 Kinga Amália Sándor-Bajusz1*
Kinga Amália Sándor-Bajusz1* Tímea Dergez2
Tímea Dergez2 Edit Molnár1Kinga Hadzsiev3
Edit Molnár1Kinga Hadzsiev3 Ágnes Till3Anna Zsigmond3Attila Vástyán4
Ágnes Till3Anna Zsigmond3Attila Vástyán4 Györgyi Csábi1
Györgyi Csábi1- 1Division of Child and Adolescent Psychiatry, Department of Pediatrics, Medical School and Clinical Center, University of Pécs, Pécs, Hungary
- 2Institute of Bioanalysis, Medical School and Clinical Center, University of Pécs, Pécs, Hungary
- 3Department of Medical Genetics, Medical School and Clinical Center, University of Pécs, Pécs, Hungary
- 4Division of Pediatric Surgery, Department of Pediatrics, Medical School and Clinical Center, University of Pécs, Pécs, Hungary
Introduction: The higher rate of neuropsychiatric disorders in individuals with non-syndromic orofacial clefts has been well documented by previous studies. Our goal was to identify children with non-syndromic orofacial clefts that are at risk for abnormal neurodevelopment by assessing their developmental history and present cognitive functioning.
Materials and methods: A single-center, case-controlled study was carried out at the Department of Pediatrics of the University of Pécs in Hungary. The study consisted of three phases including questionnaires to collect retrospective clinical data and psychometric tools to assess IQ and executive functioning.
Results: Forty children with non-syndromic oral clefts and 44 age-matched controls participated in the study. Apgar score at 5 min was lower for the cleft group, in addition to delays observed for potty-training and speech development. Psychiatric disorders were more common in the cleft group (15%) than in controls (4.5%), although not statistically significant with small effect size. The cleft group scored lower on the Continuous Performance Test. Subgroup analysis revealed significant associations between higher parental socio-economic status, academic, and cognitive performance in children with non-syndromic orofacial clefts. Analyzes additionally revealed significant associations between early speech and language interventions and higher scores on the Verbal Comprehension Index of the WISC-IV in these children.
Discussion: Children with non-syndromic orofacial clefts seem to be at risk for deficits involving the attention domain of the executive system. These children additionally present with difficulties that affect cognitive and speech development. Children with non-syndromic orofacial clefts show significant skill development and present with similar cognitive strengths as their peers. Longitudinal studies with larger sample sizes are needed to provide more conclusive evidence on cognitive deficits in children with non-syndromic orofacial clefts at risk for neurodevelopmental difficulties.
1. Introduction
Orofacial clefts are the most common craniofacial anomalies that affect the lip, palate and/or both structures (Harila et al., 2013; Li et al., 2019). Approximately 30% of oral clefts are associated with a known genetic syndrome (syndromic clefts), however, the remaining 70% occur without a known identified syndrome (non-syndromic clefts; Mossey and Modell, 2012; Saleem et al., 2019). Orofacial clefts (OFCs) are divided into three different subtypes on an anatomically basis; cleft lip (CL), cleft lip and palate (CLP) and cleft palate only (CPO; Lithovius et al., 2014). The higher risk of mental disorders in individuals born with non-syndromic OFCs is well documented in the literature (Richman and Ryan, 2003; Nopoulos et al., 2005, 2010; Boes et al., 2007; Richman et al., 2012; Pedersen et al., 2016; Tillman et al., 2018; Gallagher and Collett, 2019). These children are disproportionately afflicted by psychiatric disorders including schizophrenia, intellectual disability, autism spectrum disorder, anxiety disorders and ADHD (Pedersen et al., 2016; Ansen-Wilson et al., 2018; Tillman et al., 2018). Children with non-syndromic OFCs are also at high risk for learning disabilities (Richman and Ryan, 2003; Tillman et al., 2018; Gallagher and Collett, 2019). Multiple stress factors including repetitive cleft repair surgeries, aesthetics, and functional consequences such as speech difficulty were believed to be the basis of such deficits (Gallagher and Collett, 2019). However, the underlying mechanisms for these deficits have not been clarified (Yang et al., 2012; Gallagher and Collett, 2019). A unified maldevelopment of the brain and facial structures is a possible etiology behind the observed neuropsychiatric disorders in this patient population (Speltz, 2000; Nopoulos et al., 2005; Boes et al., 2007; Weinberg et al., 2009; Yang et al., 2012; Adamson et al., 2014; Ansen-Wilson et al., 2018; Gallagher and Collett, 2019).
Executive dysfunction occurs when cognitive skills responsible for organizing and self-regulating behaviors are impaired (Shaheen, 2014; Zelazo, 2015). Executive functions are interconnected with the maturation of the prefrontal cortex, and their dysfunctions are common in neurodevelopmental and psychiatric disorders (Shaheen, 2014; Zelazo, 2015; Bausela-Herreras et al., 2019; Faedda et al., 2019). Specific patterns of executive dysfunction manifest according to different types of neurodevelopmental disorder and may even be a precursor before the diagnosis of these conditions (Zelazo, 2015; Bausela-Herreras et al., 2019; Otterman et al., 2019). Neuroimaging studies and the underlying cognitive deficits suggest that frontal and prefrontal cortical function may be impaired in children with non-syndromic OFCs (Nopoulos et al., 2010; Adamson et al., 2014; Chollet et al., 2014), and recommend further examination of executive functioning during follow-up (Tillman et al., 2018). Previous studies have examined the executive system in children with non-syndromic OFCs (Nopoulos et al., 2002; Laasonen et al., 2004; Conrad et al., 2009; Lemos and Feniman, 2010; Bodoni et al., 2021), but screened only one or two of its dimensions. It is often unclear whether syndromic participants were excluded from these studies (Gallagher and Collett, 2019), and may include a mixed population of both syndromic and non-syndromic forms (Nopoulos et al., 2000, 2002). Underlying genetic abnormalities—which are present in syndromic oral clefts—often affect proper brain development and function (McDonald-McGinn et al., 2015; Berg et al., 2016) and may therefore misrepresent the non-syndromic population (Rincic et al., 2016; Sándor-Bajusz et al., 2022).
The primary goal of our study was to screen cognitive deficits in children with non-syndromic OFCs to identify an at-risk subpopulation for neurodevelopmental disorders. We further aimed to identify risk factors that may additionally affect the overall neurodevelopmental course of these children. We hypothesized that children with non-syndromic OFCs would present with more cognitive difficulties compared to their non-cleft peers.
2. Materials and methods
2.1. Design
A single-center, case-controlled study was carried out at the Department of Pediatrics of the University of Pécs in Hungary. The study was approved by the Regional Ethics Committee of the University of Pécs (approval number: 7967-PTE 2020) and was performed in line with the principles of the Declaration of Helsinki. Permission to utilize the materials in the study was granted by the copyright holders (PsyWay, 2020).
2.2. Participants
All participating children with non-syndromic OFCs (further mentioned as the cleft group) are patients of the Cleft Team of the Pediatric Surgery Unit, Department of Pediatrics of the University of Pécs. The inclusion criteria consisted of the following: children with non-syndromic OFCs, 6–16 years old and an IQ ≥ 70. An OFC was considered non-syndromic when the cleft was the only single malformation without additional physical or developmental anomalies (Bjørnland et al., 2021). Controls were recruited from the community of Baranya County, specifically from public elementary, high schools, and post advertisements on social media. The inclusion criteria of the controls included the following: healthy children born without oral clefts, 6–16 years old and IQ ≥ 70. Medical geneticists examined all participants of the cleft group to rule out the presence of additional congenital malformations and/or underlying syndromes. The study was carried out between July 2020 and March 2022 in the Department of Pediatrics of the University of Pécs, Hungary. Informed consent was obtained from the parents and participants in the study.
2.3. Materials
Initially all psychometric tests were completed on site. Due to the ongoing COVID-19 pandemic, parts of the study were completed online; this included the questionnaires and the four cognitive tests (Stroop, TOL, CPT, and Corsi). Measurements that required in-person completion (IQ test) were postponed onto a later period once the pandemic situation improved.
2.3.1. Questionnaires
A parental questionnaire was developed for the study to collect demographic data. This included prenatal and postnatal history, birth, motor and language development, education, previous psychiatric treatment, and history of somatic and neuropsychiatric disorders. Parental socio-economic data were additionally collected, including parental age, education, and employment status. Parents were also asked regarding family history of neuropsychiatric disorders and/or any previous psychiatric treatment. The Hungarian version of the Child Behavior Checklist (CBCL) was used to screen for behavioral and emotional problems in children and adolescents during the previous 6 months (Achenbach, 1991; Rózsa et al., 1999).
2.3.2. Computer-based cognitive tests
Four computer-based tests were used to assess the main domains of executive functioning. All tests were provided by the Psyway Hungarian psychometric website and all tests are standardized and norm-referenced (PsyWay, 2020). Each cognitive test is summarized in Table 1.
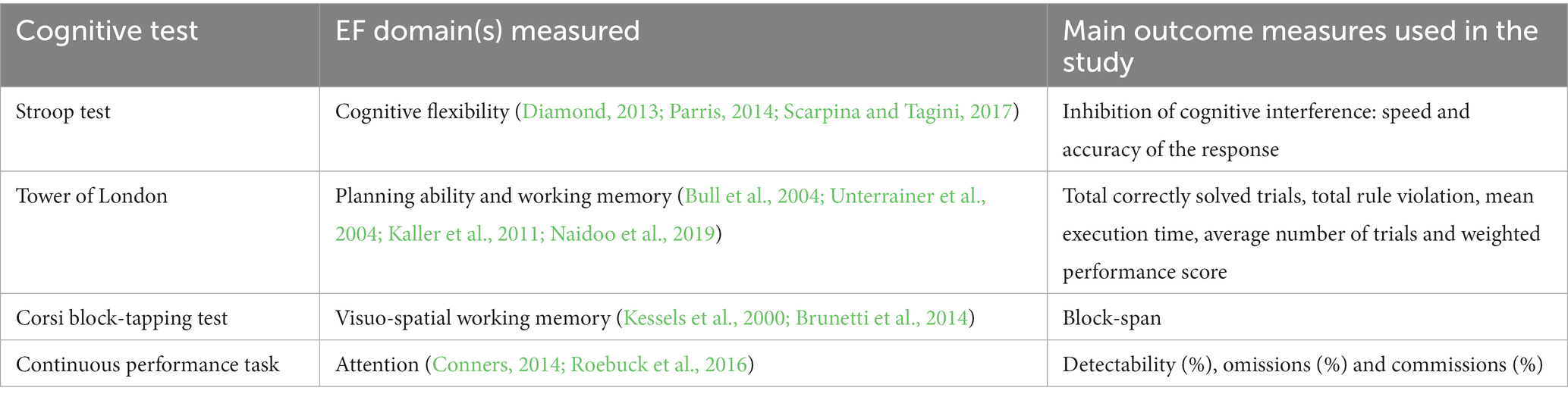
Table 1. Cognitive tests used in the study to measure executive functioning.
2.3.3. Intelligence test: WISC-IV (Wechsler intelligence scale for children—Fourth edition)
We used the official Hungarian version of the WISC-IV (Nagyné Réz et al., 2007) to measure full-scale IQ, important for the assessment of executive functioning (Grizzle, 2011; Ardila, 2018).
2.4. Procedure
The study was divided into three phases, which begun by completing two online questionnaires (Phase 1) followed by online cognitive tasks (Phase 2) and an in-person IQ test (Phase 3, see Figure 1).
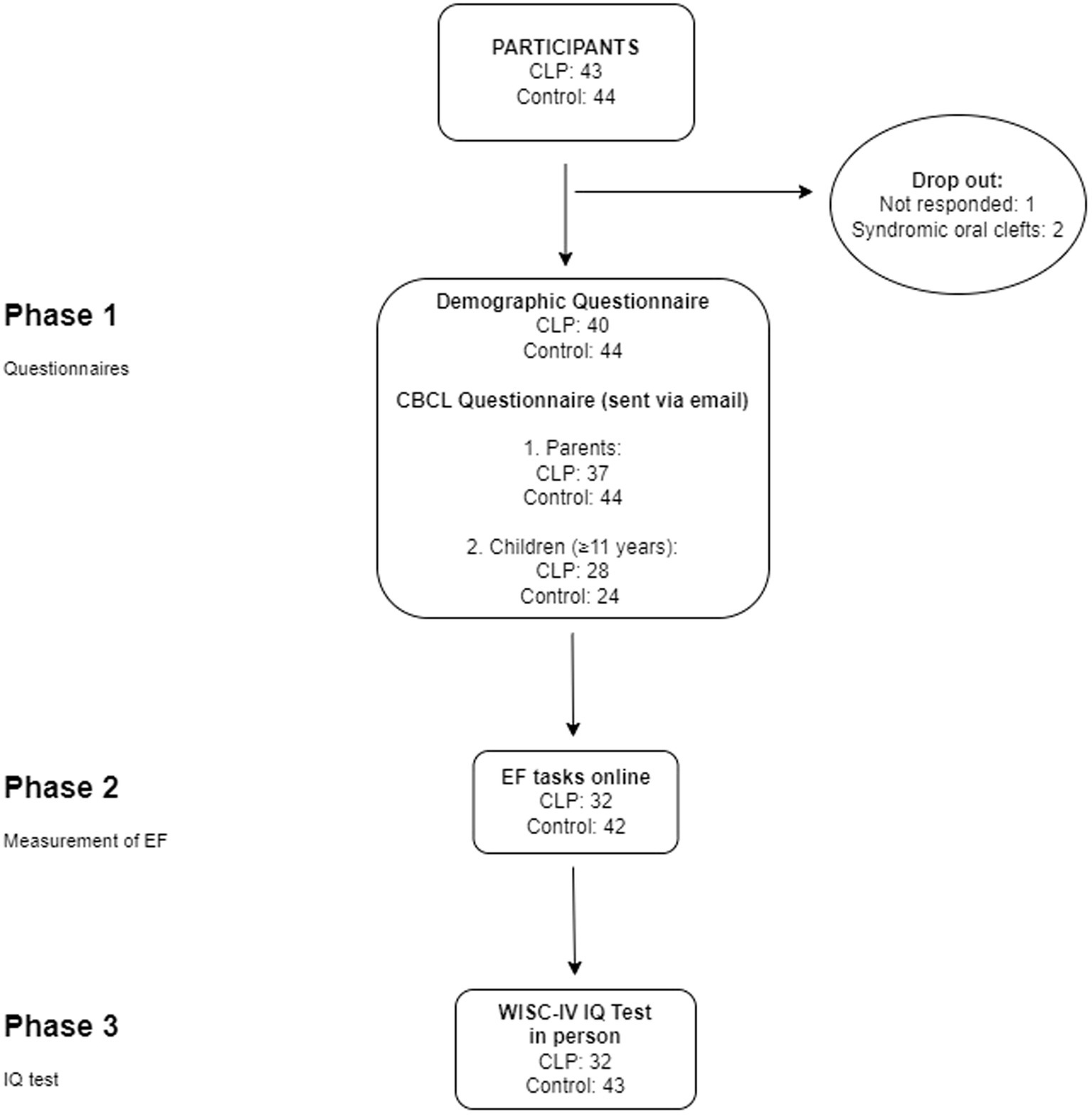
Figure 1. Study flow. The analyzes were divided into three phases. The number of the participants are provided for each phase (CLP, cleft lip and/or palate group; EF, executive function; IQ, intelligence quotient).
2.5. Statistics
Statistical analysis was carried out using IBM SPSS Statistics 28 Software. A descriptive statistical analysis was performed. The primary aim of the analysis was to compare the differences in the results of cognitive tests (London Tower, Stroop, Corsi, and Continuous Performance Test), IQ (WISC-IV), CBCL (Child Behavior Checklist) and the demographic parameters between the two study groups. Occupational statuses of the parents were classified as follows: employed, not employed, or retired. Academic levels of the parents were initially grouped into basic (elementary, lower secondary education), intermediate (upper secondary) and advanced (college or university). We later grouped these levels as either higher education (upper secondary education, college, or university) or lower education (elementary, lower secondary education) to increase statistical power.
The raw score is an untransformed score from a measurement of the above listed cognitive tests and the CBCL questionnaire. The raw scores were converted into a scale called T-score scale, which assumes a normal distribution with the mean = 50 and the standard deviation = 10. The T-scores of all psychometric tests were expressed as means ± standard deviations. The categorical data of the cleft and control groups were analyzed using contingency tables and the chi-squared or Fischer’s test, as appropriate. For quantitative variables, two-sided independent samples Student’s t-test were used. The Welch test was applied in cases when the variance was not homogenous. Analysis of variance (ANOVA) was used to test the difference among more than two groups (e.g., in case of analysis based on the type of cleft). These variables follow a normal distribution. Statistical significance was established as a value of p of <0.05. Effect sizes were defined as Cohen’s d value in case of two independent groups, η2 in case of ANOVA test, and ϕ value in case of Chi-square test (Coe, 2002).
3. Results
3.1. Participants
We recruited 43 children with non-syndromic OFCsand 44 controls for the study. Past medical history revealed two syndromic OFCs and these participants were excluded from the study. One participant of the cleft group was lost to follow up. The data of 84 study participants were analyzed (see Figure 1).
3.2. Cognitive functioning
The CPT revealed differences between the two groups: the cleft group scored lower on detectability (%) than controls (p = 0.022, d = 0.55, see Table 2). They also missed more targets than controls (p = 0.058, d = 0.46, see Table 2). We did not observed differences for the remaining cognitive test results (see Supplementary Tables 1–3). None of the participants scored below average in any of the dimensions of the WISC-IV, however controls scored higher on the PRI and WMI subtests (see Supplementary Table 4).
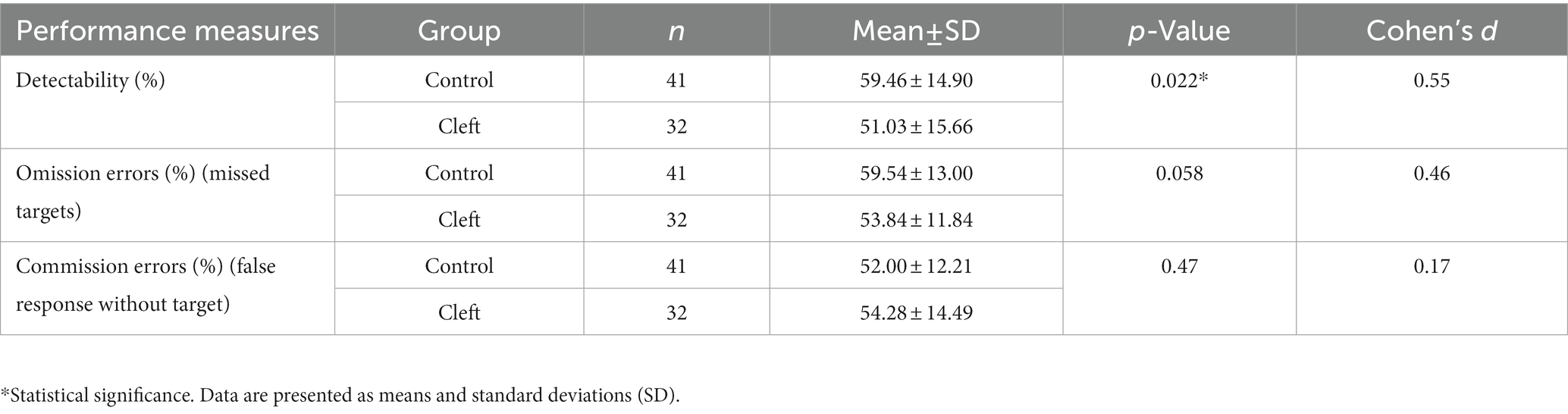
Table 2. Results of the CPT (continuous performance task).
3.3. Questionnaires
3.3.1. CBCL questionnaire
3.3.1.1. Children (self-report)
Two dimensions of the CBCL showed significant differences between the groups: controls reported higher symptoms of externalization, somatic, attention, oppositional, and behavioral problems than clefts. Clefts reported higher symptoms of affective problems (see Table 3).
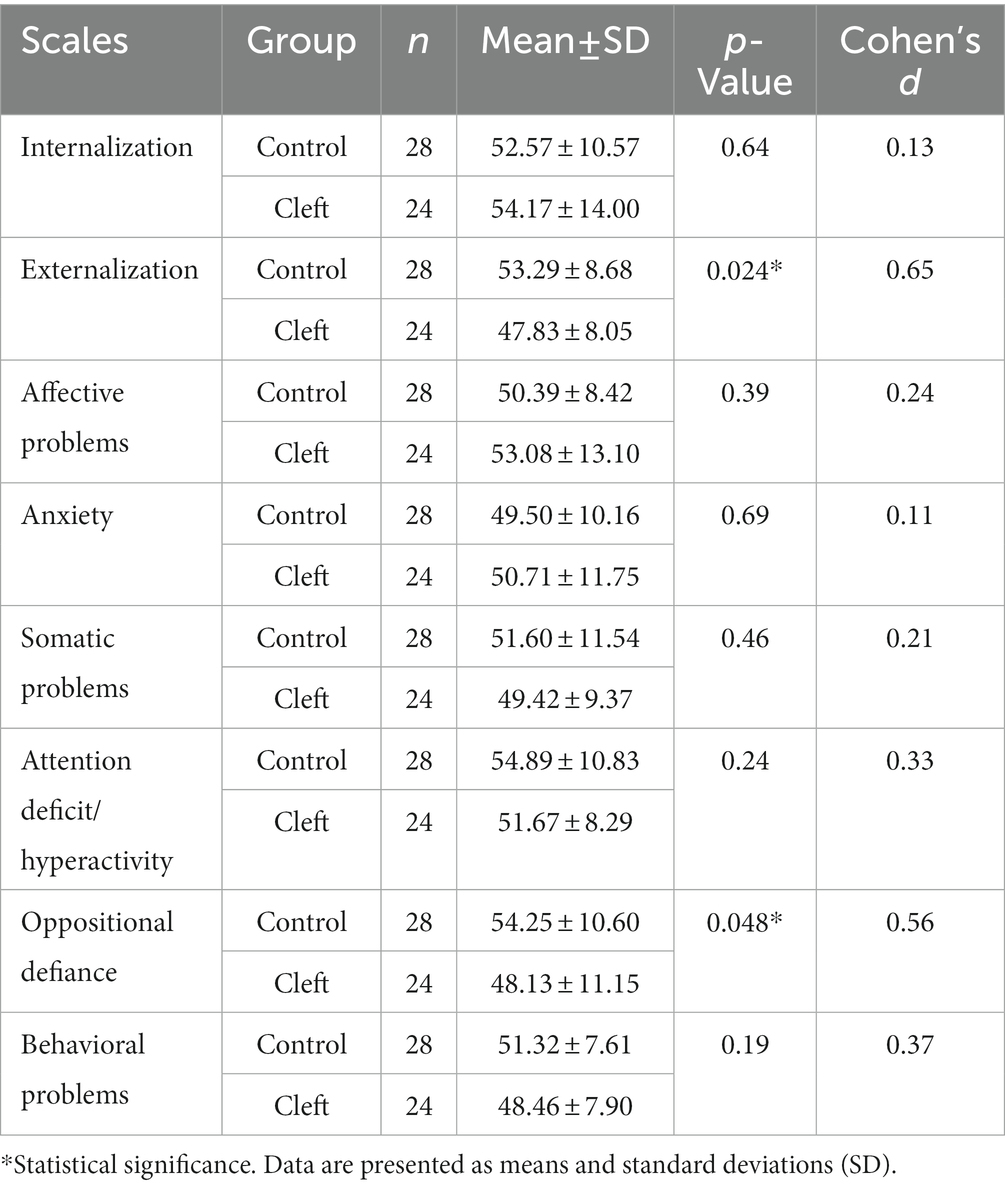
Table 3. Results of the CBCL self-report.
3.3.1.2. Parental report
Parents of the controls reported higher symptoms across all scales of the CBCL compared to parents of the cleft group, with small effect sizes (see Supplementary Table 5).
3.3.2. Demographic measures
3.3.2.1. Children
3.3.2.1.1. Cleft status
There were no significant differences between the age of cleft versus controls (see Table 4). More than half of the cleft group was represented by boys (56.6%), while controls had more girl participants (67.7%, p = 0.031, ϕ = 0.24). Three subtypes of OFCs were present in the cleft group: 45% with cleft lip and palate (CLP), 37.5% with cleft lip (CL) and 17.5% with cleft palate only (CPO). Left-sided (32.5%) and bilateral (32.5%) OFCs were the most common. Overall, 29.16% of the cleft group reported their repaired OFCs as a current medical condition. All participants of the cleft group had repaired clefts, and none of these children had persistent hearing deficiency.
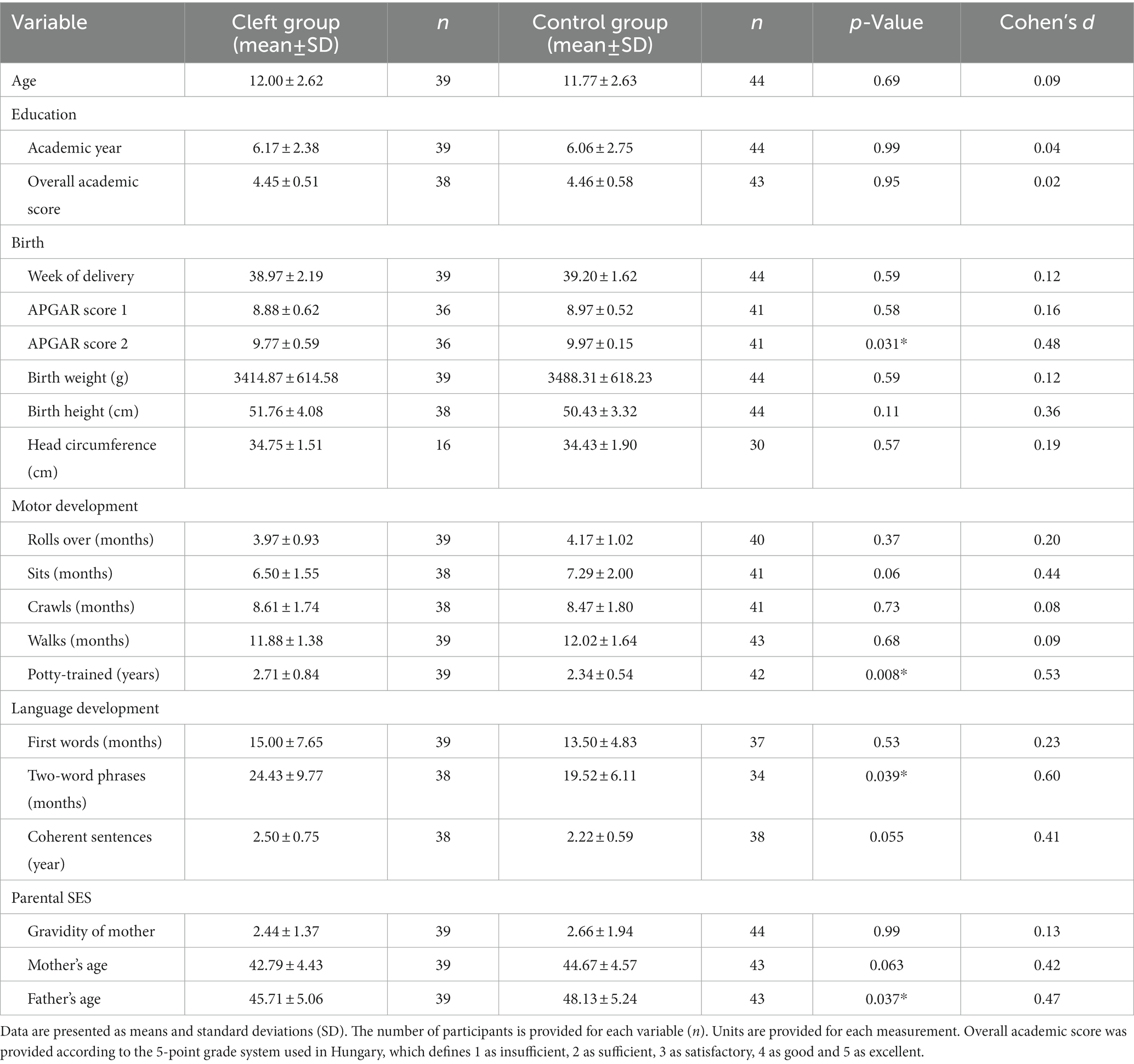
Table 4. Demographic data of the study groups.
3.3.2.1.2. Academic performance and past psychiatric history
We observed no differences in the overall academic score; both clefts and controls achieved a good overall score in the current academic year (see Table 4). Preschool integration was significantly more difficult for the cleft group compared to controls (p = 0.025, ϕ = 0.26). Both study groups did well later in preschool without requiring grade repetition (p = 0.96, ϕ = 0.005). Children of the cleft group were examined by pedagogical professional services more often than controls (p < 0.001, ϕ = 0.49). Participants in the cleft group required special education plans more often than controls (p = 0.016, ϕ = 0.29). There were no differences in the rate of elementary grade repetition between clefts and controls (p = 0.60, ϕ = 0.073). We observed a higher proportion of psychiatric disorders in the cleft group (15%) compared to controls (4.5%; p = 0.14, ϕ = 0.18). The cleft group received previous psychiatric therapy more often (15%) than controls (0%; p = 0.009, ϕ = 0.29). The reported psychiatric diagnoses were ADHD (50%), borderline personality disorder (12.5%), learning disability (12.5%), depression (12.5%) and anxiety disorder (12.5%). Children in the cleft group required additional support for learning, psychological and physical well-being during their education more often than controls (p < 0.001, ϕ = 0.49), specifically speech and language therapy (p < 0.001, ϕ = 0.51). Overall, 4.5% of controls reported having a psychiatric comorbidity, which included dyslexia (50%) and ADHD (50%).
3.3.2.1.3. Pregnancy and developmental history
All participating children were born full-term via uncomplicated births. No differences were observed in the total number of pregnancies, and natural and caesarian delivery (p = 0.63, ϕ = 0.05). Apgar score at 5 min was lower in the cleft group (p = 0.031, d = 0.48, see Table 4). No differences were observed in the week of delivery, head circumference and birthweight between the two study groups (see Table 4). The need for postnatal supportive care did not differ between clefts and controls (respiratory support, surfactant therapy, phototherapy, antibiotics, and transfusions; p = 0.23, ϕ = 0.13). Mothers of the cleft group reported feeding (p = 0.007, ϕ = 0.29) and hearing (p < 0.001, ϕ = 0.51) difficulties more often than mothers of controls. The cleft group developed motor skills (roll over, sitting) later than controls, however the effect sizes were small (see Table 4). The cleft group was potty trained at an older age than controls (p = 0.008, d = 0.53, see Table 4). Parents of the cleft group reported that their children were able to form two-word sentences at a later age compared to reports of parents of controls (p = 0.039, d = 0,60, see Table 4). First words and coherent sentences were also spoken later by children in the cleft group (See Table 4).
3.3.2.2. Parents
3.3.2.2.1. Age, marital and employment status
Parents of the control group were older at the time of assessment than those of the cleft group (see Table 4). Mothers of the cleft group gave birth to their child at an older age than mothers of controls (p = 0.50, d = 0.05). Most parents of clefts (70.0%) and controls (69.8%) were married, and no differences were observed between the relationship statuses of parents of both groups (p = 0.47, ϕ = 0.08). The employment statuses of fathers (p = 0.42, ϕ = 0.25) and mothers (p = 0.86, ϕ = 0.19) did not differ between the two groups.
3.3.2.2.2. Past psychiatric and academic history
History of psychiatric disorders was more often reported by parents of controls (27.3%) compared to clefts (7.5%; p = 0.010, ϕ = 0.39). One parent of the control group reported to have history of anxiety, but most parents did not further specify these conditions. The majority of reported psychiatric diagnoses in the family of the cleft group were depression (75%) or anxiety disorders (25%). Most parents completed high school and/or had a university degree. Significant differences were not observed in the mother’s level of education between the two study groups (p = 0.29, ϕ = 0.12). Fathers of the control group achieved a higher degree of education than fathers of the cleft group who had lower secondary education (p = 0.024, ϕ = 0.25).
3.4. Subgroup analysis of the cleft group
Following data collection and analyzes, we hypothesized that the more complex cleft subtypes would obtain lower scores on the IQ test, and present with a history of atypical neurodevelopment, academic difficulties, and psychiatric disorders. We further assumed that early interventions for speech and language would positively impact cognitive development, and the later would be reflected in the IQ score of these children.
A total of 10 girls and 30 boys were tested in the cleft group (see Table 5): Boys became potty-trained earlier (2.39 years) than girls (3.50 years; p = 0.037, d = 0.79). Hearing difficulties were in highest proportion for CPO (57.1%) than for CL (13.3%) and CPL (44.4%) however with small effect size (p = 0 0.063, d = 0.36). In the analysis according to types of clefts, CLP was the subtype that was most often referred to special education services: CL in 40%, CPO in 14% and CLP in 72% of the cases (p = 0.023, d = 0.29). CLP subtype was diagnosed with psychiatric comorbidities in highest proportion (22.2%) compared to CL (13.3%) and CPO (0%) (p = 0.53, d = 0.22). CLP subtype had additionally received previous psychiatric care in highest proportion (22.2%) compared to the rest of the cleft subtypes (p = 0.61, d = 0.23). Left (15.4%) and bilateral (30.8%) sided clefts presented the highest proportion of psychiatric diagnoses (p = 0.27, d = 0.35). The relationship between parental socioeconomic status (SES) and children’s cognitive performance.
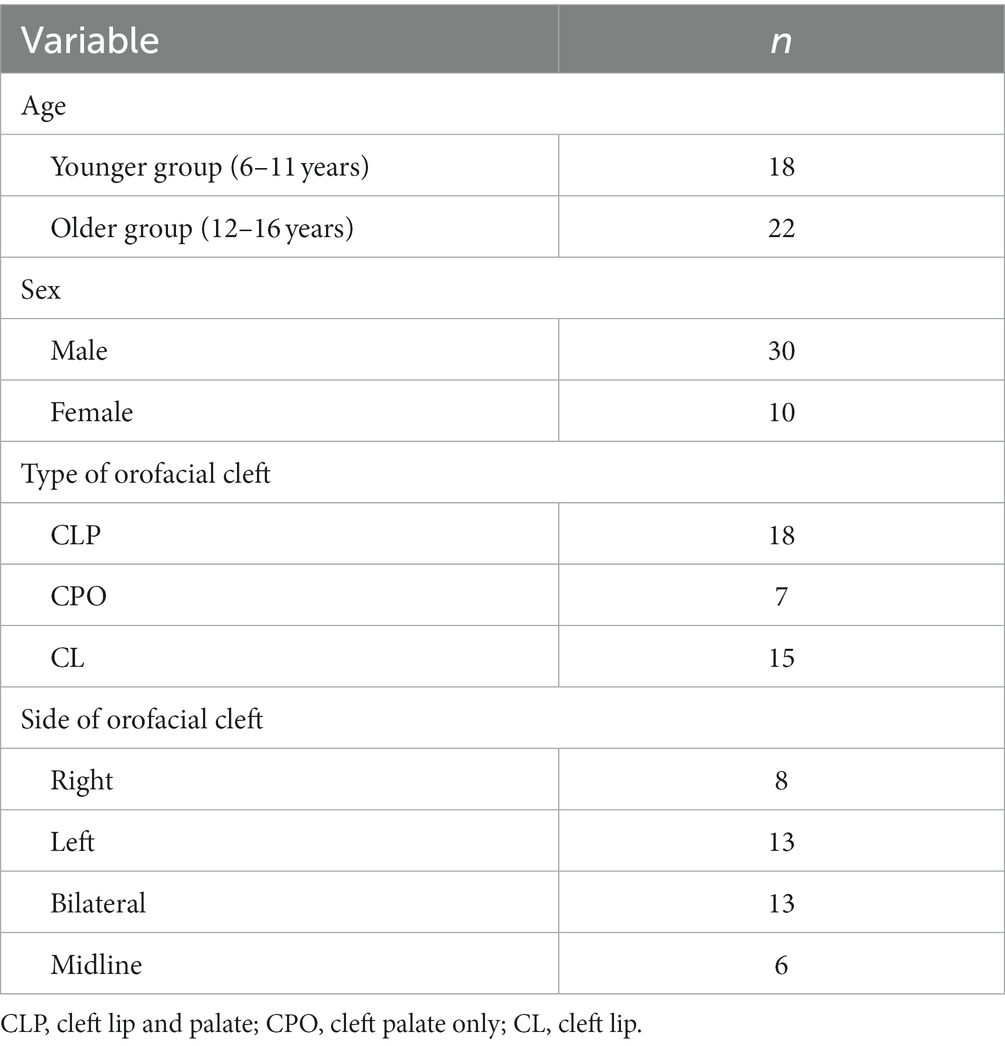
Table 5. Demographical data of the orofacial cleft group.
We aimed to explore variables of parental SES that may influence the outcome of academic and cognitive performance. Fathers with a high academic background reached a higher overall academic average compared to children with fathers of low academic background (p = 0.005, d = 0.79). Children with mothers of a high academic background reached a higher overall academic average compared to children with mothers of a low academic background (see Table 6). The same pattern was observed for the IQ scores: children who scored higher on almost all indexes of the IQ had parents with a higher academic background (see Supplementary Tables 6, 7). A total of 44.4% of cleft children with single parents had a psychiatric condition(s), while only 6.5% had psychiatric condition(s) when raised by married parents (p = 0.016, d = 0.44).
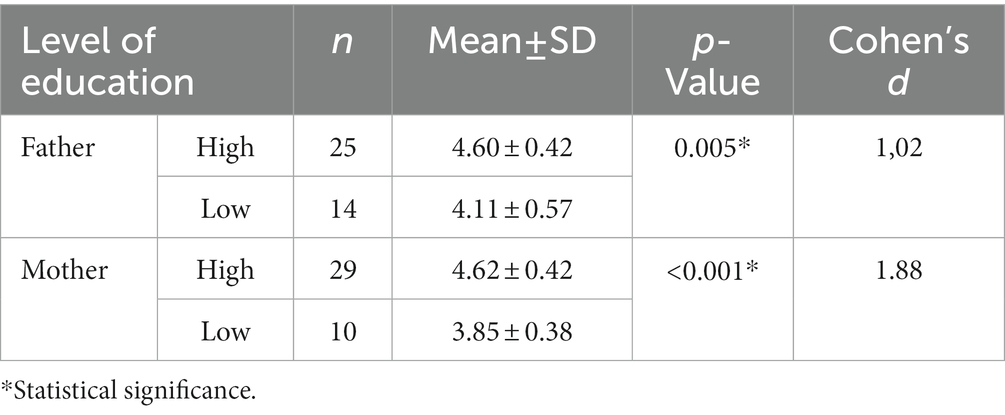
Table 6. Parental level of education in relation to overall academic average of the cleft group.
3.4.1. The relationship between speech/language therapy and the IQ score
We explored the effect of speech and language therapy on IQ scores and overall academic average. FS-IQ and VCI scores were higher for children who received therapy (see Table 7). Overall academic average was higher for cleft participants who did not undergo therapy, although with small effect size (see Table 7). A one-way ANOVA was performed to compare the effect of the affected side of the cleft (left, right, bilateral and midline) on IQ scores. We observed differences for continuous variables in WMl when tested by the affected side (p = 0.037, η2 = 0.27, see Supplementary Table 8).
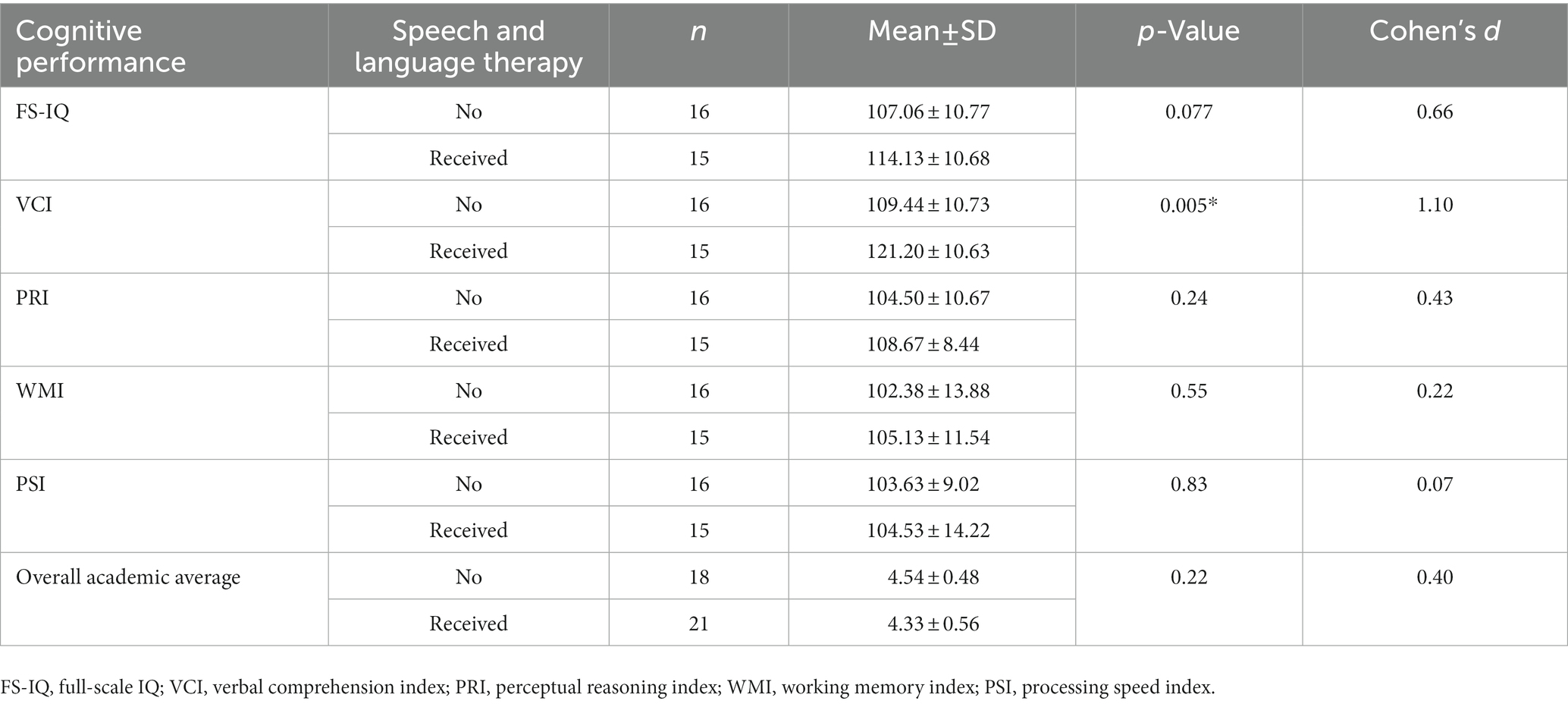
Table 7. Effect of speech and language therapy on IQ scores and overall academic average.
4. Discussion
We analyzed the cognitive functioning and clinical characteristics of 40 children with non-syndromic OFCs and 44 age-matched controls. All participants performed well on the executive function tasks, except for the CPT; children with non-syndromic OFCs scored lower and missed targets more often than controls (omission errors, see Table 4). The results raise the possibility of an underlying attention deficit in these children described previously by other studies (Nopoulos et al., 2010; Pedersen et al., 2016). The two groups scored within normal ranges on the IQ test, however controls scored higher on the PRI and WMI subtests. Subgroup analysis of the cleft group revealed significant relationships between parental SES and IQ scores: children of parents with a higher educational background scored significantly higher on the IQ test, specifically reflected in perceptual reasoning and the full-scare IQ score. We also observed a significant association between early intervention and IQ: children who received speech and language therapy achieved higher scores specifically reflected in the verbal component (VCI) of the WISC-IV (see Table 7). We further observed the influence of family structure on mental health outcomes: children raised by single parents were diagnosed with psychiatric conditions more often than children raised by married parents.
Children of the control group reported more symptoms of externalizing disorders (attention, oppositional, behavioral), while children with non-syndromic OFCs reported symptoms of internalizing disorders (affective, anxiety) more than controls (Table 3). Parents of the control group reported higher symptoms across all scales of the CBCL. However, retrospective analysis of past medical history revealed that children with non-syndromic OFCs were clinically diagnosed with psychiatric disorders at a higher proportion and received psychiatric support more often than controls. Larger cohort studies have previously described this observation (Pedersen et al., 2016; Tillman et al., 2018). While there is a clear difference in the proportion of psychiatric disorders between our two study groups, this is not statistically detectable, and the effect size is small. A larger sample may provide conclusive evidence of this observation.
Psychiatric diagnoses varied across cleft subtypes and the affected side: the highest proportion of psychiatric diagnoses were observed in CLP, and bilateral-sided clefts. These observations may suggest that the more complicated clefts more likely present with psychiatric comorbidities (Pedersen et al., 2016; Gallagher et al., 2018). We did not observe psychiatric comorbidities in CPO children, which is in contrast with previous observations (Nilsson et al., 2015; Pedersen et al., 2016; Tillman et al., 2018; Gallagher and Collett, 2019). Interestingly, less than half (29.16%) of the cleft group participants recognized their repaired OFC as a disease or medical condition. This may indicate that the causative stressor is in fact something other than the physical awareness of the defect itself (Aleksieva et al., 2021). Apgar score at 5 min was lower for the cleft group than for controls, but clinically within the normal range. We observed no further complications in the postnatal period between the two study groups. There was a tendency of a slower onset of developmental milestones in children with OFCs; potty-training and the use of two-word phrases presented at a later age compared to controls, also within clinical ranges. Children with OFCs experienced difficulties integrating into preschool, and most required additional support for learning, psychological and physical well-being throughout their education. Difficulties with speech and language development are known to be a consequence related to the primary defect; however, studies highlight the possibility of a central auditory dysfunction, which may cause developmental issues that affect these skills (Čeponien et al., 1999; Yang et al., 2012; Conrad et al., 2021). Based on our results, children with non-syndromic OFCs initially have a slower development and experience difficulties integrating into preschool; however, it seems that they go through a “catch-up phase” around school age and perform well—almost equal to their peers—throughout elementary and high school.
Our study has important limitations. The small sample size of the study, limited us to further explore relationships within gender, cleft subtype and affected side. The sample size varied across the different phases of the study. Most of the children in the cleft group were represented by males. The retrospective nature of the questionnaires may have created bias in the data provided. We could not assess the baseline level of executive functioning prior to the interventional programs (speech and language therapy), and we may observe an overall “corrected” level of cognitive functioning. However, this study has several strengths. Our study is the first to provide data on cognitive performance and clinical characteristics of Hungarian children with non-syndromic OFCs across a wide age-range. We were able to provide data on neurodevelopmental differences in children with non-syndromic OFCs in early infancy and the preschool period. We further demonstrated how these children, despite having previous difficulties during early infancy, can “catch-up” to their peers and perform well. Early intervention, additional help in school and proper parental support seem to have a strong effect on proper cognitive development for this patient population. Our observations suggest the presence of attention deficit in children with non-syndromic OFCs in support of the higher proportion of ADHD diagnosis seen in this population compared to controls. Assessing the executive system at an earlier stage of development, prior to interventional programs, may be useful to screen and identify individuals within the cleft population who are at risk for atypical neurodevelopment.
Children with non-syndromic OFCs seem to be at risk for atypical cognitive and speech development. This may be explained by a unified brain and facial maldevelopment in utero. Future studies with large sample sizes are needed to further explore this underlying etiology to identify this subpopulation, since not all children with non-syndromic OFCs present with such difficulties. Longitudinal studies are needed to provide more evidence of baseline cognitive functioning to study early signs of atypical neurodevelopment and the effect of early interventions. Under the right environment, these children present with similar cognitive strengths as their peers and show significant skill development. A good multidisciplinary team, early interventions, special education programs, and proper parental support allow most children with non-syndromic OFCs to perform just as well as other children.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Regional Ethics Committee of the University of Pécs (approval number: 7967-PTE 2020). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author contributions
KS-B, GC, AV, and KH contributed to conception and design of the study. KS-B, ÁT, AZ, KH, EM, and AV collected the data and organized the database. GC supervised the study. TD performed the statistical analysis. KS-B wrote the first draft of the manuscript. GC and TD wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors received financial support from the University of Pécs for the open-access publication of this manuscript.
Acknowledgments
We would like to acknowledge George K.B. Sándor who has dedicated his professional career for the significant advancements in cleft repair surgery, by which he has contributed to improvements in quality of life for both orofacial cleft patients and their families. His work has greatly inspired the current research, equally dedicated to improving the clinical care of children born with orofacial clefts. GC was supported by the FIKP-IV and the TNIL Projects.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2023.1115304/full#supplementary-material
References
Achenbach, T. M. (1991). Manual for the Child Behavior Checklist/4–18 and 1991 Profile. Burlington: University of Vermont, Department of Psychiatry
Adamson, C. L., Anderson, V. A., Nopoulos, P., Seal, M. L., and da Costa, A. C. (2014). Regional brain morphometric characteristics of nonsyndromic cleft lip and palate. Dev. Neurosci. 36, 490–498. doi: 10.1159/000365389
Aleksieva, A., Begnoni, G., Verdonck, A., Laenen, A., Willems, G., and Cadenas de Llano-Pérula, M. (2021). Self-esteem and oral health-related quality of life within a cleft lip and/or palate population: a prospective cohort study. Int. J. Environ. Res. Public Health 18:6078. doi: 10.3390/ijerph18116078
Ansen-Wilson, L. J., Everson, J. L., Fink, D. M., Kietzman, H. W., Sullivan, R., and Lipinski, R. J. (2018). Common basis for orofacial clefting and cortical interneuronopathy. Transl. Psychiatry 8:8. doi: 10.1038/s41398-017-0057-7
Ardila, A. (2018). Is intelligence equivalent to executive functions? Psicothema 30, 159–164. doi: 10.7334/psicothema2017.329
Bausela-Herreras, E., Tirapu-Ustárroz, J., and Cordero-Andrés, P. (2019). Executive function deficits and neurodevelopmental disorders in childhood and adolescence. Rev. Neurol. 69, 461–469. doi: 10.33588/rn.6911.2019133
Berg, E., Haaland, Ø. A., Feragen, K. B., Filip, C., Vindenes, H. A., Moster, D., et al. (2016). Health status among adults born with an Oral cleft in Norway. JAMA Pediatr. 170, 1063–1070. doi: 10.1001/jamapediatrics.2016.1925
Bjørnland, T., Nørholt, S. E., Rasmusson, L., and Sándor, G. K. (2021). Nordic Textbook of Oral and Maxillofacial Surgery Munksgaard. Available online at: https://books.google.hu/books?id=aR1rzgEACAAJ (Accessed January 26, 2022).
Bodoni, P. S. B., Leoni, R. F., do Vale, A. B., da Silva, P. H. R., Meira Junior, S. G., Richieri Costa, A., et al. (2021). Neuropsychological functioning and its relationship with brain anatomical measures of children and adolescents with non-syndromic cleft lip and palate. Child Neuropsychol. 27, 2–16. doi: 10.1080/09297049.2020.1776240
Boes, A. D., Murko, V., Wood, J. L., Langbehn, D. R., Canady, J., Richman, L., et al. (2007). Social function in boys with cleft lip and palate: relationship to ventral frontal cortex morphology. Behav. Brain Res. 181, 224–231. doi: 10.1016/J.BBR.2007.04.009
Brunetti, R., del Gatto, C., and Delogu, F. (2014). eCorsi: Implementation and testing of the Corsi block-tapping task for digital tablets. Front. Psychol. 5:939. doi: 10.3389/fpsyg.2014.00939
Bull, R., Espy, K. A., and Senn, T. E. (2004). A comparison of performance on the towers of London and Hanoi in young children. J. Child Psychol. Psychiatry 45, 743–754. doi: 10.1111/j.1469-7610.2004.00268.x
Čeponien, R., Hukki, J., Cheour, M., Haapanen, M. L., Ranta, R., and Näätänen, R. (1999). Cortical auditory dysfunction in children with oral clefts: relation with cleft type. Clin. Neurophysiol. 110, 1921–1926. doi: 10.1016/S1388-2457(99)00152-2
Chollet, M. B., DeLeon, V. B., Conrad, A. L., and Nopoulos, P. (2014). Morphometric analysis of brain shape in children with nonsyndromic cleft lip and/or palate. J. Child Neurol. 29, 1616–1625. doi: 10.1177/0883073813510603
Coe, R. (2002). “It’s the effect size, stupid: what ‘“effect size”’ is and why it is important” in Paper presented at the British Educational Research Association Annual Conference. ed. R. Coe (Exeter: University of Exeter)
Conners, C. K. (2014). Conners CPT3, Continuous Performance Test. 3rd. Toronto: Multi-Health Systems
Conrad, A. L., Richman, L., Nopoulos, P., and Dailey, S. (2009). Neuropsychological functioning in children with non-Syndromic cleft of the lip and/or palate. Child Neuropsychol. 15, 471–484. doi: 10.1080/09297040802691120
Conrad, A. L., Wermke, K., Eisenmann, M., Kuhlmann, E., Benavides, A., Koscik, T., et al. (2021). Preliminary evaluation of pre-speech and neurodevelopmental measures in 7–11-week-old infants with isolated oral clefts. Pediatr. Res. 89, 85–90. doi: 10.1038/s41390-020-0887-5
Diamond, A. (2013). Executive functions. Annu. Rev. Psychol. 64, 135–168. doi: 10.1146/annurev-psych-113011-143750
Faedda, N., Romani, M., Rossetti, S., Vigliante, M., Pezzuti, L., Cardona, F., et al. (2019). Intellectual functioning and executive functions in children and adolescents with attention deficit hyperactivity disorder (ADHD) and specific learning disorder (SLD). Scand. J. Psychol. 60, 440–446. doi: 10.1111/sjop.12562
Gallagher, E. R., and Collett, B. R. (2019). Neurodevelopmental and academic outcomes in children with Orofacial clefts: a systematic review. Pediatrics 144, 1–10. doi: 10.1542/peds.2018-4027
Gallagher, E. R., Siebold, B., Collett, B. R., Cox, T. C., Aziz, V., and Cunningham, M. L. (2018). Associations between laterality of orofacial clefts and medical and academic outcomes. Am. J. Med. Genet. A 176, 267–276. doi: 10.1002/ajmg.a.38567
Grizzle, R. (2011). “Wechsler intelligence scale for children, fourth edition” in Encyclopedia of Child Behavior and Development. eds. S. Goldstein and J. A. Naglieri (Boston, MA: Springer US), 1553–1555.
Harila, V., Ylikontiola, L. P., Palola, R., and Sándor, G. K. (2013). Maxillary arch dimensions in cleft infants in northern Finland. Acta Odontol. Scand. 71, 930–936. doi: 10.3109/00016357.2012.734420
Kaller, C. P., Unterrainer, J. M., Stefan, K., Weisbrod, M., Debelak, R., and Aschenbrenner, S. (2011). Tower of London-Freiburg Version (TOL-F). Mödling: Schuhfried
Kessels, R. P. C., van Zandvoort, M. J. E., Postma, A., Kappelle, L. J., and de Haan, E. H. F. (2000). The Corsi block-tapping task: standardization and normative data. Appl. Neuropsychol. 7, 252–258. doi: 10.1207/S15324826AN0704_8
Laasonen, M., Haapanen, M.-L., Mäenpää, P., Pulkkinen, J., Ranta, R., and Virsu, V. (2004). Visual, auditory, and tactile temporal processing in children with Oral clefts. J. Craniofacial Surg. 15, 510–518. doi: 10.1097/00001665-200405000-00033
Lemos, I. C. C., and Feniman, M. R. (2010). Teste de Habilidade de Atenção Auditiva Sustentada (THAAS) em crianças de sete anos com fissura labiopalatina. Braz. J. Otorhinolaryngol. 76, 199–205. doi: 10.1590/S1808-86942010000200009
Li, J., Rodriguez, G., Han, X., Janečková, E., Kahng, S., Song, B., et al. (2019). Regulatory mechanisms of soft palate development and malformations. J. Dent. Res. 98, 959–967. doi: 10.1177/0022034519851786
Lithovius, R. H., Ylikontiola, L. P., Harila, V., and Sándor, G. K. (2014). A descriptive epidemiology study of cleft lip and palate in northern Finland. Acta Odontol. Scand. 72, 372–375. doi: 10.3109/00016357.2013.840737
McDonald-McGinn, D. M., Sullivan, K. E., Marino, B., Philip, N., Swillen, A., Vorstman, J. A. S., et al. (2015). 22q11.2 deletion syndrome. Nat. Rev. Dis. Primers. 1:15071. doi: 10.1038/nrdp.2015.71
Mossey, P. A., and Modell, B. (2012). Epidemiology of oral clefts 2012: an international perspective. Front. Oral. Biol. 16, 1–18. doi: 10.1159/000337464
Nagyné Réz, I., Lányiné Engelmayer, A., and Kuncz, E. (2007). WISC-IV: Wechsler Gyermek Intelligenciateszt-Negyedik kiadás. 4th Edn. Budapest (Hungary): OS Hungary Tesztfejlesztő Kft.
Naidoo, R., Shuttleworth-Edwards, A. B., Botha, R., and Pienaar, I. (2019). The tower of London-DX 2nd edition test: preliminary norms for educationally disadvantaged Xhosa-speaking individuals. J. Psychol. Afr. 29, 60–66. doi: 10.1080/14330237.2019.1568074
Nilsson, S., Merlo, J., Lyberg-Åhlander, V., and Psouni, E. (2015). Psychotropic drug use in adolescents born with an orofacial cleft: a population-based study. BMJ Open 5:e005306. doi: 10.1136/bmjopen-2014-005306
Nopoulos, P., Berg, S., Canady, J., Richman, L., van Demark, D., and Andreasen, N. C. (2000). Abnormal brain morphology in patients with isolated cleft lip, cleft palate, or both: a preliminary analysis. Cleft Palate Craniofac. J. 37, 441–446. doi: 10.1597/1545-1569_2000_037_0441_abmipw_2.0.co_2
Nopoulos, P., Berg, S., Van Demark, D., Richman, L., Canady, J., and Andreasen, N. C. (2002). Cognitive dysfunction in adult males with non-syndromic clefts of the lip and/or palate. Neuropsychologia 40, 2178–2184. doi: 10.1016/S0028-3932(02)00043-X
Nopoulos, P., Boes, A. D., Jabines, A., Conrad, A. L., Canady, J., Richman, L., et al. (2010). Hyperactivity, impulsivity, and inattention in boys with cleft lip and palate: relationship to ventromedial prefrontal cortex morphology. J. Neurodev. Disord. 2, 235–242. doi: 10.1007/s11689-010-9060-5
Nopoulos, P., Choe, I., Berg, S., van Demark, D., Canady, J., and Richman, L. (2005). Ventral frontal cortex morphology in adult males with isolated Orofacial clefts: relationship to abnormalities in social function. Cleft Palate Craniofac. J. 42, 138–144. doi: 10.1597/03-112.1
Otterman, D. L., Koopman-Verhoeff, M. E., White, T. J., Tiemeier, H., Bolhuis, K., and Jansen, P. W. (2019). Executive functioning and neurodevelopmental disorders in early childhood: a prospective population-based study. Child Adolesc. Psychiatry Ment. Health 13:38. doi: 10.1186/s13034-019-0299-7
Parris, B. A. (2014). Task conflict in the Stroop task: when Stroop interference decreases as Stroop facilitation increases in a low task conflict context. Front. Psychol. 5:1182. doi: 10.3389/fpsyg.2014.01182
Pedersen, D. A., Wehby, G. L., Murray, J. C., and Christensen, K. (2016). Psychiatric diagnoses in individuals with non-Syndromic Oral clefts: a Danish population-based cohort study. PLoS One 11:e0156261. doi: 10.1371/journal.pone.0156261
PsyWay (2020). PsyWay Pszichológiai tesztek online kiértékelése. Available at: http://www.pszichotesztek.hu
Richman, L. C., McCoy, T. E., Conrad, A. L., and Nopoulos, P. C. (2012). Neuropsychological, behavioral, and academic sequelae of cleft: early developmental, school age, and adolescent/young adult outcomes. Cleft Palate Craniofac. J. 49, 387–396. doi: 10.1597/10-237
Richman, L. C., and Ryan, S. M. (2003). Do the reading disabilities of children with cleft fit into current models of developmental dyslexia? Cleft Palate Craniofac. J. 40, 154–157. doi: 10.1597/1545-1569_2003_040_0154_dtrdoc_2.0.co_2
Rincic, M., Rados, M., Krsnik, Z., Gotovac, K., Borovecki, F., Liehr, T., et al. (2016). Complex intrachromosomal rearrangement in 1q leading to 1q32.2 microdeletion: a potential role of SRGAP2 in the gyrification of cerebral cortex. Mol. Cytogenet. 9:19. doi: 10.1186/s13039-016-0221-4
Roebuck, H., Freigang, C., and Barry, J. G. (2016). Continuous performance tasks: not just about sustaining attention. J. Speech Lang. Hear. Res. 59, 501–510. doi: 10.1044/2015_JSLHR-L-15-0068
Rózsa, S., Kő, N., and Gádoros, J. (1999). A gyermekpszichiátriai zavarok kérdőíves mérése: Agyermekviselkedési kérdőív diagnosztikai megbízhatósága és a több információ forrásonalapuló jellemzések egyezése. Psychiatr. Hung. 4, 375–392.
Saleem, K., Zaib, T., Sun, W., and Fu, S. (2019). Assessment of candidate genes and genetic heterogeneity in human non syndromic orofacial clefts specifically non syndromic cleft lip with or without palate. Heliyon 5:e03019. doi: 10.1016/j.heliyon.2019.e03019
Sándor-Bajusz, K. A., Sadi, A., Varga, E., Csábi, G., Antonoglou, G. N., and Lohner, S. (2022). The brain in Oral Clefting: a systematic review with meta-analyses. Front. Neuroanat. 16:863900. doi: 10.3389/FNANA.2022.863900
Scarpina, F., and Tagini, S. (2017). The stroop color and word test. Front. Psychol. 8:00557. doi: 10.3389/fpsyg.2017.00557
Shaheen, S. (2014). How Child’s play impacts executive function–related behaviors. Appl. Neuropsychol. Child 3, 182–187. doi: 10.1080/21622965.2013.839612
Speltz, M. L. (2000). Brief report: cognitive and psychomotor development of infants with orofacial clefts. J. Pediatr. Psychol. 25, 185–190. doi: 10.1093/jpepsy/25.3.185
Tillman, K. K., Hakelius, M., Höijer, J., Ramklint, M., Ekselius, L., Nowinski, D., et al. (2018). Increased risk for neurodevelopmental disorders in children with orofacial clefts. J. Am. Acad. Child Adolesc. Psychiatry 57, 876–883. doi: 10.1016/j.jaac.2018.06.024
Unterrainer, J. M., Rahm, B., Kaller, C. P., Leonhart, R., Quiske, K., Hoppe-Seyler, K., et al. (2004). Planning abilities and the tower of London: is this task measuring a discrete cognitive function? J. Clin. Exp. Neuropsychol. 26, 846–856. doi: 10.1080/13803390490509574
Weinberg, S. M., Andreasen, N. C., and Nopoulos, P. (2009). Three-dimensional morphometric analysis of brain shape in nonsyndromic orofacial clefting. J. Anat. 214, 926–936. doi: 10.1111/j.1469-7580.2009.01084.x
Yang, F. F., McPherson, B., Shu, H., Xie, N., and Xiang, K. (2012). Structural abnormalities of the central auditory pathway in infants with nonsyndromic cleft lip and/or palate. Cleft Palate Craniofac. J. 49, 137–145. doi: 10.1597/11-014
Keywords: cleft lip, cleft palate, neurodevelopment, executive function, developmental outcomes
Citation: Sándor-Bajusz KA, Dergez T, Molnár E, Hadzsiev K, Till Á, Zsigmond A, Vástyán A and Csábi G (2023) Cognitive functioning and clinical characteristics of children with non-syndromic orofacial clefts: A case-control study. Front. Psychol. 14:1115304. doi: 10.3389/fpsyg.2023.1115304
Edited by:
Fabrizio Stasolla, Giustino Fortunato University, ItalyReviewed by:
Jonathan Fries, University of Vienna, AustriaVirpi Harila, University of Oulu, Finland
Copyright © 2023 Sándor-Bajusz, Dergez, Molnár, Hadzsiev, Till, Zsigmond, Vástyán and Csábi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kinga Amália Sándor-Bajusz, sandor.kinga@pte.hu