anterior decompression and hybrid reconstruction with titanium mesh cage plus plate and self-locking stand-alone cage for the treatment of three-level cervical spondylotic myelopathy. J Clin Neurosci. (2017) 43:196–201. doi: 10.1016/j.jocn.2017.04.022
34. Rapuano BE, Lee JJ, MacDonald DE. Titanium alloy surface oxide modulates the conformation of adsorbed fibronectin to enhance its binding to α(5) β(1) integrins in osteoblasts. Eur J Oral Sci. (2012) 120:185–94. doi: 10.1111/j.1600-0722.2012.954.x
35. Olivares-Navarrete R, Gittens RA, Schneider JM, Hyzy SL, Haithcock DA, Ullrich PF, et al. Osteoblasts exhibit a more differentiated phenotype and increased bone morphogenetic protein production on titanium alloy substrates than on poly-ether-ether-ketone. Spine J. (2012) 12:265–72. doi: 10.1016/j.spinee.2012.02.002
Keywords: 3D-printed artificial vertebral body, anterior cervical corpectomy and fusion, titanium mesh cage, C2–C7 cobb angle, visual analog scale (VAS) scores, Japanese orthopedic association (JOA) scores, meta-analysis
Citation: Cheng H, Luo G, Xu D, Li Y, Wang Z, Yang H, Liu Y, Jia Y and Sun T (2023) Comparison of radiological and clinical outcomes of 3D-printed artificial vertebral body with Titanium mesh cage in single-level anterior cervical corpectomy and fusion: A meta-analysis. Front. Surg. 9:1077551. doi: 10.3389/fsurg.2022.1077551
Received: 23 October 2022; Accepted: 27 December 2022;
Published: 11 January 2023.
Edited by:
Harvinder Singh Chhabra, Indian Spinal Injuries Centre, IndiaReviewed by:
Liangbin Gao, Sun Yat-sen Memorial Hospital, ChinaEdvin Zekaj, Galeazzi Orthopedic Institute (IRCCS), Italy
© 2023 Cheng, Luo, Xu, Li, Wang, Yang, Liu, Jia and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tianwei Sun billsuntw@163.com
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Orthopedic Surgery, a section of the journal Frontiers in Surgery