 Henrik Myhre Ihler1*
Henrik Myhre Ihler1* Siv Hege Lyngstad2
Siv Hege Lyngstad2 Lynn Egeland Mørch-Johnsen1,3
Lynn Egeland Mørch-Johnsen1,3 Trine Vik Lagerberg1
Trine Vik Lagerberg1 Ingrid Melle1
Ingrid Melle1 Kristin Lie Romm4
Kristin Lie Romm4- 1Norment, Division of Mental Health and Addiction, Oslo University Hospital, Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 2Nydalen DPS, Division of Mental Health and Addiction, Oslo University Hospital, Oslo, Norway
- 3Department of Psychiatry and Department of Clinical Research, Østfold Hospital, Grålum, Norway
- 4Early Intervention in Psychosis Advisory Unit for South-East Norway, Division of Mental Health and Addiction, Oslo University Hospital, Oslo, Norway
Background: Negative symptoms are increasingly recognized as transdiagnostic phenomena, linked to reduced quality of life and functioning, and often caused or worsened by amendable external factors such as depression, social deprivation, side-effects of antipsychotics or substance use. The structure of negative symptoms fits into two dimensions: diminished expression and apathy. These may differ in association with external factors that influence their severity and may thus require different treatment approaches. The dimensions are comprehensively established in non-affective psychotic disorders but are understudied in bipolar disorders.
Methods: We conducted exploratory and confirmatory factor analyses in a sample of 584 individuals with bipolar disorder to assess the latent factor structure of negative symptoms as measured by the Positive and Negative Syndrome Scale (PANSS), and performed correlational analyses and multiple hierarchical regression analyses to investigate links between the two dimensions of negative symptoms and clinical and sociodemographic correlates.
Results: The latent factor structure of negative symptoms fits into two dimensions, i.e., diminished expression and apathy. A diagnosis of bipolar type I or a history of psychotic episodes predicted more severe levels of diminished expression. Depressive symptoms were associated with more severe negative symptoms across dimensions, yet 26.3% of euthymic individuals still displayed at least one mild or more severe negative symptom (PANSS score ≥ 3).
Discussion: The two-dimensional structure of negative symptoms seen in non-affective psychotic disorders reproduces in bipolar disorders indicating similarities in their phenomenology. Diminished expression was associated with a history of psychotic episodes and a diagnosis of BD-I, which may infer closer connections to psychosis liability. We found significantly less severe negative symptoms in euthymic than depressed participants. Nevertheless, more than a quarter of the euthymic individuals had at least one mild negative symptom, demonstrating some degree of persistence beyond depressed states.
1. Introduction
Negative symptoms have been considered intrinsic to psychotic disorders and are part of the diagnostic criteria for schizophrenia spectrum disorders (SCZ), i.e., schizophrenia, schizophreniform disorder and schizoaffective disorder (1–3). The underlying neurobiological mechanisms of negative symptoms are largely unknown. Still, they are of increasing interest (4, 5), due to the strong associations with low remission rates, reduced quality of life and impaired functioning (6, 7). Recent developments in psychiatry have moved toward a dimensional rather than a categorical understanding of clinical symptoms and diagnoses (8, 9). Negative symptoms are thus not pathognomonic to any specific psychiatric or neurological disorder – despite their historical link to schizophrenia – and are regularly present in other psychiatric disorders, such as bipolar disorder (BD) (10). Previous estimates of negative symptoms’ prevalence vary significantly across diagnostic categories (10), and range from rare in healthy adults (11), to 20–89% in affective disorders, and 32–80% in neurological disorders (12), yet little is still known about prevalence and characteristics in subcategories of BD.
BD is usually categorized as an affective disorder (1–3), even if genetic, neuroimaging and clinical studies find significant overlaps with SCZ (13–16). As SCZ, BD is considered a severe mental disorder, associated with impairments in cognition and functioning, and a reduced quality of life (17–19). Furthermore, severe mental disorders share environmental risk factors including substance use, adverse life events, and early trauma (20, 21). Development into different clinical phenotypes may be based on individual combinations of these factors (20, 22). Positive psychotic symptoms are present in up to 70% of individuals with BD type I (BD-I) (23, 24). BD is thus often considered part of the psychosis spectrum continuum (23, 25). One problem with diagnostic categories is the potential to ignore or misinterpret relevant symptoms that occur across a diagnostic spectrum because the symptoms are seen as a criterion for a specific diagnosis (e.g., negative symptoms and schizophrenia). The presence of negative symptoms in other disorders may thus be overlooked. Indeed, a recent study found that euthymic participants with BD-I had equal levels of apathy as participants with SCZ (26). Yet, negative symptoms are understudied in BD. This limits our progress in understanding these phenomena, and hampers the development and provision of proper treatment.
In SCZ, negative symptoms comprise two main dimensions, i.e., diminished expression (blunted affect and alogia, also called expressive negative symptoms) and apathy (avolition, anhedonia and asociality, also called experiential negative symptoms) (27, 28). This distinction is important as it could mirror different underlying pathophysiological mechanisms (4). Previous research has, however, mainly focused on negative symptoms as a unidimensional construct, which limits the understanding of diminished expression and apathy as potential separate entities. Exploratory and confirmatory factor analyses have shown that the two dimensions can be assessed using the Positive and Negative Syndrome Scale (PANSS) (29–32). However, these studies have only included participants with SCZ, and there is limited knowledge about the robustness of the two-dimensional structure in other severe mental disorders such as BD.
One way to approach this issue is to study whether current knowledge about negative symptoms in SCZ, such as their dimensional structure, translates across diagnostic groups. Two previous studies have investigated and compared the structure of psychotic symptoms in SCZ and BD using the PANSS (33, 34). Both studies employed a five-factor model of the PANSS scores and they replicated unidimensional negative symptoms as one factor in BD. The negative symptom factor could be distinguished from the depressive factor in both studies, in line with findings in SCZ and other non-affective psychoses (35–38). Differentiating negative from depressive symptom dimensions is clinically challenging (39) because of similar clinical presentations. Neither of these two studies, however, used a two-dimensional measure of negative symptoms, nor investigated clinical and sociodemographic correlates of the identified negative factor.
Strauss et al. (40) examined the two-dimensional structure of negative symptoms using the Brief Negative Symptom Scale (BNSS) to investigate symptom levels and internal consistency in SCZ, BD and healthy controls (HC). They found higher levels of the two negative symptom dimensions in both SCZ and BD, compared to HC, in addition to good internal consistency. Discriminant validity was assessed with correlational analyses to other symptom dimensions and external validators. In BD, the total score of negative symptoms and apathy was significantly correlated with depressive symptoms as measured by the Hamilton Depressive Rating Scale (HDRS) (r = 0.38 and r = 0.53, respectively), while diminished expression was not. Apathy was also significantly correlated with positive symptoms (r = 0.37). In addition, both dimensions were significantly correlated with the use of antipsychotics. The authors concluded that this might indicate that the negative symptoms they assessed in BD could be secondary to depression, psychotic symptoms or antipsychotic effects, a phenomenon also seen in SCZ and other non-affective psychoses (5, 39).
Another important factor associated with negative symptoms is substance use (39). We recently demonstrated an association between cannabis use and diminished expression in SCZ (41). Intake of cannabis can cause acute psychiatric symptoms (42), and cannabis use is further associated with increased risk of several detrimental outcomes (43, 44). Importantly, almost a quarter of patients with BD either use cannabis or have a cannabis use disorder (CUD) (44).
In sum, it is important to investigate the dimensional structure of negative symptoms, and their sociodemographic and clinical correlates, transdiagnostically. It may progress our understanding of these debilitating phenomena, and ultimately pave the way for new treatment approaches. The aims of the current study were:
• To explore if the two-factor structure of negative symptoms previously shown in SCZ can be replicated in a sample of BD participants.
• To validate the findings by examining the association between the identified factors and clinical characteristics previously found to be associated with negative symptoms in SCZ, including cannabis use.
• To characterize the prevalence of negative symptoms in BD, across diagnostic subgroups and affective states.
2. Materials and methods
2.1. Study design and sample
The current study is part of the ongoing Thematically Organized Psychosis study (TOP) at the Norwegian Centre for Mental Disorders Research (NORMENT). Information about the TOP-study and research activity at NORMENT were disseminated to health care professionals working in the in- and outpatient mental health care services in the Oslo catchment area through on-site visits by our research personnel and website information. Additionally, user representatives from the Norwegian Bipolar Association disseminated information to their members. Participants with an established or suspected diagnosis of BD were then recruited by referrals from the treating specialist or GP. The inclusion criteria were: age 18–65 years; meeting DSM-IV criteria (1) for BD-I, BD-II or BD not otherwise specified (BD-NOS), speaking and understanding a Scandinavian language and being able to give a written, informed consent. Exclusion criteria were IQ below 70, a history of moderate or severe head injury, somatic illness or neurological disorder that could influence or mimic affective states.
A total sample of 584 participants with BD (BD type 1: n = 348, BD type 2: n = 201, BD NOS = 35) was included for analysis. Thirty-eight participants had missing data on affective state, and were excluded from analyses that included these variables.
2.2. Clinical assessment
Trained clinical research personnel (medical doctors or psychologists) undertook diagnostic interviews with the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) (45), including the modules for affective and psychotic disorders, and substance use disorders. Detailed sociodemographic data were collected by interview and self-report. They included the history of previous and current frequency of alcohol-, nicotine-, cannabis- and other illegal substance use, and information regarding current psychotropic medication use. Premorbid social and academic functioning was assessed with the Premorbid Adjustment Scale (PAS) (46), and expressed by the sum score of PAS childhood and early adolescence for both domains. Current symptoms were assessed with the following scales: psychotic symptoms with the Positive and Negative Syndrome Scale (PANSS) (47), depressive symptoms with the Inventory for Depressive Symptomatology (IDS) (48), manic symptoms with the Young Mania Rating Scale (YMRS) (49). Positive symptoms were expressed as the sum score of PANSS items P1, P3, P5 and G9 (35). Euthymia was defined as IDS < 12 (i.e., no or mild depressive symptoms) and YMRS <8 (i.e., no or mild (hypo-)manic symptoms). Potential side-effects of medications were assessed with the Udvalg for Kliniske Undersøgelser (UKU) side-effect rating scale (50). Relevant side-effects for the current analyses were rated as present if an UKU scale score of ≥2 for the items: 1.10 emotional indifference, 2.1 dystonia, 2.1 rigidity, and 2.3 hypokinesia/akinesia.
2.3. Selecting the specific items for each negative symptom dimension
While several studies have validated a two-factor model of negative symptoms in PANSS in SCZ, the specific items included in each factor differ slightly (29–31, 51). The recent review by The European Psychiatric Association (EPA) (28) also underlines that some items from the general psychopathology subscale show more instability. For these reasons, we chose to investigate three possible two-factor solutions, and one unidimensional solution, as displayed in Table 1. Negative symptom scores were operationalized as the sum of included items, divided by the total number of items included.
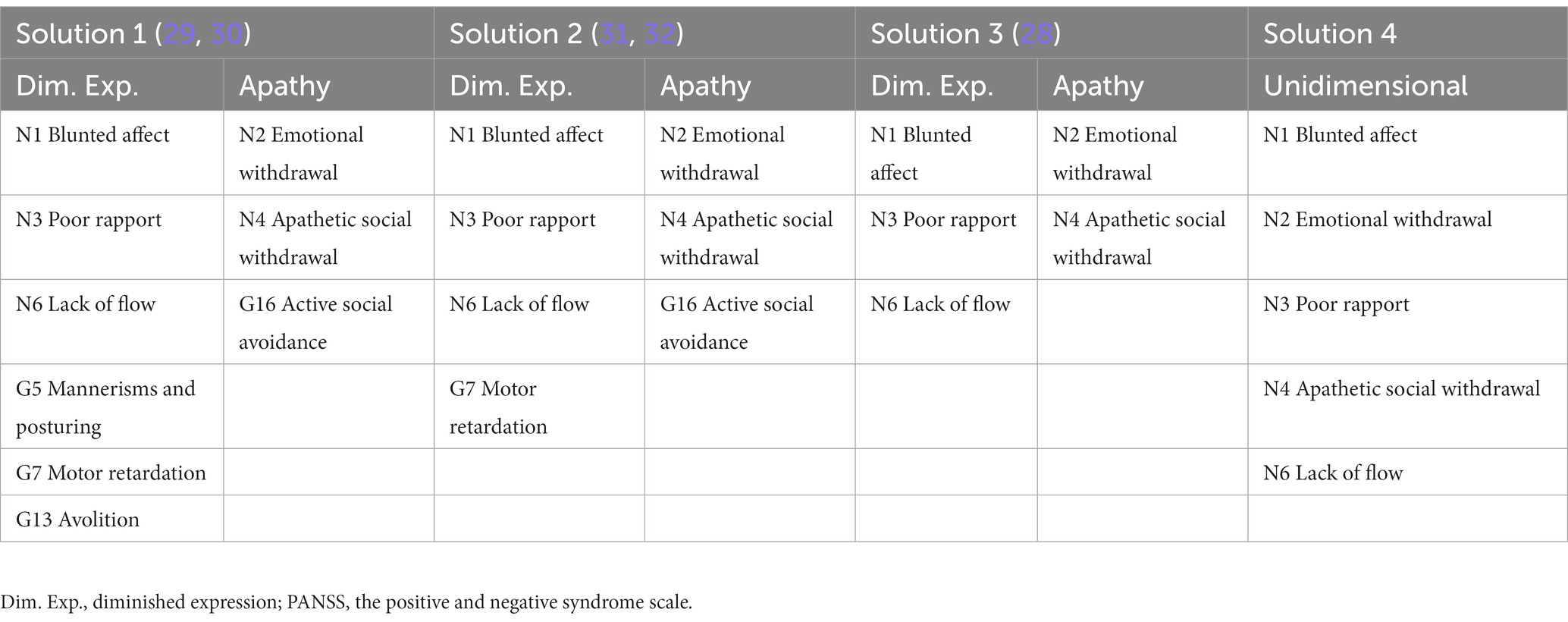
Table 1. Possible factor solutions for negative symptoms in PANSS.
2.4. Statistics
IBM SPSS package 27 and STATA SE 16 were used for data analyses.
First, we did an Exploratory Factor Analysis (EFA) (with Principal Axis Factoring) of the presupposed two-factor structure of negative symptoms. The EFA was performed to investigate individual factor loadings and to explore the factorability in the sample. We started by including the solution with the most items (Solution 1), and then reduced the number of items according to previous factor analytic work (29–32) and existing theoretical assumptions (4) (Solution 2–4). The Kaiser-Meyer-Oklin (KMO) (52) and Bartlett’s test for sphericity were calculated and inspected for suitability of data for factor analysis. A KMO > 0.6 and a significant Bartlett’s sphericity test were considered indicators of suitability. Oblimin rotated factor loadings are reported in the results.
Second, we performed a Confirmatory Factor Analysis (CFA) to test each of the model’s goodness of fit. The maximum likelihood method was used for estimation. The following goodness of fit indices were then inspected for each model: the Comparative Fit Index (CFI > 0.9), the Goodness-of-Fit index (GFI > 0.9), The Tucker-Lewis Index (TLI >0.9) (53), the Root Mean Square Error of Approximation (RMSEA, < 0.05 = very good fit, 0.05–0.08 = reasonable fit, 0.08–0.10 = mediocre fit, > 0.10 = unacceptable fit) (54), the Standardized Root Mean Square of Residuals (SRMR <0.05) (55). Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) measured comparative fit. Residuals that were statistically significantly correlated were introduced into the model to improve the fit (56). The best models obtained from the factor analyses, considering results from the EFA and CFA, were chosen for the further analyses.
Third, to validate the resulting factor-based dimensions, we carried out bivariate correlation analyses (Spearman’s rho) to investigate correlations between sociodemographic and clinical variables, and the two negative symptom dimensions (and a unidimensional measure as reference). Point-Biserial correlations were carried out for dichotomous variables. The variables were selected based on previous reports of associations to negative symptoms in SCZ (10, 28, 39–41, 57).
Fourth, we conducted hierarchical linear regression analyses, with the two dimensions of negative symptoms, as well as the unidimensional measure for negative symptoms, as dependent variables. All dependent variables were successfully log-transformed, due to skewed distribution. Variables that were significantly correlated (p < 0.05) with either factor in the bivariate correlation analyses were entered as independent variables. The final models only contain independent variables that made a significant contribution, in addition to age and sex. A dummy variable for a diagnosis of BD-1 vs. BD-2 and BD NOS was used to test the significance of subgroups within BD. Residuals were analyzed to assess the assumptions of normality, linearity, homoscedasticity, and independence. The variance inflation factor (VIF) was assessed to avoid multicollinearity in the final model (<1.6).
Finally, we investigated the prevalence of negative symptoms in different subgroups of BD (a score of 3 indicates that a symptom is present, but to a low degree, and a score of 4 to a moderate degree), and used the Mann–Whitney U test to investigate differences in negative symptom levels between BD-1 and BD-2, and between depressed and euthymic individuals. In the former, BD NOS was excluded due to their comparatively low n (n = 35); in the latter, participants with mixed or manic symptoms were excluded. Effect sizes were calculated by the following formula: r = |z| / √n.
3. Results
3.1. Participants’ characteristics
Out of all participants, 32.5% (n = 190) were euthymic, 47.1% (n = 275) had clinically significant depressive symptoms (IDS ≥ 12), 5.8% (n = 34) had clinically significant manic symptoms (YMRS >8), and 8% (n = 47) experienced mixed symptoms (IDS ≥ 12 and YMRS ≥8) at the point of assessment. A total of 31.2% reported any cannabis use within the last 2 years (n = 182), and 9.1% (n = 53) reported cannabis use in the last 2 weeks. Other descriptive characteristics are given in Table 2.
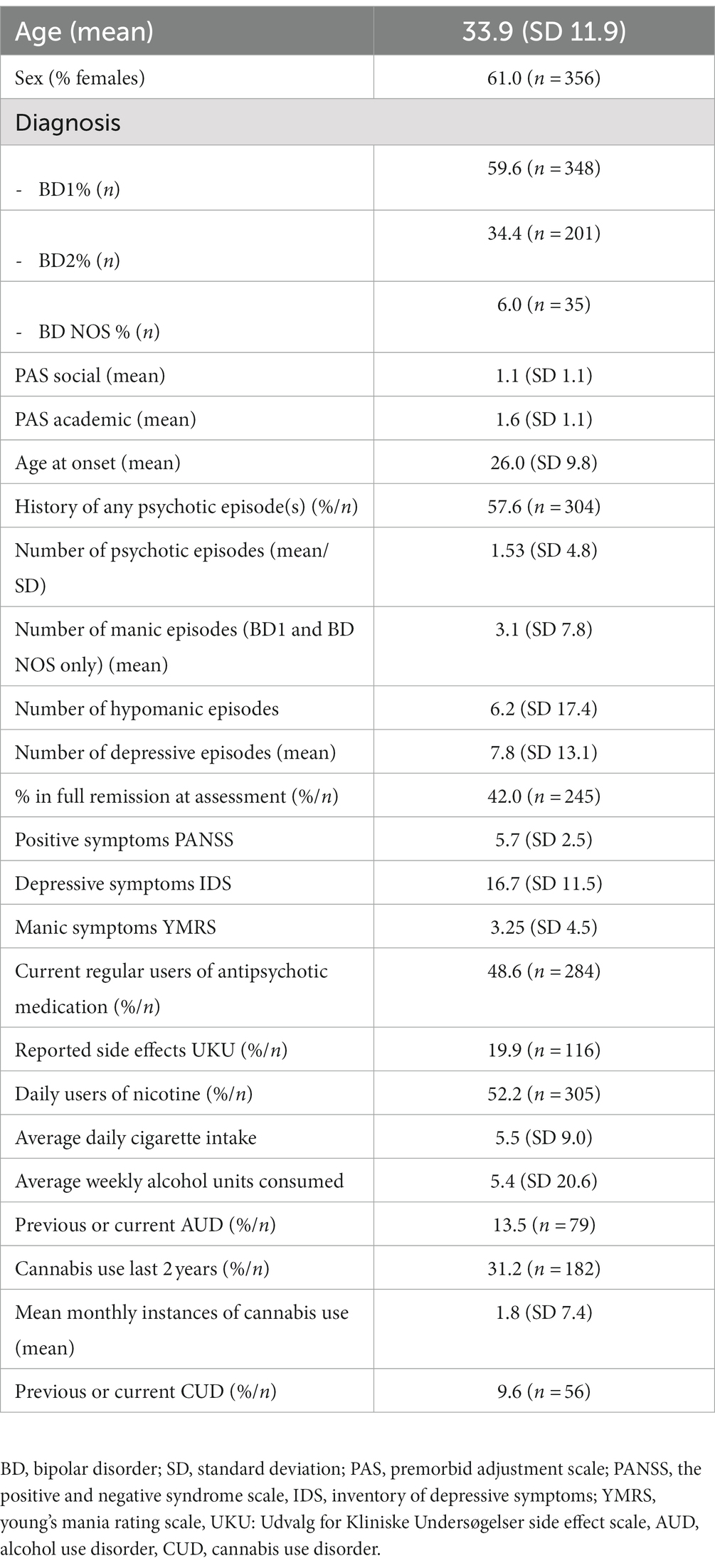
Table 2. Participants’ sociodemographic and clinical characteristics.
3.2. Results from the factor analyses
The results from the factor analyses are presented in Table 3.
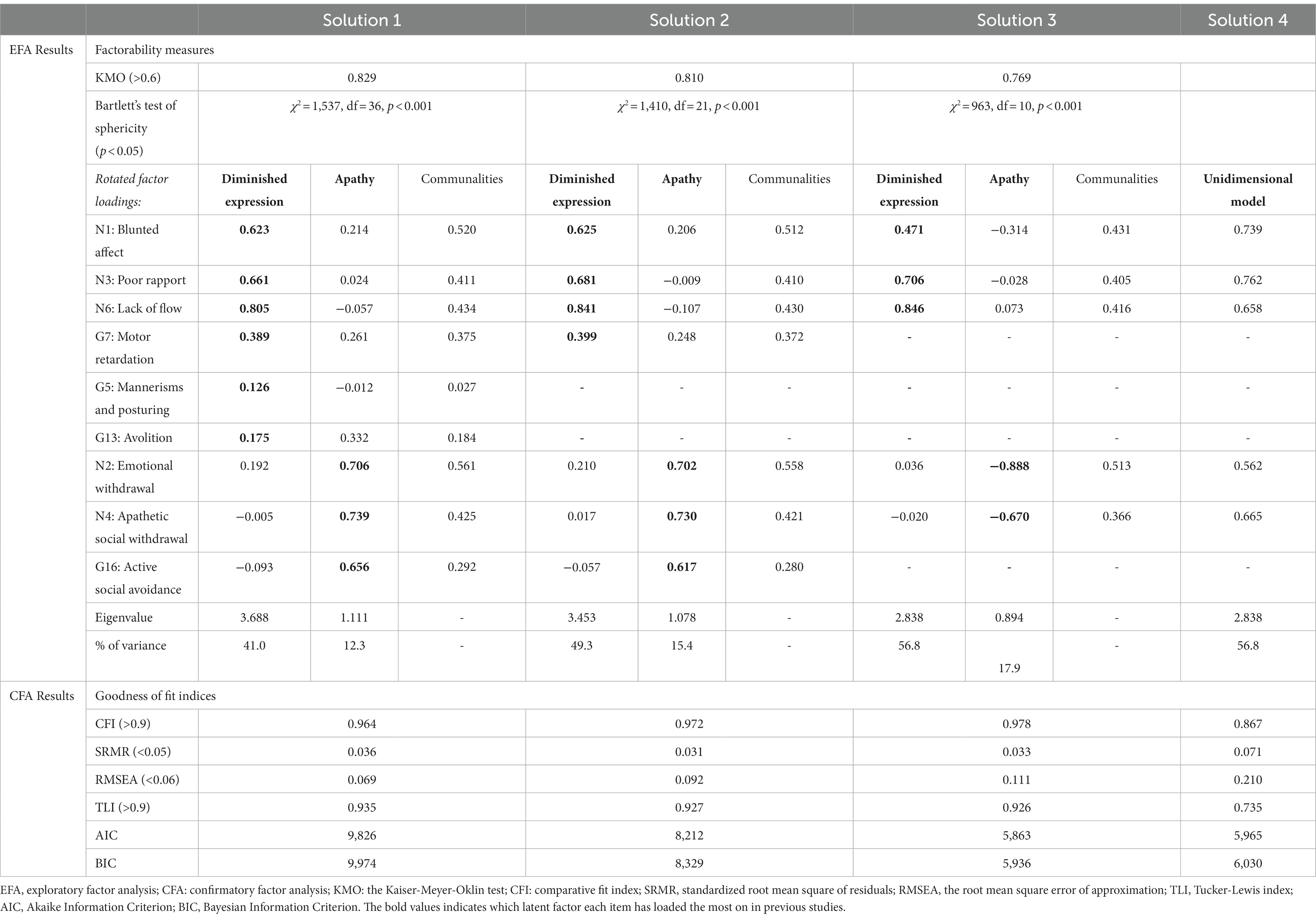
Table 3. Results from factor analyses.
Solution 1 resulted in two factors with Eigenvalues > 1.0, accounting for 53.3% of the variance. The factor loadings of items G5 Mannerisms and posturing and G13 Avolition showed the weakest factor loadings (0.126 and 0.175, respectively) and the weakest communalities (0.027 and 0.184, respectively). Additionally, G13 Avolition loaded most on the apathy factor (0.332), not the diminished expression-factor.
Solution 2 also resulted in two factors with Eigenvalues >1.0, accounting for 64.7% of the variance. Several goodness of fit indices from the CFA also indicated a good fit for this model (CFI = 0.972, SRMR = 0.031, CD = 929, TLI = 0.927, AIC = 8,212, BIC = 8,329), the weakest being a RMSEA of 0.092 only suggestive of mediocre fit. The items G7 Motor Retardation and G16 Social Avoidance loaded 0.399 and 0.617 on diminished dxpression and apathy respectively, and displayed the weakest but still acceptable communalities (0.372 and 0.280, respectively).
Solutions 3 and 4 (i.e., item N1, N2, N3, N4, and N6 only) revealed only one factor with Eigenvalue >1.0, accounting for 56.8% of the variance.
Based on these results, we chose Solution 2 (31) as the two-factor model with the best fit, and Solution 4 as the unidimensional reference for further analyses.
3.3. Bivariate correlations between the two dimensions of negative symptoms, the unidimensional measure of negative symptoms, and relevant sociodemographic and clinical variables
Male sex, poor premorbid social functioning, less time in remission, more depressive and positive symptoms, reported side effects of medication and less alcohol use were significantly correlated with higher levels of both negative symptom dimensions. Younger age, a higher number of previous psychotic episodes, less manic symptoms and current use of antipsychotics was significantly correlated with higher levels of diminished expression, but not apathy. Poor premorbid academic functioning and a higher number of previous depressive episodes correlated with higher levels of apathy, but not with diminished expression. Neither frequency of cannabis use, nor cannabis use disorder was significantly correlated with either negative symptom dimension.
Table 4 displays all results from the bivariate correlation analyses.
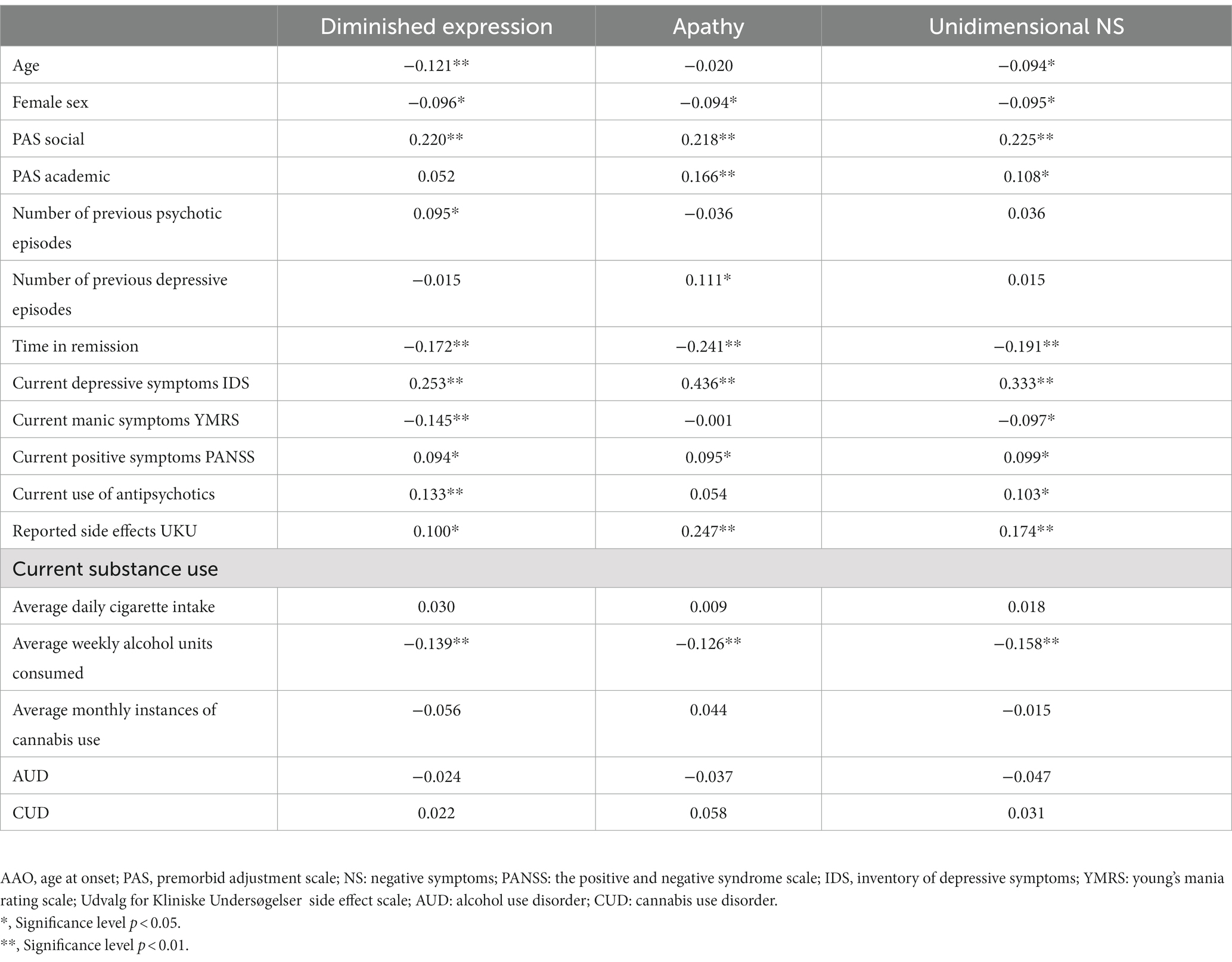
Table 4. Bivariate correlations (Spearman’s rho).
3.4. Multiple hierarchical regression analyses with negative symptom dimensions as dependent variables and sociodemographic and clinical factors as independent variables
Table 5 displays the results from the final models of the multiple hierarchical regression analyses, i.e., comprising variables with significant contributions to the different negative symptom dimensions. The independent variables explained 20.8% of the variance of diminished expression, 27.5% of apathy, and 21.3% of unidimensional negative symptoms. A diagnosis of BD-1 was associated with higher levels of diminished expression (β = 0.113, p = 0.007), but was excluded from the final model due to multicollinearity with a history of psychotic episodes. Premorbid academic functioning was also excluded from the final model of apathy due to multicollinearity with premorbid social functioning. Positive symptoms, time in remission, and average weekly alcohol use did not contribute significantly to any of the models. For the remaining independent variables with a significant contribution to the different models, please see Table 5.
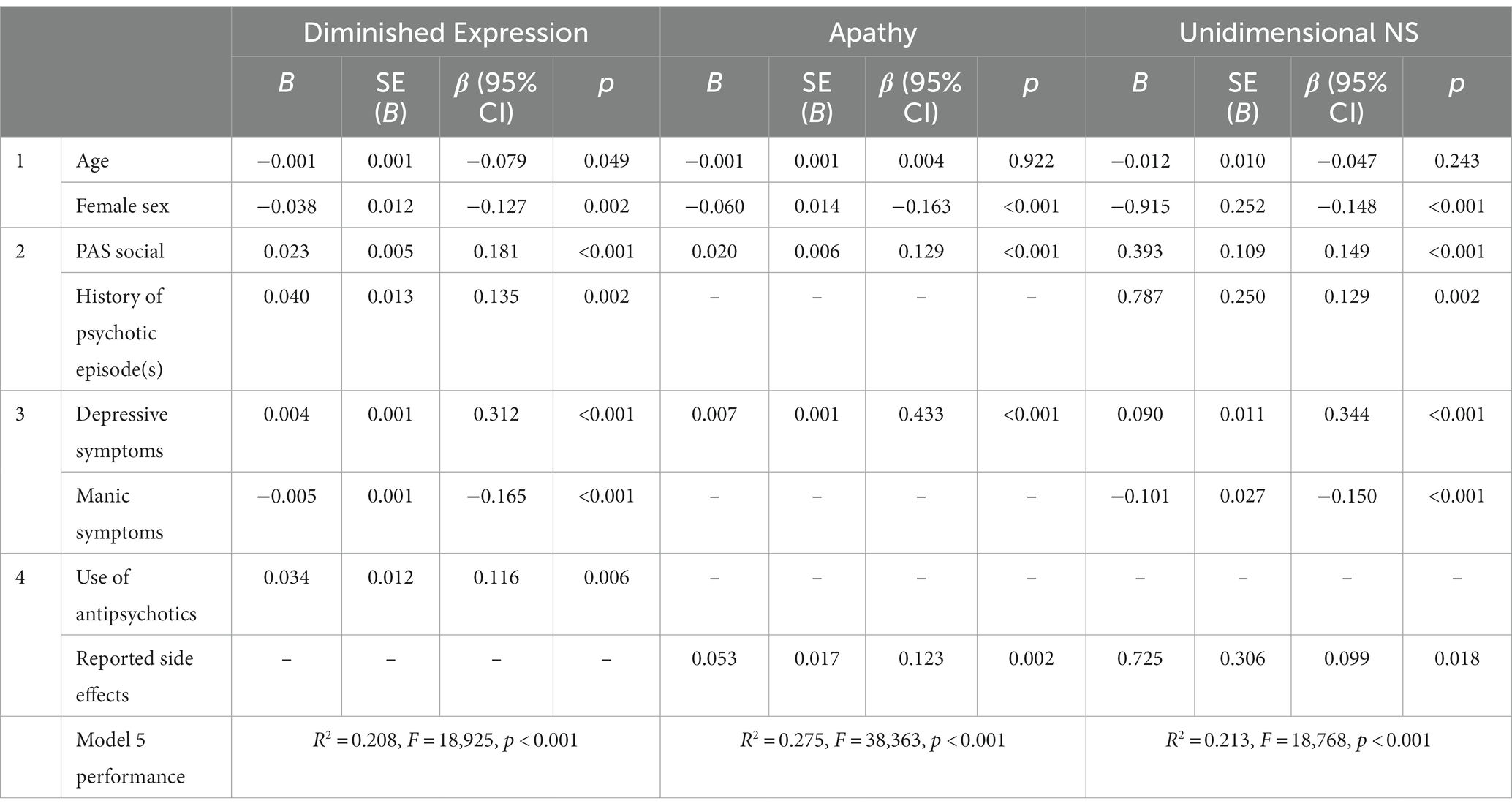
Table 5. Final model of multiple hierarchical regression analyses.
3.5. Prevalence and correlates of negative symptoms across diagnostic categories and affective states
In total, 41.5% (n = 238) scored ≥3 and 12.5% (n = 73) scored ≥4 on at least one of the negative symptom items (N1, N2, N3, N4, N6, G7, or G16). Concerning dimension specificity, 22.8% (n = 133) scored ≥3 and 7.2% (n = 42) ≥ 4 on diminished expression-items, and 31.9% (n = 186) scored ≥3 and 8.4% (n = 49) on apathy-items. Scores on each negative symptom item are presented in Figures 1, 2 for the whole sample. Among individuals with clinically significant depressive symptoms, 52% (n = 142) scored ≥3 and 16.5% (n = 45) scored ≥4 on at least one of the negative symptom items. Among euthymic individuals, 26.3% (n = 50) scored ≥3 and 5.3% (n = 10) scored ≥4.
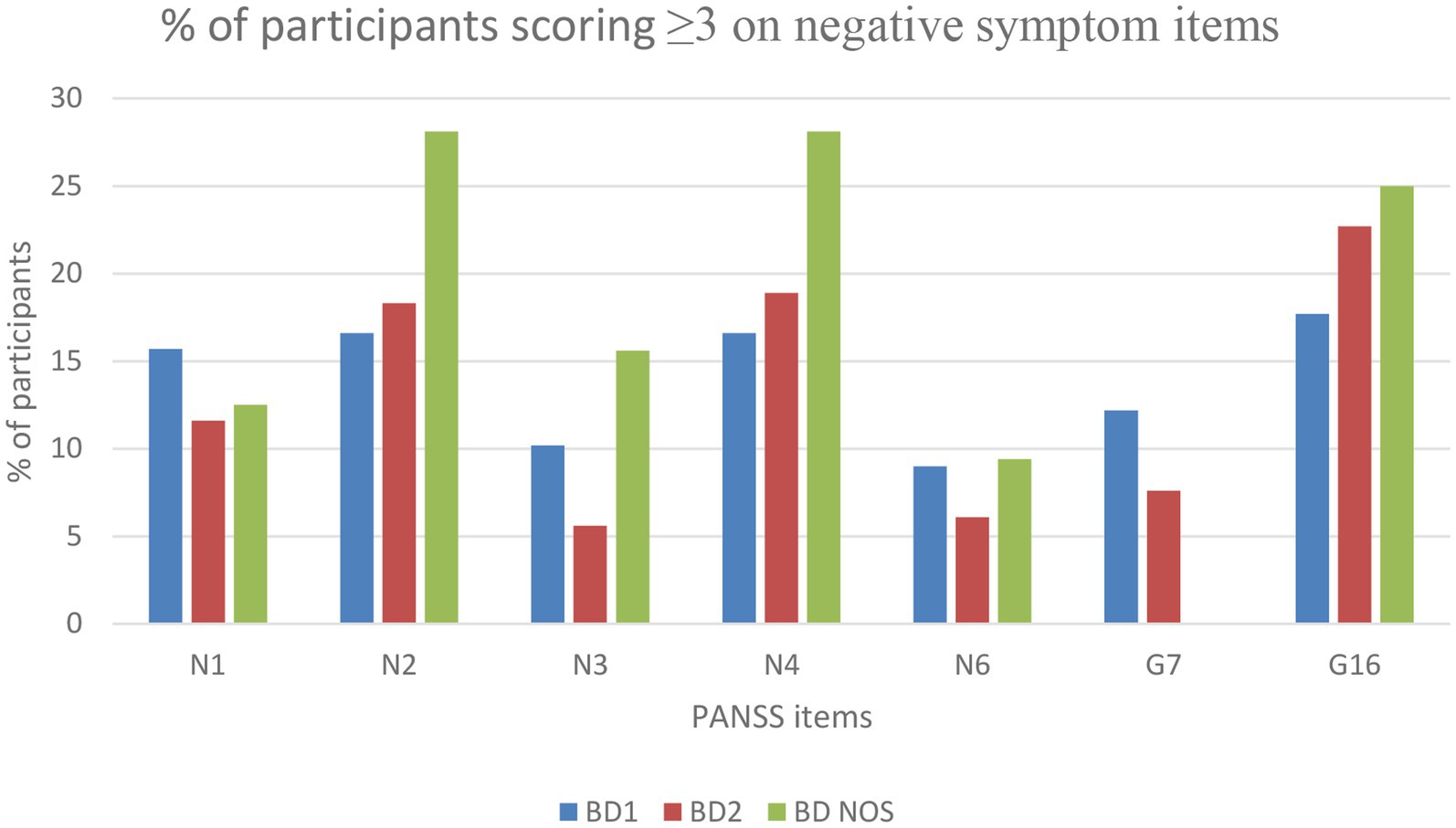
Figure 1. Number of participants with negative symptom scores equal to or above 3.
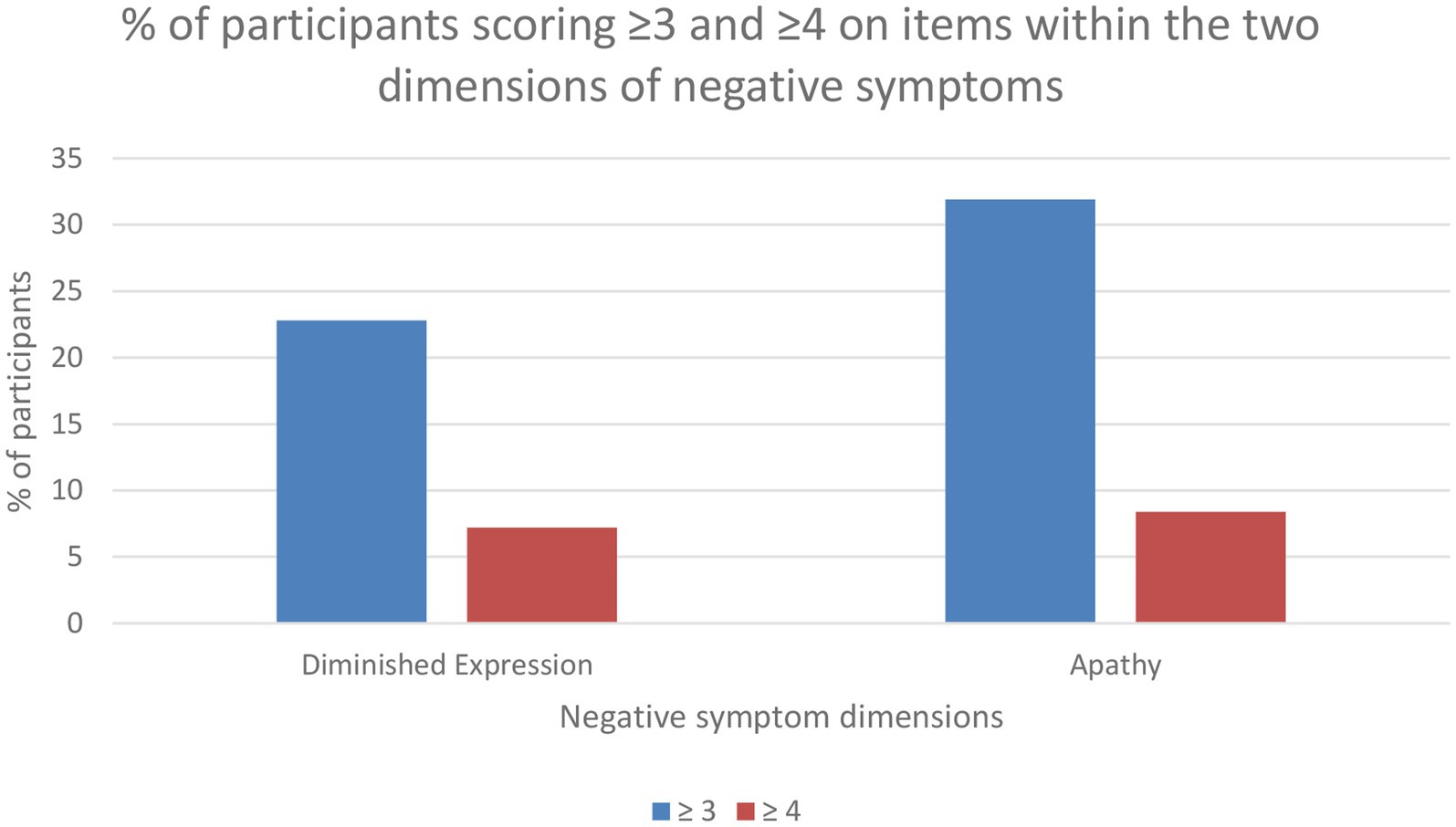
Figure 2. Percentage of participants with symptoms present within diminished expression and apathy.
Comparisons of diminished expression, apathy, and the unidimensional measure of negative symptoms between diagnostic category and euthymia vs. depression are presented in Tables 6, 7, respectively. We found significantly higher levels of apathy in BD-2, with a small effect size (r = 0.123). Depressed participants had significantly higher levels of all negative symptom dimensions, compared to euthymic individuals, with a moderate effect size for apathy (r = 0.311), and small effect sizes for diminished expression (r = 0.161) and unidimensional negative symptoms (r = 0.235).
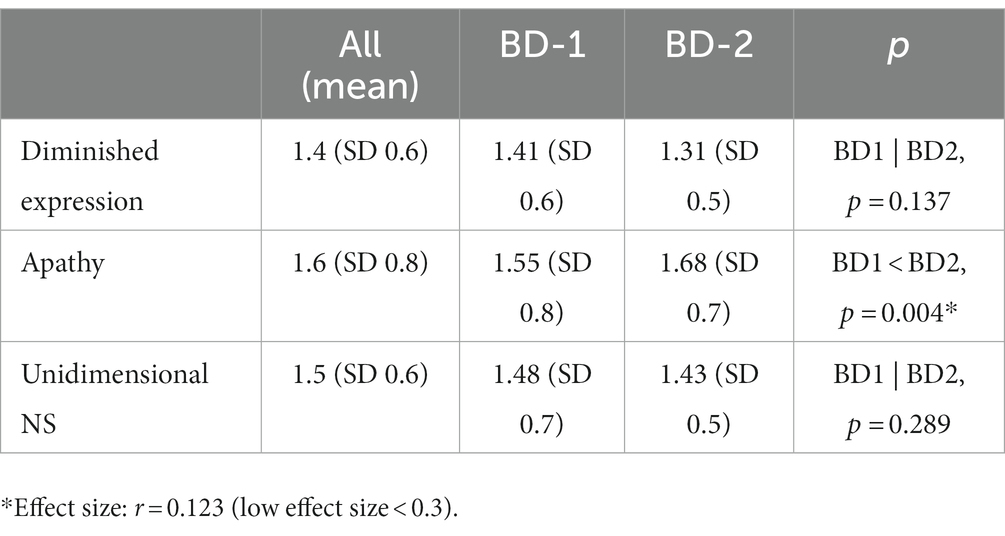
Table 6. Comparison of negative symptoms across diagnostic subgroups.
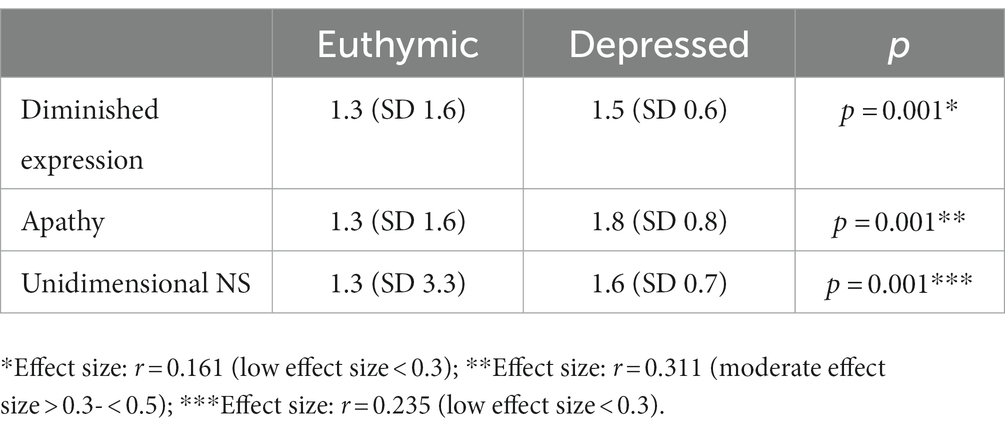
Table 7. Comparison of negative symptoms between depressed and euthymic state.
4. Discussion
The main findings of this study include a replication of the previously validated two-factor model of negative symptoms in SCZ using PANSS in a BD sample. Several correlates of negative symptoms known in SCZ were reproduced in BD, suggesting a similar phenomenology and demonstrating the external validity of the two negative symptom dimensions across SCZ and BD. The discriminant validity with positive symptoms, depressive symptoms, manic symptoms, and use and reported side-effects of antipsychotics were generally comparable to previous investigations (40), with the apathy dimension displaying the most overlap with depressive symptoms. At the time of assessment, 41.5% of all participants displayed some degree of negative symptoms, while 12.5% had at least one moderate negative symptom. Depressed participants had significantly more negative symptoms than euthymic participants. A diagnosis of BD-I and a history of psychotic episodes were associated with more severe diminished expression. Contrary to previous findings in participants with SCZ (41), we found no association between cannabis use and diminished expression.
We performed factor analyses for three possible two-factor solutions for negative symptoms based on the PANSS scores. Our findings partly confirm EPA’s (28) statement that the items from general psychopathology show the most inconsistent loadings on the negative symptom dimensions. The items from Solution 3 and 4 (N1, N2, N3, N4, and N6) displayed the most consistent and highest factor loadings. However, these items alone did not display a factorability into a two-factor solution, and were thus only able to represent a unidimensional construct of negative symptoms. Including items G7 and G16 from general psychopathology (Solution 2) increased the total variance explained and allowed for the two-factor model fit. Our results are in line with previous factor analyses in SCZ (29–32), which suggests that the structure of negative symptoms found in SCZ is also reproduced in BD.
Both poles of affect, as measured by the IDS and YMRS, showed associations to negative symptoms. Depressive symptoms were associated with more severe negative symptoms of both dimensions, while manic symptoms were associated with lower levels of diminished expression. A previous study by Kirschner et al. (26) also found subclinical depressive symptoms to be associated with negative symptoms in BD, but remarked that they did not find the same association in participants with SCZ. Strauss et al. (40) found significant correlations between depressive symptoms and apathy in both SCZ and BD-I. Distinguishing depressive from negative symptoms is difficult due to significant phenotypical overlap, and limited knowledge of the underlying mechanisms. We found a significant but still relatively low correlation between depressive symptoms and diminished expression, and a significant moderate correlation between depressive symptoms and apathy. In line with Strauss et al.’s (40) findings, diminished expression thus showed less overlap with depressive symptoms. It is previously suggested that diminished expression is more characteristic of negative symptoms (28, 58). Considering that the apathy dimension includes anhedonia and avolition, two key features also present in depression, this overlap is not unexpected. The IDS includes two items that measure engagement and pleasure of social and/or other activities, which may contribute to this association. The overlap between apathy and depression is also observed in SCZ and FEP (40, 41, 59), with examples of avolition and anhedonia being present both with and without depression (6, 39, 60, 61).
There are, however, indications that the quality of anhedonia and avolition differs between SCZ and depression. It is suggested that anticipatory anhedonia is more common to SCZ, while consummatory anhedonia is more typical for depression (62–65). This may reflect differences in the underlying pathophysiological mechanisms (66). Moreover, avolition per se does not necessitate the experience of sad mood/dysphoria, feelings of guilt, worthlessness or failure, as are common parts of the syndrome of depression. However, measures of anhedonia and avolition are frequently included in scales of both negative symptoms and depression, causing potential criteria overlap. Anhedonia and avolition are nevertheless strongly interrelated and transdiagnostically co-occurring (67). Taken together, assigning these symptoms to a specific dimension (i.e., depression vs. negative symptom) remains a challenge. From a clinical perspective, once negative symptoms are recognized, it would be prudent to explore and consider all potential sources of secondary negative symptoms, as they remain more amendable by current treatments than primary negative symptoms (68).
Furthermore, we found that participants with BD-II had higher levels of apathy, compared to BD-I, but with a small effect size. The effect was insignificant in the multiple hierarchical regression model, suggesting that other factors, such as more depressive symptoms, contributed to driving this difference. A diagnosis of BD-I and a history of psychotic episodes were both associated with more severe diminished expression. This could support the notion that negative symptoms in the form of diminished expression are tied to liability for psychosis (40), and may point toward a shared etiology.
We found an inverse correlation with time in remission, which suggests that negative symptoms vary over time and are more prominent close to a mood episode. This is in line with previous research that finds negative symptoms to vary over time (59, 69–71), with more persistence in SCZ (10), and more fluctuations in affective disorders (66, 72, 73). However, the persistence of negative symptoms into euthymic phases of BD has also been described (72, 74, 75), although with lower severity levels than SCZ (10). More frequent fluctuations of negative symptoms in affective disorders are suggested to be caused by the co-varying fluctuations of affective symptoms. In line with this, we found significantly less severe negative symptoms in euthymic than depressed participants. Nevertheless, more than a quarter of the euthymic individuals had at least one mild (or more severe) negative symptom, and 5.3% had one moderate negative symptom, attesting to some degree of persistence beyond depressed states. Given that many of the participants in the current study had lived with the diagnosis for several years, factors such as social deprivation may also contribute to sustain negative symptoms beyond mood episodes.
In contrast to previous findings of an association between cannabis use and diminished expression in SCZ (41), we found no significant associations in BD. The lack of such a relationship in BD could strengthen the hypothesis that the diagnostic groups considered on the more “severe end” of the psychosis spectrum, such as schizophrenia, are more vulnerable to cannabis exposure (76). An extension to this line of reasoning could suggest that cannabis use itself is not a sufficient cause of diminished expression, and that the previously observed association between cannabis use and more severe diminished expression represents cannabis’ effect on central pathophysiological mechanisms of SCZ and primary negative symptoms. Average recent alcohol use had a weak inverse correlation to both negative symptom dimensions in the bivariate analyses, but did not contribute independently to the final regression models. In line with our previous study, neither alcohol- nor nicotine use showed any independent association with negative symptoms (41).
The main strength of this study is the relatively high number of participants, the thorough diagnostic and psychopathologic assessment of the participants, and the inclusion of a range of potential correlates of negative symptoms. Limitations include the cross-sectional design, limiting the ability to make causal inferences between potential sources of negative symptoms and negative symptom severity. The PANSS is usually considered inferior to newer scales, such as the BNSS. One important limitation of the PANSS is its lack of assessing subjective experience. However, compared to the validation study by Strauss et al. using BNSS (40), our results attest to the validity of discriminating the two negative symptom dimensions with PANSS. Further, using the frequency of cannabis use and/or the presence of CUD in the analyses does not directly represent the type and amount of different cannabinoids present in the ingested substances.
4.1. Concluding remarks
Our findings regarding the presence and structure of negative symptoms in participants with BD generally verify previous researchers’ suggestions of negative symptoms as a transdiagnostic phenomenon (10, 12, 77). This is in line with previous investigations of negative symptoms outside of SCZ (12, 40, 72). Diminished expression was associated with a history of psychotic episodes and a diagnosis of BD-I, which may infer closer connections to psychosis liability. At the same time apathy displayed closer links to depressive symptoms. We found no association between cannabis use and negative symptoms.
Future studies should seek to continue negative symptom research with a dimension- or domain-specific granularity, and search for links to external validators across diagnostic categories.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Regional Etisk Komite (REK) Sør-Øst C, reference #2009/2485/REJ sør-øst C Gullhaugveien 1-3 0484 Oslo Norway. The patients/participants provided their written informed consent to participate in this study.
Author contributions
HI undertook the statistical analyses and wrote the first draft of the manuscript, under the supervision of TL, IM, and KR. TL and IM have leading roles in the management and funding of the TOP study. All authors have at some point contributed in participant recruitment and assessment for data collection, critically revised methodology, analyses, and manuscript through several steps of revision.
Funding
This work was supported by the Centre of Excellence (CoE) (Grant #223273/F50 and #287714) and the Southern and Eastern Norway Regional Health Authority (Grant #2006233, #2006258, #2011085, #2014102, and #2015088). We also benefited from the resource: TSD p33 (#NS9666S).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. APA . Diagnostic and statistical manual of mental disorders (DSM-IV). Washington, DC: American Psychiatric Association (1994).
2. World Health Organization . ICD-10: International statistical classification of diseases and related health problems: tenth revision. 2nd ed. Geneva: World Health Organization (2004).
3. APA . Diagnostic and statistical manual of mental disorders : DSM-5™. 5th ed. Washington, DC: American Psychiatric Publishing, a division of American Psychiatric Association (2013).
4. Bègue, I, Kaiser, S, MJN, K, and Reviews, B. Pathophysiology of negative symptom dimensions of schizophrenia–current developments and implications for treatment. Neurosci Biobehav Rev. (2020) 116:74–88. doi: 10.1016/j.neubiorev.2020.06.004
5. Mosolov, SN, and Yaltonskaya, PA. Primary and secondary negative symptoms in schizophrenia. Front Psychiatry. (2022) 12:766692. doi: 10.3389/fpsyt.2021.766692
6. Galderisi, S, Mucci, A, Buchanan, RW, and Arango, C. Negative symptoms of schizophrenia: new developments and unanswered research questions. Lancet Psychiatry. (2018) 5:664–77. doi: 10.1016/S2215-0366(18)30050-6
7. Marder, SR, and Galderisi, S. The current conceptualization of negative symptoms in schizophrenia. World Psychiatry. (2017) 16:14–24. doi: 10.1002/wps.20385
8. Walther, S, and Morrens, M. What can be learned from dimensional perspectives on psychiatry? Neuropsychobiology. (2020) 79:249–50. doi: 10.1159/000508762
9. Kelly, JR, Clarke, G, Cryan, JF, and Dinan, TG. Dimensional thinking in psychiatry in the era of the research domain criteria (RDoC). Ir J Psychol Med. (2018) 35:89–94. doi: 10.1017/ipm.2017.7
10. Strauss, GP, and Cohen, AS. A Transdiagnostic review of negative symptom phenomenology and etiology. Schizophr Bull. (2017) 43:712–9. doi: 10.1093/schbul/sbx066
11. Emmerson, LC, Ben-Zeev, D, Granholm, E, Tiffany, M, Golshan, S, and Jeste, DV. Prevalence and longitudinal stability of negative symptoms in healthy participants. Int J Geriatr Psychiatry. (2009) 24:1438–44. doi: 10.1002/gps.2284
12. Foussias, G, Agid, O, Fervaha, G, and Remington, G. Negative symptoms of schizophrenia: clinical features, relevance to real world functioning and specificity versus other CNS disorders. Eur Neuropsychopharmacol. (2014) 24:693–709. doi: 10.1016/j.euroneuro.2013.10.017
13. O'Connell, KS, and Coombes, BJ. Genetic contributions to bipolar disorder: current status and future directions. Psychol Med. (2021) 51:2156–67. doi: 10.1017/S0033291721001252
14. Oraki Kohshour, M, Papiol, S, Ching, CRK, and Schulze, TG. Genomic and neuroimaging approaches to bipolar disorder. BJPsych Open. (2022) 8:e36. doi: 10.1192/bjo.2021.1082
15. Disorder WCftA-DH, Disorder AS, Disorder B, Disorder MD, Disorder O-C, Groups aSEW . Virtual histology of cortical thickness and shared neurobiology in 6 psychiatric disorders. JAMA. Psychiatry. (2021) 78:47–63. doi: 10.1001/jamapsychiatry.2020.2694
16. Park, B-y, Kebets, V, Larivière, S, Hettwer, MD, Paquola, C, van Rooij, D, et al. Multiscale neural gradients reflect transdiagnostic effects of major psychiatric conditions on cortical morphology. Commun Biol. (2022) 5:1024. doi: 10.1038/s42003-022-03963-z
17. Bonnín, CM, Sánchez-Moreno, J, Martínez-Arán, A, Solé, B, Reinares, M, Rosa, A, et al. Subthreshold symptoms in bipolar disorder: impact on neurocognition, quality of life and disability. J Affect Disord. (2012) 136:650–9. doi: 10.1016/j.jad.2011.10.012
18. Michalak, EE, Yatham, LN, and Lam, RW. Quality of life in bipolar disorder: a review of the literature. Health Qual Life Outcomes. (2005) 3:1–17. doi: 10.1186/1477-7525-3-72
19. Martínez-Arán, A, Vieta, E, Reinares, M, Colom, F, Torrent, C, Sánchez-Moreno, J, et al. Cognitive function across manic or hypomanic, depressed, and euthymic states in bipolar disorder. Am J Psychiatr. (2004) 161:262–70. doi: 10.1176/appi.ajp.161.2.262
20. Post, RM, Altshuler, LL, Kupka, R, McElroy, SL, Frye, MA, Rowe, M, et al. Age of onset of bipolar disorder: combined effect of childhood adversity and familial loading of psychiatric disorders. J Psychiatr Res. (2016) 81:63–70. doi: 10.1016/j.jpsychires.2016.06.008
21. Arango, C, Dragioti, E, Solmi, M, Cortese, S, Domschke, K, Murray, RM, et al. Risk and protective factors for mental disorders beyond genetics: an evidence-based atlas. World Psychiatry. (2021) 20:417–36. doi: 10.1002/wps.20894
22. Vieta, E, Salagre, E, Grande, I, Carvalho, AF, Fernandes, BS, Berk, M, et al. Early intervention in bipolar disorder. Am J Psychiatr. (2018) 175:411–26. doi: 10.1176/appi.ajp.2017.17090972
23. van Bergen, AH, Verkooijen, S, Vreeker, A, Abramovic, L, Hillegers, MH, Spijker, AT, et al. The characteristics of psychotic features in bipolar disorder. Psychol Med. (2019) 49:2036–48. doi: 10.1017/S0033291718002854
24. Aminoff, SR, Onyeka, IN, Ødegaard, M, Simonsen, C, Lagerberg, TV, Andreassen, OA, et al. Lifetime and point prevalence of psychotic symptoms in adults with bipolar disorders: a systematic review and meta-analysis. Psychol Med. (2022) 52:2413–25. doi: 10.1017/S003329172200201X
25. International Schizophrenia ConsortiumPurcell, SM, Wray, NR, Stone, JL, Visscher, PM, O'Donovan, MC, et al. Common polygenic variation contributes to risk of schizophrenia and bipolar disorder. Nature. (2009) 460:748–52. doi: 10.1038/nature08185
26. Kirschner, M, Cathomas, F, Manoliu, A, Habermeyer, B, Simon, JJ, Seifritz, E, et al. Shared and dissociable features of apathy and reward system dysfunction in bipolar I disorder and schizophrenia. Psychol Med. (2020) 50:936–47. doi: 10.1017/S0033291719000801
27. Kirkpatrick, B, Fenton, WS, Carpenter, JWT, and Marder, SR. The NIMH-MATRICS consensus statement on negative symptoms. Schizophr Bull. (2006) 32:214–9. doi: 10.1093/schbul/sbj053
28. Galderisi, S, Mucci, A, Dollfus, S, Nordentoft, M, Falkai, P, Kaiser, S, et al. EPA guidance on assessment of negative symptoms in schizophrenia. Eur Psychiatry. (2021) 64:e23. doi: 10.1192/j.eurpsy.2021.11
29. Liemburg, E, Castelein, S, Stewart, R, van der Gaag, M, Aleman, A, and Knegtering, H. Two subdomains of negative symptoms in psychotic disorders: established and confirmed in two large cohorts. J Psychiatr Res. (2013) 47:718–25. doi: 10.1016/j.jpsychires.2013.01.024
30. Stiekema, APM, Liemburg, EJ, van der Meer, L, Castelein, S, Stewart, R, van Weeghel, J, et al. Confirmatory factor analysis and differential relationships of the two subdomains of negative symptoms in chronically ill psychotic patients. PLoS One. (2016) 11:e0149785. doi: 10.1371/journal.pone.0149785
31. Khan, A, Liharska, L, Harvey, PD, Atkins, A, Ulshen, D, and Keefe, RSE. Negative symptom dimensions of the positive and negative syndrome scale across geographical regions: implications for social, linguistic, and cultural consistency. Innov Clin Neurosci. (2017) 14:30–40.
32. Fervaha, G, Foussias, G, Agid, O, and Remington, G. Motivational and neurocognitive deficits are central to the prediction of longitudinal functional outcome in schizophrenia. Acta Psychiatr Scand. (2014) 130:290–9. doi: 10.1111/acps.12289
33. Lindenmayer, JP, Bossie, CA, Kujawa, M, Zhu, Y, and Canuso, CM. Dimensions of psychosis in patients with bipolar mania as measured by the positive and negative syndrome scale. Psychopathology. (2008) 41:264–70. doi: 10.1159/000128325
34. Anderson, AE, Mansolf, M, Reise, SP, Savitz, A, Salvadore, G, Li, Q, et al. Measuring pathology using the PANSS across diagnoses: inconsistency of the positive symptom domain across schizophrenia, schizoaffective, and bipolar disorder. Psychiatry Res. (2017) 258:207–16. doi: 10.1016/j.psychres.2017.08.009
35. Wallwork, RS, Fortgang, R, Hashimoto, R, Weinberger, DR, and Dickinson, D. Searching for a consensus five-factor model of the positive and negative syndrome scale for schizophrenia. Schizophr Res. (2012) 137:246–50. doi: 10.1016/j.schres.2012.01.031
36. Lindenmayer, J-P, Brown, E, Baker, RW, Schuh, LM, Shao, L, Tohen, M, et al. An excitement subscale of the positive and negative syndrome scale. Schizophr Res. (2004) 68:331–7. doi: 10.1016/S0920-9964(03)00087-2
37. Reininghaus, U, Priebe, S, and Bentall, RP. Testing the psychopathology of psychosis: evidence for a general psychosis dimension. Schizophr Bull. (2012) 39:884–95. doi: 10.1093/schbul/sbr182
38. Quattrone, D, di Forti, M, Gayer-Anderson, C, Ferraro, L, Jongsma, HE, Tripoli, G, et al. Transdiagnostic dimensions of psychopathology at first episode psychosis: findings from the multinational EU-GEI study. Psychol Med. (2019) 49:1378–91. doi: 10.1017/S0033291718002131
39. Kirschner, M, Aleman, A, and Kaiser, S. Secondary negative symptoms — a review of mechanisms, assessment and treatment. Schizophr Res. (2017) 186:29–38. doi: 10.1016/j.schres.2016.05.003
40. Strauss, GP, Vertinski, M, Vogel, SJ, Ringdahl, EN, and Allen, DN. Negative symptoms in bipolar disorder and schizophrenia: a psychometric evaluation of the brief negative symptom scale across diagnostic categories. Schizophr Res. (2016) 170:285–9. doi: 10.1016/j.schres.2015.12.014
41. Ihler, HM, Lagerberg, TV, Lyngstad, SH, Melle, I, and Romm, KL. Exploring the relationship between recency and frequency of cannabis use and diminished expression and apathy as two dimensions of negative symptoms in first episode psychosis. A one-year follow-up study. Schizophr Res. (2021) 236:89–96. doi: 10.1016/j.schres.2021.08.004
42. Hindley, G, Beck, K, Borgan, F, Ginestet, CE, McCutcheon, R, Kleinloog, D, et al. Psychiatric symptoms caused by cannabis constituents: a systematic review and meta-analysis. Lancet Psychiatry. (2020) 7:344–53. doi: 10.1016/S2215-0366(20)30074-2
43. Lowe, DJE, Sasiadek, JD, Coles, AS, and George, TP. Cannabis and mental illness: a review. Eur Arch Psychiatry Clin Neurosci. (2019) 269:107–20. doi: 10.1007/s00406-018-0970-7
44. Pinto, JV, Medeiros, LS, Santana da Rosa, G, Santana de Oliveira, CE, Crippa, JAS, Passos, IC, et al. The prevalence and clinical correlates of cannabis use and cannabis use disorder among patients with bipolar disorder: a systematic review with meta-analysis and meta-regression. Neurosci Biobehav Rev. (2019) 101:78–84. doi: 10.1016/j.neubiorev.2019.04.004
45. First, MB, Spitzer, RL, Gibbon, M, and Williams, JB. Structured clinical interview for DSM-IV axis I disorders. New York: New York State Psychiatric Institute (1995).
46. Cannon-Spoor, HE, Potkin, SG, and Wyatt, RJ. Measurement of premorbid adjustment in chronic schizophrenia. Schizophr Bull. (1982) 8:470–84. doi: 10.1093/schbul/8.3.470
47. Kay, SR, Fiszbein, A, and Opler, LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. (1987) 13:261–76. doi: 10.1093/schbul/13.2.261
48. Rush, AJ, Gullion, CM, Basco, MR, Jarrett, RB, and Trivedi, MH. The inventory of depressive symptomatology (IDS): psychometric properties. Psychol Med. (1996) 26:477–86. doi: 10.1017/S0033291700035558
49. Young, R, Biggs, J, Ziegler, V, and Meyer, D. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
50. Lingjærde, O, Ahlfors, UG, Bech, P, Dencker, SJ, and Elgen, K. The UKU side effect rating scale: a new comprehensive rating scale for psychotropic drugs and a cross-sectional study of side effects in neuroleptic-treated patients. Acta Psychiatr Scand. (1987) 76:1–100. doi: 10.1111/j.1600-0447.1987.tb10566.x
51. Jang, S-K, Choi, H-I, Park, S, Jaekal, E, Lee, G-Y, Cho, YI, et al. A two-factor model better explains heterogeneity in negative symptoms: evidence from the positive and negative syndrome scale. Front Psychol. (2016) 7:707. doi: 10.3389/fpsyg.2016.00707
52. Kaiser, HF . An index of factorial simplicity. Psychometrika. (1974) 39:31–6. doi: 10.1007/BF02291575
53. Tucker, LR, and Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika. (1973) 38:1–10. doi: 10.1007/BF02291170
54. MacCallum, RC, Browne, MW, and Sugawara, HM. Power analysis and determination of sample size for covariance structure modeling. Psychol Methods. (1996) 1:130–49. doi: 10.1037/1082-989X.1.2.130
55. Lt, H, and Bentler, PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model Multidiscip J. (1999) 6:1–55. doi: 10.1080/10705519909540118
56. Gerbing, DW, and Anderson, JC. The effects of sampling error and model characteristics on parameter estimation for maximum likelihood confirmatory factor analysis. Multivariate Behav Res. (1985) 20:255–71. doi: 10.1207/s15327906mbr2003_2
57. Sabe, M, Zhao, N, Kaiser, SJN, and Reviews, B. Cannabis, nicotine and the negative symptoms of schizophrenia: systematic review and meta-analysis of observational studies. Neurosci Biobehav Rev. (2020) 116:415–25. doi: 10.1016/j.neubiorev.2020.07.007
58. Richter, J, Hölz, L, Hesse, K, Wildgruber, D, and Klingberg, S. Measurement of negative and depressive symptoms: discriminatory relevance of affect and expression. Eur Psychiatry. (2019) 55:23–8. doi: 10.1016/j.eurpsy.2018.09.008
59. Lyngstad, SH, Gardsjord, ES, Engen, MJ, Haatveit, B, Ihler, HM, Wedervang-Resell, K, et al. Trajectory and early predictors of apathy development in first-episode psychosis and healthy controls: a 10-year follow-up study. Eur Arch Psychiatry Clin Neurosci. (2020) 270:709–22. doi: 10.1007/s00406-020-01112-3
60. Carpenter, WT Jr, Heinrichs, DW, and Alphs, LD. Treatment of negative symptoms. Schizophr Bull. (1985) 11:440–52. doi: 10.1093/schbul/11.3.440
61. Kirkpatrick, B . Developing concepts in negative symptoms: primary vs secondary and apathy vs expression. J Clin Psychiatry. (2014) 75:3–7. doi: 10.4088/JCP.13049su1c.01
62. Gard, DE, Kring, AM, Gard, MG, Horan, WP, and Green, MF. Anhedonia in schizophrenia: distinctions between anticipatory and consummatory pleasure. Schizophr Res. (2007) 93:253–60. doi: 10.1016/j.schres.2007.03.008
63. Horan, WP, Green, MF, Kring, AM, and Nuechterlein, KH. Does anhedonia in schizophrenia reflect faulty memory for subjectively experienced emotions? J Abnorm Psychol. (2006) 115:496–508. doi: 10.1037/0021-843X.115.3.496
64. Juckel, G, Schlagenhauf, F, Koslowski, M, Wüstenberg, T, Villringer, A, Knutson, B, et al. Dysfunction of ventral striatal reward prediction in schizophrenia. NeuroImage. (2006) 29:409–16. doi: 10.1016/j.neuroimage.2005.07.051
65. Mote, J, Minzenberg, MJ, Carter, CS, and Kring, AM. Deficits in anticipatory but not consummatory pleasure in people with recent-onset schizophrenia spectrum disorders. Schizophr Res. (2014) 159:76–9. doi: 10.1016/j.schres.2014.07.048
66. Barch, DM, Pagliaccio, D, and Luking, K. Mechanisms underlying motivational deficits in psychopathology: similarities and differences in depression and schizophrenia In: EH Simpson and PD Balsam, editors. Behavioral neuroscience of motivation. Cham: Springer International Publishing (2016). 411–49.
67. Husain, M, and Roiser, JP. Neuroscience of apathy and anhedonia: a transdiagnostic approach. Nat Rev Neurosci. (2018) 19:470–84. doi: 10.1038/s41583-018-0029-9
68. Galderisi, S, Kaiser, S, Bitter, I, Nordentoft, M, Mucci, A, Sabé, M, et al. EPA guidance on treatment of negative symptoms in schizophrenia. Eur Psychiatry. (2021) 64:e21. doi: 10.1192/j.eurpsy.2021.13
69. Stiekema, APM, Islam, MA, Liemburg, EJ, Castelein, S, van den Heuvel, ER, van Weeghel, J, et al. Long-term course of negative symptom subdomains and relationship with outcome in patients with a psychotic disorder. Schizophr Res. (2018) 193:173–81. doi: 10.1016/j.schres.2017.06.024
70. Chang, WC, Ho, RWH, Tang, JYM, Wong, CSM, Hui, CLM, Chan, SKW, et al. Early-stage negative symptom trajectories and relationships with 13-year outcomes in First-episode nonaffective psychosis. Schizophr Bull. (2018) 45:610–9. doi: 10.1093/schbul/sby115
71. Austin, SF, Mors, O, Budtz-Jørgensen, E, Secher, RG, Hjorthøj, CR, Bertelsen, M, et al. Long-term trajectories of positive and negative symptoms in first episode psychosis: a 10year follow-up study in the OPUS cohort. Schizophr Res. (2015) 168:84–91. doi: 10.1016/j.schres.2015.07.021
72. Herbener, ES, and Harrow, M. Longitudinal assessment of negative symptoms in schizophrenia/schizoaffective patients, other psychotic patients, and depressed patients. Schizophr Bull. (2001) 27:527–37. doi: 10.1093/oxfordjournals.schbul.a006893
73. Blanchard, JL, Horan, WP, and Brown, SA. Diagnostic differences in social anhedonia: a longitudinal study of schizophrenia and major depressive disorder. J Abnorm Psychol. (2001) 110:363–71. doi: 10.1037/0021-843X.110.3.363
74. Hoffman, RE, and Rakfeldt, J. Cognition, negative symptoms, and diagnosis: a comparison of schizophrenic, bipolar, and control samples. Neurosciences. (1997) 9:81–9.
75. Lewine, RR . A discriminant validity study of negative symptoms with a special focus on depression and antipsychotic medication. Am J Psychiatry. (1990) 147:1463–6.
76. D’Souza, DC, Abi-Saab, WM, Madonick, S, Forselius-Bielen, K, Doersch, A, Braley, G, et al. Delta-9-tetrahydrocannabinol effects in schizophrenia: implications for cognition, psychosis, and addiction. Biol Psychiatry. (2005) 57:594–608. doi: 10.1016/j.biopsych.2004.12.006
Keywords: bipolar disorder, negative symptoms, diminished expression, apathy, cannabis use
Citation: Ihler HM, Lyngstad SH, Mørch-Johnsen LE, Lagerberg TV, Melle I and Romm KL (2023) A transdiagnostic approach to negative symptoms: exploring factor structure and negative symptoms in bipolar disorders. Front. Psychiatry 14:1136097. doi: 10.3389/fpsyt.2023.1136097
Edited by:
Daniel Stjepanović, The University of Queensland, AustraliaReviewed by:
Matthias Kirschner, University of Zurich, SwitzerlandRaimo Kalevi Rikhard Salokangas, University of Turku, Finland
Copyright © 2023 Ihler, Lyngstad, Mørch-Johnsen, Lagerberg, Melle and Romm. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henrik Myhre Ihler, henrikih@uio.no;;heihle@ous-hf.no