 Yongfu Yan1†Yingying Jiang2†
Yongfu Yan1†Yingying Jiang2† Rong Liu3‡Michael Eddleston4
Rong Liu3‡Michael Eddleston4 Chuanjiang Tao5Andrew Page6Lijun Wang2
Chuanjiang Tao5Andrew Page6Lijun Wang2 Guoshuang Feng7*
Guoshuang Feng7* Shiwei Liu1*
Shiwei Liu1*- 1Tobacco Control Office, Chinese Center for Disease Control and Prevention, Beijing, China
- 2National Center for Chronic and Noncommunicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing, China
- 3The George Institute for Global Health, Faculty of Medicine, The University of New South Wales (UNSW), Sydney, NSW, Australia
- 4Centre for Pesticide Suicide Prevention, University of Edinburgh, Edinburgh, United Kingdom
- 5Institute for the Control of Agrochemicals, Ministry of Agriculture and Rural Affairs, Beijing, China
- 6Translational Health Research Institute, Western Sydney University, Penrith, NSW, Australia
- 7Big Data Center, Beijing Children's Hospital, Capital Medical University, National Center for Children's Health, Beijing, China
Background: Pesticide bans and regulatory restrictions have been shown to be effective strategies for preventing suicide in several countries. Suicide and suicide by pesticides have decreased significantly in China over the past two decades. However, whether the reduction was associated with pesticide regulation is unknown.
Methods: The monthly data on suicide and suicide by pesticide from 2006 to 2018 were obtained from China's Disease Surveillance Point (DSP) system. Information on China's pesticide regulations since 1970 was obtained from Pesticide Action Network International (PAN International), Joint Meeting on Pesticide Management Highly Hazardous Pesticides (JMPM HHP) lists, the website of the Ministry of Agriculture of China, Pesticide Information Network of China, and the Wan Fang database. Change point detection and policy analysis were combined to identify the time of any trend change breakpoint of suicide and suicide by pesticide. Interrupted time series analysis was used to investigate the pre- and post-breakpoint trends of monthly standardized rates in suicide and suicide by pesticide.
Results: The standardized pesticide suicide rate decreased by 60.5% from 6.50 in 2006 to 2.56 per 100,000 in 2018. Larger declines were evident among people in urban areas (67.3%), female individuals (63.5%), and people aged 15–44 years (68.1%). The effect of policies banning highly hazardous organophosphorus pesticides (HHOP) [rate ratio (RR) = 0.993, 95% CIs (0.991–0.994)] in December 2008 and stopping domestic sales and use of paraquat aqueous solution (RR = 0.992, 95% CIs: 0.990–0.994) in July 2016 were more pronounced than regulating the paraquat-related products (RR = 1.003, 95% CIs: 1.002–1.004) in April 2012.
Conclusion: Declines in suicide by pesticide in China occurred contemporaneously with regulatory bans and restrictions implemented on several pesticides, particularly in urban areas, among female individuals, and the relatively low age profile. These findings indicate the potential influence of these bans on trends of suicide by pesticides.
1. Introduction
Suicide is a serious and important global health problem. There were approximately 703,000 suicides worldwide in 2019 (an age-standardized rate of 9 per 100,000 people), accounting for 1.3% of all deaths and ranking as the 17th leading cause of death globally (1, 2). Importantly, 79% of these suicides occurred in low- and middle-income countries (3). To effectively address this issue, multi-sectoral organizations and relevant stakeholders have been encouraged to take concerted action through comprehensive national strategies and measures (4–6). The World Health Organization's (WHO) Comprehensive Mental Health Action Plan 2013–2030 and Sustainable Development Goal 3 (target 3.4 and indicator 3.4.2) set out the global goal of reducing suicide rates by one-third by 2030 (3, 7).
Despite declines in the rate of suicide in the past two decades, the number of suicides in China is still very large compared to the rest of the world (3, 8–12). Research suggests that a substantial proportion of suicidal acts in China are impulsive, following acute psychosocial stress or crisis (13). The leading method of suicide in China is pesticide poisoning, accounting for approximately half of all suicide deaths (9, 14). It is widely recognized that one of the most effective approaches for preventing suicide is restricting the availability of commonly used, high-lethality methods (15). In countries where pesticides account for a high proportion of suicides, such as China, the WHO, and the Food and Agriculture Organization of the United Nations (FAO) currently recommend the pesticide regulator identify, and withdraw from the sale, the pesticides most commonly used in fatal self-poisoning (16). These recommendations are supported by a systematic review of the impact of pesticide bans on suicides by pesticide poisoning as well as overall suicide rates, which is best exemplified by evaluations of bans in South Korea and Sri Lanka, which have both enacted bans on highly hazardous pesticides in recent years (17–19). Cost-effectiveness analysis shows that national bans of highly hazardous pesticides are highly cost-effective for reducing suicide by pesticides (20).
In China, pesticide regulation began in the 1970s (Table 1) (21). Local evaluations on the association between pesticide exposure and suicide attempt patterns have been undertaken in several provinces in China (22–25). The impact of these bans has not been investigated at a national level. This study (1) collates information on the array of pesticide bans and regulatory changes since 1970 and (2) investigates the association between pesticide bans and regulations on national trends of suicide in China.
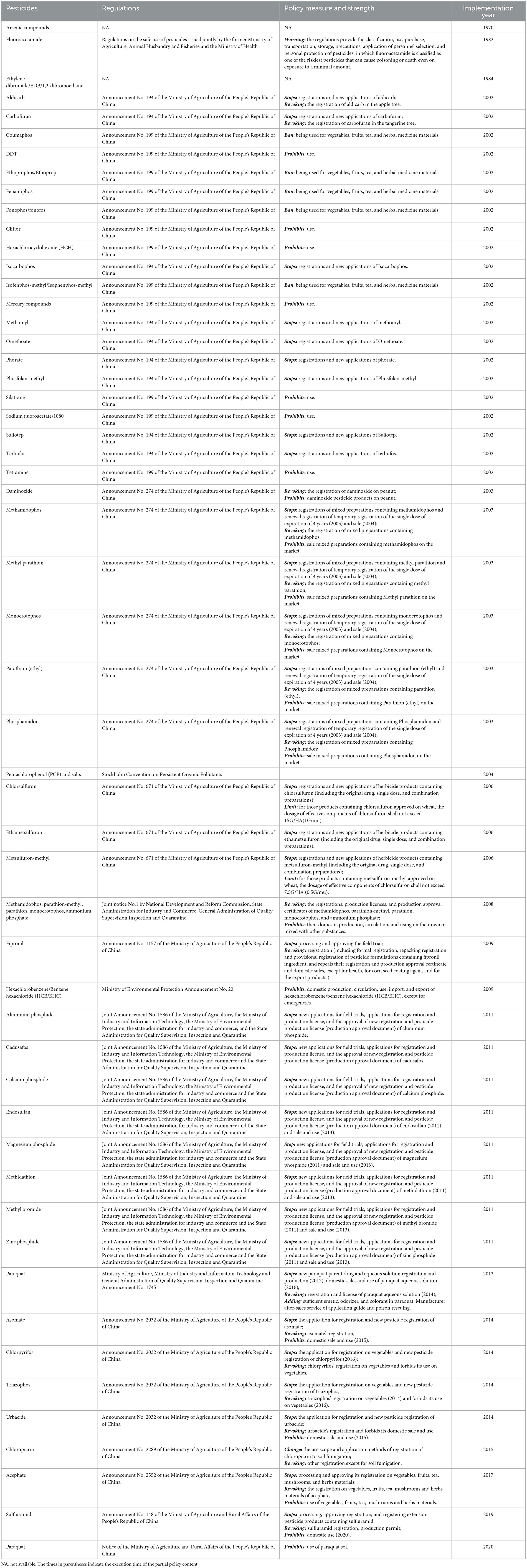
Table 1. Banned or restricted pesticides and issued years in China.
2. Materials and methods
2.1. Suicide and population data
Suicide data were obtained from the China National Disease Surveillance Point (DSP) system for the period 2006–2018. The DSP system of cause-of-death data developed into a national and regionally representative sample vital registration system in 1990 with 145 DSPs. In 2004, the number of DSPs increased from 145 to 161, and the cause-of-death data were collected through a household survey before being reported to the local CDC. In 2013, the DSP system further expanded and the number of DSPs increased to 605, covering approximately 24% of the Chinese people with provincial representativeness (26). Cases of death in the DSP system are collected from hospitals and from household surveys to capture non-hospital deaths. All the data obtained are exchanged and certified with relevant departments, including civil affairs, public security, and the maternal and child healthcare sector (26, 27). In this study, 158 DSPs that are consistent in the surveillance system from January 2006 to December 2018 were included in the analysis (with 3 DSPs excluded since 2013). Population data were derived from the National Statistical Bureau of China, and suicide rates were age-standardized using the standard population of China's 2010 census. Suicide counts in this study were defined based on the International Classification of Diseases 10th Revision (ICD-10) codes X60-X84, Y10-Y34, W75-W76, and X48. ICD-10 codes for counts of suicide by pesticide were X68 (intentional pesticide suicide), X48 (accidental pesticide suicide), and Y18 (intentional unknown pesticide suicide). Deaths by accidental pesticide (X48) poisoning were also included, as research indicates many of these deaths may be missed suicides (28).
2.2. Pesticide regulation data
Data on China's pesticide bans and regulations were collated using several sources. The key source was data from the Pesticide Action Network International (PAN International) (29–31). Information was also obtained from the FAO/WHO Joint Meeting on Pesticide Management Highly Hazardous Pesticide (JMPM HHP) lists (31). The website of the Ministry of Agriculture of China, the China Pesticide Information Network, and the Wan Fang database were used as additional sources as well as the personal notes of one of the authors (CJT). The search period for pesticide bans and regulations related to the earliest available period (1970) to 31 December 2021.
2.3. Definition of the intervention point
The intervention points were defined by combined change point detection (CPD) and content analysis of the pesticide policy. Altogether, 54 pesticides have been banned and restricted in China since 1970, with almost half [n = 24 (44.4%)] of them being banned or restricted in 2002 (Table 1). However, for many of the key highly hazardous organophosphorus pesticides (HHOP) used for self-harm, the years 2002–2004 represented only restrictions on registration. The pesticides were available (although at likely lower levels) for agriculture until their ultimate ban in December 2008. Therefore, December 2008 was defined as the primary intervention point for subsequent time-series models. The CPD method estimates the model by fitting iteratively the linear model and was implemented by the segmented package in R (32, 33) and explored the monthly location of suicide by pesticides breakpoints, assuming that 1–4 breakpoints existed in 2006–2018 (Appendix Table 1). Considering the content of the policy and its implementation, we identified the potentially effective policies, including banning HHOP in December 2008, stopping registration and production of new paraquat parent drug and aqueous solutions, regulating the existing paraquat production and after-sales services in April 2012, and stopping domestic sales and use of paraquat aqueous solution in July 2016. We analyzed the three breakpoints corresponding to the abovementioned policies (Table 1).
2.4. Statistical analysis
An interrupted time series (ITS) regression method was used in this study to evaluate the impact of the enactment of pesticide regulations on suicide in China (34–36). Our null hypothesis was that the intervention point was not associated with any changes in suicides by pesticide among adults aged 15 years and older in China. Segmented regression analysis was conducted for the analysis of three intervention policies (37). Generalized least squares method and fitting linear segmented model (function gls in R package nlme) were used to investigate the relationship between the standardized monthly number of deaths, interventions, and time (38). We considered January 2006 as the starting time, December 2008 as intervention 1, April 2012 as intervention 2, and July 2016 as intervention 3 to investigate whether trends of suicide changed after the pesticide regulations. The final regression equation is as follows:
where St is the standardized monthly suicide number in time t, peoplet is the number of standard population (in person-years) with log-transformed and was used as an offset term in time t, β0 is the intercept, time is the corresponding month and year calculated in cumulative months, and β1 represents the underlying pre-intervention trend. intervention1, intervention2, and intervention3 were coded as a binary variable to reflect the pesticide policy enactment (pre-intervention period: 0; began and post-intervention period: 1), and the corresponding regression coefficients β2, β4, and β6 indicate the level change and reflect the immediate effect following interventions 1–3, respectively. T1, T2, and T3 were the time points when interventions started. (time−T1)*intervention1, (time−T2)*intervention2, and t(time−T3)*intervention3 were interaction terms between intervention and year, and β3, β5, andβ7, respectively, indicate the slope change following the intervention. Fourier terms consisting of sine/cosine three pairs were used to adjust seasonal variations. εt is the error term.
We conducted two further analyses to evaluate the intervention effects. First, models were stratified to investigate any differences in trends by gender, the urbanization rate (≤ 45.14 vs. >45.14 %), age group, and the number of pesticide vs. non-pesticide suicides. The urbanization rate in all surveillance sites was dichotomized at the median as the cutoff point (high-urbanization rate sites as urban or low-urbanization rate sites as rural) based on China's 2010 census data. Age was categorized into three groups (15–44, 45–64, and ≥65 years old). Suicides involving methods other than pesticides were calculated by subtracting suicides by pesticide from suicides by all other methods. Second, due to the potential lag effect of the intervention, we repeated the ITS analysis in suicide by pesticide using the time lags between 1 and 18 months after introducing the policy in December 2008, April 2012, and July 2016, respectively.
We calculated the rate ratio (RR), the monthly percent change (MPC), the average monthly percent change (AMPC), and its 95% confidence intervals (CIs) for the periods pre-intervention and post-intervention. The details are found in the Appendix. The deseasonalized curve was used to depict the trend of change in suicide. We checked for autocorrelation by the autocorrelation function and the partial autocorrelation function (Appendix Figure 3). The model-selection strategies in this study were the smallest Bayesian Information Criterion (BIC) and optimal interpretability. R 4.1.2 software (R Foundation for Statistical Computing, Vienna, Austria, https://www.R-project.org/) was used for all statistical analyses.
3. Results
3.1. Overall trends
The age-standardized suicide rate in China showed a downward trend from 2006 to 2018 declining by 45.1% from 12.70 in 2006 to 6.98 per 100,000 in 2018 (Table 2). Similarly, the age-standardized pesticide suicide rate decreased by 60.5% from 6.50 in 2006 to 2.56 per 100,000 in 2018 and suicides using methods other than pesticides declined by 28.9% from 6.20 to 4.41 per 100,000 (Table 2). From 2006 to 2018, the proportional contribution of pesticide poisoning to total suicides decreased from 51.2 to 36.8% (Table 2, Appendix Table 2). The lag effect test showed that the trend of suicides by pesticide was significantly changed and tended to steepen after interventions 1 and 3 lagged from 0 to 14 and from 0 to 18 months, respectively, and tended to flatten after intervention 2 lagged from 0 to 6 months (Appendix Figure 1).
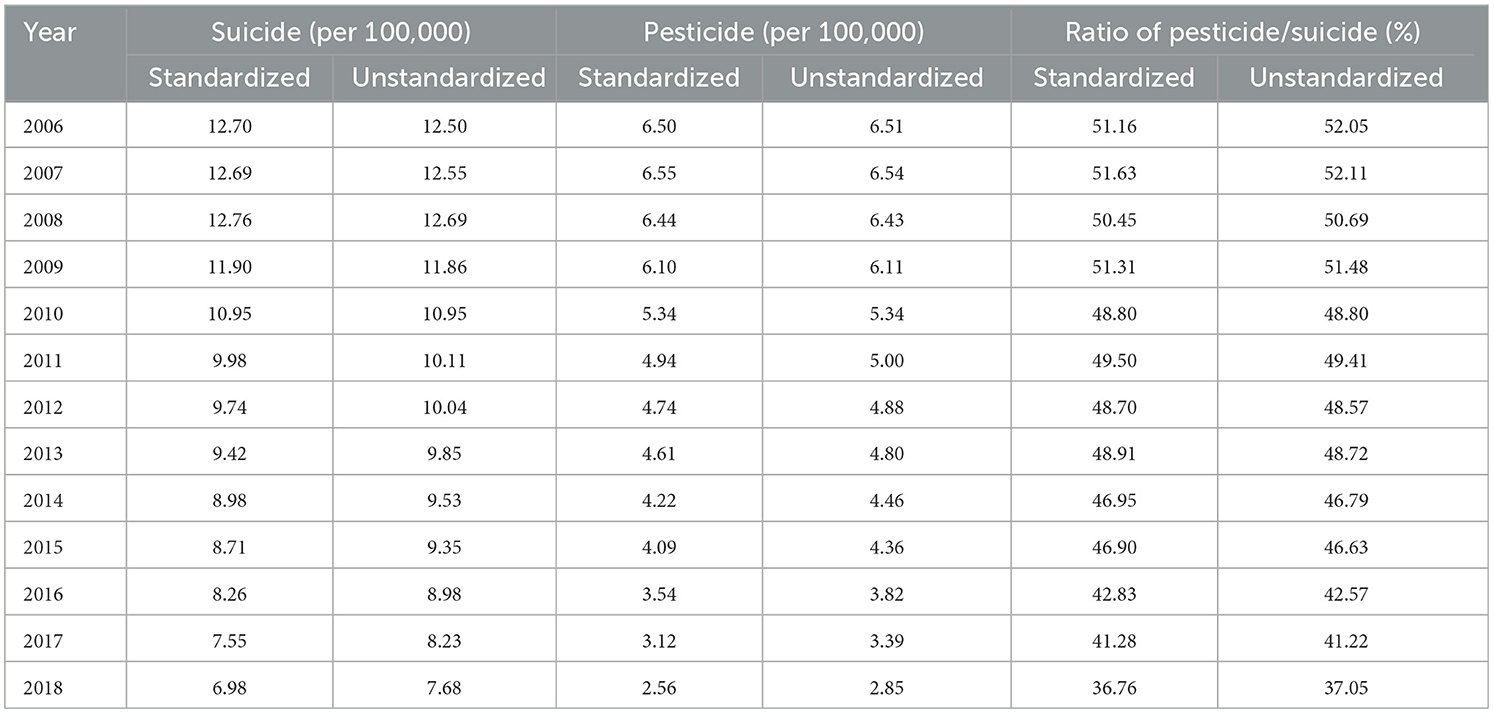
Table 2. Yearly suicide rate and pesticide suicide rates in China, 2006–2018.
Before the policy intervention period in December 2008, suicide by pesticide and non-pesticide MPC was not statistically significant, but a significant decrease was evident after December 2008, and the decreasing trend significantly flattened after the policy in April 2012 (Figure 2, Table 3, Appendix Table 3). After July 2016, the decreasing trend of suicide by pesticide became significantly steeper (RR = 0.992, 95% CIs: 0.990–0.994), while the trend change in suicide by non-pesticide methods was not significant (RR = 0.999, 95% CIs: 0.997–1.001) (Figure 2, Table 3, Appendix Table 3).
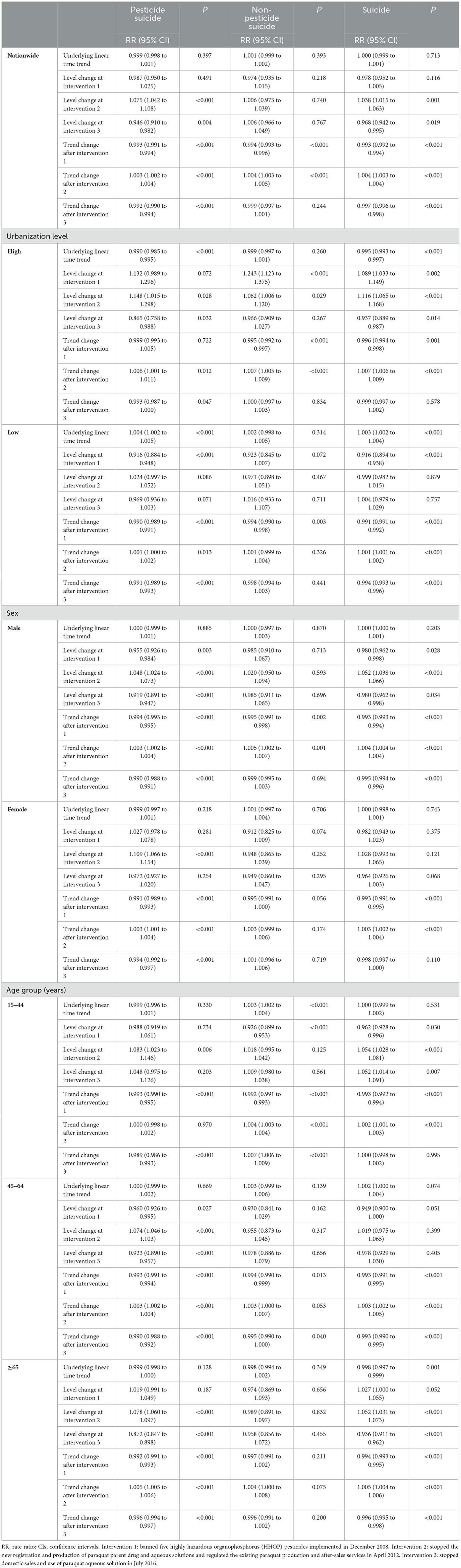
Table 3. Slope and level changes for suicide, pesticide suicide, and non-pesticide suicide rate ratio before and after pesticide bans in December 2008, April 2012, and July 2016.
3.2. Trends by sex
The standardized suicide rate for male and female individuals decreased by 40.6 and 50.8% from 14.15 and 11.22 per 100,000 in 2006 to 8.41 and 5.53 per 100,000 in 2018. At the same time, the rate of suicide by pesticide for male and female individuals decreased by 57.7 and 63.5%, respectively, from 2006 to 2018, from 6.66 to 2.82 per 100,000 for male individuals and from 6.33 to 2.31 per 100,000. Before the policy intervention (December 2008), the MPC in suicide by pesticides among male and female individuals was not statistically significant, but a significant decrease (male individuals: MPC = −0.6, 95% CIs: −0.8 to −0.5; female individuals: MPC = −1.0, 95% CIs: −1.2 to −0.8) was evident after December 2008 (male individuals: RR = 0.994, 95% CIs: 0.993–0.995; female individuals: RR = 0.991, 95% CIs: 0.989–0.993). The trend of suicide by pesticide tended to be flat and was significant in both male and female individuals after the intervention in April 2012 (male individuals: RR = 1.003, 95% CIs: 1.002–1.004; female individuals: RR = 1.003, 95% CIs: 1.001–1.004). After the intervention in July 2016, suicide by pesticide fell significantly in both male individuals and female individuals (male individuals: RR = 0.990, 95% CIs: 0.988–0.991; female individuals: RR = 0.994, 95% CIs: 0.992–0.997). However, the trend change in suicide by the non-pesticide method was significant only for male individuals, with a significant decrease after the intervention in December 2008 and a tendency to slow down after April 2012 (Table 3, Figures 1, 2, Appendix Table 3).
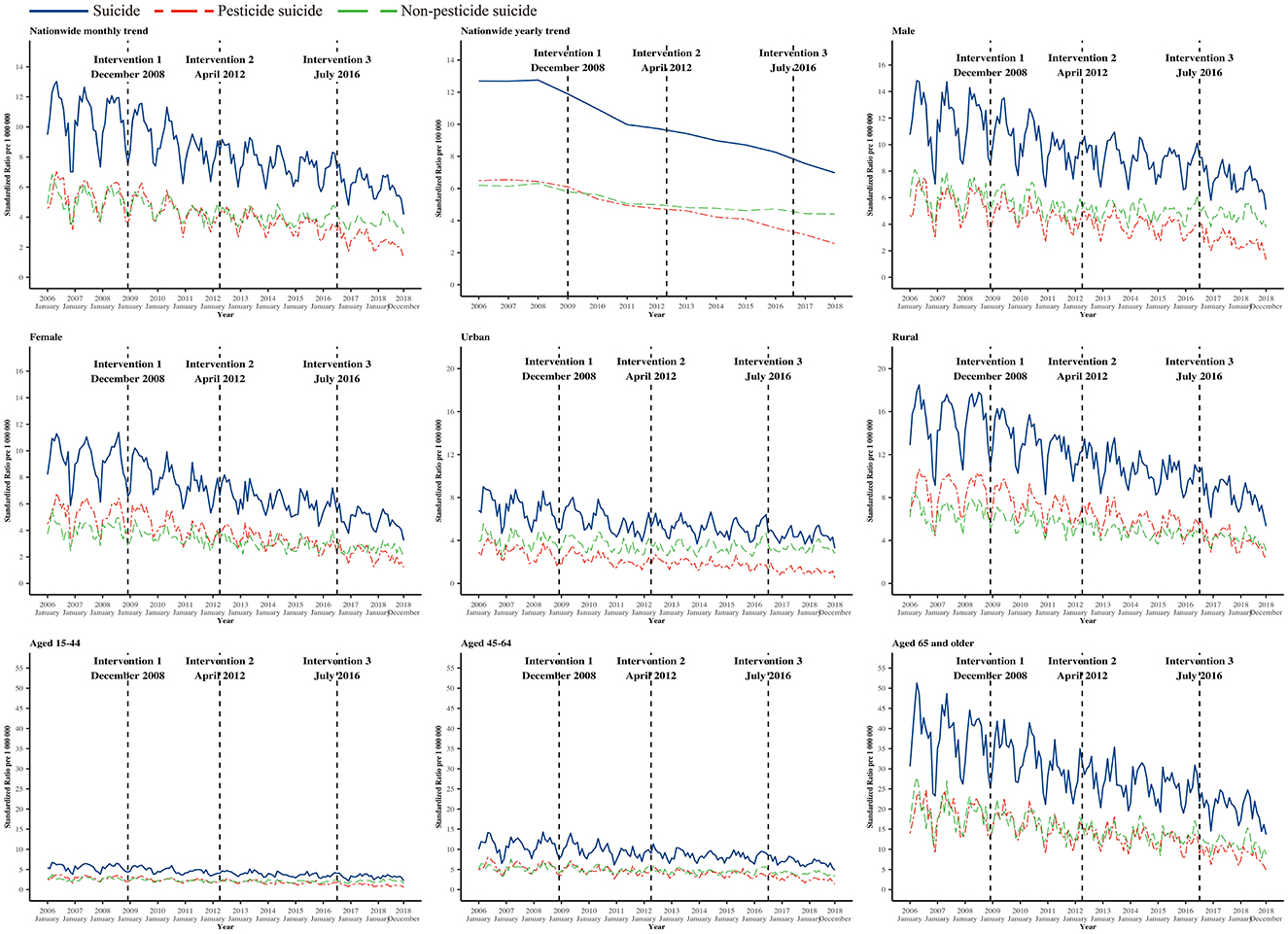
Figure 1. Trend of monthly suicide, pesticide suicide, and non-pesticide suicide rate in China from January 2006 to December 2018. Intervention 1: banned five highly hazardous organophosphorus (HHOP) pesticides implemented in December 2008. Intervention 2: stopped the new registration and production of paraquat parent drug and aqueous solutions and regulated the existing paraquat production and after-sales services in April 2012. Intervention 3: stopped domestic sales and use of paraquat aqueous solution in July 2016.
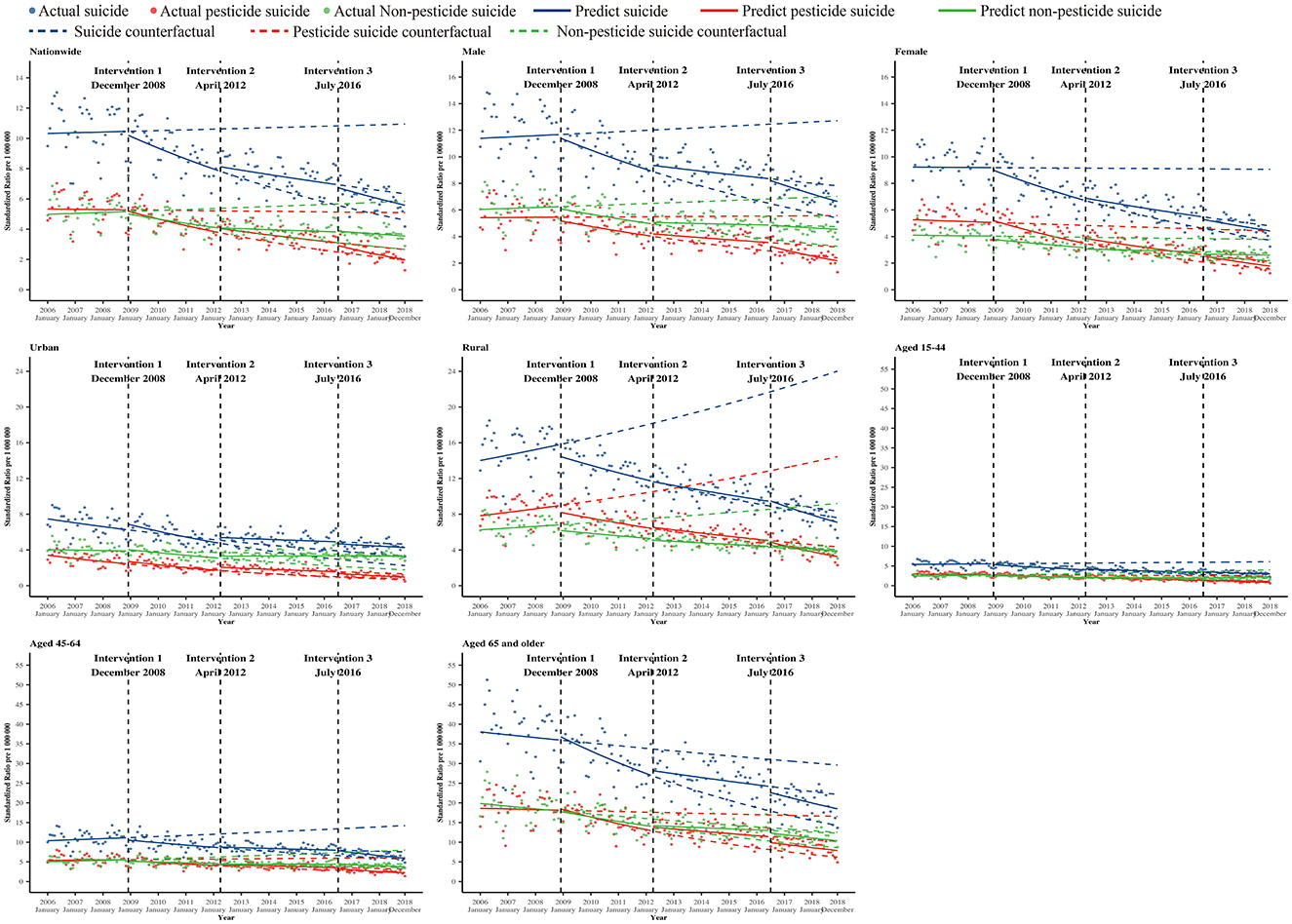
Figure 2. The isolated trend cycle curve was smoothed of monthly suicide, pesticide suicide, and non-pesticide suicide rate after excluding the seasonal variations, including the counterfactual in China from January 2006 to December 2018. Intervention 1: banned five highly hazardous organophosphorus (HHOP) pesticides implemented in December 2008. Intervention 2: stopped the new registration and production of paraquat parent drug and aqueous solutions and regulated the existing paraquat production and after-sales services in April 2012. Intervention 3: stopped domestic sales and use of paraquat aqueous solution in July 2016.
3.3. Trends by age group
The standardized rate of suicide among those aged 15–44, 45–65, and ≥65 years declined by 43.5, 40.9, and 49.7%, respectively, from 6.68, 13.01, and 45.80 per 100,000 in 2006 to 3.78, 7.70, and 23.03 per 100,000 in 2018. At the same time, the rate of suicide by pesticide for people aged 15–44, 45–64, and ≥65 years also declined by 68.1, 57.4, and 56.4%, from 3.55, 6.83, and 22.23 per 100,000 in 2006 to 1.13, 2.91, and 9.69 per 100,000 in 2018. Before the policy intervention in December 2008, the changes in the rate of suicide by pesticide, the non-pesticide suicide rate, and the suicide rate in all age groups were not statistically significant. However, after the policy intervention in December 2008, the changes in the rate of suicide by pesticides for all age groups were statistically significant, with MPC −0.9 (95% CIs: −1.1 to −0.6), −0.7 (95% CIs: −0.8 to −0.6), and −0.9 (95% CIs: −1.0 to −0.8), respectively. After the intervention in April 2012, the change was significant in those aged 45–64 years and aged 65 years and older, and the trend tended to be flat (aged 15–44 years: RR=1.000, 95% CIs: 0.998–1.002; aged 45–64 years: RR = 1.003, 95% CIs: 1.002 to 1.004; aged 65 years and older: RR = 1.005, 95% CIs: 1.005 to 1.006). After the intervention in July 2016, the trend was decreasing and significant in all age groups. Meanwhile, the non-pesticide suicide rate significantly decreased in those aged 15–44 and 45–64 years after the intervention in December 2008, the trend change tended to flat significant only in those aged 15–44 years after the intervention in April 2012 and July 2016. All changes in suicide by non-pesticide for those aged 65 years and older were not significant after interventions 1, 2, and 3 (Table 3, Figures 1, 2, Appendix Table 3).
3.4. Trends by the urbanization level
The age-standardized rate in areas of low urbanization decreased by 48.6% from 17.68 per 100,000 in 2006 to 9.08 per 100,000 in 2018. Age-standardized rates decreased by 39.4% from 8.77 per 100,000 in 2006 to 5.31 per 100,000 in 2018 in areas of high urbanization. The rate of suicide by pesticides in low- and high-urbanization rate areas declined by 57.2 and 67.3%, respectively, from 9.82 and 3.87 per 100,000 in 2006 to 4.21 and 1.27 per 100,000 in 2018. Before the policy intervention (December 2008), the underlying trend showed a significant decrease with MPC of −1.0 (95% CIs: −1.5 to −0.5) in the pesticide suicide rate in high-urbanization areas (RR = 0.990, 95% CIs: 0.985–0.995), a significant increase with MPC of 0.4 (95% CIs: 0.2–0.5) in the pesticide suicide rate in low-urbanization areas (RR = 1.004, 95% CIs: 1.002–1.005), and no significant change in non-pesticide rate in high- and low-urbanization areas. In contrast, following the intervention in December 2008, a decrease in the rate of suicide by pesticide was evident in low-urbanization areas (RR = 0.990, 95% CIs: 0.989–0.991). After the intervention in April 2012, there was no change in the trend of suicide by pesticide change in low-urbanization areas but increased in high-urbanization areas (high-urbanization areas: RR = 1.006, 95% CIs: 1.001–1.011; low-urbanization areas: RR = 1.001, 95% CIs: 1.000–1.002). After the intervention in July 2016, the trend changed significantly and fell more steeply in low-urbanization areas (high-urbanization areas: RR = 0.993, 95% CIs: 0.987–1.000; low-urbanization areas: RR = 0.991, 95% CIs: 0.989–0.993). During the same period, the underlying trend change in suicide by non-pesticide was not significant. The decreasing trend tended to be steeper in high- and low-urbanization areas only after the intervention in December 2008, and the decreasing trend tended to be flattened in high-urbanization areas after the intervention in April 2012 (Table 3, Figures 1, 2, Appendix Table 3).
4. Discussion
This study showed that China's regulations of banning and restricting pesticides were associated with significant contemporaneous declines in total suicide from 2006 to 2018, largely due to reductions in suicide by pesticide poisoning. A decline in total suicide and suicide by pesticide was evident in the period after the policy intervention in December 2008 (when HHOP pesticides were fully banned rather than restricted in use), with a flat decreasing trend after the policy intervention in April 2012 (when the new registration and production of paraquat parent drug and aqueous solution stopped and the existing paraquat production and after-sales services were regulated), and a steep decreasing trend after the policy intervention in July 2016 (when paraquat aqueous solutions were entirely banned rather than restricted in use). The decreases were more prominent in people living in urban areas, among female individuals, and people aged 15–44 years. Meanwhile, a lagged analysis suggests an increase in the association after the implementation of China's pesticide regulations in July 2016.
A study from South Korea also showed that the impact of a pesticide (paraquat) ban was more significant for both men and the elderly on suicide prevention and control, but the study only observed the short-term association over a 2-year follow-up period (19). Qin et al. conducted research to explore the suicide rate change trend in Inner Mongolia of China between 2008 and 2015 (25). The findings showed that suicide rates were higher in 2008–2011 than in 2012–2015, a period prior to the implementation of pesticide regulations in this region in 2011 (25). Chang et al. evaluated the trends of suicide by pesticide poisoning before and after paraquat ban implementation in Taiwan from 2011 to 2019 (39). The result showed that pesticide and paraquat suicides in the whole population substantially reduced with the paraquat ban implementation. Jiang et al. (40) found that, during the period 2002 to 2015, there is a significant drop in suicide rates in China. However, the overall suicide rate showed a slower pace after 2006 (40). Liu et al. concentrated on the trends of the suicide rate and the pesticide self-poisoning suicide rate in rural China from 2009 to 2014 (41). Given the inconsistent time periods and locations of these several studies, we were unable to compare the trend and speed of the national suicide rate decline. The current study extends this regional study (25, 39) and is based on an assessment of national pesticide regulations over a longer period and evaluates whether there were any contemporaneous declines in suicide over a much longer period and the first-time studied paraquat pesticide policies' effect on suicide in mainland China.
Similar to the research performed in other countries (42, 43), the obvious seasonality of suicide and pesticide suicide in China was present in our study, with the suicide rate peaking in spring and declining in winter (43), although seasonality tended to diminish (44). Between 2006 and 2018, the rate of suicide by pesticides in China declined at an average annual rate of 4.7%, with 4.4, 4.4, and 5.2% for male individuals, people living in rural areas, and people aged 15–44 years, respectively. At present, the suicide rate of male individuals in China is still higher than that of female individuals and remains much higher in rural areas than in urban areas (14). Considering that the suicide rate in China has declined dramatically over the past for more than a decade and the proportion of suicide by pesticides dropped from over half to approximately a third, we consider the pesticide ban and restriction policy to have been implemented effectively in reducing the burden of suicide.
Our findings suggest that the potential impact of pesticide prohibition and restriction on suicide by pesticide was greater in rural areas. Simultaneously, the reduction in suicide by the non-pesticide method implies that the trend change in this period may be attributed to natural variation or other non-pesticide national suicide intervention policies, but the natural variation assumption can be discredited by comparing urban areas with rural areas and male suicide changes with female suicide changes. Moreover, the trend showed a different shift in the suicide and non-pesticide suicide groups. The association can be observed after the policy of banning and restricting pesticides was introduced intensively after December 2008, as the intervention point, when the five important HHOPs (methamidophos, monocrotophos, methyl parathion, parathion, and ammonium phosphate) were wholly removed from the market in China (45). Before 2008, the prohibition and restriction policies on these high-toxicity pesticides had focused on revoking the relevant certificates of production, sale, and use (46, 47), which implies that it was only in 2008 that these organophosphorus pesticides were removed entirely from the Chinese market. Therefore, it is likely that the policy of banning and restricting the sale and use of pesticides had lagged impacts on the prevention of suicide by pesticides in the period post-2008, which was consistent with the stronger association evident in the lagged analysis in this current study.
Our results showed an unlikely effect of the regulated paraquat-related product in April 2012. The trend of suicide by pesticide tended to slow down significantly. Compared with the non-pesticide suicide group, a similar trend changed in both groups, prompting us to infer that a risk factor of suicide flattened the decrease of suicide, and even in rural areas where the intervention effect was more evident, the policy restriction effect may be masked by the risk factor. China has the largest periodically floating population of individuals migrating from rural to urban regions, who tend to have low socioeconomic and health status (48). The inter-provincial migrants increased to the highest level in 2012 and faced more life challenges than others (49, 50). We hypothesize that the social phenomenon of migration influenced suicide and suicide by pesticides in China, particularly in 2012. However, stopping domestic sales and the use of paraquat aqueous solutions in July 2016 effectively decreased suicide by pesticide.
China is the world's largest pesticide user, is the second-largest pesticide producer, and has the largest agricultural population. Many suicides in China are believed to be impulsive as a reaction to acute psychological distress (13); the availability of highly hazardous pesticides facilitates such impulsive suicides (making low-intent acts of self-poisoning lethal). Research from other countries indicates regulations banning highly toxic pesticide regulations can lead to falls in method-specific and, in some cases (e.g., Sri Lanka, Bangladesh, South Korea, and China Taiwan), overall suicides (39, 51). Page et al. analyzed the national suicide mortality trends of China from 2006 to 2013 and found that hanging, as a proportion of all suicides, increased from 27 to 31%, while the contribution of pesticide poisoning to total suicides declined from 55 to 49%, although the absolute numbers of suicides using both methods reduced substantially (9). The current study also found that the proportion of suicide by pesticide has decreased in recent decades. The results of this study are consistent with those from previous studies and further provide evidence for timely and effective intervention in low- and middle-income countries where suicide by pesticide remains the main method of suicide.
In order to improve the quality and safety of agricultural products and reduce environmental pollution, the production, use, and trade of high-toxic and high-risk pesticides is increasingly controlled worldwide. The formulation and implementation of pesticide bans and policies of restriction is a process of multi-sectoral integration and cooperation with relevant stakeholders. This multi-sectoral collaboration is indispensable in the context of suicide prevention. Since the Stockholm Convention on Persistent Organic Pollutants (POPs) was signed by the Chinese delegation comprising representatives from the Ministry of Health, the Ministry of Agriculture, the State Economic and Trade Commission, and the General Administration of Environmental Protection in 2002, China's pesticide ban and restriction has been much strengthened, institutionalized, and standardized (45, 52). With the introduction of a series of prohibition and restriction policies, the Ministry of Agriculture has intensified the research and development of low-toxic biological pesticides.
One key strength of this study was the use of a 15-year period of monthly suicide data collected by the DSP system, a continuous and consistent source of data that included certification of death with relevant local departments (civil affairs, public security, and the maternal and child healthcare sector) (26). This strongly supports the accessibility, comprehensiveness, and quality of suicide information in China (27). Another strength of our study concerns the comprehensive analyses of the effect on multiple key pesticide policies to avoid pesticide suicide decrease misattributed to concerned ban but neglected potential policy or elusive factor effects; thus, we further discussed the pesticides policies on suicide and non-pesticide suicide. Additionally, an ITS analysis was designed to evaluate the trends of population-level intervention (34), including at various lag periods, which accounted for seasonality and autocorrelation in time series.
This study had some limitations. First, similar to all other surveillance systems worldwide, the problem of accuracy and completeness is inevitable in the DSP system, where the potential sources of system bias remain. The surveillance data included in the analysis also did not adjust for potential under-reporting of suicide, which may cause information bias (11). However, its impact on trend analysis would be small. Second, the primary purpose of this study was to evaluate the single pesticide policy effect, but multiple policy efforts to ban different pesticides occurred at different time points during 2006–2021. Despite the substantial evidence collected, the performance of these policies and the effect between these policies could not be definitely determined. Furthermore, the multiple interventions also make it challenging to define the intervention time points in the interrupted time series regression analysis. Our approach to define the intervention time points was informed by the change point detection method implemented by segmented regression, and this may potentially lead to false positive findings in the interrupted time series regression analysis, although our final decision of the intervention time points was based on an analysis of the content of the pesticide ban policies. Third, only 2 years of suicide data are available before the HHOP pesticides ban in 2008 in our analyses, even though no specific number of time points was demanded, a short pre-intervention period may raise the uncertainty in the post-intervention trend judgment (34, 36), but the monthly data would make up for this deficiency, to a certain extent. Fourth, ITS analysis is a quasi-experimental design method that assumes the omitted variable effect consistent across the study period; however, the facts may be different (12).
5. Conclusion
Recent declines in suicide in China occurred contemporaneously with regulatory bans and restrictions on five key HHOPS in 2008 and a paraquat aqueous solution ban in 2016. Similar declines were observed for suicide by pesticide poisoning and for suicides using other methods since 2008. Larger declines were observed for suicide by pesticide poisoning than that for suicides using other methods, indicating the potential influence of pesticide bans on pesticide suicide trends since 2008.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
SL designed and supervised the study. YY, YJ, and RL analyzed the data and wrote the first draft. All authors have interpreted the data and contributed to intellectual content.
Funding
This study was supported by Beihang University and Capital Medical University Advanced Innovation Center for Big Data-Based Precision Medicine Plan [No. BHME-201901]. The Centre for Pesticide Suicide Prevention is funded by a grant from Open Philanthropy, at the recommendation of GiveWell, USA.
Acknowledgments
The authors are grateful to Professor David Gunnell from the National Institute for Health Research Biomedical Research Centre, University Hospitals Bristol NHS Foundation Trust, and the University of Bristol for advice and discussion regarding the data analysis and manuscript draft. The authors thank all staff from CDCs at all levels for their great contribution to data collection, auditing, and database management. As a Chinese partner of PAN, Pesticide Eco Alternative Center (PEAC) assisted this study in obtaining data on pesticide bans and restrictions in China.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1189923/full#supplementary-material
References
1. WHO. Suicide worldwide in 2019. (2021). Available online at: https://www.who.int/publications/i/item/9789240026643 (accessed June 16, 2021).
2. WHO. Summary tables of mortality estimates by cause, age and sex, globally and by region. (2000–2019). Available online at: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed August 24, 2023).
3. WHO. SDG Target 3.4 Reduce by one third premature mortality from non-communicable diseases through prevention and treatment and promote mental health and well-being. Available online at: https://www.who.int/data/gho/data/themes/topics/sdg-target-3_4-noncommunicable-diseases-and-mental-health (accessed August 24, 2023).
5. D'Anci KE, Uhl S, Giradi G, Martin C. Treatments for the prevention and management of suicide: a systematic review. Ann Intern Med. (2019) 171:334–42. doi: 10.7326/M19-0869
6. WHO. LIVE LIFE: An implementation guide for suicide prevention in countries. (2021). Available online at: https://www.who.int/publications/i/item/9789240026629 (accessed June 17, 2021).
7. WHO. Comprehensive Mental Health Action Plan 2013-2030. (2021). Available online at: https://www.who.int/publications/i/item/9789240031029 (accessed September 21, 2021).
8. Yang G, Wang Y, Zeng Y, Gao GF, Liang X, Zhou M, et al. Rapid health transition in China, 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet. (2013) 381:1987–2015. doi: 10.1016/S0140-6736(13)61097-1
9. Page A, Liu S, Gunnell D, Astell-Burt T, Feng X, Wang L, et al. Suicide by pesticide poisoning remains a priority for suicide prevention in China: Analysis of national mortality trends 2006-2013. J Affect Disord. (2017) 208:418–23. doi: 10.1016/j.jad.2016.10.047
10. Yip PS, Liu KY, Hu J, Song XM. Suicide rates in China during a decade of rapid social changes. Soc Psychiatry Psychiatr Epidemiol. (2005) 40:792–8. doi: 10.1007/s00127-005-0952-8
11. Liu S, Page A, Yin P, Astell-Burt T, Feng X, Liu Y, et al. Spatiotemporal variation and social determinants of suicide in China, 2006-2012: findings from a nationally representative mortality surveillance system. Psychol Med. (2015) 45:3259–68. doi: 10.1017/S0033291715001269
12. Cai Z, Chen M, Ye P, Yip PSF. Socio-economic determinants of suicide rates in transforming China: A spatial-temporal analysis from 1990 to 2015. Lancet Reg Health West Pac. (2022) 19:100341. doi: 10.1016/j.lanwpc.2021.100341
13. Conner KR, Phillips MR, Meldrum S, Knox KL, Zhang Y, Yang G. Low-planned suicides in China. Psychol Med. (2005) 35:1197–204. doi: 10.1017/S003329170500454X
14. Wang L, Wu Y, Yin P, Cheng P, Liu Y, Schwebel DC, et al. Poisoning deaths in China, 2006-2016. Bull World Health Organ. (2018) 96:314–26A. doi: 10.2471/BLT.17.203943
15. Zalsman G, Hawton K, Wasserman D, van Heeringen K, Arensman E, Sarchiapone M, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiat. (2016) 3:646–59. doi: 10.1016/S2215-0366(16)30030-X
16. WHO FAO. Preventing suicide: a resource for pesticide registrars regulators. (2019). Available online at: https://apps.who.int/iris/bitstream/handle/10665/326947/9789241516389-eng.pdf (accessed August 24, 2023).
17. Gunnell D, Knipe D, Chang S-S, Pearson M, Konradsen F, Lee WJ, et al. Prevention of suicide with regulations aimed at restricting access to highly hazardous pesticides: a systematic review of the international evidence. Lancet Global Health. (2017) 5:e1026–e37. doi: 10.1016/S2214-109X(17)30299-1
18. Gunnell D, Fernando R, Hewagama M, Priyangika WD, Konradsen F, Eddleston M. The impact of pesticide regulations on suicide in Sri Lanka. Int J Epidemiol. (2007) 36:1235–42. doi: 10.1093/ije/dym164
19. Cha ES, Chang SS, Gunnell D, Eddleston M, Khang YH, Lee WJ. Impact of paraquat regulation on suicide in South Korea. Int J Epidemiol. (2016) 45:470–9. doi: 10.1093/ije/dyv304
20. Lee YY, Chisholm D, Eddleston M, Gunnell D, Fleischmann A, Konradsen F, et al. The cost-effectiveness of banning highly hazardous pesticides to prevent suicides due to pesticide self-ingestion across 14 countries: an economic modelling study. The Lancet Global Health. (2021) 9:e291–300. doi: 10.1016/S2214-109X(20)30493-9
21. Liu L, Sun Y, Zhou W. Implementation and proposal of management policy for banned and restricted pesticides in china pesticide science and administration. Pestic Sci Admin. (2013) 34:1–4.
22. Zhu RT, Ma Z, Jia C, Zhou L. Suicide means used by the older adults in rural china: a comparison between those using pesticides and other means. J Geriatr Psychiatry Neurol. (2019) 32:319–26. doi: 10.1177/0891988719862625
23. Zhang M, Fang X, Zhou L, Su L, Zheng J, Jin M, et al. Pesticide poisoning in Zhejiang, China: a retrospective analysis of adult cases registration by occupational disease surveillance and reporting systems from 2006 to 2010. BMJ Open. (2013) 3:e003510. doi: 10.1136/bmjopen-2013-003510
24. Zhang J, Stewart R, Phillips M, Shi Q, Prince M. Pesticide exposure and suicidal ideation in rural communities in Zhejiang province, China. Bull World Health Organ. (2009) 87:745–53. doi: 10.2471/BLT.08.054122
25. Qin P, Du M, Wang S, Zhang X, Wang Y, Yan T, et al. The waterfall pattern of suicide mortality in Inner Mongolia for 2008-2015. J Affect Disord. (2019) 256:331–6. doi: 10.1016/j.jad.2019.05.057
26. Liu S, Wu X, Lopez AD, Wang L, Cai Y, Page A, et al. An integrated national mortality surveillance system for death registration and mortality surveillance, China. Bull World Health Organ. (2016) 94:46–57. doi: 10.2471/BLT.15.153148
27. Sha F, Chang Q, Law YW, Hong Q, Yip PSF. Suicide rates in China, 2004-2014: comparing data from two sample-based mortality surveillance systems. BMC Public Health. (2018) 18:239. doi: 10.1186/s12889-018-5161-y
28. Chang SS, Sterne JA, Lu TH, Gunnell D. ‘Hidden' suicides amongst deaths certified as undetermined intent, accident by pesticide poisoning and accident by suffocation in Taiwan. Soc Psychiatry Psychiatr Epidemiol. (2010) 45:143–52. doi: 10.1007/s00127-009-0049-x
29. PAN. PAN International Consolidated List of Banned Pesticides. (2021). Available online at: https://files.panap.net/resources/Consolidated-List-of-Bans-Explanatory.pdf (accessed March 2021).
30. PAN. PAN International List of Highly Hazardous Pesticides. (2021). Available online at: https://pan-international.org/wp-content/uploads/PAN_HHP_List.pdf (accessed March 2021).
31. WHO FAO. Report of the 14th FAO/WHO joint meeting on pesticide management: 14–15 October 2021, virtual meeting. (2022). Available online at: https://www.who.int/publications/i/item/9789240039957 (accessed April 25, 2022).
32. Muggeo VM. Estimating regression models with unknown break-points. Stat Med. (2003) 22:3055–71. doi: 10.1002/sim.1545
33. Muggeo VM. Segmented: an R package to fit regression models with broken-line relationships. R news. (2008) 8:20–5.
34. Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol. (2017) 46:348–55. doi: 10.1093/ije/dyw098
35. Bhaskaran K, Gasparrini A, Hajat S, Smeeth L, Armstrong B. Time series regression studies in environmental epidemiology. Int J Epidemiol. (2013) 42:1187–95. doi: 10.1093/ije/dyt092
36. Lopez Bernal J, Soumerai S, Gasparrini A. A methodological framework for model selection in interrupted time series studies. J Clin Epidemiol. (2018) 103:82–91. doi: 10.1016/j.jclinepi.2018.05.026
37. Wagner AK, Soumerai SB, Zhang F, Ross-Degnan D. Segmented regression analysis of interrupted time series studies in medication use research. J Clin Pharm Ther. (2002) 27:299–309. doi: 10.1046/j.1365-2710.2002.00430.x
38. Fox J. Time-series regression and generalized least squares. In: An R S-PLUS Companion to Applied Regres. Thousand Oaks, CA (2002). p. 1–8.
39. Chang SS, Lin CY, Lee MB, Shen LJ, Gunnell D, Eddleston M. The early impact of paraquat ban on suicide in Taiwan. Clin Toxicol (Phila). (2022) 60:131–5. doi: 10.1080/15563650.2021.1937642
40. Jiang H, Niu L, Hahne J, Hu M, Fang J, Shen M, et al. Changing of suicide rates in China, 2002-2015. J Affect Disord. (2018) 240:165–70. doi: 10.1016/j.jad.2018.07.043
41. Liu Y, Lan Z, Yin Y, Liu NH, Tong Y. Trends in suicide rates and the case-fatality of pesticide self-poisoning in an agricultural county in china, 2009 to 2014. J Affect Disord. (2021) 283:52–9. doi: 10.1016/j.jad.2021.01.024
42. Woo JM, Okusaga O, Postolache TT. Seasonality of suicidal behavior. Int J Environ Res Public Health. (2012) 9:531–47. doi: 10.3390/ijerph9020531
43. Yu J, Yang D, Kim Y, Hashizume M, Gasparrini A, Armstrong B, et al. Seasonality of suicide: a multi-country multi-community observational study. Epidemiol Psychiatr Sci. (2020) 29:e163. doi: 10.1017/S2045796020000748
44. Ajdacic-Gross V, Bopp M, Ring M, Gutzwiller F, Rossler W. Seasonality in suicide–a review and search of new concepts for explaining the heterogeneous phenomena. Soc Sci Med. (2010) 71:657–66. doi: 10.1016/j.socscimed.2010.05.030
45. Liu JG, Hu JX, Tang XY. Preliminary identification of China's basic obligations and obstacles in fulfilling the Stockholm Convention. Legal Syst Manag. (2002) 8:23.
47. Ministry of Agriculture Rural Affairs of the People's Republic of China. Ministry of Agriculture and Other five Departments Jointly Banned Highly Toxic Rodenticides and Highly Toxic Pesticides. (2002). Available online at: http://www.moa.gov.cn/xw/zwdt/200212/t20021213_35585.htm (accessed August 24, 2023).
48. Hu X, Cook S, Salazar MA. Internal migration and health in China. Lancet. (2008) 372:1717–9. doi: 10.1016/S0140-6736(08)61360-4
49. Li B. Floating population or urban citizens? Status, social provision and circumstances of rural-urban migrants in China. Soc Policy Admin. (2006) 40:174–95. doi: 10.1111/j.1467-9515.2006.00483.x
50. Wang L, Xue C. Spatio-temporal characteristics and influencing factors of urban floating population in China from 2011 to 2015. Chin J Populat Resour Environ. (2019) 17:359–73. doi: 10.1080/10042857.2019.1628606
51. Karunarathne A, Gunnell D, Konradsen F, Eddleston M. How many premature deaths from pesticide suicide have occurred since the agricultural Green Revolution? Clin Toxicol (Phila). (2020) 58:227–32. doi: 10.1080/15563650.2019.1662433
52. Yu YF. China Environment Yearbook. China Ocean Press (2002). Available online at: https://data.cnki.net/yearBook/single?id=N2005120258 (accessed August 24, 2023).
Keywords: epidemiology, impact evaluation, pesticide, suicide, interrupted time series design
Citation: Yan Y, Jiang Y, Liu R, Eddleston M, Tao C, Page A, Wang L, Feng G and Liu S (2023) Impact of pesticide regulations on mortality from suicide by pesticide in China: an interrupted time series analysis. Front. Psychiatry 14:1189923. doi: 10.3389/fpsyt.2023.1189923
Received: 24 March 2023; Accepted: 08 August 2023;
Published: 04 September 2023.
Edited by:
S. M. Yasir Arafat, Enam Medical College, BangladeshReviewed by:
Ashish Bhalla, Post Graduate Institute of Medical Education and Research (PGIMER), IndiaXiang Dong Jian, Shandong University, China
Copyright © 2023 Yan, Jiang, Liu, Eddleston, Tao, Page, Wang, Feng and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shiwei Liu, shiwei_liu@aliyun.com; Guoshuang Feng, glxfgsh@163.com
†These authors have contributed equally to this work
‡ORCID: Rong Liu orcid.org/0000-0002-8609-5463