 Meiheng Liu
Meiheng Liu Leiyu Shi2
Leiyu Shi2 Manfei Yang
Manfei Yang Junyan Yang
Junyan Yang Gang Sun
Gang Sun- 1Department of Health Management, School of Health Management, Southern Medical University, Guangzhou, China
- 2Department of Health Policy and Management, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, United States
Objective: The purpose of this study is to provide experience and evidence support for countries to deal with similar public health emergencies such as COVID-19 by comparing and analyzing the measures taken by six countries in epidemic prevention and control.
Methods: This study extracted public data on COVID-19 from the official website of various countries and used ecological comparative research methods to compare the specific situation of indicators such as daily tests per thousand people, stringency index, and total vaccinations per hundred people in countries.
Results: The cumulative death toll in China, Germany and Australia was significantly lower than that in the United States, South Africa and Italy. Expanding the scale of testing has helped control the spread of the epidemic to some extent. When the epidemic situation is severe, the stringency index increases, and when the epidemic situation tends to ease, the stringency index decreases. Increased vaccination rates, while helping to build an immune barrier, still need to be used in conjunction with non-drug interventions.
Conclusion: The implementation of non-drug interventions and vaccine measures greatly affected the epidemic prevention and control effect. In responding to public health emergencies such as the COVID-19 epidemic, countries should draw on international experience, closely align with their national conditions, follow the laws of epidemiology, actively take non-drug intervention measures, and vigorously promote vaccine research and development and vaccination.
1 Introduction
Since December 2019, a number of cases of pneumonia of unknown cause with a history of exposure to seafood markets in South China have been found in some hospitals in Hubei Province, China, which have been confirmed as acute respiratory infectious diseases caused by novel coronavirus infection. The outbreak has since rapidly spread around the world. The initial genome sequencing data of the virus did not match that of previously sequenced coronaviruses (1). On 30 January 2020, the World Health Organization declared the COVID-19 outbreak a public health emergency of international concern. The COVID-19 epidemic is characterized by high prevalence and long incubation period. According to official reports, as of December 31, 2022, the cumulative number of confirmed cases worldwide exceeded 700 million and the cumulative death toll exceeded 6.7 million (2). Due to the emergence of the mutated strain, countries have limited epidemic prevention and control measures, and the epidemic has rebounded several times, posing a serious threat to human life and seriously affecting global public health and economy (3, 4). And the emergence of mutated strains further compounds the challenge of containing the COVID-19 pandemic, as these mutants become more resistant to vaccines (5). The COVID-19 pandemic is considered the most serious public health threat since the 1918 H1N1 Spanish flu. The COVID-19 pandemic has had a severe impact on the economy, politics and people’s lives around the world, and has exposed the chronic deficiencies in the health systems of many countries (6). Based on this, some international scholars have also carried out extensive research on the status quo, impact and countermeasures of the epidemic. For example, some scholars have conducted in-depth studies on housing and public space during the COVID-19 epidemic and the impact of COVID-19 on urban public space (7, 8).
Non-drug interventions are actions taken by individuals and groups, other than vaccination and medication, to slow the spread of an epidemic disease, with the primary objective of controlling the source of infection and cutting off transmission routes. Vaccination is one of the effective methods to control the COVID-19 epidemic (9). It is therefore essential that countries set strategic targets for vaccine research and development and reach broad consensus (10). Since the outbreak of the epidemic, countries have taken non-drug intervention measures of different degrees and vaccine research and development and vaccination measures to control the spread of the epidemic according to the development status of the epidemic, economic strength, service capacity of the medical and health system, population distribution and other factors, in an attempt to control the large-scale spread of the epidemic from the perspective of controlling the source of infection, cutting off the route of transmission, and protecting the vulnerable population (11). With the development and spread of the epidemic, different countries have achieved different results in the prevention and control efforts. In this study, six countries including China, Germany, Australia, the United States, South Africa and Italy were selected as research objects. China was the first country to detect the novel coronavirus, and has controlled the rapid spread of the epidemic in a relatively short period of time, so it is necessary to conduct an in-depth analysis of its successful experience. Germany and Australia are representative countries in Europe and Oceania respectively, and have their own characteristics in epidemic management. The United States, South Africa and Italy have all been hit hard by the outbreak, and have been among the hardest hit countries in the global epidemic. At the same time, the selection of these countries also takes into account the relatively even geographical distribution. Based on the implementation intensity of non-drug intervention measures and the implementation of vaccination, this study analyzed the strategies and effects of epidemic prevention and control in each country. In view of the heavy losses caused by the COVID-19 epidemic to mankind, the international community has paid close attention to the research related to public health emergencies. To a certain extent, this study provides a small reference for the management of public health emergencies.
2 Research objects and methods
2.1 Research objects and indicators
Six typical countries, namely China in Asia, Germany and Italy in Europe, Australia in Oceania, the United States in North America, and South Africa in Africa, were selected as research objects. Indicators such as total cases and deaths per million people, daily tests per thousand people, stringency index, total vaccinations per hundred people, daily new cases per million people, and daily new deaths per million people were included in the analysis.
2.2 Data sources
In this study, official Data of countries on COVID-19 were collected from the official website of the World Health Organization and the Novel Coronavirus Resource Center of Johns Hopkins University, specific measures taken in response to COVID-19 were collected from government websites of countries, and indicator data involved in this study were collected from Our World in Data website (12–20). The purpose of the World Health Organization is to achieve the highest possible level of health for the world’s people. During the COVID-19 epidemic, the World Health Organization updated authoritative data daily, which provided the data source for this study. The Novel Coronavirus Resource Center of Johns Hopkins University has provided unprecedented near-real-time data tracking of this unprecedented outbreak, providing visualizations of reported cases and deaths to the public, journalists and policymakers around the world. Our World in Data is a website that provides global data. The research team of Our World in data is affiliated with the Oxford Martin Global Development Program at the University of Oxford in the United Kingdom, and focuses on decades of national data on human living standards. The data density and value of the website are high, including population, economic, health and other data, providing us with a comprehensive perspective of global population and health. The Oxford Coronavirus Government Response Tracker (OxCGRT) project calculate a Stringency Index, a composite measure of nine of the response metrics. Nine metrics are used to calculate the Stringency Index: school closures; workplace closures; cancellation of public events; restrictions on public gatherings; closures of public transport; stay-at-home requirements; public information campaigns; restrictions on internal movements; and international travel controls. The index on any given day is calculated as the mean score of the nine metrics, each taking a value between 0 and 100. A higher score indicates a stricter response (100 = strictest response). Data collection varies from country to country; for example, Germany does not continuously report the number of tests. In order to improve the visibility and accuracy of the results, the index of “new tests per thousand” in this study uses the smoothed data after official processing on the database website.
2.3 Research methods
Ecological comparative study is a method widely used in ecological research. The simplest method is to observe the distribution of a disease in different populations or regions, and then propose etiological hypotheses based on the differences in the distribution of the disease. Ecological comparative research can also be applied to evaluate the effectiveness of social facilities, population interventions, and the implementation of policies and laws. This study uses ecological comparative study method to describe the epidemic prevention policies and vaccine measures in six countries. In this study, Excel data analysis software is used to make visual analysis by making statistical charts. Based on the analysis of the epidemic prevention and control effect in six countries, this study proposed the hypothesis that “the implementation of non-drug interventions and vaccine measures greatly affected the epidemic prevention and control effect.” The effects of non-drug interventions and vaccination on epidemic prevention and control in each country were analyzed by comparing the indicators such as total cases and deaths per million people, daily tests per thousand people, stringency index, and total vaccinations per hundred people, combined with the development status of the epidemic in each country, the economic strength, the service capacity of the medical and health system, and the population distribution.
3 Results
3.1 Non-drug interventions by countries
3.1.1 Containment strategies of China, Germany, and Australia
China, Germany, and Australia have tended to adopt strict containment strategies in the fight against COVID-19. China is following a classic containment strategy. Rapid response is critical in the early stages of an infectious disease outbreak (21). China became the first country to report a case of pneumonia of unknown cause after it was first reported in Wuhan, Hubei province. As the epidemic spread, the Chinese government attached great importance to it, took swift measures and brought the epidemic under control in a relatively short period of time (22, 23). During the epidemic, major measures include establishing a command system for COVID-19 prevention and control and building medical isolation facilities. When the epidemic is spreading, communities should play a role in epidemic prevention by adopting lockdown and medical treatment policies. In the phase of regular epidemic prevention and control, targeted measures have been taken across the country at different regions and levels to prevent imports and rebound at home. The policy focus on COVID-19 has shifted from medical support in the early stage to economic development in the later stage (24). Germany, one of the early countries in Europe to be affected by the outbreak, confirmed its first case of the novel coronavirus on January 27, 2020 local time, with an explosive increase in confirmed cases in late February. The German government has taken various measures to limit the gathering of people, strictly prevent the importation of the virus from abroad, initiated emergency plans, and increased the number of medical staff and hospital beds in an effort to contain the spread of the epidemic. Germany and Hong Kong produced the WHO-approved diagnostic test kits and distributed them to countries around the world on January 17, 2020. In addition, affected by the novel coronavirus epidemic, the German economy shrank and the employment situation was grim. The German government implemented the “short-time working plan.” Germany has a wide distribution of laboratories qualified for virus testing, and timely inclusion of relevant costs in the medical reimbursement system. Strict public health policies and generous social policies have been successful in Germany (25). Among the many countries affected by the novel coronavirus, Oceania’s epidemic prevention and control effect is relatively optimistic. Australia is relatively isolated on the land, and most of the domestic outbreaks are imported from abroad and spread in clusters. Since January 2020, Australia has screened airline passengers and subsequently ordered the closure of all public commercial places to prevent the spread of the virus. Unprecedented government spending on health care, employment and housing may have reduced anxiety and stress among some Australians (26). Although the worst impact was avoided, it still suffered many negative effects (27, 28). (Examples of specific measures taken by China, Germany and Australia are shown in Table 1).
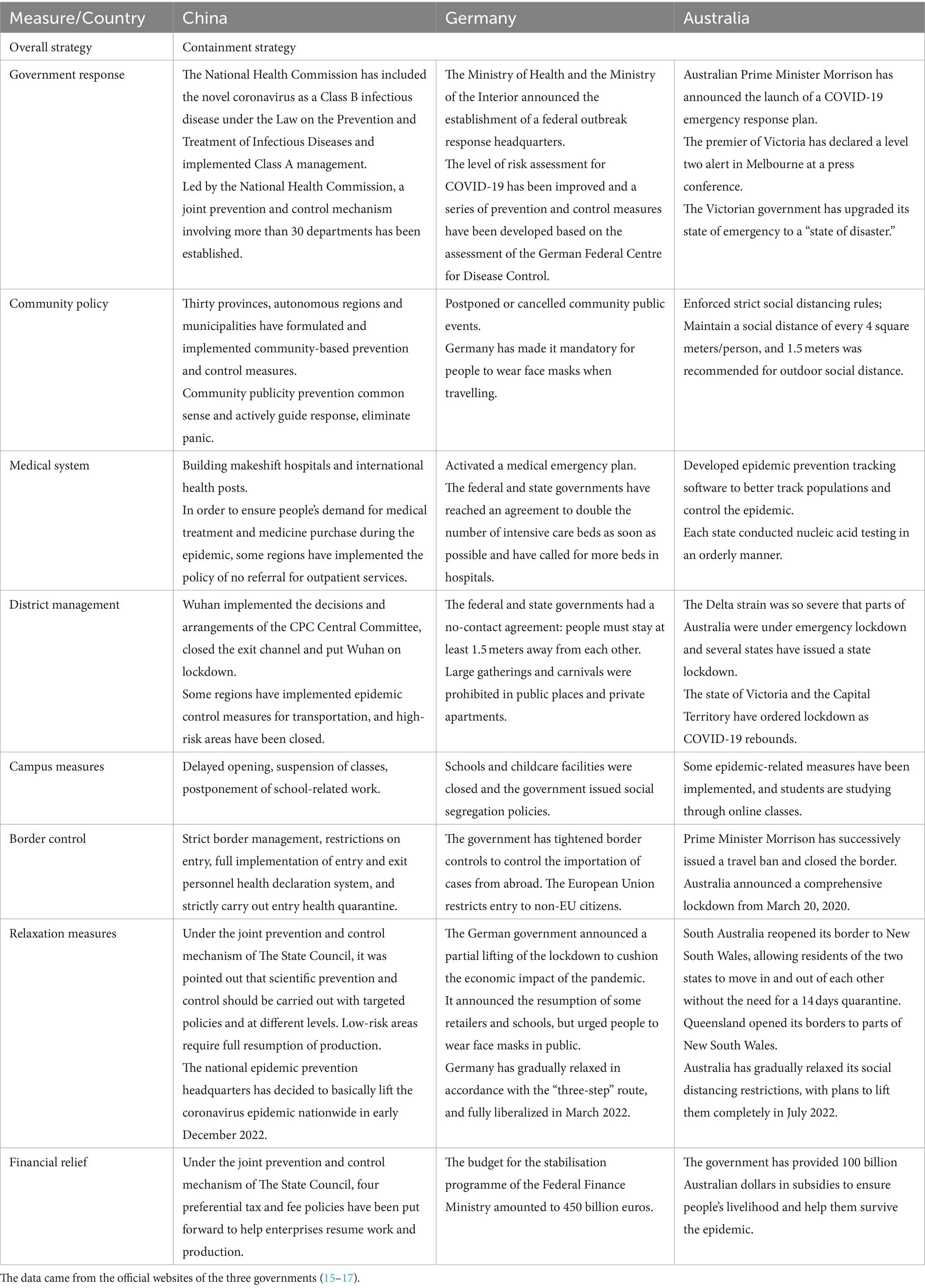
Table 1. Major non-drug interventions in response to COVID-19 in China, Germany, and Australia.
3.1.2 Mitigation strategies in the United States, South Africa, and Italy
Mitigation strategies aim to keep the number of infections low through modest control measures, but could overwhelm health service capacity if COVID-19 infections increase (29). The United States, South Africa, and Italy have tended to adopt relatively lenient mitigation strategies in the fight against COVID-19. After the outbreak of COVID-19, the United States announced its first case of COVID-19 on January 21, 2020 with the number of confirmed cases exceeding 1,000 on March 10, 2020 and confirmed cases in all 50 states on March 17, 2020. The United States has adopted a strategy of “containment” and “mitigation” to respond to the epidemic through multiple channels and means, including virus testing, campus prevention and control, and social distancing. But in the early stages of the outbreak, the United States only advised the public to take precautions but not to wear masks for healthy people. Most U.S. states and territories issued stay-at-home orders and shutdowns after the government imposed quarantines and curfews as the number of confirmed cases rose. At the same time, the United States increased investment to accelerate vaccine development and vaccination schedule (30, 31). However, the epidemic has not been fully alleviated, and states across the United States have begun to relax their epidemic control measures, reopening restaurants and gradually resuming production. South Africa was the first African country to declare a state of national disaster (32). On March 5, 2020, South Africa reported its first confirmed case of COVID-19. Soon, South Africa began to seal off the country, strictly implementing the “lockdown order” throughout the country, and set the lockdown level as the most stringent level five (33). However, after May 2020, the South African government gradually lowered the lockdown level from phase 5 to Phase 1, gradually easing the quarantine measures. Since the resumption of work and production in May, the number of newly confirmed cases in South Africa has fluctuated and the epidemic has shown a rebound trend.
Italy has taken different measures to contain the spread of the virus during the COVID-19 outbreak (34). As early as January 31, 2020, the Italian government began to implement border control measures. Italy did not initially implement strict restrictions, which led to the spread of the epidemic. At this point, the government began to act, but it was too late. Italy’s large population and high population density have exacerbated the difficulties of fighting the epidemic. With the first COVID-19 case reported on February 20, 2020, the outbreak has deteriorated rapidly in Italy, which also has the highest death rate in the world. From March to May, the government divided the country into different regions and quickly adopted radical lockdown measures, followed by national lockdown measures (35). In late May, 2020, the epidemic prevention and control measures were gradually relaxed. (Examples of specific measures taken by the United States, South Africa, and Italy are shown in Table 2).
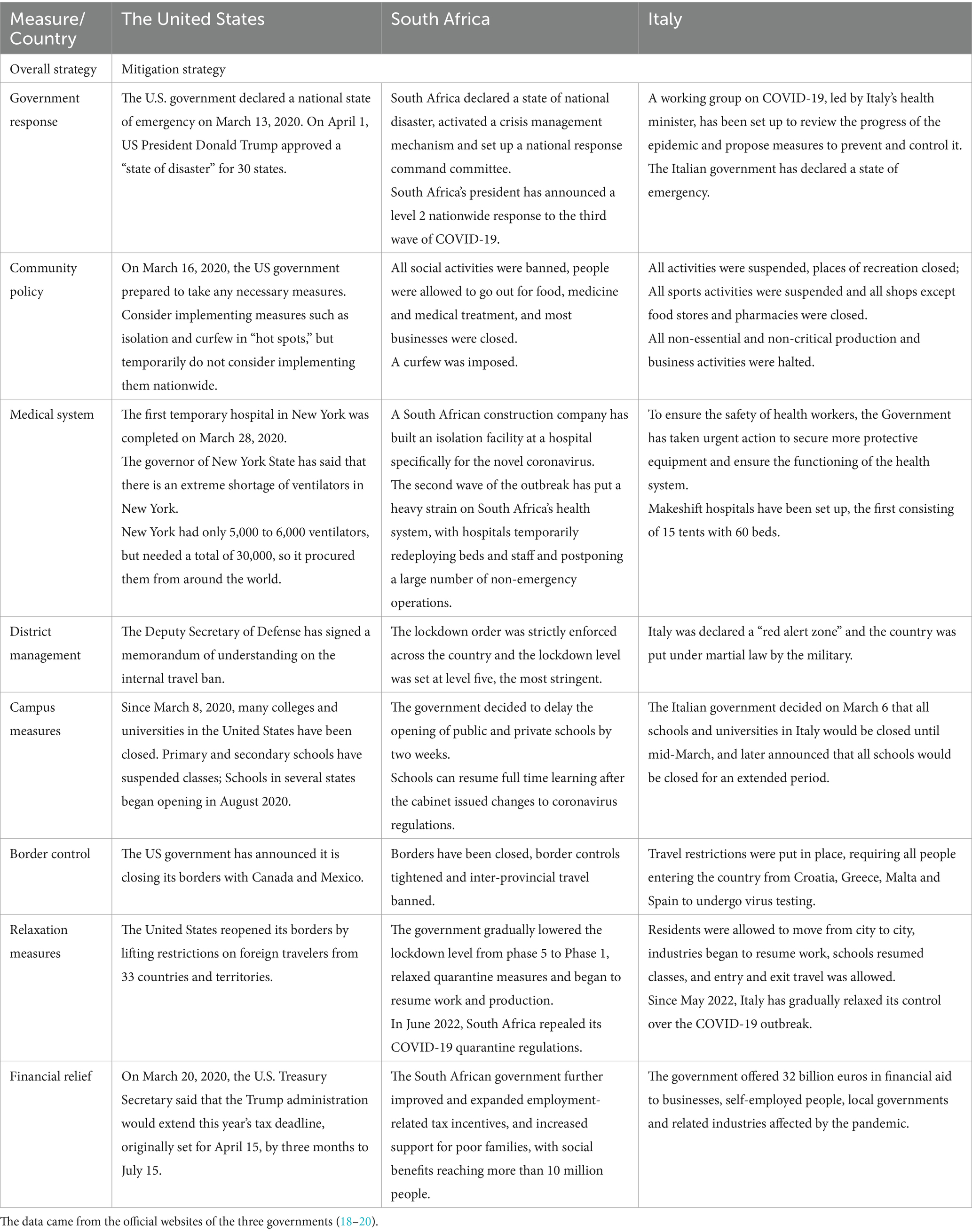
Table 2. Major non-drug interventions in response to COVID-19 in the United States, South Africa, and Italy.
3.2 Vaccine measures taken by countries
The research and development of COVID-19 vaccine is a race between human beings and the virus. Different countries and research and development institutions may have different tracks, but they are heading for the same destination. Since Chinese scientists released the whole genome sequence of the novel coronavirus on Jan 11, 2020, the global research and development of a vaccine against the novel coronavirus has been in high tide. As early as March 16, 2020, a candidate COVID-19 vaccine entered clinical testing for the first time, the fastest pace in history. (Detailed information on COVID-19 vaccine development and vaccination in six countries is shown in Table 3). First, in December 2020, some 20 million health care workers and older adult people in nursing homes across the United States were among the first to receive a vaccine against COVID-19. From January to March 2021, the second batch of people who received the COVID-19 vaccine include: teachers, police and other core posts, high-risk disease patients and people over 65 years old. From April to June 2021, vaccines were available for free throughout the United States.

Table 3. Main vaccine interventions in six countries.
3.3 Analysis of epidemic prevention and control effect in six countries
3.3.1 Basic information and epidemic situation in six countries
The basic characteristics of the six countries are shown in Table 4. Australia is the lowest population density of the six countries, which may reduce the difficulty of prevention and control to some extent, while Germany is the highest population density of the six countries. China and South Africa have relatively small populations over the age of 65. Of the six countries, China has the fewest cumulative confirmed cases per million people and cumulative deaths per million people. Of the six countries, China had the highest tightening index, while Australia and South Africa had the lowest. Germany has the highest number of hospital beds per 1,000 people, significantly higher than any other country. As the coronavirus epidemic has spread, governments have embraced a variety of non-drug interventions and issued a series of policy documents. With the changes in the trend of the epidemic and the needs of economic and social development, each country adjusted its prevention and control strategy based on its own national conditions.
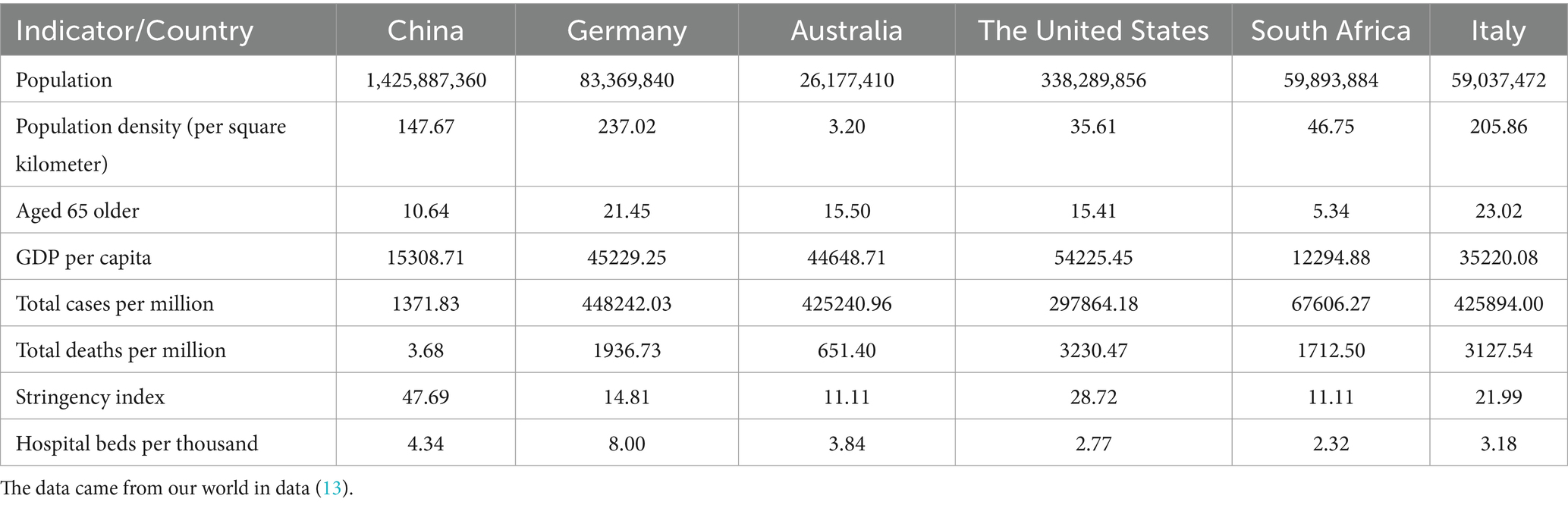
Table 4. Comparison of basic characteristics of six countries (as at 31 December 2022).
Figure 1 (Trends in total cases and deaths per million people) shows that the six countries have different epidemic prevention and control effects. In China, the cumulative number of confirmed cases per million people increased slowly and at a low level in the early stage, and there were two rising peaks in the later stage. The cumulative death cases per million people rose twice at the early stage of the epidemic, and then the growth rate was very slow. In Germany, the cumulative confirmed cases per million people and cumulative deaths per million people grew relatively slowly on the whole, but there was a peak of growth, respectively. In the early stage of the epidemic, the epidemic in Australia was well controlled, but since 2022, the epidemic has deteriorated sharply, with the cumulative number of confirmed cases per million people and the cumulative number of deaths per million people, respectively, showing a peak increase. The epidemic is growing rapidly in the United States, with the cumulative number of confirmed cases per million and the cumulative number of deaths per million continuing to increase. In South Africa, the cumulative number of confirmed cases and deaths per million people increased rapidly in the early period and experienced several growth peaks, but the growth slowed down in the later period. In Italy, the cumulative number of confirmed cases per million people increased rapidly, with one peak, and the cumulative number of deaths per million people showed a stepped increase trend, with three peaks. As of December 31, 2022, the cumulative number of confirmed cases per million people in China, Germany, Australia, the United States, South Africa and Italy was 1371.83, 448242.03, 425240.96, 297864.18, 67606.27 and 425894.00, respectively. The cumulative death cases per million population were 3.68, 1936.73, 651.40, 3230.47, 1712.50 and 3127.54.
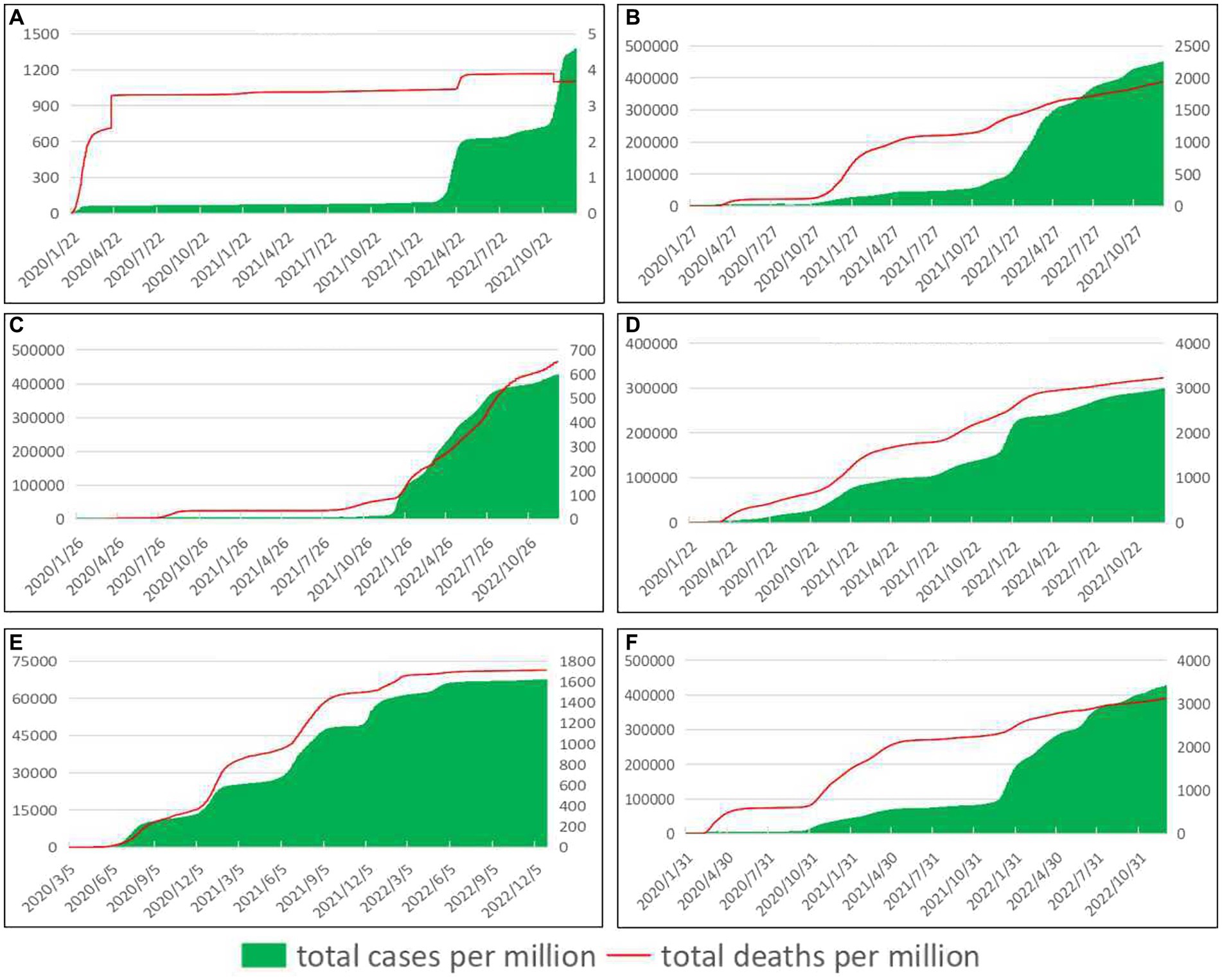
Figure 1. Trends in total cases and deaths per million people. See primary axis (left) for “total cases per million people” and secondary axis (right) for “total deaths per million people” (The data came from our world in data (13)).
3.3.2 The three principles of epidemic prevention in six countries
3.3.2.1 Control the source of infection
Since the outbreak of the novel coronavirus, countries have tested their citizens in order to keep track of the situation. As can be seen from Figure 2 (Trends in daily new cases per million people and daily tests per thousand people), when the number of newly confirmed cases increased, countries intensified their COVID-19 testing efforts to control the further epidemic to some extent, and the number of newly confirmed cases showed a downward trend after the number of each test reached its peak. Germany, the United States, South Africa, and Italy are particularly visible. In addition, a reduction in the number of daily tests may also lead to a sharp increase in the number of daily new confirmed cases in the future. For example, South Africa increased the number of tests when the epidemic was severe, and then relaxed after getting the epidemic slightly under control, leading to a rebound of the epidemic, and thus multiple peaks. During the epidemic period, in order to control and manage the source of infection in a timely manner and achieve early detection, isolation and treatment, multiple rounds of large-scale testing were carried out in various regions of China, and regular testing was flexibly arranged in accordance with the development of the epidemic situation. Since the number of daily tests in China is not reported continuously, there is no complete official authoritative data on daily tests per thousand people. The analysis of discontinuous data may cause errors in the results, so it is not shown in Figure 2.
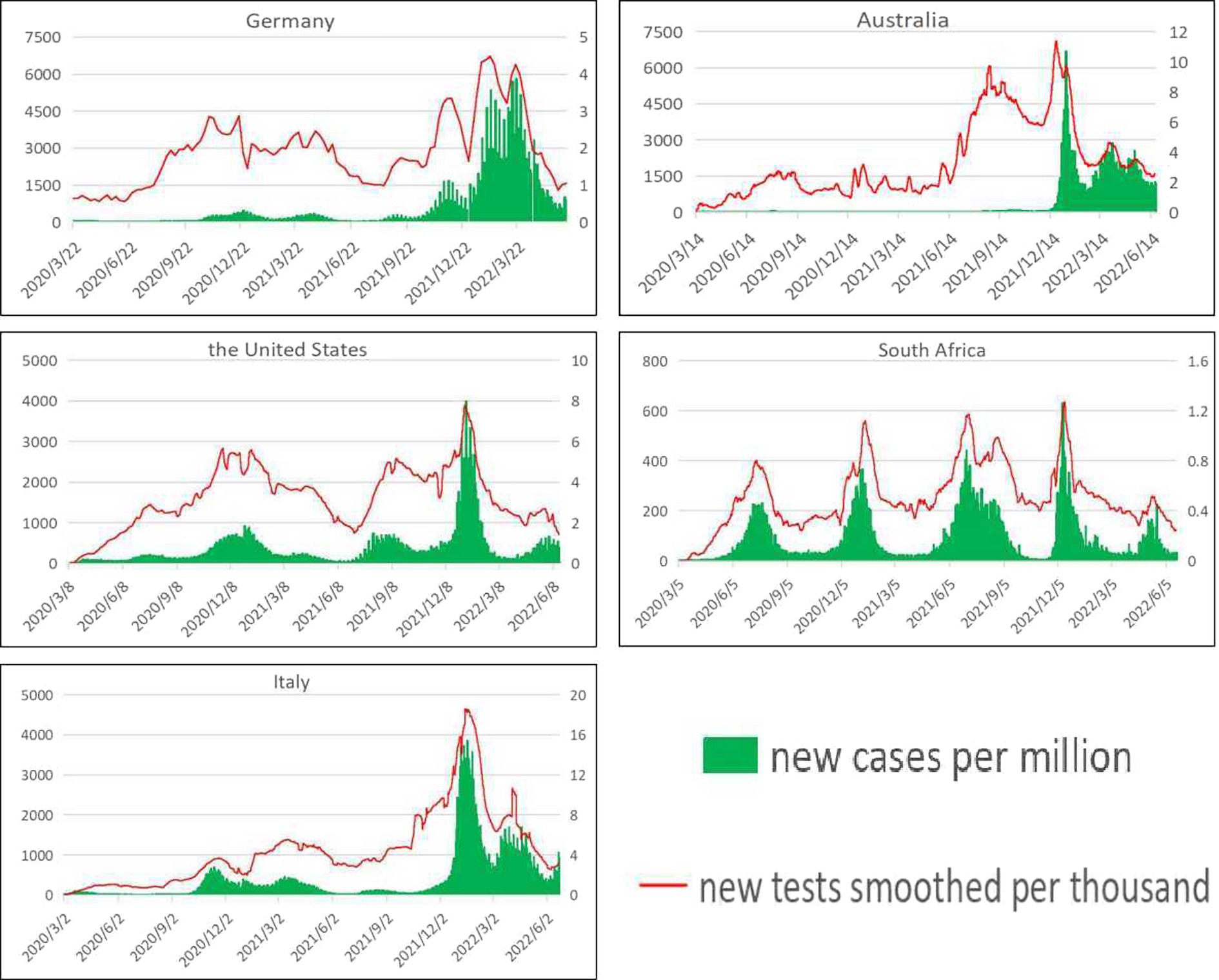
Figure 2. Trends in daily new cases per million people and daily tests per thousand people. See primary axis (left) for “daily new cases per million people” and secondary axis (right) for “daily tests per thousand people” (The data came from our world in data (13)).
3.3.2.2 Cut off transmission routes
Novel coronavirus pneumonia is a kind of acute infectious pneumonia, its infectivity is relatively strong, most will be transmitted through respiratory droplets. As a result, countries have adopted a series of measures to block transmission routes. As can be seen from Figure 3 (Trends in daily new cases per million people and stringency index), since 2020, countries have introduced a series of epidemic prevention and control policies when the epidemic becomes more serious, but the degree of stringency and effectiveness of prevention and control policies vary from country to country. In general, in the early stage of the epidemic, countries adopted stricter epidemic prevention and control policies with a higher stringency index. In the later period, epidemic prevention and control was gradually relaxed, and the level of stringency index was lowered. In addition, when the pandemic situation is severe, the stringency index of countries increases; as the situation of the epidemic eases, the stringency index of countries shows a downward trend, but as the epidemic prevention and control is relaxed, the epidemic will rebound, such as in the United States.
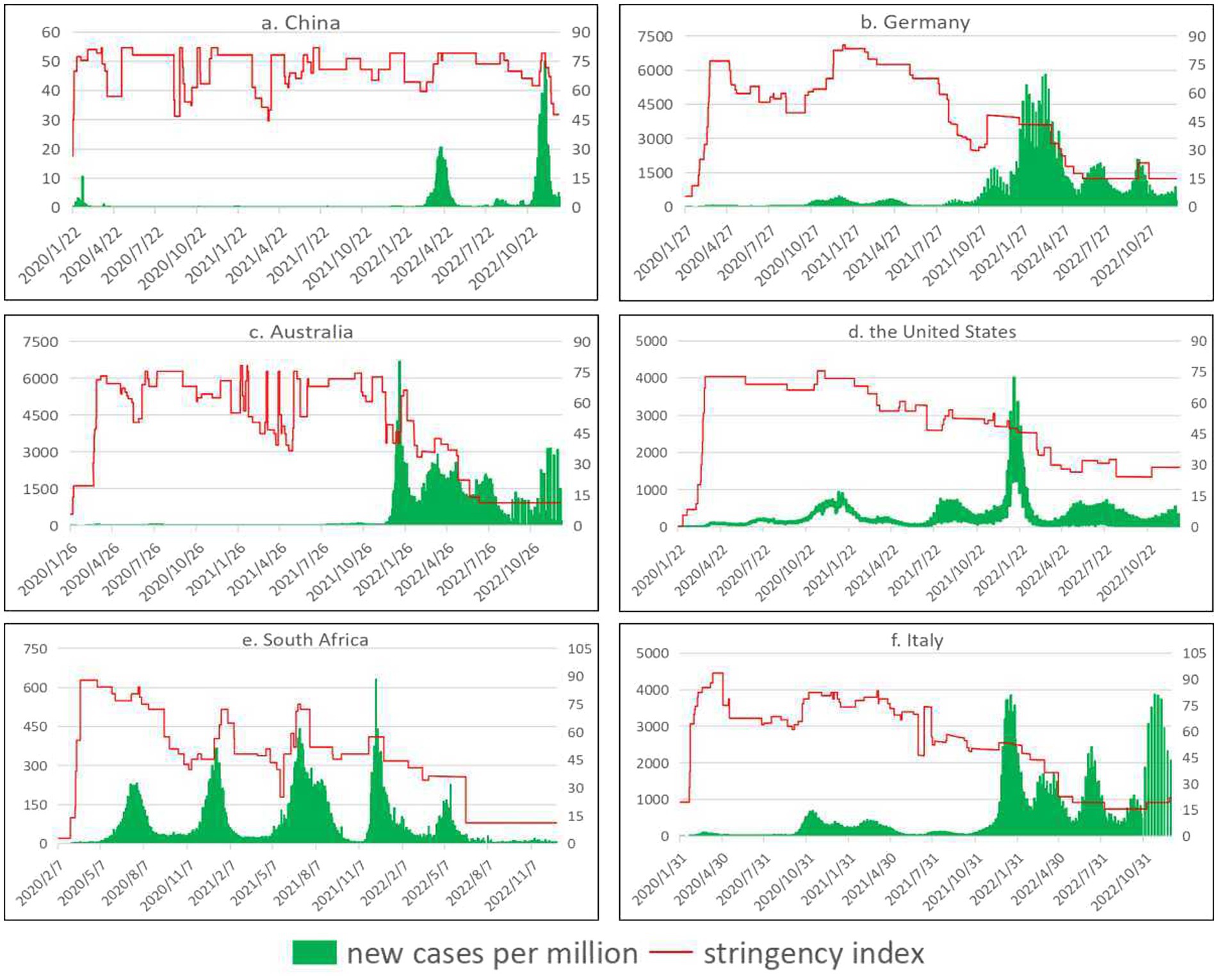
Figure 3. Trends in daily new cases per million people and stringency index. See primary axis (left) for “daily new cases per million people” and secondary axis (right) for “stringency index” (The data came from our world in data (13)).
3.3.2.3 Protect vulnerable populations
Since the outbreak of COVID-19, countries have actively developed vaccines and carried out continuous vaccination. As can be seen from Figure 4 (Trends in daily new deaths per million people and total vaccinations per hundred people), the number of daily new deaths per million people in China, Germany, and South Africa showed a downward trend with the increase of the number of vaccines administered per 100 people. Even if there was a peak, the number of daily new deaths per million people was moderate compared with the early stage of the epidemic. In Australia, the United States, and Italy, daily new deaths per million people continued to peak after vaccination, and the outbreak has eased, but not significantly. According to the latest statistical data in December 2022, the number of people fully vaccinated per 100 people in China, Germany, Australia, the United States, South Africa, and Italy is 89.35, 76.23, 82.72, 69.09, 35.13, and 81.26, respectively. Germany, Australia, the United States, and Italy had a high rate of full vaccination, but also saw a peak in the number of daily new deaths. South Africa has a low rate of full vaccination, but it also saw a decline in the number of daily new deaths in the later stages of the epidemic.
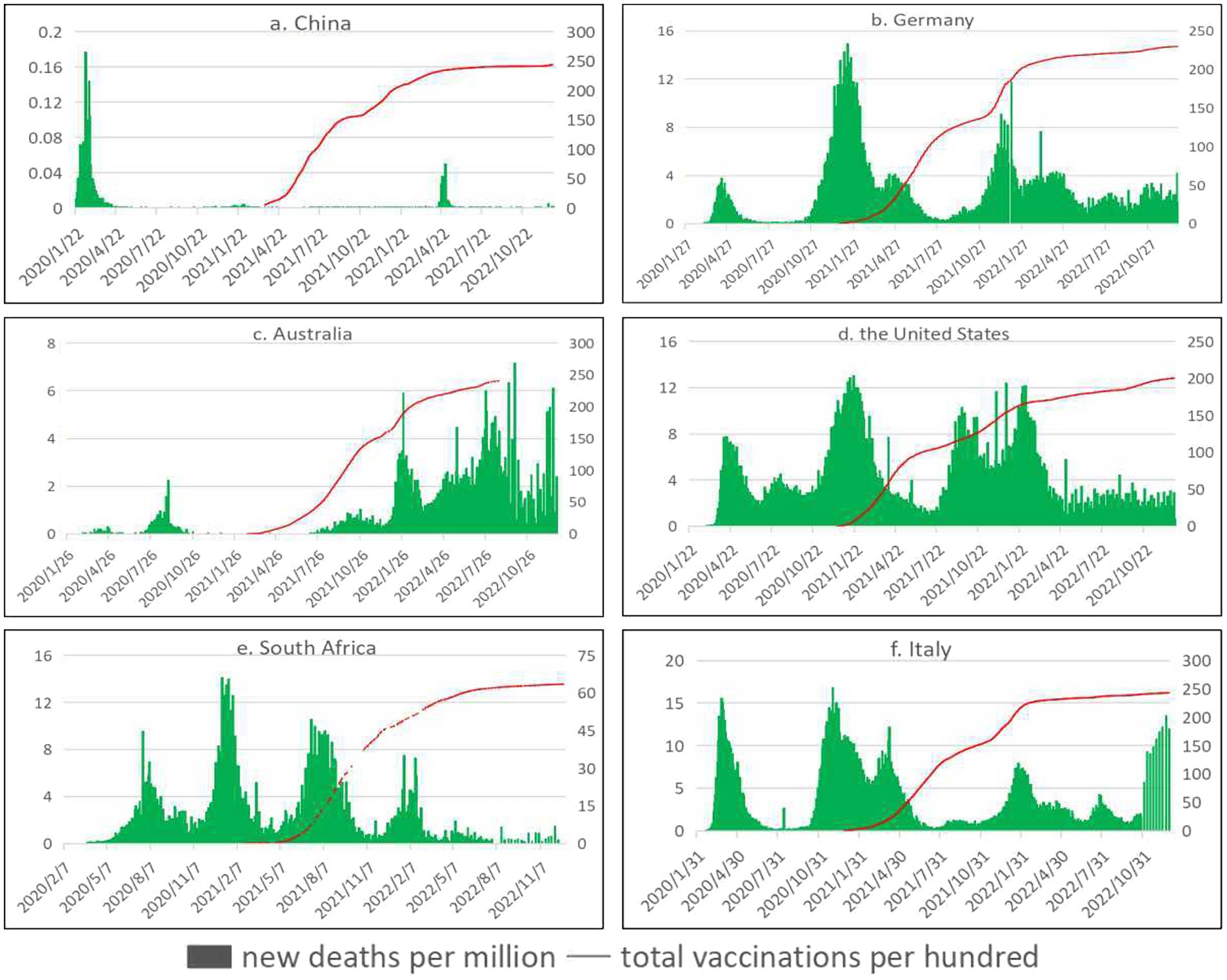
Figure 4. Trends in daily new deaths per million people and total vaccinations per hundred people. See primary axis (left) for “daily new deaths per million people” and secondary axis (right) for “total vaccinations per hundred people” (The data came from our world in data (13)).
4 Discussion
4.1 Containment strategies and mitigation strategies
Since the outbreak of COVID-19 as a public health emergency, countries have taken a series of measures and issued a series of policy documents in various aspects. For example, home quarantine, shutdown of production and schools, emergency response mechanism, strict border control, vaccine clinical trials, etc. In addition, some scholars have explored how transmission can decline after disease detection and implementation of combined non-drug measures, based on the analysis of the early epidemiological characteristics of the COVID-19 outbreak (36). The policies and measures adopted by various countries in response to the COVID-19 epidemic have their own characteristics, strengths and weaknesses, and the effectiveness of epidemic prevention is also significantly different. China, which adopted a strict containment strategy, initially contained the spread of the epidemic in more than a month, controlled the daily new cases within a single digit in about 2 months, and achieved decisive results in the defense battle in Wuhan and Hubei in about 3 months. However, the United States, which adopted mitigation strategies, once had the highest cumulative number of confirmed cases and cumulative number of deaths in the world (37). In addition, some scholars have conducted in-depth analysis of the measures taken during the epidemic in many countries, and believe that non-drug interventions can effectively level the epidemic curve, and rapid and strict comprehensive containment strategies are successful measures to control the epidemic, especially in the absence of vaccines and effective therapies (38–40). In view of this, countries should be able to make prompt decisions when responding to public health emergencies, have enough sensitivity, and adopt strict containment strategies in a timely manner to reduce the risk of explosive spread of the epidemic.
4.2 Control the source of infection
Infectious diseases are diseases caused by various pathogens that can be transmitted from person to person. In the prevention and treatment of infectious diseases, it is necessary to control the source of infection, such as early detection and treatment, and observation of close contacts. Early detection of the novel coronavirus is extremely important to contain the spread of the pandemic. It can grasp the development of the epidemic to a certain extent, track cases in a timely manner, and intervene in close contacts. Germany and Hong Kong have rapidly developed the WHO-approved PCR test, which has become the standard around the world (except in the United States). The Australian government had allocated more than a $750 million to ramp up testing, which in the early months of the outbreak was among the highest in the world in testing per 1,000 people. Extensive and frequent testing is also critical to the containment of COVID-19 in the United States (41). Combined, the countries showed a decline in the number of daily new cases per million people in the coming months after the increased testing. With the different situation of the development of the epidemic, countries have also made adjustments to the cost of testing. For example, whether nucleic acid testing is free in China depends on the identity of the person tested and the local disease control policy. Generally, for personnel who must be tested, the cost of nucleic acid testing shall be borne by the state and local governments, while for personnel who voluntarily test, the cost of nucleic acid testing shall be borne by units or individuals. Therefore, when dealing with COVID-19 and other similar public health emergencies, we should actively carry out case detection, and strive to achieve early detection and isolation, so as to reduce the probability of human to human transmission.
4.3 Cut off transmission routes
Infectious diseases are spread by respiratory droplets, blood transmission, contact transmission and so on. After an outbreak of an infectious disease, disinfection and isolation can be carried out. For example, wear a mask, keep the air circulating at home, and sterilize the air when necessary. Some researchers have also designed and evaluated various strategies to increase people’s wearing of masks, and have assessed the impact of community wearing of masks on COVID-19 infection rates (42). Some countries like China implemented strict policies at the early stage of the epidemic. As the epidemic eased, countries gradually relaxed their vigilance and relaxed quarantine and mask measures, leading to varying degrees of rebound of the epidemic. For example, around Independence Day in the United States in 2020, people held large outdoor parties to celebrate Independence Day. Crowds were crowded and many people did not wear masks, leading to an increasing number of cluster infections, and the number of people infected with the novel coronavirus continued to soar in about 40 of the 50 states. Therefore, strict government policies, especially quarantine policies, are essential for epidemic prevention and control, especially in the early stages without vaccine assistance. However, it is worth noting that the implementation time of lockdown policies in many countries has also greatly affected the effectiveness of epidemic prevention and control. In early December 2019, unexplained infections were first detected in Wuhan, Hubei Province, China. The Wuhan lockdown, which took place on January 23, 2020, was one of the largest and most widespread in China’s history, and played an important role in the country’s ability to quickly contain the spread of the disease. South Africa’s Minister of Health held a press conference on 5 March 2020 to confirm the first confirmed case of novel coronavirus pneumonia in South Africa. In order to contain the rapid spread of the epidemic, the National COVID-19 Command Committee decided to implement a nationwide lockdown from March 26 local time. On the evening of February 20, 2020, a hospital detected Italy’s first indigenous confirmed case, known as Patient 1. Italy’s prime minister has announced a nationwide lockdown from March 10, 2020. During this time, Italy has seen an explosion in confirmed cases. Comparing the time of the first confirmed case and the time of strict lockdown measures in these countries, we can find that the response measures in countries are relatively delayed. Although these efforts are commendable, relatively delayed policies will weaken the effect. Major infectious diseases and other sudden public health emergencies pose a threat to human health. Countries should implement strict policy measures in the face of similar public health emergencies, restrict personnel contact from multiple aspects, cut off the transmission routes of the virus, and strive to control the epidemic in a short period of time. At the same time, the public should also actively cooperate with government policies, wear masks, actively isolate at home, maintain social distance, work together, and overcome difficulties together.
4.4 Protect vulnerable populations
The COVID-19 epidemic has gradually spread around the world, with a rapid increase in confirmed cases, increasing the burden on medical systems and shortages of health supplies in many countries, and prompting countries to take response measures. Germany’s Federal Ministry of Health has focused on purchasing protective equipment for clinics and hospitals, doubling the number of intensive care beds in the short term. In March 2020, a US Navy hospital ship docked at SAN Pedro Pier in Los Angeles to provide 1,000 beds for California, which was severely affected by the epidemic, and ease the burden on onshore hospitals. On March 27, 2020, the governor of New York State announced the completion of the first temporary hospital in Manhattan, New York City, to adapt to the COVID-19 outbreak. At the same time, countries are also actively carrying out vaccine research and development and vaccination. When the human body resistance is relatively poor, the risk of infectious diseases is also greater. The older adult, children, pregnant women and other groups have poor resistance, and are susceptible to infectious diseases. These people can then receive the appropriate vaccine, improve the body’s immune mechanism. Vaccination can prevent the infection of novel coronavirus or Omicron, and reduce the incidence of novel coronavirus infection. Vaccination of novel coronavirus vaccine is of great significance to strengthen the immune barrier of the population and stop the epidemic of novel coronavirus pneumonia. Some scholars have confirmed the effectiveness of BNT162b2 vaccine against COVID-19 infection in their studies and some research results have provided support for high effectiveness of BNT162b2 against hospital admissions up until around 6 months after being fully vaccinated (43, 44). Adherence to COVID-19 preventive measures and appropriate population vaccination levels are undoubtedly important means to control the outbreak (45). Of the six countries, China has the highest number of fully vaccinated people per 100 and the fewest cumulative deaths. South Africa also has low vaccination rates and should use available COVID-19 vaccines (46). It is worth noting that incomplete vaccine coverage, combined with continued community transmission, has facilitated the emergence of mutated strains. The protective effectiveness of the vaccine wanes to some extent over time, so when the mutant strain appears, countries bounce back due to its greater transmissibility and shorter incubation period. To sum up, countries should actively support vaccine research and development and vaccination when responding to public health emergencies such as the COVID-19 outbreak. People in all countries should pay attention to physical fitness and actively cooperate with the vaccination work. However, it is important to note that vaccination measures cannot replace non-drug interventions, and the two complement each other to have a greater impact.
4.5 Limitations
The study also has the following limitations. The stringency index used in this article does not measure or imply the adequacy or effectiveness of a country’s response. A higher score does not necessarily mean a better response from a country. For example, it may be that some countries have a high stringency index, but there are large election campaigns or large rallies in the meantime, and this does not reflect it. In ecological research, ecological fallacy is the most important shortcoming of this kind of research, which is because ecological research is made up of individuals in different situations, the group is the unit of observation and analysis, and the existence of confounding factors and other reasons cause the research results are not consistent with the real situation. For this reason, it is difficult to avoid ecological fallacy in ecological research in general. In view of the characteristics and limitations of ecological research, this study focuses on the research purpose as much as possible and sets only one research question. At the same time, more variables are included in the process of analyzing the problem and testing the hypothesis to reduce errors. In addition, due to statistical differences between countries, it is not possible to find all the continuous data needed for the study, resulting in many analysis limitations. Finally, when speculating on the research results, try to compare with other non-ecological research results, and combine the professional knowledge of the research problem to make a comprehensive analysis and judgment. In addition, factors such as population, culture, geography and economic level have complicated impacts on the development and prevention and control of the epidemic, and further in-depth research is needed.
5 Conclusion
This study analyzed the effect of non-drug intervention measures and vaccine coverage on COVID-19 prevention and control through ecological comparative study on COVID-19 in six countries. Based on the three principles for the prevention and control of epidemiological infectious diseases, the current situation of epidemic prevention and control in each country and the effect of prevention and control measures were analyzed in detail. Studies have confirmed that the implementation of non-drug interventions and vaccination will greatly affect the effectiveness of epidemic prevention and control. In the early stage of the epidemic, in the absence of effective vaccine support, non-drug interventions are an important means to deal with the epidemic, and a rapid and strict comprehensive containment strategy is an important measure to control the rapid spread of the epidemic. Vaccine development and vaccination is an important part of the prevention and control of COVID-19. However, the coverage rate of vaccines in some countries is still low, so it is still necessary to vigorously promote the vaccination of COVID-19 vaccines and booster shots. Vaccines cannot replace non-drug interventions, and when vaccine coverage is insufficient to establish a solid population immunity barrier, premature elimination of non-drug interventions is highly likely to lose the previous prevention and control achievements, leading to the rebound of the epidemic. Therefore, vaccination alone cannot completely stop the outbreak and needs to be combined with non-drug interventions. Each community should do a good job in health education, vaccination, and disease detection to improve the health literacy and disease prevention ability of residents. All countries should actively participate in international cooperation, review the experience of responding to public health emergencies in COVID-19 prevention and control, and learn from the successful experience of other countries to make up for their weaknesses. Countries also need to improve their public health emergency response mechanisms and be able to respond quickly to public health emergencies. In view of the limitations and shortcomings of this study, the team will use more accurate data and more abundant indicators in the future to conduct in-depth research on global epidemic prevention and control, and continue to explore effective measures to deal with public health emergencies.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found at: https://github.com/owid/covid-19-data/tree/master/public/data.
Author contributions
ML: Data curation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. LS: Data curation, Project administration, Resources, Writing – review & editing. MY: Data curation, Writing – review & editing. JJ: Data curation, Writing – review & editing. JY: Data curation, Supervision, Writing – review & editing. MM: Data curation, Supervision, Writing – review & editing. WX: Data curation, Investigation, Writing – review & editing. GS: Data curation, Funding acquisition, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
This research was funded by Philosophy and Social Sciences Planning Project of Guangdong Province in 2023: Research on the mechanism of national voluntary epidemic prevention behavior based on Repast-fsQCA in the context of COVID-19 “Class B and B control”, grant number GD23CGL11, and Natural Science Foundation of Guangdong Province in 2022: Construction and application of COVID-19 control model PSR-SOR-Haddon in Guangdong Province, grant number 2022A1515011112.
Acknowledgments
The authors gratefully acknowledge the study participants who have been involved and contributed to the procedure of data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Dhama, K, Khan, S, Tiwari, R, Sircar, S, Bhat, S, Malik, YS, et al. Coronavirus disease 2019-COVID-19. Clin Microbiol Rev. (2020) 33:e00028. doi: 10.1128/CMR.00028-20
2. Chung, JY, Thone, MN, and Kwon, YJ. COVID-19 vaccines: the status and perspectives in delivery points of view. Adv Drug Deliv Rev. (2021) 170:1–25. doi: 10.1016/j.addr.2020.12.011
3. Chavda, VP, Kapadia, C, Soni, S, Prajapati, R, Chauhan, SC, Yallapu, MM, et al. A global picture: therapeutic perspectives for COVID-19. Immunotherapy. (2022) 14:351–71. doi: 10.2217/imt-2021-0168
4. Karamouzian, M, and Madani, N. COVID-19 response in the Middle East and North Africa: challenges and paths forward. Lancet Glob Health. (2020) 8:e886–7. doi: 10.1016/S2214-109X(20)30233-3
5. Raman, R, Patel, KJ, and Ranjan, K. COVID-19: unmasking emerging SARS-CoV-2 variants. Vaccines Ther Strat Biomol. (2021) 11:993. doi: 10.3390/biom11070993
6. Mustafa, S, Zhang, Y, Zibwowa, Z, Seifeldin, R, Ako-Egbe, L, McDarby, G, et al. COVID-19 preparedness and response plans from 106 countries: a review from a health systems resilience perspective. Health Policy Plan. (2022) 37:255–68. doi: 10.1093/heapol/czab089
7. Rosa-Jiménez, C, and Jaime-Segura, C. Living space needs of small housing in the post-pandemic era: Malaga as a case study. J Contemp Urban Affairs. (2022) 6:51–8. doi: 10.25034/ijcua.2022.v6n1-5
8. Nia, HA. A comprehensive review on the effects of COVID-19 pandemic on public urban spaces. Architect Urban Planning. (2021) 17:79–87. doi: 10.2478/aup-2021-0008
9. Park, T, Hwang, H, Moon, S, Kang, SG, Song, S, Kim, YH, et al. Vaccines against SARS-CoV-2 variants and future pandemics. Expert Rev Vaccines. (2022) 21:1363–76. doi: 10.1080/14760584.2022.2110075
10. Hu, Y, and Chen, S. What can we learn from COVID-19 vaccine R&D in China? A discussion from a public policy perspective. J Travel Med. (2021) 28:taab026. doi: 10.1093/jtm/taab026
11. Dong, Y, Dai, T, Wang, B, Zhang, L, Zeng, LH, Huang, J, et al. The way of SARS-CoV-2 vaccine development: success and challenges. Signal Transduct Target Ther. (2021) 6:387. doi: 10.1038/s41392-021-00796-w
12. World Health Organization. Number of COVID-19 cases reported to WHO. Available at: https://data.who.int/dashboards/covid19/cases?n=c. (Accessed 10 February 2023)
13. Our World in Data. Coronavirus pandemic (COVID-19). Available at: https://ourworldindata.org/coronavirus-data-explorer. (Accessed 20 February 2023)
14. Johns Hopkins Coronavirus Resource Center. Ongoing Johns Hopkins COVID-19 resources. Available at: https://coronavirus.jhu.edu/#:~:text=Ongoing%20Johns%20Hopkins%20COVID%2D19%20Resources. (Accessed 3 February 2023)
15. Central People's Government of the People's Republic of China. Library of State Department policy documents. Available at: http://sousuo.www.gov.cn/zcwjk/policyDocumentLibrary?q=&t=zhengcelibrary. (Accessed 7 March 2023)
16. Federal Foreign Office. Federal Foreign Office. Available at: https://www.auswaertiges-amt.de/en. (Accessed 13 March 2023)
17. Australian Government Department of Foreign Affairs and Trade. Australian government Department of Foreign Affairs and Trade. Available at: https://www.dfat.gov.au/. (Accessed 17 March 2023)
18. The United States government. COVID-19 testing and vaccinations. Available at: https://www.usa.gov/covid-tests-vaccinations. (Accessed 20 March 2023)
19. South African Government. South African Government. Available at: https://www.gov.za/. (Accessed 25 March 2023)
20. Italian Government Presidency of the Council of Ministers. Italian government presidency of the Council of Ministers. Available at: https://www.governo.it/en/government. (Accessed 29 March 2023)
21. Chen, S, Chen, Q, Yang, W, Xue, L, Liu, Y, Yang, J, et al. Buying time for an effective epidemic response: the impact of a public holiday for outbreak control on covid-19 epidemic spread. Engineering. (2020) 6:1108–14. doi: 10.1016/j.eng.2020.07.018
22. Mei, C. Policy style, consistency and the effectiveness of the policy mix in China's fight against COVID-19. Polic Soc. (2020) 39:309–25. doi: 10.1080/14494035.2020.1787627
23. Zhang, A, Yang, H, Tong, S, and Gao, J. An investigation on Chinese public acceptance of COVID-19 prevention measures. Int J Environ Res Public Health. (2022) 19:5087. doi: 10.3390/ijerph19095087
24. Wu, J, Wang, K, He, C, Huang, X, and Dong, K. Characterizing the patterns of China’s policies against COVID-19: a bibliometric study. Inf Process Manag. (2021) 58:102562. doi: 10.1016/j.ipm.2021.102562
25. Greer, SL, Jarman, H, Falkenbach, M, Massard da Fonseca, E, Raj, M, and King, EJ. Social policy as an integral component of pandemic response: learning from COVID-19 in Brazil, Germany, India and the United States. Glob. Public Health. (2021) 16:1209–22. doi: 10.1080/17441692.2021.1916831
26. Berger, E, and Reupert, A. The COVID-19 pandemic in Australia: lessons learnt. Psychol Trauma. (2020) 12:494–6. doi: 10.1037/tra0000722
27. Basseal, JM, Bennett, CM, Collignon, P, Currie, BJ, Durrheim, DN, Leask, J, et al. Key lessons from the COVID-19 public health response in Australia. Lancet Reg Health West Pac. (2023) 30:100616. doi: 10.1016/j.lanwpc.2022.100616
28. Duckett, SJ, and Sutton, B. On entering Australia’s third year with COVID-19. Med J Aust. (2021) 215:509–10. doi: 10.5694/mja2.51328
29. Lu, G, Razum, O, Jahn, A, Zhang, Y, and Müller, O. COVID-19 in Germanyand China: mitigation versus elimination strategy. Glob Health Action. (2021) 14:1. doi: 10.1080/16549716.2021.1875601
30. Wood, S, and Schulman, K. Beyond politics – promoting Covid-19 vaccination in the United States. N Engl J Med. (2021) 384:e23. doi: 10.1056/NEJMms2033790
31. Burki, TK. A new year, but familiar challenges from COVID-19 in the USA. Lancet Respir Med. (2021) 9:e19. doi: 10.1016/S2213-2600(21)00011-4
32. Saloshni, N, and Nithiseelan, NR. Vulnerability of south African women workers in the COVID-19 pandemic. Front Public Health. (2022) 10:964073. doi: 10.3389/fpubh.2022.964073
33. Hatefi, S, Smith, F, Abou-El-Hossein, K, and Alizargar, J. The pandemic of COVID-19: current situation in South Africa. Disaster Med Public Health Prep. (2022) 16:1715–6. doi: 10.1017/dmp.2021.61
34. Reno, C, Sanmarchi, F, Stoto, MA, Fantini, MP, Lenzi, J, and Golinelli, D. The impact of health policies and vaccine rollout on the COVID-19 pandemic waves in Italy. Health Policy Technol. (2022) 11:100604. doi: 10.1016/j.hlpt.2022.100604
35. Capano, G. Policy design and state capacity in the COVID-19 emergency in Italy: if you are not prepared for the (un)expected, you can be only what you already are. Polic Soc. (2020) 39:326–44. doi: 10.1080/14494035.2020.1783790
36. Riccardo, F, Ajelli, M, Andrianou, XD, Bella, A, Del Manso, M, Fabiani, M, et al. Epidemiological characteristics of COVID-19 cases and estimates of the reproductive numbers 1 month into the epidemic, Italy, 28 January to 31 march 2020. Euro Surveill. (2020) 25:2000790. doi: 10.2807/1560-7917.ES.2020.25.49.2000790
37. Sung, B. A spatial analysis of the association between social vulnerability and the cumulative number of confirmed deaths from COVID-19 in United States counties through November 14, 2020. Osong Public Health Res Perspect. (2021) 12:149–57. doi: 10.24171/j.phrp.2020.0372
38. Wu, S, Neill, R, De Foo, C, Chua, AQ, Jung, AS, Haldane, V, et al. Aggressive containment, suppression, and mitigation of COVID-19: lessons learnt from eight countries. BMJ. (2021) 375:e067508. doi: 10.1136/bmj-2021-067508
39. Ilhan, MN, Tüzün, H, Kiliç, R, and Yildirim, N. Nonpharmaceutical interventions in Turkey and worldwide during COVID-19 pandemic. Turk J Med Sci. (2021) 51:3207–14. doi: 10.3906/sag-2106-210
40. Wong, MCS, Ng, RWY, Chong, KC, Lai, CKC, Huang, J, Chen, Z, et al. Stringent containment measures without complete city lockdown to achieve low incidence and mortality across two waves of COVID-19 in Hong Kong. BMJ Glob Health. (2020) 5:e003573. doi: 10.1136/bmjgh-2020-003573
41. Rosenberg, ES, and Holtgrave, DR. Widespread and frequent testing is essential to controlling coronavirus disease 2019 (COVID-19) in the United States. Clin Infect Dis. (2021) 73:e2918–20. doi: 10.1093/cid/ciaa1508
42. Kwong, LH, Bates-Jefferys, E, Crawford, EE, Benjamin-Chung, J, and Benhachmi, S. The impact of mask distribution and promotion on mask uptake and COVID-19 in Bangladesh. Environ Sci. (2021) 375:e9069. doi: 10.1126/science.abi9069
43. Tartof, SY, Slezak, JM, Fischer, H, Hong, V, Ackerson, BK, Ranasinghe, ON, et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: a retrospective cohort study. Lancet. (2021) 398:1407–16. doi: 10.1016/S0140-6736(21)02183-8
44. Polack, FP, Thomas, SJ, Kitchin, N, Absalon, J, Gurtman, A, Lockhart, S, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. (2020) 383:2603–15. doi: 10.1056/NEJMoa2034577
45. Umakanthan, S, Sahu, P, Ranade, AV, Bukelo, MM, Rao, JS, Abrahao-Machado, LF, et al. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. (2020) 96:753–8. doi: 10.1136/postgradmedj-2020-138234
Keywords: COVID-19, non-drug interventions, vaccination measures, containment strategies, mitigation strategies, ecological comparison
Citation: Liu M, Shi L, Yang M, Jiao J, Yang J, Ma M, Xie W and Sun G (2024) Ecological comparison of six countries in two waves of COVID-19. Front. Public Health. 12:1277457. doi: 10.3389/fpubh.2024.1277457
Edited by:
Brent M. Egan, American Medical Association, United StatesReviewed by:
Ornella Punzo, National Institute of Health (ISS), ItalyHourakhsh Ahmad Nia, Alanya University, Türkiye
Copyright © 2024 Liu, Shi, Yang, Jiao, Yang, Ma, Xie and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gang Sun, sunhoney163@163.com; gsun15@jhu.edu