 Susanna Asseyer1,2,3,4*
Susanna Asseyer1,2,3,4* Nasrin Asgari5,6
Nasrin Asgari5,6 Jeffrey Bennett7
Jeffrey Bennett7 Omer Bialer8,9
Omer Bialer8,9 Yolanda Blanco10
Yolanda Blanco10 Francesca Bosello11
Francesca Bosello11 Anna Camos-Carreras12
Anna Camos-Carreras12 Edgar Carnero Contentti13Sara Carta11
Edgar Carnero Contentti13Sara Carta11 John Chen14
John Chen14 Claudia Chien1,2,3,4Mashina Chomba15Russell C. Dale16,17,18Josep Dalmau19,20Kristina Feldmann1,2,3
Claudia Chien1,2,3,4Mashina Chomba15Russell C. Dale16,17,18Josep Dalmau19,20Kristina Feldmann1,2,3 Eoin P. Flanagan21Caroline Froment Tilikete22Carolina Garcia-Alfonso23
Eoin P. Flanagan21Caroline Froment Tilikete22Carolina Garcia-Alfonso23 Joachim Havla24Mark Hellmann8,9
Joachim Havla24Mark Hellmann8,9 Ho Jin Kim25Philipp Klyscz1,2,3,4
Ho Jin Kim25Philipp Klyscz1,2,3,4 Frank Konietschke2Chiara La Morgia26,27
Frank Konietschke2Chiara La Morgia26,27 Marco Lana-Peixoto28
Marco Lana-Peixoto28 Maria Isabel Leite29
Maria Isabel Leite29 Netta Levin30
Netta Levin30 Michael Levy31
Michael Levy31 Sara Llufriu32,33
Sara Llufriu32,33 Pablo Lopez13
Pablo Lopez13 Itay Lotan8,9,31
Itay Lotan8,9,31 Alessandra Lugaresi34,35
Alessandra Lugaresi34,35 Romain Marignier22
Romain Marignier22 Sara Mariotto11
Sara Mariotto11 Susan P. Mollan36,37Cassandra Ocampo38Frederike Cosima Oertel1,2,3,4Maja Olszewska4Jacqueline Palace29
Susan P. Mollan36,37Cassandra Ocampo38Frederike Cosima Oertel1,2,3,4Maja Olszewska4Jacqueline Palace29 Lekha Pandit39José Luis Peralta Uribe23
Lekha Pandit39José Luis Peralta Uribe23 Sean Pittock31
Sean Pittock31 Sudarshini Ramanathan17,40,41
Sudarshini Ramanathan17,40,41 Natthapon Rattanathamsakul42
Natthapon Rattanathamsakul42 Albert Saiz32,33
Albert Saiz32,33 Sara Samadzadeh1,2,3,4,5,6
Sara Samadzadeh1,2,3,4,5,6 Bernardo Sanchez-Dalmau12
Bernardo Sanchez-Dalmau12 Deanna Saylor15,43
Deanna Saylor15,43 Michael Scheel1,2,3,4,44
Michael Scheel1,2,3,4,44 Tanja Schmitz-Hübsch1,2,3,4Jemal Shifa45
Tanja Schmitz-Hübsch1,2,3,4Jemal Shifa45 Sasitorn Siritho42,46
Sasitorn Siritho42,46 Pia S. Sperber1,2,3,4,47
Pia S. Sperber1,2,3,4,47 Prem S. Subramanian7
Prem S. Subramanian7 Alon Tiosano8,9
Alon Tiosano8,9 Adi Vaknin-Dembinsky30
Adi Vaknin-Dembinsky30 Alvaro Jose Mejia Vergara48
Alvaro Jose Mejia Vergara48 Adi Wilf-Yarkoni49Luis Alfonso Zarco23
Adi Wilf-Yarkoni49Luis Alfonso Zarco23 Hanna G. Zimmermann1,2,3,50
Hanna G. Zimmermann1,2,3,50 Friedemann Paul1,2,3,4†
Friedemann Paul1,2,3,4† Hadas Stiebel-Kalish8,9†
Hadas Stiebel-Kalish8,9†- 1Experimental and Clinical Research Center, A Cooperation Between the Max Delbrück Center for Molecular Medicine in the Helmholtz Association and Charité Universitätsmedizin Berlin, Berlin, Germany
- 2Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Experimental and Clinical Research Center, Berlin, Germany
- 3Max Delbrück Center for Molecular Medicine in the Helmholtz Association (MDC), Berlin, Germany
- 4NeuroCure Clinical Research Center, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 5Department of Neurology, Slagelse Hospital, Slagelse, Denmark
- 6Institutes of Regional Health Research and Molecular Medicine, University of Southern Denmark, Odense, Denmark
- 7Programs in Neuroscience and Immunology, Departments of Neurology and Ophthalmology, Sue Anschutz-Rodgers Eye Center, University of Colorado Anschutz Medical Campus, Aurora, CO, United States
- 8Department of Neuro-Ophthalmology, Rabin Medical Center, Petah Tikva, Israel
- 9Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
- 10Neuroimmunology and Multiple Sclerosis Unit, Neurology Service, Hospital Clinic de Barcelona, and Institut d'Investigacions August Pi i Sunyer (IDIVAPS), University of Barcelona, Barcelona, Spain
- 11Neurology Unit, Department of Neurosciences, Biomedicine, and Movement Sciences, University of Verona, Verona, Italy
- 12Ophthalmology Department, Hospital Clínic de Barcelona, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), University of Barcelona, Barcelona, Spain
- 13Neuroimmunology Unit, Department of Neuroscience, Hospital Aleman, Buenos Aires, Argentina
- 14Department of Ophthalmology and Neurology, Mayo Clinic, Rochester, MN, United States
- 15Department of Internal Medicine, University Teaching Hospital, Lusaka, Zambia
- 16Clinical Neuroimmunology Group, Kids Neuroscience Centre, Sydney, NSW, Australia
- 17Faculty of Medicine and Health and Brain and Mind Centre, University of Sydney, Sydney, NSW, Australia
- 18TY Nelson Department of Paediatric Neurology, Children's Hospital Westmead, Sydney, NSW, Australia
- 19ICREA-IDIBAPS, Service of Neurology, Hospital Clínic, University of Barcelona, Barcelona, Spain
- 20Department of Neurology, University of Pennsylvania, Philadelphia, PA, United States
- 21Laboratory Medicine and Pathology, Departments of Neurology, Center for MS and Autoimmune Neurology, Mayo Clinic, Rochester, MN, United States
- 22Neuro-Ophthalmology Unit, Pierre Wertheimer Neurological Hospital, Hospices Civils de Lyon, Lyon 1 University, Lyon Neuroscience Research Center, INSERM U1028, CNRS UMR5292, IMPACT Team, Lyon, France
- 23Pontificia Universidad Javeriana and Hospital Unviersitario San Ignacio, Bogotá, Colombia
- 24Institute of Clinical Neuroimmunology, LMU Hospital, Ludwig-Maximilians-Universität München, Munich, Germany
- 25Department of Neurology, National Cancer Center, Goyang, Republic of Korea
- 26Neurology Unit, IRCCS Institute of Neurological Sciences, Bologna, Italy
- 27Department of Biomedical and Neuromotor Sciences, University of Bologna, Bologna, Italy
- 28CIEM MS Center, Federal University of Minas Gerais Medical School, Belo Horizonte, Brazil
- 29Department of Neurology, Oxford University Hospitals, National Health Service Trust, Oxford, United Kingdom
- 30Department of Neurology, Hadassah Medical Center, Hebrew University, Jerusalem, Israel
- 31Neuromyelitis Optica Research Laboratory, Massachusetts General Hospital and Harvard Medical School, Boston, MA, United States
- 32Neuroimmunology and Multiple Sclerosis Unit, Neurology Service, Hospital Clinic de Barcelona, Barcelona, Spain
- 33Institut d'Investigacions August Pi i Sunyer (IDIVAPS), University of Barcelona, Barcelona, Spain
- 34IRCCS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italy
- 35Dipartimento di Scienze Biomediche e Neuromotorie, Università di Bologna, Bologna, Italy
- 36Birmingham Neuro-Ophthalmology, Queen Elizabeth Hospital, University Hospitals Birmingham NHS Foundation Trust, Birmingham, United Kingdom
- 37Translational Brian Science, Institute of Metabolism and Systems Research, University of Birmingham, Edgbaston, United Kingdom
- 38Faculty of Medicine, University of Botswana, Gaborone, Botswana
- 39Center for Advanced Neurological Research, KS Hegde Medical Academy, Nitte (Deemed to be University), Mangalore, India
- 40Translational Neuroimmunology Group, Kids Neuroscience Centre, Children's Hospital Westmead, Sydney, NSW, Australia
- 41Department of Neurology, Concord Hospital, Sydney, NSW, Australia
- 42Siriraj Neuroimmunology Center, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
- 43Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States
- 44Department of Neuroradiology, Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 45Department of Surgery, University of Botswana, Gaborone, Botswana
- 46Neuroscience Center, Bumrungrad International Hospital, Bangkok, Thailand
- 47German Center for Cardiovascular Research (DZHK), Berlin, Germany
- 48Department of Ophthalmology, Fundación Universitaria Sanitas Facultad de Medicina, Bogotá, Colombia
- 49Department of Neurology, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel
- 50Einstein Center Digital Future, Berlin, Germany
Optic neuritis (ON) often occurs at the presentation of multiple sclerosis (MS), neuromyelitis optica spectrum disorders (NMOSD), and myelin oligodendrocyte glycoprotein (MOG) antibody-associated disease (MOGAD). The recommended treatment of high-dose corticosteroids for ON is based on a North American study population, which did not address treatment timing or antibody serostatus. The Acute Optic Neuritis Network (ACON) presents a global, prospective, observational study protocol primarily designed to investigate the effect of time to high-dose corticosteroid treatment on 6-month visual outcomes in ON. Patients presenting within 30 days of the inaugural ON will be enrolled. For the primary analysis, patients will subsequently be assigned into the MS-ON group, the aquapotin-4-IgG positive ON (AQP4-IgG+ON) group or the MOG-IgG positive ON (MOG-IgG+ON) group and then further sub-stratified according to the number of days from the onset of visual loss to high-dose corticosteroids (days-to-Rx). The primary outcome measure will be high-contrast best-corrected visual acuity (HC-BCVA) at 6 months. In addition, multimodal data will be collected in subjects with any ON (CIS-ON, MS-ON, AQP4-IgG+ON or MOG-IgG+ON, and seronegative non-MS-ON), excluding infectious and granulomatous ON. Secondary outcomes include low-contrast best-corrected visual acuity (LC-BCVA), optical coherence tomography (OCT), magnetic resonance imaging (MRI) measurements, serum and cerebrospinal fluid (CSF) biomarkers (AQP4-IgG and MOG-IgG levels, neurofilament, and glial fibrillary protein), and patient reported outcome measures (headache, visual function in daily routine, depression, and quality of life questionnaires) at presentation at 6-month and 12-month follow-up visits. Data will be collected from 28 academic hospitals from Africa, Asia, the Middle East, Europe, North America, South America, and Australia. Planned recruitment consists of 100 MS-ON, 50 AQP4-IgG+ON, and 50 MOG-IgG+ON. This prospective, multimodal data collection will assess the potential value of early high-dose corticosteroid treatment, investigate the interrelations between functional impairments and structural changes, and evaluate the diagnostic yield of laboratory biomarkers. This analysis has the ability to substantially improve treatment strategies and the accuracy of diagnostic stratification in acute demyelinating ON.
Trial registration: ClinicalTrials.gov, identifier: NCT05605951.
Introduction
Optic neuritis (ON) is the most common optic neuropathy in young adults with an annual incidence rate of three to five per 100,000 person-years (1–4). ON involves primary inflammation, demyelination, and axonal injury in the optic nerves and the chiasm (1, 5). This can lead to retinal ganglion cell destruction and significant visual loss (4, 6). ON can be the initial event in multiple sclerosis (MS), including clinically isolated syndrome (CIS) (3), in aquaporin-4-IgG positive (AQP4-IgG+) and seronegative neuromyelitis optica spectrum disorders (NMOSD) (7), and in myelin oligodendrocyte glycoprotein-IgG (MOG-IgG+)-associated disease (MOGAD) (8). The incidence of ON is stable and similar around the world (4, 9), but the proportion of ON patients with AQP4-IgG+ON and MOG-IgG+ON vs. MS-ON differs greatly in different races (4). Visual outcomes vary between the three diseases (10): in MS-ON and MOG-IgG+ON, visual prognosis is good (10–13), but AQP4-IgG+ON is associated with significant visual loss (11, 14–16). As the three disease entities require different acute and long-term treatment strategies, earlier diagnostic stratification has the potential to assist tailored treatment decisions and thereby improve visual outcomes (17).
The Acute Optic Neuritis Network (ACON) is a global cooperation of 28 academic centers longitudinally investigating subjects with inaugural acute ON (Figure 1). Here, we present the protocol for the ACON study, which primarily aims to evaluate the effect of time to corticosteroid treatment (measured as the number of days from onset of visual loss to treatment with high-dose corticosteroids; days-to-Rx) on visual and structural outcomes in MS-ON, AQP4-IgG+ON, and MOG-IgG+ON respecting the novel diagnostic criteria for ON (18).

Figure 1. Participating ACON centers. Twenty-eight ACON centers (status 10/2022) Africa (Botswana, Zambia), Asia (India, Korea, Thailand, Vietnam), the Middle East (Israel), North America (USA), South America (Argentina, Brazil, Colombia), Australia, and Europe (Denmark, France, Germany, Italy, Spain, United Kingdom).
The effect of hyperacute high-dose corticosteroid treatment on functional outcome in inaugural MS-ON, AQP4-IgG+ON, and MOG-IgG+ON
Current treatment protocols for ON are based on the landmark 1992 Optic Neuritis Treatment Trial (ONTT), which involved 457 patients with new onset ON. The trial included three arms: placebo, 250 mg of IVMP every 6 hours for three days followed by oral prednisone at 1 mg/kg for 11 days, and oral prednisone at 1 mg/kg for 14 days (19). As treatment with IVMP was associated with a more rapid recovery of visual function and showed the most benefit within the first 15 days of follow-up, many centers used this protocol to treat people who present with ON. Importantly, the inclusion criteria stipulated that people with visual loss in the preceding 8 days could be enrolled in the ONTT (19), and the subsequent results of the ONTT showed that there was a delay in initiation of the treatment (mean 5 days ± 1.6 days) (19, 20). The ONTT was not designed to investigate the impact of time from visual loss or indeed the preceding pain to high-dose corticosteroid therapy. The ONTT was conducted prior to the advent of the serological tests for AQP4-IgG and MOG-IgG. On subsequent testing of all the ONTT participants, it did not contain any patients with AQP4-IgG+ON and only a few patients with MOG-IgG+ON (21). The recommendations formed by this landmark article are limited by the inclusion criteria and are likely of limited applicability in countries and across races where the proportion of AQP4-IgG+ON and MOG-IgG+ON is higher, as compared with North America. Preliminary evidence from several retrospective studies suggests a benefit to visual outcomes of initiating early high-dose corticosteroids to treat AQP4-IgG+ON and MOG-IgG+ON (20, 22–25). We propose verifying the functional benefit of early high-dose corticosteroids in a global, multi-racial prospective study including patients with inaugural MS-ON, AQP4-IgG+ON, and MOG-IgG+ON.
Developing data for ON escalation treatment protocols
There is currently no consensus on escalation treatment protocols for protocols for plasma exchange (PLEX) or intravenous immunoglobulines (IVIG) in the treatment of antibody-mediated ON and a lack of specific recommendations with respect to treatment duration. With no prior studies analyzing the varying patterns of ON severity, the speed of disease progression, the degree of response to high-dose corticosteroids, and the difficulty in comparing patients presenting late vs. early after the onset of visual loss, all of which make treatment escalation guidelines difficult to develop. The development of this study and the detailed database, which accurately captures ON severity and course, builds the basis for the development of treatment escalation guidelines.
Structural biomarkers as an aid to tailor ON treatment
To explore possible means to aid hyperacute treatment decisions, the ACON study will collect data on and evaluate the potential of structural biomarkers as methods to enhance timely diagnoses. These structural biomarkers will be explored using magnetic resonance imaging (MRI) and optical coherence tomography (OCT).
MRI of the brain and the orbits is one of the most established clinical tools for investigating acute ON. The radiological features of ON differ between the three disease etiologies: optic nerve lesions in AQP4-IgG+ON and MOG-IgG+ON are more frequently bilateral and more extensive than in MS-ON (26–28). AQP4-IgG+ON typically affects posterior parts of the optic nerve and the chiasm, while MOG-IgG+ON typically affects long segments of the anterior optic nerve (10, 28). During the acute phase of ON, optic nerve lesion length has been shown to be a useful imaging biomarker, predictive of retinal neuro-axonal loss and chronic visual impairment (29). We will explore the diagnostic and clinical relevance of visual pathway lesions and their persistence following the inaugural ON.
OCT with the peripapillary retinal nerve fiber thickness (pRNFL), the macular ganglion cell layer (GCL), or the ganglion cell complex (GCC) measurements aid differentiation between acute MS-ON and MOG-IgG+ON (30). However, age and race have been reported to impact pRNFL (31). We will re-explore whether pRNFL robustly differentiates MS-ON from MOG-IgG+ON in a multi-racial population of subjects with inaugural ON. Assessment of OCT imaging parameters such as the ganglion cell analysis may allow disease stratification and detection of subclinical activity prior to the initial ON and may provide insightful longitudinal data such as rate of progression, which has the potential to correlate with disease severity (32, 33).
Biological biomarkers
Neurofilament light chain (NfL) is a major structural component of neurons and can be detected in the serum and cerebrospinal fluid (CSF). Elevated NfL levels are an indicator of neuronal damage (34) in acute ON (35), coinciding with visual dysfunction (36) and structural retinal damage (37). However, the role of serum NfL levels and dynamics in the acute stage of ON as potential indicators for subsequent conversion to MS, NMOSD, or MOGAD remains unexplored.
Glial fibrillary acidic protein (GFAP) is the predominant intermediate filament in mature astrocytes (38, 39) and was identified in astrogliosis MS lesions (40). It is differentially elevated in the CSF and the blood in the three inflammatory diseases of interest in this study (41–43). ACON aims to collect data on NfL and GFAP in the serum and CSF of patients following acute ON and to investigate their patterns in MS-ON, AQP4-IgG+ON, MOG-IgG+ON and also in double-seronegative non-MS-ON.
The detection of serum MOG-IgG is a crucial step for correctly diagnosing MOGAD (44). Live cell-based assays (CBA) using full-length human MOG are optimal and have consistently shown a 99% specificity for typical MOGAD phenotypes (44, 45). Many centers worldwide use a commercially available cell-based assay using fixed transfected cells (Euroimmun AG, Lübeck Germany), which has excellent (98%) specificity (46). Titers of MOG-IgG can decrease to undetectable levels following an acute attack, after treatment or disease remission. Thus, potential factors affecting the duration of seropositivity will be explored using longitudinal serum samples from patients exhibiting MOG-IgG seropositivity following acute ON. The diagnostic value of CSF antibody testing remains unclear. Since AQP4-IgG and MOG-IgG are both produced extrathecally, testing CSF is currently not routinely recommended (47). However, a few cases of seronegative NMOSD have been described, where MOG-IgG was present in CSF only (48). ACON aims to clarify the role of MOG-IgG in CSF in double-seronegative non-MS-ON.
Clinical phenotypes
Pain patterns differ between MS-ON, AQP4-IgG+ON, and MOG-IgG+ON. Typically, both MS-ON and AQP4-IgG+ON are preceded by relatively mild retrobulbar pain, which worsens with eye movement (1, 49–51). By contrast, pain in MOG-IgG+ON is typically intense (52, 53). No comparative studies to date have investigated pain scoring to distinguish MS-ON and AQP4-IgG+ON from MOG-IgG+ON.
Measurements of visual function in daily routine and quality of life (QoL) are understudied in neuroscience, though of great value to patients. Issues impacting QoL after an ON event include perceived visual dysfunction, the degree of anxiety regarding future loss of vision and further relapses, pain patterns, depression, and adjustment difficulties. Visual function in daily routine correlates with functional (e.g., visual acuity) and structural measurements (e.g., pRNFL) of visual outcome in NMOSD (16). The long-term visual function in daily routine and Qol following ON is an understudied aspect, which may be explored through a high-quality detailed database of questionnaires filled in by patients in a prospective fashion.
In summary, ACON will build a broad dataset to serve as a platform to revise and tailor acute ON treatment recommendations, improve the differential diagnoses between neuroimmunological disease entities, and identify determinants of disease progression and QoL in subjects after inaugural MS-ON, AQP4-IgG+ON, and MOG-IgG+ON.
Methods and analysis
Study objectives
The primary objective of ACON is to investigate whether MS-ON, AQP4-IgG+ON, and MOG-IgG+ON patients treated with early high-dose corticosteroids for visual loss have better visual outcomes than those with late treatment. Treatment with both IVMP and oral high-dose corticosteroids is currently used as the standard of care in ON and will be included. According to previous data (24), subjects will be stratified into three groups: those presenting within 3 days of the onset of visual loss, those presenting between 4 and 7 days from the onset of visual loss, and those presenting between 8 and 30 days from onset of visual loss (days-to-Rx). The stratification will be performed within each respective disease group (MS, AQP4-IgG+NMOSD, and MOGAD).
Secondary objectives will consist of the interaction between clinical and para-clinical parameters, as well as their association with patient-reported QoL aspects (see Table 1; Figure 2).
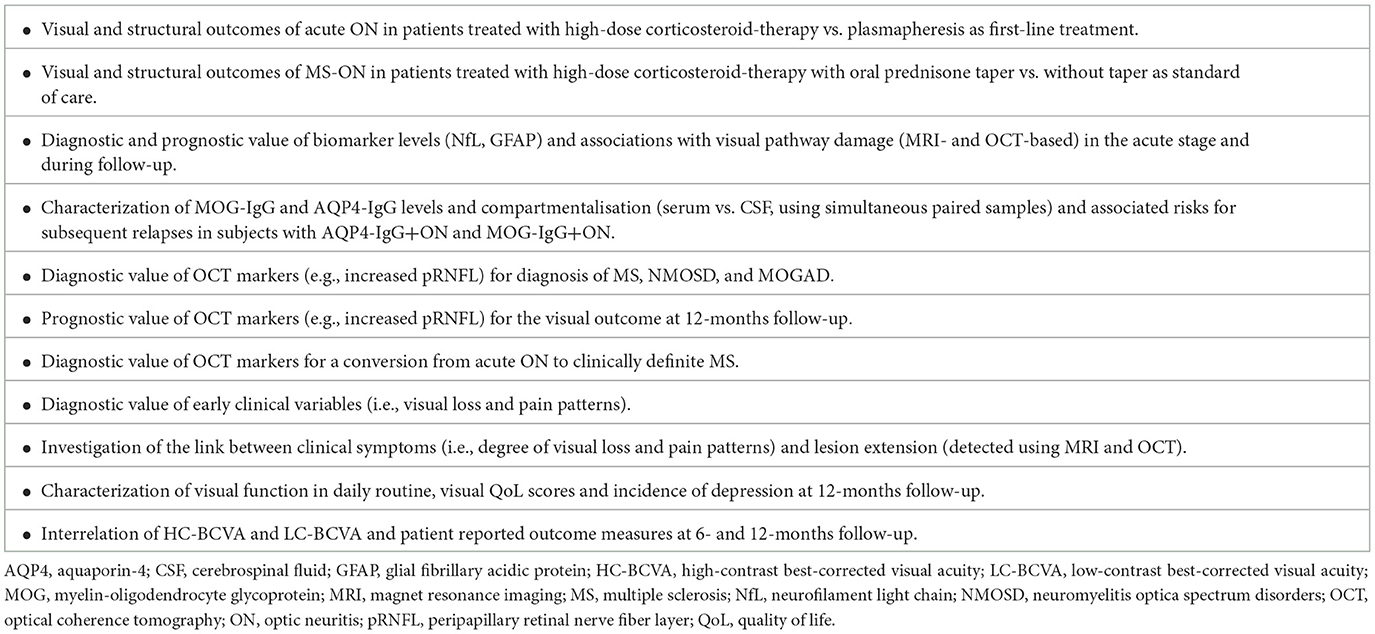
Table 1. Secondary objectives.
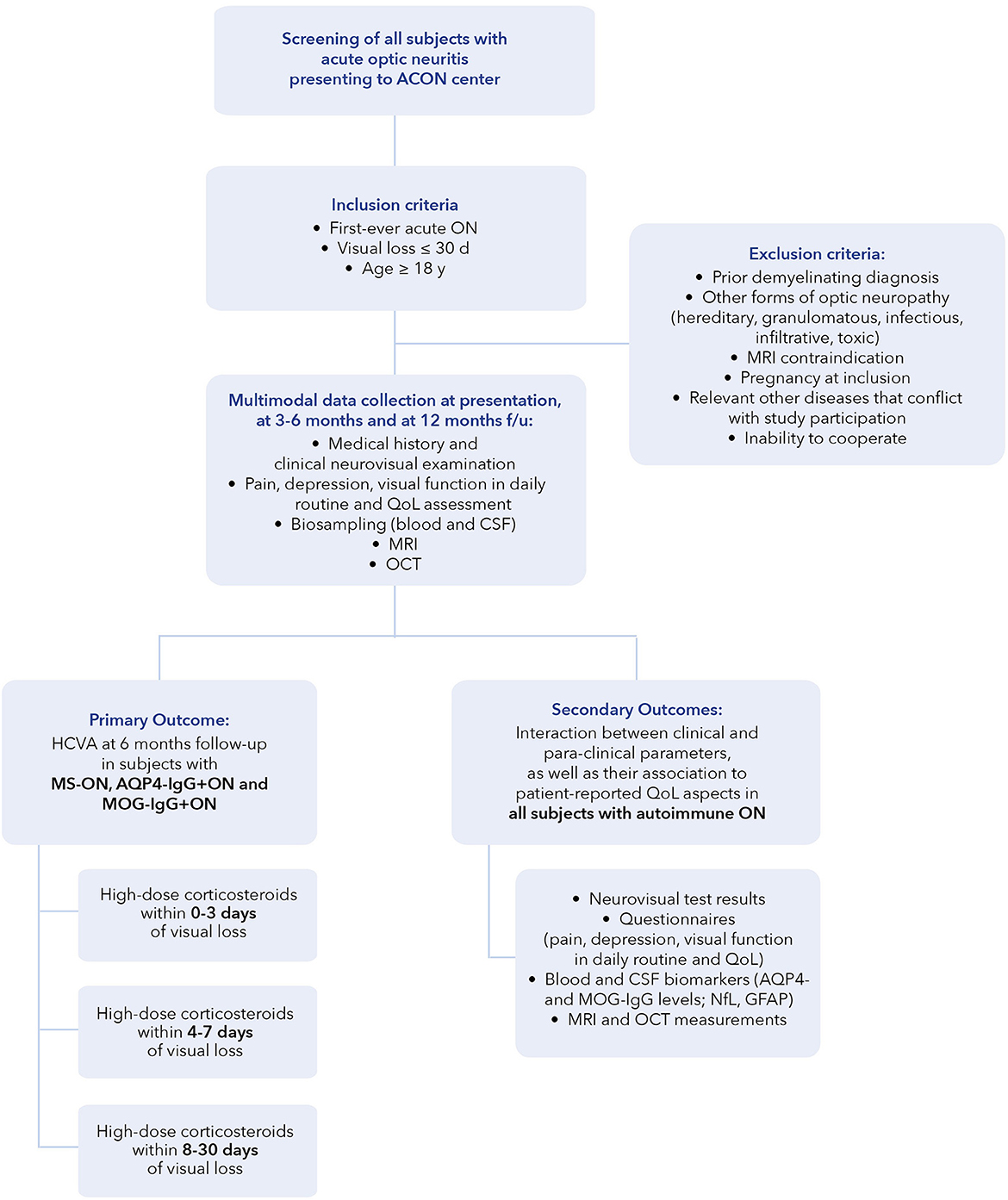
Figure 2. Flowchart of ACON study design. ACON, Acute Optic Neuritis Network; AQP4, aquaporin-4; CSF, cerebrospinal fluid; days; f/u, follow-up; GFAP, glial fibrillary acidic protein; MRI, magnet resonance imaging; MOG, myelin-oligodendrocyte glycoprotein; NEI-VFQ-25, National Eye Institute Visual Function Questionnaire; NfL, neurofilament light chain; OCT, optical coherence tomography; ON, optic neuritis; QoL, quality of life; y, years.
Study design
ACON is an international, multicenter non-interventional study network aiming to optimize treatment decisions in subjects with acute ON and to improve understanding of the underlying pathologies. It currently includes 28 teaching hospitals from Africa (Botswana, Zambia), Asia (India, Korea, Thailand, and Vietnam), the Middle East (Israel), North America (USA), South America (Argentina, Brazil, and Colombia), Australia, and Europe (Denmark, France, Germany, Italy, Spain, and United Kingdom) (for details see Supplementary material).
ACON centers will recruit and prospectively collect data from all subjects with inaugural acute ON (see study population).
Local staff will have confirmed up-to-date training in the conduct of studies according to the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) and good clinical practice (GCP) standards.
All study participants will be evaluated during hospitalization or through outpatient clinics at the time of presenting with inaugural acute ON as well as during follow-ups (at 6- and 12-month after onset). Visits at additional time points are optional, based on patient-tailored needs and the recruiting centers' standard of care. The recruitment period is planned for 36 months. Acute ON treatment is provided as part of routine care according to the clinical best practice at the respective study center. This study will not include the randomization of patients to receive early or late high-dose corticosteroids. Disease diagnosis will be assessed at 6- and 12-month follow-up visits, respecting the diagnostic criteria for MS according to the 2017 revised McDonald criteria (54), diagnosis of AQP4-IgG-positive or seronegative NMOSD according to the 2015 international consensus diagnostic criteria (55), and diagnosis of MOGAD in subjects with clinical characteristics consistent with MOGAD and positive testing of MOG-IgG with respect to the new MOGAD diagnostic criteria (44, 56, 57).
Study population
A total of 300 patients with acute ON will be screened for study eligibility. We will include only patients with inaugural ON. Subjects presenting for the first time with isolated ON or ON with additional demyelinating syndromes, e.g., myelitis or acute disseminated encephalomyelitis (ADEM) occurring within 30 days of the acute ON, will be included. Furthermore, patients with dissemination in time and space on MRI will be included. Patients with prior soft symptoms, which can retrospectively be considered to be a demyelinating manifestation will be included, excluding patients with a prior demyelinating diagnosis or prior symptoms of optic neuritis (see exclusion criteria). The prevalence of MS-ON, AQP4-IgG+ON, and MOG-IgG+ON differs in each of the participating centers. For the primary analysis, we collect data from subjects with MS-ON, AQP4-IgG+ON, and MOG-IgG+ON. For the secondary analysis, multimodal data will be collected in subjects with any demyelinating ON (CIS-ON, MS-ON, AQP4-IgG+ON, or MOG-IgG+ON and seronegative non-MS-ON) with the aim of exploring clinical, structural, and laboratory biomarkers to expedite the diagnosis and tailoring of treatment. This data will include OCT measurements, an MRI of the visual pathway including orbital cuts, questionnaires (headache, visual function in daily routine, depression, and QoL), basal metabolic index (BMI), IVMP, and oral corticosteroid treatment duration, utility of escalation therapy with PLEX or IVIG, and serum and CSF biomarkers (AQP4- and MOG-IgG levels, NFL, and GFAP).
We expect between 30 and 50% of subjects will be ineligible due to the rigorous exclusion criteria.
The inclusion criteria include written informed consent, age ≥18 years, and diagnosis of an inaugural ON with respect to the novel diagnostic criteria for ON (18) within 30 days from the onset of visual loss and in the absence of previously diagnosed demyelinating events.
The exclusion criteria comprise other forms of optic neuropathy (e.g., glaucoma, Leber's hereditary optic neuropathy, other inherited optic neuropathies such as OPA1/OPA3-mutations, granulomatous, infectious, infiltrative, or toxic neuropathies, as well as incidental signs of prior optic neuropathy, prior events of visual loss, and clinical evidence of optic nerve thinning at presentation), other significant comorbidities (i.e., medically uncontrolled severe arterial hypertension, severe diabetes mellitus, chronic infectious diseases, drug abuse, and severe psychiatric or psychological disorders), prior demyelinating diagnosis, pregnancy at inclusion, MRI contraindications, and medical or psychological constraints impacting the ability to give informed consent to study participation and fulfill the study protocol.
The inclusion and exclusion criteria are summarized in Table 2. They are applied at the time of screening by the study physician. Throughout the study duration, we will apply drop-out criteria (see Table 2) as a guideline to evaluate the case for a premature end-of-study.
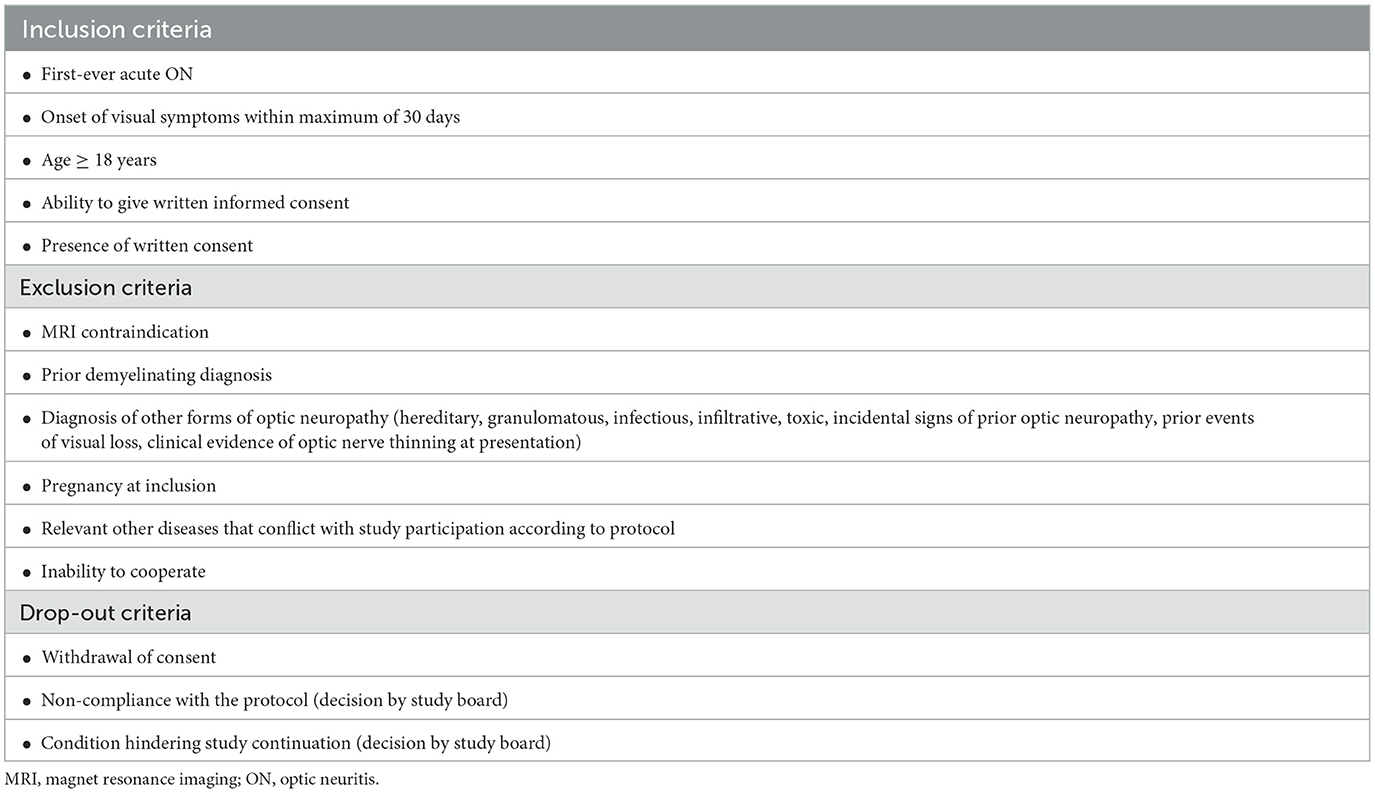
Table 2. Inclusion and exclusion criteria.
Data collection
Screening for study eligibility occurs at the time of presentation at the respective study center. Data collection according to the standard of care at the respective institution is performed in the acute phase of an inaugural acute ON (baseline visit) and at 6- and 12-month follow-up visits.
Medical history and clinical examination
The medical history will be gathered at each visit and consists of demographics (age, sex, race), height and weight, acute attack-related symptoms with a focus on visual symptoms and pain, vaccination history, previous infections, fertility history, comorbidities, and treatment (drugs and supportive therapies).
For acute ON treatment, ACON specifies the following list of treatment options from which each center will select their choice:
(1) IVMP 1 g for 3 days followed by a taper
(2) IVMP 1 g for 5 days followed by a taper
(3) IVMP 1 g for 3 days without taper
(4) IVMP 1 g for 5 days without taper
(5) Oral prednisone 1,250 mg every other day (EOD)
(6) Others, specified.
In patients with severe visual loss (6/60 or worse) or mean visual field defect of −12 MD and worse at presentation, we recommend rechecking high-contrast best-corrected visual acuity (HC-BCVA) and visual fields on day 5 of IVMP. If vision is not improved by 2 or more lines or more than 4 DB on the visual field, we recommend to consider starting escalation treatment.
For escalation therapy, ACON proved the following treatment suggestions for patients whose vision does not improve with IVMP:
(1) PLEX for 5 days and then reassess vision
(2) Immunoadsorption
(3) IVIG at the dose of 2 g/kg over 5 days (0.4 per day).
At follow-up, all recurrent ON events as well as all demyelinating events will be captured. We will also capture and describe treatment complications and any other comorbidities occurring during the study period.
The neurological examination includes an Expanded Disability Status Scale (EDSS) according to neurostatus definitions (58, 59). The visual examination measures refraction by an autorefraction device or through direct skiascopy/retinoscopy, 100% high-contrast visual acuity, and 2.5% low-contrast visual acuity measured with Sloan charts, automated visual fields (24-2 or 30-2), and visual evoked potentials (VEP).
HC-BCVA and visual fields are the two visual parameters used globally to define blindness. In addition, HC-BCVA and visual fields are used to determine which patients have a vision that allows driving. Thus, these are two of the most clinically relevant endpoints for the patients themselves (3). Low-contrast best-corrected visual acuity (LC-BCVA) is used as a more sensitive measure of visual dysfunction (60) and will be measured in the acute setting and during follow-up.
Pain, depression, visual function in daily routine, and QoL assessment
We will assess pain patterns using a semi-standardized interview. Questions focus on ON-related headache characteristics including the onset of pain, pain intensity, pain quality, location, duration, additional symptoms, response to pain treatment, and pain response to steroid treatment. Second, the Brief Pain Inventory (BPI) will be performed to assess (1) pain severity within the previous 24 h and (2) seven domains of pain-related interference with daily life including general activity, mood, walking ability, working ability, relations with other people, sleep, and enjoyment of life (61). The Beck's Depression Inventory version II (BDI-II) will be used to capture signs of depression both in the acute phase and during follow-ups (62). Visual quality function in daily routine is measured with the National Eye Institute Visual Function Questionnaire (NEI-VFQ-25), with its neuro-ophthalmological supplement (63). QoL is measured with the EuroQol 5-dimension (EQ-5D) index in five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression (64).
Biosampling
Blood and CSF will be collected within one week from the presentation. Venous blood samples will be collected, comprising of serum, plasma, as well as optional PAXGen and peripheral blood mononuclear cell (PBMC) vials. Biosample analysis includes a clinical standard laboratory diagnostic panel as well as testing for AQP4- and MOG-antibodies, GFAP, and NfL. Systematic serum antibody measurements including AQP4-IgG and MOG-IgG will be performed with fixed or live cell-based assays (CBA) (65–67). MOG-IgG samples will be tested and reconfirmed employing both the commercially available assay and the human cell-based assay. Cell-based assays for MOG-IgG will either be performed at centers at which this assay is available (Mayo clinic, Barcelona, etc.) or shipped to a participating ACON center to reconfirm fixed cell-based assays.
CSF will be obtained from clinical routine diagnostics (only in the acute phase) and collected for further analysis at the respective center. Routine diagnostics include oligoclonal band detection and cell count. In addition to a clinical standard CSF analysis, MOG-IgG in CSF will be assessed. Preserves of biospecimens will be stored at −80°C for future scientific analyses.
Magnetic resonance imaging
Cerebral MRI with dedicated orbital cuts at the baseline will be performed as part of the clinical routine diagnostic tests. Patients will receive 1.5 or 3-Tesla imaging, including a cerebral 3D T2-weighted and/or Fluid Attenuated Inversion Recovery (FLAIR) sequence, and, if available, a 3D T1-weighted Magnetization Prepared Rapid Gradient Echo (MPRAGE) sequence. In the acute setting and at 6-month follow-up, 3D T1-weighted, fat suppression (FS) sequences and/or MPRAGE will be performed following gadolinium administration. Radiological analysis parameters include brain lesion number and volume, location, and extension (for details see Supplementary material Questionnaires and Data Collection CRFs). The MRI characterization score of the optic nerve developed by Ramanathan et al. (28) takes into account optic nerve lesion extent and character, as well as the presence or absence of abnormalities in other parts of the brain.
Optical coherence tomography
Participants will undergo OCT of the retina and the optic nerve head within 10 days from the presentation. The following Spectral Domain OCT devices will be included: Cirrus HD-OCT, Carl Zeiss Meditec, Jena, Germany; Topcon, Optovue, Canon or Spectralis, Heidelberg Engineering, Heidelberg, Germany.
Scans will be obtained in adherence to the Advised Protocol for OCT Study Terminology and Elements (APOSTEL) 2.0 nine-point recommendations and the OSCAR-IB quality criteria (68, 69). Documented OCT measurements include the average pRNFL thickness, GCL or GCC as collected by the different platforms (e.g., Spectralis measuring GCL, Zeiss measuring GCC). The OCT images will subsequently be analyzed using post-hoc analysis with semi-automatic, device-independent algorithms (70).
We will exclude patients with insufficient documentation or those who have their OCT imaging on time-domain devices. Low-quality spectral-domain OCT data will be excluded from the OCT analysis. We plan to qualitatively explore concomitant OCT findings, including microcystic macular oedema (MMO) or peripapillary hyperreflective ovoid mass-like structures (PHOMS) (71, 72).
Table 3 summarizes the data collection.
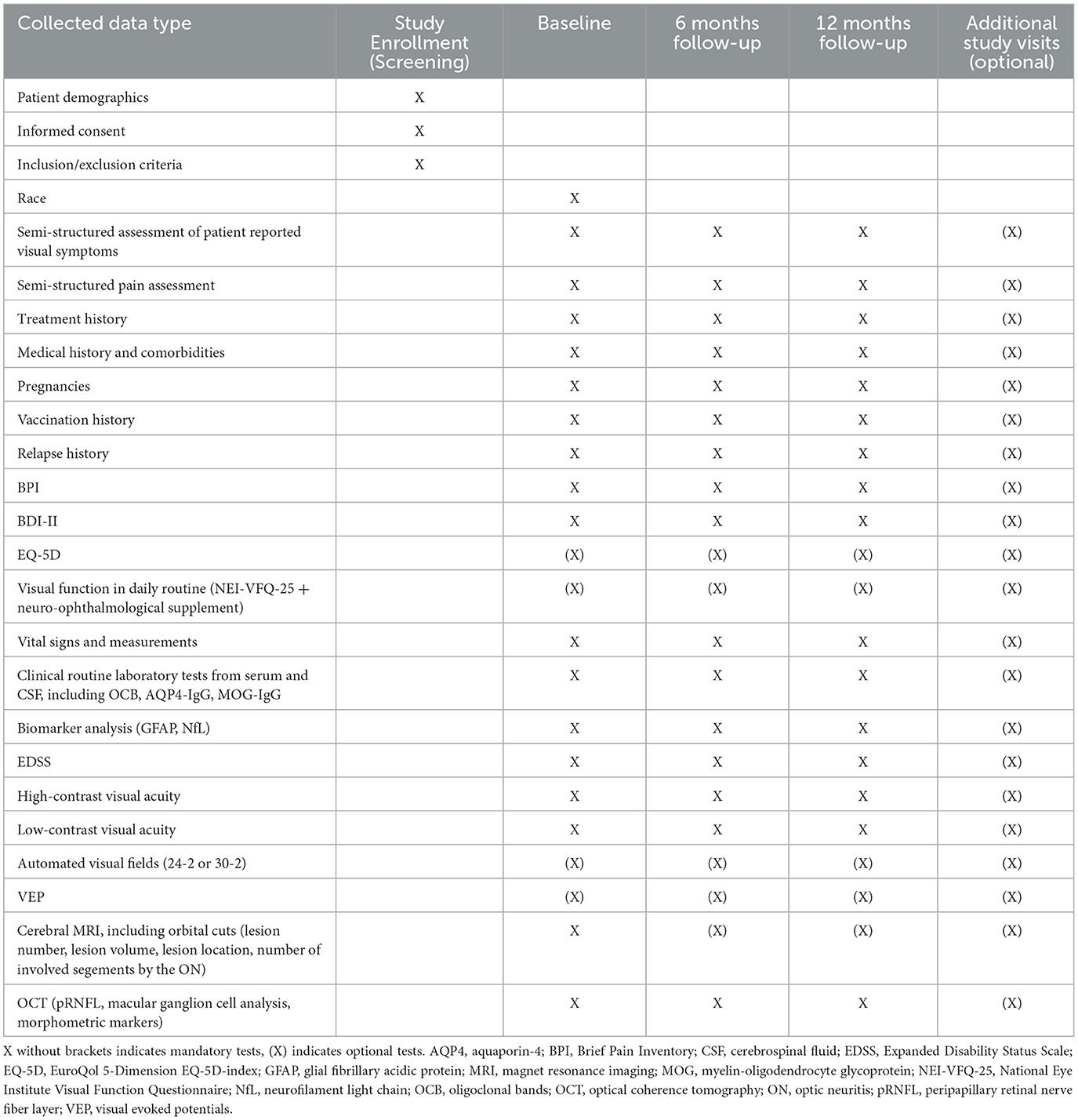
Table 3. Data collection overview.
Data management
All clinical results and MRI imaging data will be pseudonymized and stored in electronic case report form (eCRF) in an electronic database hosted by Research Electronic Data Capture (REDCap), a secure web application developed by Vanderbilt University, for building and managing academic databases (73) on a secure server at Charité—Universitätsmedizin Berlin, Germany. Regular monitoring in the form of independent data quality checks is ensured. OCT image data will be analyzed at Charité—Universitätsmedizin Berlin, Germany.
Sample size considerations
The study is exploratory, and therefore, a formal sample-size computation is not possible. Hence, we justify the sample size by feasibility, which is n = 100 for MS-ON and n = 50 for AQP4-IgG+ON and MOG-IgG+ON. For each disease (MS-ON, AQP4-IgG+ON, and MOG-IgG+ON), patients will be stratified into subgroups according to the number of days since the onset of visual loss: 0–3 days, 4–7 days, and 8–30 days until high-dose corticosteroid treatment. With n = 50, the width of the 95% confidence interval for the treatment effects (=difference between visual acuities between these strata) is ~0.55 standard deviations of the mean difference depending on the actual number of patients within each subgroup.
Statistical analysis
For data analysis, subjects will be assigned into groups according to their diagnosis at the 6-month follow-up. For the primary objective, data from subjects with a diagnosis of MS, AQP4-IgG+ NMOSD, and MOGAD will be analyzed. Data from subjects with other diagnoses (other autoimmune, e.g., CIS-ON, seronegative non-MS-ON) will be described and characterized separately but not included in the primary analysis.
Primary objective
We will estimate the treatment effect from a mixed model with visual acuity as an outcome variable, and the following fixed and random factors will be adjusted to the baseline:
• Diagnosis (fixed; 3 levels)
• Days from visual loss (fixed; 3 levels: 0–3 days, 4–7 days, and 8–30 days until high-dose corticosteroid treatment)
• Dosage (fixed)
• Interaction between diagnosis and days since the visual loss (fixed)
• Eye (random; cluster effect to account for dependencies)
• Initiation of disease-modifying treatment (fixed; 2 levels)
• Center (random).
In case of interactions, diagnose-specific effects will be estimated from mixed models along with 95% confidence intervals.
Secondary objectives
We will characterize all secondary endpoints descriptively. All secondary methods will be analyzed with standard methods (e.g., t-test, Wilcoxon Mann–Whitney test, chi-square test, etc.), depending on their scales (metric vs. non-metric data). All secondary objectives are considered exploratory with limited inferential value. We will apply prediction modeling with measures of performance (accuracy/calibration) to study the diagnostic or prognostic value of novel markers for etiology determination and outcomes.
Potential bias and methods to reduce bias
Since this study is observational and thus randomization and masking to treatment assignment are not possible, it has potential sources of the known bias. First, the study has a selection bias, as some people do not present in the clinic for an inaugural ON at all or are more likely to present with a more severe ON. To mitigate this, a patient's medical history is assessed in a semi-standardized way to detect potential previous attacks, leading to study exclusion. In addition, an ophthalmological examination is conducted to assess for evidence of prior ON damage. Furthermore, prior polling of participating centers carried out in 2021/2022 regarding the number of patients with acute ON seen in each clinic demonstrates the feasibility of including a representative population of subjects with inaugural ON of all severities.
Second, the study has a confounder bias, as subjects will receive treatment according to their time of presentation at the hospital as the standard of care. Furthermore, disease-modifying treatments and other medication initiated between the baseline and follow-up will be analyzed as potential confounders. While high-dose corticosteroid treatment cannot be delayed for ethical reasons, a thorough record will keep the process transparent, and confounders will be minimized by advanced biostatistical techniques, such as confounder adjustment.
Information bias may be introduced when recording the primary visual outcomes, stemming from differences in visual acuity recording techniques, room lighting, and different physicians measuring visual acuity. Therefore, a training course for all participating centers will be held, which aims to standardize assessments across centers. To overcome analytic differences within different OCT machines, we have developed a pipeline for device-independent intraretinal layer OCT segmentation (74), allowing for standardized analysis regarding the region of interest and layer boundaries. Additional potential biases include OCT-captured artifacts for which ACON agreed to adhere to the APOSTEL guidelines for performing and reporting OCT measurements (75). Similarly, different MRI techniques pose another source of information bias. To counteract this, ACON will offer short MRI evaluation training to the participating centers, focusing on the interpretation of optic nerve abnormalities.
To overcome biases through assay differences, blood and CSF samples will be stored to perform centralized testing during follow-up.
Discussion
ACON is the first global prospective longitudinal study on acute ON that includes participating centers from Africa, America, Asia, Australia, and Europe. It intends to build up a comprehensive, systematic, multimodal database of ON patients both in the acute phase and during longitudinal follow-up. Since the publication of the ONTT results in 1992 (21), no large-scale international multicenter study has investigated the treatment of acute ON. In particular, the effect of time to treatment on visual outcomes has not been examined prospectively, either in a multi-racial cohort or with regard to different ON etiologies. Therefore, clinical treatment decisions are largely based on individual choices but lack scientific evidence. ACON will address the question of the potential benefit of hyperacute high-dose corticosteroids on visual acuity, visual function in daily routine, QoL, and optic nerve structural outcomes in acute MS-ON, AQP4-IgG+ON, and MOG-IgG+ON. ACON will investigate the viability of early clinical clues as potential indicators, both for the underlying diagnosis and the respective disease course. The medical history is the first step in the diagnostic workup. To investigate pain scores as a means of distinguishing MS-ON and AQP4-IgG+ON from MOG-IgG+ON, we will carry out a semi-structured interview to assess the chronology of visual symptoms and characterize pain patterns. Data obtained from this interview, collected from multiple countries, including a wide range of races, are expected to result in an easily accessible clinical tool to accelerate the diagnosis with regard to etiology. Furthermore, ACON aims to explore the implications of early dynamics in levels of NfL and GFAP in the serum of patients with acute ON and their potential prognostic value for a subsequent disease conversion to MS, NMOSD, and MOGAD. MRI of the brain and the spinal cord plays an essential role in the diagnosis of these three diseases. For example, prior studies could show that the combination of two radiologic parameters (e.g., absence of brain abnormalities and a greater lesion extension) offers a valuable tool to discriminate between MS-ON and antibody-associated ON (28, 76). Furthermore, a recent study shows that the length of optic nerve inflammation seen in MRI correlates with retinal neuro-axonal loss and chronic visual impairment (29).
ACON will have the potential to provide information about the interrelation between MRI-based lesion characteristics and clinical symptoms, the duration of contrast enhancement, and predictors of the respective diagnosis.
OCT is the method of choice to measure precisely the thickness of retinal layers and to detect structural damage (77, 78). Axonal degeneration begins on a molecular level, within hours of ON onset and can be reliably quantified by OCT after ~3 months (6, 79, 80). OCT-derived retinal measurements have been used as structural biomarkers for disease progression and tissue damage in MS and related disorders (74, 81–88). Thinning of the combined ganglion cell–inner plexiform layer (GCIPL) in non-ON eyes of people with CIS and early MS is associated with future MS disease activity (84, 85). However, there is no such investigation in acute ON. Prior studies from our groups have shown that cumulative axonal damage, macular GCIPL thinning, and visual loss are typically more severe in AQP4-IgG+ON than in MS-ON and MOG-IgG+ON (89–91), and higher grade pRNFL swelling is closely correlated with MOG-IgG+ON in distinction to MS-ON (30).
ACON will investigate the ability to predict the development of clinically manifested MS through acute OCT parameters including pRNFL and macular ganglion cell analysis, as well as advanced parameters such as the shape of the optic nerve head (92).
ACON provides a global effort for collecting real-world information and high-quality prospective multimodal data on subjects with acute ON from 28 participating centers across six continents. It focuses on the longitudinal observation of subjects with MS-ON, AQP4-IgG+ON, and MOG-IgG+ON. With a better understanding of these distinct neuroimmunological conditions, ACON aims to accelerate ON diagnosis and establish acute ON treatment standards that are applicable globally.
Moreover, the ACON study will provide invaluable insights into the course of these diseases. Particularly, ACON has the capacity to give novel insights into MOGAD for which the proportion of monophasic vs. relapsing cases is far from clear (8). Given a follow-up of 12 months minimum (a longer observation period is envisioned), the study will also generate data on the implementation of preventative immunotherapy (when to treat, whom to treat, and potentially which drug to use?). While there is broad consensus that immediate immunotherapy after diagnosis is indicated in AQP4-IgG+NMOSD given the high risk of recurrence and poor prognosis if left untreated (93–95), the situation is less clear in MS and MOGAD (96, 97), and finally, in light of the rapidly changing treatment landscape with approved drugs for AQP4-IgG+NMOSD and several clinical trials in MOGAD currently underway, the ACON study will collect clinically useful data on individual treatment sequences for on-label or off-label immunotherapies in patients with acute ON (97–100).
Ethics statement
The study was approved by the Ethics Committees from the initiating centers Charité-Universitätsmedizin Berlin (EA2/215/21) and the Rabin Medical Center (0721-18). Ethics Committee approvals and exemptions are obtained separately by each participating center.
Author contributions
SA, NA, JC, FK, IL, SMa, SR, FP, and HS-K: conceptualization. SA, NA, JB, OB, YB, FB, AC-C, EC, SC, JC, CC, MC, RD, JD, KF, EF, CF, CG-A, JH, MH, HK, PK, FK, CLM, ML-P, MLei, NL, MLev, SL, PL, IL, AL, SMo, RM, SMa, CO, FC, MO, JPa, LP, JPe, SP, SR, NR, AS, SSa, BS-D, DS, MS, TS-H, JS, SSi, PSp, PSu, AT, AV-D, AM, AW-Y, LZ, HZ, FP, and HS-K: investigation. SA, NA, JC, FK, RM, SM, ML, IL, MO, JPa, SR, AW-Y, HZ, FP, and HS-K: methodology. SA, FP, and HS-K: project administration. SA, KF, MO, and AT: software. SA, FP, and HS-K: supervision. SA, FK, PSp, FP, and HS-K: validation. SA and HS-K: visualization and writing—original draft preparation. SA, NA, JB, OB, YB, FB, AC-C, EC, SC, JC, CC, MC, RD, JD, KF, EF, CF, CG-A, JH, MH, HK, PK, FK, CLM, ML-P, MLei, NL, MLev, SL, PL, IL, AL, SMo, RM, SM, CO, FC, MO, JPa, LP, JPe, SP, SR, NR, AS, SSa, BS-D, DS, MS, TS-H, JS, SSi, PSp, PSu, AT, AV-D, AM, AW-Y, LZ, HZ, FP, and HS-K: writing—review and editing. All authors contributed to the article and approved the submitted version.
Acknowledgments
We thank Axel Petzold for the discussions and comments on the manuscript. We thank the administrative office of the NeuroCure Clinical Research Center (NCRC), funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) under Germany's Excellence Strategy—EXC-2049-390688087 and Charité-BIH Clinical Study Center for their support.
Conflict of interest
SA has received speaker honoraria from Alexion, Bayer, and Roche. JB reports payment for consultation from Horizon Therapeutics, Alexion, Antigenomycs, BeiGene, Chugai, Clene Nanomedicine, Genentech, Reistone Bio, Roche, Imcyse, and TG; grants from Alexion, Novartis, and the National Institutes of Health. In addition, JB has a patent on Compositions and methods for the treatment of neuromyelitis optica. YB has received speaker honoraria from Novartis, Roche, Genzyme-Sanofi, Merck, and Biogen. EC has received reimbursement for developing educational presentations, educational and research grants, consultation fees, and/or travel stipends from Biogen Argentina, Genzyme Argentina, Merck Argentina and LATAM, Roche Argentina and LATAM, Raffo, Novartis Argentina, LACTRIMS, and The Guthy-Jackson Charitable Foundation.
JC has served on advisory boards for Horizon, Roche, and UCB. CC has received honoraria for speaking from Bayer and research funding from Novartis. JD has received royalties from Wolters Kluwer, Neurology—UpToDate and from Medlink Neurology as contributing author, from Athena Diagnostics for the use of Ma2 as an autoantibody test, and from Euroimmun for the use of NMDA-receptor, GABA(B)-receptor, GABA(A)-receptor, DPPX, and IgLON5 as autoantibody tests and has received research support from Advance Medical (allosteric modulation of NMDAR) SAGE Therapeutics, Instituto Carlos III/FEDER (FIS PI20/00197, CIBERER CB15/00010, Proyectos Integrados de Excelencia, PIE 16/00014 and AC18/00009), Agencia de Gestio d'Ajuts Universitaris i de Recerca (AGAUR), CERCA Programme Generalitat de Catalunya, ERA-NET NEURON, La Caixa Foundation Health Research Award, Pablove Foundation Childhood Cancer Grant, Safra Foundation, Sage therapeutics, Cellex Foundation, and La Caixa Health Foundation. EF has served on advisory boards for Alexion, Genentech, Horizon Therapeutics, and UCB. He has received speaker honoraria from Pharmacy Times. He received royalties from up-to-date. EF was a site primary investigator in a randomized clinical trial on Inebilizumab in neuromyelitis optica spectrum disorder run by Medimmune/Viela-Bio/Horizon Therapeutics. EF has received funding from the NIH (R01NS113828). EF is a member of the medical advisory board of the MOG project. EF is an editorial board member of the Journal of the Neurological Sciences and Neuroimmunology Reports. A patent has been submitted on DACH1-IgG as a biomarker of paraneoplastic autoimmunity. CF participates in a regional medical board advisory of Alexion. CG-A has received grants from Biogen Colombia. JH reports grants for OCT research from the Friedrich-Baur-Stiftung and Merck, personal fees, and non-financial support from Celgene, Janssen, Bayer, Merck, Alexion, Horizon, Novartis, Roche, Biogen, and non-financial support of the Guthy-Jackson Charitable Foundation, all outside the submitted work. JH was partially funded by the German Federal Ministry of Education and Research [(DIFUTURE), Grant Numbers 01ZZ1603[A-D] and 01ZZ1804[A-H]]. HK has received a grant from the National Research Foundation of Korea; consultancy/speaker fees or research support from Alexion, Aprilbio, Altos Biologics, Biogen, Celltrion, Daewoong, Eisai, GC Pharma, HanAll BioPharma, Handok, Horizon Therapeutics (formerly Viela Bio), Kolon Life Science, MDimune, Mitsubishi Tanabe Pharma, Merck Serono, Novartis, Roche, Sanofi Genzyme, Teva-Handok, and UCB; and is a coeditor for the Multiple Sclerosis Journal and an associated editor for the Journal of Clinical Neurology. CLM reports consultancy fees for Chiesi Farmaceutici, Regulatory PharmaNet, and Thenewway Srl and received speaker honoraria and/or travel support for meetings from Santhera Pharmaceuticals, Chiesi Farmaceutici, Regulatory Pharma Net, Thenewway Srl, First Class Srl, and Biologix. ML-P has received funding for travel and speaker honoraria from Novartis, Biogen, and Roche. MLei was funded by NHS (Myasthenia and Related Disorders Service and National Specialized Commissioning Group for Neuromyelitis Optica, UK) and by the University of Oxford, UK. She has been awarded research grants from the UK association for patients with myasthenia—Myaware and the University of Oxford. She has received speaker honoraria or travel grants from Biogen Idec, Novartis, Argenx, UCB, and the Guthy–Jackson Charitable Foundation. MLei serves on scientific or educational advisory boards for UCB Pharma, Argenx, and Viela/Horizon. SL has received consulting fees and speaker honoraria from Biogen, Novartis, TEVA, Genzyme, Sanofy, and Merck. PL has received reimbursement for developing educational presentations, educational and research grants, consultation fees, and/or travel stipends from Biogen Argentina and LATAM, Genzyme Argentina, Merck Argentina, Roche Argentina, Novartis Argentina, and LACTRIMS. AL has served as a Biogen, Bristol Myers Squibb, Merck Serono, Novartis, Roche, Sanofi/Genzyme, and Teva Advisory Board Member, has received congress and travel/accommodation expense compensations, or speaker honoraria from Biogen, Merck Serono, Mylan, Novartis, Roche, Sanofi/Genzyme, Teva, and Fondazione Italiana Sclerosi Multipla (FISM), her institutions received research grants from Novartis and Sanofi/Genzyme. SMo reports consultancy fees (Invex Therapeutics); advisory board fees (Invex therapeutics, Gensight); and speaker fees (Heidelberg engineering, Chugai-Roche Ltd., Allergan, Santen, Chiesi, and Santhera), all outside the submitted work. RM serves on scientific advisory boards for Alexion, Horizon Therapeutics, Roche, and UCB has received speaker honoraria from Alexion, Biogen, Horizon Therapeutics, Novartis, Roche, and Sanofi Genzyme, has received support for attending scientific meetings by Merck and Euroimmun, has received speaker honoraria from Biogen and Novartis. SMa received speaker honoraria for presenting at scientific meetings by Novartis and Biogen. SMo reports consultancy fees (Invex Therapeutics); advisory board fees (Invex therapeutics, Gensight); and speaker fees (Heidelberg engineering, Chugai-Roche Ltd., Allergan, Santen, Chiesi, and Santhera). All outside the submitted work. FC receives ongoing research support from the National Multiple Sclerosis Society (NMSS), the American Academy of Neurology (AAN), and Deutsche Gesellschaft für Neurologie (DGN). JPa has received support for scientific meetings and honorariums for advisory work from Merck Serono, Novartis, Chugai, Alexion, Roche, Medimmune, Argenx, UCB, Mitsubishi, Amplo, Janssen, and Sanofi. Grants from Alexion, Roche, Medimmune, UCB, and Amplo biotechnology. Patent ref P37347WO and license agreement Numares multimarker MS diagnostics Shares in AstraZeneca. Acknowledges Partial funding by Highly specialized services NHS England. SP is a named inventor on filed patents that relate to functional AQP4/NMO-IgG assays and NMO-IgG as a cancer marker, was consulted for Alexion and MedImmune, has received research support from Grifols, MedImmune, and Alexion, all compensation for consulting activities is paid directly to Mayo Clinic. SR has received research funding from the National Health and Medical Research Council (Australia), the Petre Foundation, the Brain Foundation (Australia), the Royal Australasian College of Physicians, and the University of Sydney. She was supported by an NHMRC Investigator Grant (GNT2008339). She serves as a consultant on an advisory board for UCB and Limbic Neurology and has been an invited speaker for Biogen, Excemed, and Limbic Neurology. AS received personal compensation for consulting, serving on a scientific advisory board, speaking, or other activities with Merck-Serono, Sanofi, Biogen, Roche, Novartis, Alexion, Janssen, and Horizon Therapeutics. DS received a grant from the National Multiple Sclerosis Society and serves on several advisory committees for the Multiple Sclerosis International Federation in unpaid roles. MS received speaker honoraria from Teva Pharmaceuticals and has received funding from the German Research Foundation, Federal Ministry of Education and Research and Federal Ministry for Economic Affairs and Energy, Volkswagen Stiftung, and Berlin Institute of Health. He is holding patents for the 3D printing of computed tomography models and is a shareholder of PhantomX and MSC3D. All unrelated to this work. PSu has served on advisory boards for Horizon Therapeutics, Viridian Therapeutics, Invex Therapeutics, Kriya Therapeutics, and GenSight Biologics. He receives research support from the NIH, DOD, Horizon, Invex, and Viridian. AM has received a grant for Biopas Laboratories and reports speaking fees from Chiesi. HZ received research grants from Novartis and speaking fees from Bayer Healthcare, unrelated to this project. FP served on the scientific advisory boards of Novartis and MedImmune; received travel funding and/or speaker honoraria from Bayer, Novartis, Biogen, Teva, Sanofi-Aventis/Genzyme, Merck Serono, Alexion, Chugai, MedImmune, and Shire; is an associate editor of Neurology: Neuroimmunology & Neuroinflammation; is an academic editor of PLoS ONE; consulted for Sanofi Genzyme, Biogen, MedImmune, Shire, and Alexion; received research support from Bayer, Novartis, Biogen, Teva, Sanofi-Aventis/Geynzme, Alexion, and Merck Serono; and received research support from the German Research Council, Werth Stiftung of the City of Cologne, German Ministry of Education and Research, Arthur Arnstein Stiftung Berlin, EU FP7 Framework Program, Arthur Arnstein Foundation Berlin, Guthy-Jackson Charitable Foundation, and NMSS. HS-K received speaker honoraria from Roche.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1102353/full#supplementary-material
References
1. Toosy AT, Mason DF, Miller DH. Optic neuritis. Lancet Neurol. (2014) 13:83–99. doi: 10.1016/S1474-4422(13)70259-X
2. Ducloyer JB, Marignier R, Wiertlewski S, Lebranchu P. Optic neuritis classification in 2021. Eur J Ophthalmol. (2022) 32:754–66. doi: 10.1177/11206721211028050
3. Petzold A, Wattjes MP, Costello F, Flores-Rivera J, Fraser CL, Fujihara K, et al. The investigation of acute optic neuritis: a review and proposed protocol. Nat Rev Neurol. (2014) 10:447–58. doi: 10.1038/nrneurol.2014.108
4. Soelberg K, Jarius S, Skejoe HPB, Engberg H, Mehlsen JJ, Nilsson AC, et al. A population-based prospective study of optic neuritis. Mult Scler. (2017) 23:1893–901. doi: 10.1177/1352458517734070
5. Juenger V, Cooper G, Chien C, Chikermane M, Oertel FC, Zimmermann H, et al. Optic chiasm measurements may be useful markers of anterior optic pathway degeneration in neuromyelitis optica spectrum disorders. Eur Radiol. (2020) 30:5048–58. doi: 10.1007/s00330-020-06859-w
6. Soelberg K, Specovius S, Zimmermann HG, Grauslund J, Mehlsen JJ, Olesen C, et al. Optical coherence tomography in acute optic neuritis: a population-based study. Acta Neurol Scand. (2018) 138:566–73. doi: 10.1111/ane.13004
7. Pache AF, Wildemann B, Paul F, Jarius S. Neuromyelitis optica. Fortschr Neurol Psychiatr. (2017) 85:100–14. doi: 10.1055/s-0042-124186
8. Marignier R, Hacohen Y, Cobo-Calvo A, Pröbstel A-K, Aktas O, Alexopoulos H, et al. Myelin-oligodendrocyte glycoprotein antibody-associated disease. Lancet Neurol. (2021) 20:762–72. doi: 10.1016/S1474-4422(21)00218-0
9. Braithwaite T, Subramanian A, Petzold A, Galloway J, Adderley NJ, Mollan SP, et al. Trends in optic neuritis incidence and prevalence in the uk and association with systemic and neurologic disease. JAMA Neurol. (2020) 77:1514–23. doi: 10.1001/jamaneurol.2020.3502
10. Srikajon J, Siritho S, Ngamsombat C, Prayoonwiwat N, Chirapapaisan N. Differences in clinical features between optic neuritis in neuromyelitis optica spectrum disorders and in multiple sclerosis. Mult Scler J Exp Transl Clin. (2018) 4:1–12. doi: 10.1177/2055217318791196
11. Jarius S, Ruprecht K, Kleiter I, Borisow N, Asgari N, Pitarokoili K, et al. MOG-IgG in NMO and related disorders: a multicenter study of 50 patients. Part 2: epidemiology, clinical presentation, radiological and laboratory features, treatment responses, and long-term outcome. J Neuroinflamm. (2016) 13:1–45. doi: 10.1186/s12974-016-0718-0
12. Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome). Neurology. (1999) 53:1107–14. doi: 10.1212/WNL.53.5.1107
14. Kitley J, Leite MI, Nakashima I, Waters P, McNeillis B, Brown R, et al. Prognostic factors and disease course in aquaporin-4 antibody-positive patients with neuromyelitis optica spectrum disorder from the United Kingdom and Japan. Brain. (2012) 135:1834–49. doi: 10.1093/brain/aws109
15. Akaishi T, Sato DK, Takahashi T, Nakashima I. Clinical spectrum of inflammatory central nervous system demyelinating disorders associated with antibodies against myelin oligodendrocyte glycoprotein. Neurochem Int. (2019) 130:104319. doi: 10.1016/j.neuint.2018.10.016
16. Schmidt F, Zimmermann H, Mikolajczak J, Oertel FC, Pache F, Weinhold M, et al. Severe structural and functional visual system damage leads to profound loss of vision-related quality of life in patients with neuromyelitis optica spectrum disorders. Mult Scler Relat Disord. (2017) 11:45–50. doi: 10.1016/j.msard.2016.11.008
17. Graves JS, Oertel FC, Van der Walt A, Collorone S, Sotirchos ES, Pihl-Jensen G, et al. Leveraging visual outcome measures to advance therapy development in neuroimmunologic disorders. Neurol Neuroimmunol Neuroinflamm. (2022) 9:e1126. doi: 10.1212/NXI.0000000000001126
18. Petzold A, Fraser CL, Abegg M, Alroughani R, Alshowaeir D, Alvarenga R, et al. Diagnosis and classification of optic neuritis. Lancet Neurol. (2022) 4422:1120–34.
19. Group RWB and the optic neuritis study, Beck RW, Cleary PA, Anderson MM, Keltner JL, Shults WT. A Randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. N Engl J Med. (1992) 326:581–8. doi: 10.1056/NEJM199202273260901
20. Plant GT, Sibtain NA, Thomas D. Hyperacute corticosteroid treatment of optic neuritis at the onset of pain may prevent visual loss: a case series. Mult Scler Int. (2011) 2011:1–8. doi: 10.1155/2011/815068
21. Beck RW. The optic neuritis treatment trial: three-year follow-up results. Arch Ophthalmol. (1995) 113:136–7. doi: 10.1001/archopht.1995.01100020014004
22. Nakamura M, Nakazawa T, Doi H, Hariya T, Omodaka K, Misu T, et al. Early high-dose intravenous methylprednisolone is effective in preserving retinal nerve fiber layer thickness in patients with neuromyelitis optica. Graefe's Arch Clin Exp Ophthalmol. (2010) 248:1777–85. doi: 10.1007/s00417-010-1344-7
23. Osinga E, van Oosten B, de Vries-Knoppert W, Petzold A. Time is vision in recurrent optic neuritis. Brain Res. (2017) 1673:95–101. doi: 10.1016/j.brainres.2017.08.012
24. Stiebel-Kalish H, Hellmann MA, Mimouni M, Paul F, Bialer O, Bach M, et al. Does time equal vision in the acute treatment of a cohort of AQP4 and MOG optic neuritis? Neurol Neuroimmunol NeuroInflamm. (2019) 6:1–7. doi: 10.1212/NXI.0000000000000572
25. Ramanathan S, Mohammad S, Tantsis E, Nguyen TK, Merheb V, Fung VSC, et al. Clinical course, therapeutic responses and outcomes in relapsing MOG antibody-associated demyelination. J Neurol Neurosurg Psychiatry. (2018) 89:127–37. doi: 10.1136/jnnp-2017-316880
26. Khanna S, Sharma A, Huecker J, Gordon M, Naismith RT, Van Stavern GP. Magnetic resonance imaging of optic neuritis in patients with neuromyelitis optica versus multiple sclerosis. J Neuro Ophthalmol. (2012) 32:216–20. doi: 10.1097/WNO.0b013e318254c62d
27. Storoni M, Davagnanam I, Radon M, Siddiqui A, Plant GT. Distinguishing optic neuritis in neuromyelitis optica spectrum disease from multiple sclerosis: a novel magnetic resonance imaging scoring system. J Neuro Ophthalmol. (2013) 33:123–7. doi: 10.1097/WNO.0b013e318283c3ed
28. Ramanathan S, Prelog K, Barnes EH, Tantsis EM, Reddel SW, Henderson APD, et al. Radiological differentiation of optic neuritis with myelin oligodendrocyte glycoprotein antibodies, aquaporin-4 antibodies, and multiple sclerosis. Mult Scler. (2016) 22:470–82. doi: 10.1177/1352458515593406
29. Denis M, Woillez JP, Smirnov VM, Drumez E, Lannoy J, Boucher J, et al. Optic nerve lesion length at the acute phase of optic neuritis is predictive of retinal neuronal loss. Neurol Neuroimmunol Neuroinflamm. (2022) 9:e200021. doi: 10.1212/NXI.0000000000001135
30. Chen JJ, Sotirchos ES, Henderson AD, Vasileiou ES, Flanagan EP, Bhatti MT, et al. OCT retinal nerve fiber layer thickness differentiates acute optic neuritis from MOG antibody-associated disease and Multiple Sclerosis: RNFL thickening in acute optic neuritis from MOGAD vs MS. Mult Scler Relat Disord. (2022) 58:103525. doi: 10.1016/j.msard.2022.103525
31. Glass KM, Greecher CP, Kim K. Doheny. Retinal nerve fiber layer thickness in healthy eyes of african, chinese, and latino americans: a population-based multiethnic study. Ophthalmology. (2011) 128:1005–15. doi: 10.1016/j.ophtha.2020.11.015
32. Xu SC, Kardon RH, Leavitt JA, Flanagan EP, Pittock SJ, Chen JJ. Optical coherence tomography is highly sensitive in detecting prior optic neuritis. Neurology. (2019) 92:e527–35. doi: 10.1212/WNL.0000000000006873
33. Behbehani R, Al-Moosa A, Sriraman D, Alroughani R. Ganglion cell analysis in acute optic neuritis. Mult Scler Relat Disord. (2016) 5:66–9. doi: 10.1016/j.msard.2015.10.008
34. van den Bosch A, Fransen N, Mason M, Rozemuller AJ, Teunissen C, Smolders J, et al. Neurofilament light chain levels in multiple sclerosis correlate with lesions containing foamy macrophages and with acute axonal damage. Neurol Neuroimmunol Neuroinflamm. (2022) 9:1–12. doi: 10.1212/NXI.0000000000001154
35. Olesen MN, Soelberg K, Debrabant B, Nilsson AC, Lillevang ST, Grauslund J, et al. Cerebrospinal fluid biomarkers for predicting development of multiple sclerosis in acute optic neuritis: a population-based prospective cohort study. J Neuroinflamm. (2019) 16:1–12. doi: 10.1186/s12974-019-1440-5
36. Petzold A, Rejdak K, Plant GT. Axonal degenaration and inflammation in acute optic neuritis. J Neurol Neurosurg Psychiatry. (2004) 75:1178–80. doi: 10.1136/jnnp.2003.017236
37. Modvig S, Degn M, Sander B, Horwitz H, Wanscher B, Sellebjerg F, et al. Cerebrospinal fluid neurofilament light chain levels predict visual outcome after optic neuritis. Mult Scler. (2016) 22:590–8. doi: 10.1177/1352458515599074
38. Middeldorp J, Hol EM. GFAP in health and disease. Prog Neurobiol. (2011) 93:421–43. doi: 10.1016/j.pneurobio.2011.01.005
39. Hol EM, Pekny M. Glial fibrillary acidic protein (GFAP) and the astrocyte intermediate filament system in diseases of the central nervous system. Curr Opin Cell Biol. (2015) 32:121–30. doi: 10.1016/j.ceb.2015.02.004
40. Eng LF, Vanderhaeghen JJ, Bignami A, Gerstl B. An acidic protein isolated from fibrous astrocytes. Brain Res. (1971) 28:351–4. doi: 10.1016/0006-8993(71)90668-8
41. Kaneko K, Kazutoshi Sato D, Nakashima I, Nishiyama S, Tanaka S, Marignier R, et al. Myelin injury without astrocytopathy in neuroin fl ammatory disorders with MOG antibodies. J Neurol Neurosurg Psychiatry. (2016) 87:1257–9. doi: 10.1136/jnnp-2015-312676
42. Misu T, Takano R, Fujihara K, Takahashi T, Sato S, Itoyama Y. Marked increase in cerebrospinal fluid glial fibrillar acidic protein in neuromyelitis optica: an astrocytic damage marker. J Neurol Neurosurg Psychiatry. (2009) 80:575–7. doi: 10.1136/jnnp.2008.150698
43. Ikeda K, Kiyota N, Kuroda H, Sato DK, Nishiyama S, Takahashi T, et al. Severe demyelination but no astrocytopathy in clinically definite neuromyelitis optica with anti-myelin-oligodendrocyte glycoprotein antibody. Mult Scler J. (2015) 21:656–9. doi: 10.1177/1352458514551455
44. Banwell B, Bennett JL, Marignier R, Kim HJ, Brilot F, Flanagan EP, et al. Personal View Diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease : international MOGAD Panel proposed criteria. Lancet Neurol. (2023) 4422:1–15. doi: 10.1016/S1474-4422(22)00431-8
45. Reindl M, Waters P. Myelin oligodendrocyte glycoprotein antibodies in neurological disease. Nat Rev Neurol. (2019) 15:89–102. doi: 10.1038/s41582-018-0112-x
46. Waters PJ, Komorowski L, Woodhall M, Lederer S. A multicenter comparison of MOG-IgG cell- based assays. Neurology. (2019) 92:e1250–5. doi: 10.1212/WNL.0000000000007096
47. Jarius S, Franciotta D, Paul F, Ruprecht K, Bergamaschi R, Rommer PS, et al. Cerebrospinal fluid antibodies to aquaporin-4 in neuromyelitis optica and related disorders: frequency, origin, and diagnostic relevance. J Neuroinflamm. (2010). doi: 10.1186/1742-2094-7-52
48. Mariotto S, Gajofatto A, Batzu L, Delogu R, Sechi G Pietro, Leoni S, et al. Relevance of antibodies to myelin oligodendrocyte glycoprotein in CSF of seronegative cases. Neurology. (2019) 93:E1867–72. doi: 10.1212/WNL.0000000000008479
49. Zhou L, Huang Y, Li H, Fan J, Zhangbao J, Yu H, et al. MOG-antibody associated demyelinating disease of the CNS : a clinical and pathological study in Chinese Han patients. J Neuroimmunol. (2017) 305:19–28. doi: 10.1016/j.jneuroim.2017.01.007
50. Qian P, Lancia S, Alvarez E, Klawiter EC, Cross AH, Naismith RT. Association of neuromyelitis optica with severe and intractable pain. Arch Neurol. (2012) 69:1482–7. doi: 10.1001/archneurol.2012.768
51. Asseyer S, Schmidt F, Chien C, Scheel M, Ruprecht K, Bellmann-Strobl J, et al. Pain in AQP4-IgG-positive and MOG-IgG-positive neuromyelitis optica spectrum disorders. Mult Scler J Exp Transl Clin. (2018) 4:1–12. doi: 10.1177/2055217318796684
52. Asseyer S, Hamblin J, Messina S, Mariano R, Siebert N, Everett R, et al. Prodromal headache in MOG-antibody positive optic neuritis. Mult Scler Relat Disord. (2020) 40:101965. doi: 10.1016/j.msard.2020.101965
53. Leishangthem L, Beres S, Moss HE, Chen J. A tearfully painful darkness. Surv Ophthalmol. (2020) 66:543–9. doi: 10.1016/j.survophthal.2020.06.002
54. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis : 2017 revisions of the McDonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/S1474-4422(17)30470-2
55. Wingerchuk DM, Banwell B, Bennett JL, Cabre P, Carroll W, Chitnis T, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. (2015) 85:177–89. doi: 10.1212/WNL.0000000000001729
56. Jarius S, Paul F, Aktas O, Asgari N, Dale RC, Seze J De, et al. MOG encephalomyelitis : international recommendations on diagnosis and antibody testing. J Neuroinflamm. (2018) 15:1–10. doi: 10.1186/s12974-018-1144-2
57. Reindl M, Schanda K, Woodhall M, Tea F, Ramanathan S, Sagen J, et al. International multicenter examination of MOG antibody assays. Neurol Neuroimmunol Neuroinflamm. (2020) 7:1–12. doi: 10.1212/NXI.0000000000000674
58. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. (1983) 33:1444–52. doi: 10.1212/WNL.33.11.1444
59. Kappos L, D'Souza M, Lechner-Scott J, Lienert C. On the origin of neurostatus. Mult Scler Relat Disord. (2015) 4:182–5. doi: 10.1016/j.msard.2015.04.001
60. Park SH, Park CY, Shin YJ, Jeong KS, Kim NH. Low contrast visual acuity might help to detect previous optic neuritis. Front Neurol. (2020) 11:602193. doi: 10.3389/fneur.2020.602193
61. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. (1994) 23:129–38.
62. Fischer A, Fischer M, Nicholls RA, Lau S, Poettgen J, Patas K, et al. Diagnostic accuracy for major depression in multiple sclerosis using self-report questionnaires. Brain Behav. (2015) 5:e00365. doi: 10.1002/brb3.365
63. Raphael BA, Galetta KM, Jacobs DA, Markowitz CE, Liu GT, Nano-Schiavi ML, et al. Validation and test characteristics of a 10-item neuro-ophthalmic supplement to the NEI-VFQ-25. Am J Ophthalmol. (2006) 142:1026–35. doi: 10.1016/j.ajo.2006.06.060
64. Group TE. EuroQol - a new facility for the measurement of health-related quality of life. Health Policy. (1990) 16:199–208. doi: 10.1016/0168-8510(90)90421-9
65. Jarius S, Probst C, Borowski K, Franciotta D, Wildemann B, Stoecker W, et al. Standardized method for the detection of antibodies to aquaporin-4 based on a highly sensitive immunofluorescence assay employing recombinant target antigen. J Neurol Sci. (2010) 291:52–6. doi: 10.1016/j.jns.2010.01.002
66. Waters P, Reindl M, Saiz A, Schanda K, Tuller F, Kral V, et al. Multicentre comparison of a diagnostic assay: aquaporin-4 antibodies in neuromyelitis optica. J Neurol Neurosurg Psychiatry. (2016) 87:1005–15. doi: 10.1136/jnnp-2015-312601
67. Reindl M, Jarius S, Rostasy K, Berger T. Myelin oligodendrocyte glycoprotein antibodies: how clinically useful are they? Curr Opin Neurol. (2017) 30:295–301. doi: 10.1097/WCO.0000000000000446
68. Schippling S, Balk LJ, Costello F, Albrecht P, Balcer L, Calabresi PA, et al. Quality control for retinal OCT in multiple sclerosis: validation of the OSCAR-IB criteria. Mult Scler J. (2015) 21:163–70. doi: 10.1177/1352458514538110
69. Aytulun A, Cruz-Herranz A, Aktas O, Balcer LJ, Balk L, Barboni P, et al. APOSTEL 2.0 Recommendations for reporting quantitative optical coherence tomography studies. Neurology. (2021) 97:68–79.
70. Yadav SK, Kafieh R, Zimmermann HG, Kauer-Bonin J, Nouri-Mahdavi K, Mohammadzadeh V, et al. Intraretinal layer segmentation using cascaded compressed U-nets. J Imaging. (2022) 8:139. doi: 10.3390/jimaging8050139
71. Gernert JA, Wicklein R, Hemmer B, Kümpfel T, Knier B, Havla J. Peripapillary hyper–reflective ovoid mass–like structures (PHOMS) in AQP4–IgG–positive neuromyelitis optica spectrum disease (NMOSD) and MOG–IgG–associated disease (MOGAD). J Neurol. (2022) 270:1135–40. doi: 10.1007/s00415-022-11381-8
72. Petzold A, Coric D, Balk LJ, Hamann S, Uitdehaag BMJ, Denniston AK, et al. Longitudinal development of peripapillary hyper-reflective ovoid masslike structures suggests a novel pathological pathway in multiple sclerosis. Ann Neurol. (2020) 88:309–19. doi: 10.1002/ana.25782
73. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)-a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
74. Motamedi S, Gawlik K, Ayadi N, Zimmermann HG, Asseyer S, Bereuter C, et al. Normative data and minimally detectable change for inner retinal layer thicknesses using a semi-automated OCT image segmentation pipeline. Front Neurol. (2019) 10:1117. doi: 10.3389/fneur.2019.01117
75. Cruz-Herranz A, Balk LJ, Oberwahrenbrock T, Saidha S, Martinez-Lapiscina EH, Lagreze WA, et al. The APOSTEL recommendations for reporting quantitative optical coherence tomography studies. Neurology. (2016) 86:2303–9. doi: 10.1212/WNL.0000000000002774
76. Denève M, Biotti D, Patsoura S, Ferrier M, Meluchova Z, Mahieu L, et al. MRI features of demyelinating disease associated with anti-MOG antibodies in adults. J Neuroradiol. (2019) 46:312–8. doi: 10.1016/j.neurad.2019.06.001
77. Costello F, Chen JJ. The role of optical coherence tomography in the diagnosis of afferent visual pathway problems: a neuroophthalmic perspective. Handb Clin Neurol. (2021) 178:97–113. doi: 10.1016/B978-0-12-821377-3.00007-6
78. Zimmermann H, Oberwahrenbrock T, Brandt AU, Paul F, Dörr J-M. Optical coherence tomography for retinal imaging in multiple sclerosis. Degener Neurol Neuromuscul Dis. (2014) 4:153–62. doi: 10.2147/DNND.S73506
79. Brandt AU, Specovius S, Oberwahrenbrock T, Zimmermann HG, Paul F, Costello F. Frequent retinal ganglion cell damage after acute optic neuritis. Mult Scler Relat Disord. (2018) 22:141–7. doi: 10.1016/j.msard.2018.04.006
80. Gabilondo I, Martínez-Lapiscina EH, Fraga-Pumar E, Ortiz-Perez S, Torres-Torres R, Andorra M, et al. Dynamics of retinal injury after acute optic neuritis. Ann Neurol. (2015) 77:517–28. doi: 10.1002/ana.24351
81. Oertel FC, Zimmermann H, Paul F, Brandt AU. Optical coherence tomography in neuromyelitis optica spectrum disorders: potential advantages for individualized monitoring of progression and therapy. EPMA J. (2018) 9:21–33. doi: 10.1007/s13167-017-0123-5
82. Oertel FC, Outteryck O, Knier B, Zimmermann H, Borisow N, Bellmann-Strobl J, et al. Optical coherence tomography in myelin-oligodendrocyte-glycoprotein antibody-seropositive patients: a longitudinal study. J Neuroinflamm. (2019) 16:154. doi: 10.1186/s12974-019-1521-5
83. Lu A, Zimmermann HG, Specovius S, Motamedi S, Chien C, Bereuter C, et al. Astrocytic outer retinal layer thinning is not a feature in AQP4-IgG seropositive neuromyelitis optica spectrum disorders. J Neurol Neurosurg Psychiatry. (2022) 93:188–95. doi: 10.1136/jnnp-2021-327412
84. Lin TY, Vitkova V, Asseyer S, Martorell Serra I, Motamedi S, Chien C, et al. Increased serum neurofilament light and thin ganglion cell-inner plexiform layer are additive risk factors for disease activity in early multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. (2021) 8:1–10. doi: 10.1212/NXI.0000000000001051
85. Zimmermann HG, Knier B, Oberwahrenbrock T, Behrens J, Pfuhl C, Aly L, et al. Association of retinal ganglion cell layer thickness with future disease activity in patients with clinically isolated syndrome. JAMA Neurol. (2018) 75:1071–9. doi: 10.1001/jamaneurol.2018.1011
86. Motamedi S, Oertel FC, Yadav SK, Kadas EM, Weise M, Havla J, et al. Altered fovea in AQP4-IgG-seropositive neuromyelitis optica spectrum disorders. Neurol Neuroimmunol Neuroinflamm. (2020) 7:1–12. doi: 10.1212/NXI.0000000000000805
87. Oertel FC, Sotirchos ES, Zimmermann HG, Motamedi S, Specovius S, Asseyer ES, et al. Longitudinal retinal changes in MOGAD. Ann Neurol. (2022) 92:476–85.
88. Oertel FC, Havla J, Roca-Fernández A, Lizak N, Zimmermann H, Motamedi S, et al. Retinal ganglion cell loss in neuromyelitis optica: a longitudinal study. J Neurol Neurosurg Psychiatry. (2018) 89:1259–65. doi: 10.1136/jnnp-2018-318382
89. Stiebel-Kalish H, Lotan I, Brody J, Chodick G, Bialer O, Marignier R, et al. Retinal nerve fiber layer may be better preserved in MOG-IgG versus AQP4-IgG optic neuritis: a cohort study. PLoS ONE. (2017) 12:e0170847. doi: 10.1371/journal.pone.0170847
90. Pache F, Zimmermann H, Mikolajczak J, Schumacher S, Lacheta A, Oertel FC, et al. MOG-IgG in NMO and related disorders: a multicenter study of 50 patients. Part 4: afferent visual system damage after optic neuritis in MOG-IgG-seropositive versus AQP4-IgG-seropositive patients. J Neuroinflamm. (2016) 13:282. doi: 10.1186/s12974-016-0720-6
91. Pardo S, Wang J, Ogbuokiri E, Cowley NJ, Pellegrini N, Murphy OC, et al. Aquaporin-4 IgG seropositivity is associated with worse visual outcomes after optic neuritis than MOG-IgG seropositivity and multiple sclerosis, independent of macular ganglion cell layer thinning. Mult Scler J. (2021) 26:1360–71. doi: 10.1177/1352458519864928
92. Yadav SK, Kadas EM. Optic nerve head three-dimensional shape analysis. J Biomed Opt. (2018) 23:1. doi: 10.1117/1.JBO.23.10.106004
93. Weinshenker BG, Wingerchuk DM, Vukusic S, Linbo L, Pittock SJ, Lucchinetti CF, et al. Neuromyelitis optica IgG predicts relapse after longitudinally extensive transverse myelitis. Ann Neurol. (2006) 59:566–9. doi: 10.1002/ana.20770
94. Kim SH, Jang H, Park NY, Kim Y, Kim SY, Lee MY, et al. Discontinuation of immunosuppressive therapy in patients with neuromyelitis optica spectrum disorder with aquaporin-4 antibodies. Neurol Neuroimmunol Neuroinflamm. (2021) 8:1–5. doi: 10.1212/NXI.0000000000000947
95. Trebst C, Jarius S, Berthele A, Paul F, Schippling S, Wildemann B, et al. Update on the diagnosis and treatment of neuromyelitis optica: recommendations of the Neuromyelitis Optica Study Group (NEMOS). J Neurol. (2014) 261:1–16. doi: 10.1007/s00415-013-7169-7
96. Narayan R, Simpson A, Fritsche K, Salama S, Pardo S, Mealy M, et al. MOG antibody disease: a review of MOG antibody seropositive neuromyelitis optica spectrum disorder. Mult Scler Relat Disord. (2018) 25:66–72. doi: 10.1016/j.msard.2018.07.025
97. Whittam DH, Karthikeayan V, Gibbons E, Kneen R, Chandratre S, Ciccarelli O, et al. Treatment of MOG antibody associated disorders: results of an international survey. J Neurol. (2020) 267:3565–77. doi: 10.1007/s00415-020-10026-y
98. Ringelstein M, Ayzenberg I, Lindenblatt G, Fischer K, Gahlen A, Novi G, et al. Interleukin-6 receptor blockade in treatment-refractory MOG-IGG-associated disease and neuromyelitis optica spectrum disorders. Neurol Neuroimmunol Neuroinflamm. (2022) 9:1–18. doi: 10.1212/NXI.0000000000001100
99. Whittam DH, Cobo-calvo A, Lopez-chiriboga AS, Pardo S, Gornall M, Cicconi S, et al. Treatment of MOG-IgG-associated disorder with rituximab: an international study of 121 patients. Mult Scler Relat Disord. (2020) MSARD 1022:S2211-0348(20)30327-8.
Keywords: Aquaporin-4-IgG (AQP4-IgG), clinically isolated syndrome (CIS), MOG-IgG associated disorders (MOGAD), multiple sclerosis (MS), neuromyelitis optica spectrum disorders (NMOSD), optic neuritis (ON)
Citation: Asseyer S, Asgari N, Bennett J, Bialer O, Blanco Y, Bosello F, Camos-Carreras A, Carnero Contentti E, Carta S, Chen J, Chien C, Chomba M, Dale RC, Dalmau J, Feldmann K, Flanagan EP, Froment Tilikete C, Garcia-Alfonso C, Havla J, Hellmann M, Kim HJ, Klyscz P, Konietschke F, La Morgia C, Lana-Peixoto M, Leite MI, Levin N, Levy M, Llufriu S, Lopez P, Lotan I, Lugaresi A, Marignier R, Mariotto S, Mollan SP, Ocampo C, Cosima Oertel F, Olszewska M, Palace J, Pandit L, Peralta Uribe JL, Pittock S, Ramanathan S, Rattanathamsakul N, Saiz A, Samadzadeh S, Sanchez-Dalmau B, Saylor D, Scheel M, Schmitz-Hübsch T, Shifa J, Siritho S, Sperber PS, Subramanian PS, Tiosano A, Vaknin-Dembinsky A, Mejia Vergara AJ, Wilf-Yarkoni A, Zarco LA, Zimmermann HG, Paul F and Stiebel-Kalish H (2023) The Acute Optic Neuritis Network (ACON): Study protocol of a non-interventional prospective multicenter study on diagnosis and treatment of acute optic neuritis. Front. Neurol. 14:1102353. doi: 10.3389/fneur.2023.1102353
Received: 18 November 2022; Accepted: 30 January 2023;
Published: 24 February 2023.
Edited by:
Harald Hegen, Innsbruck Medical University, AustriaReviewed by:
Franziska Di Pauli, Innsbruck Medical University, AustriaRana Khalil Zabad, University of Nebraska Medical Center, United States
Copyright © 2023 Asseyer, Asgari, Bennett, Bialer, Blanco, Bosello, Camos-Carreras, Carnero Contentti, Carta, Chen, Chien, Chomba, Dale, Dalmau, Feldmann, Flanagan, Froment Tilikete, Garcia-Alfonso, Havla, Hellmann, Kim, Klyscz, Konietschke, La Morgia, Lana-Peixoto, Leite, Levin, Levy, Llufriu, Lopez, Lotan, Lugaresi, Marignier, Mariotto, Mollan, Ocampo, Cosima Oertel, Olszewska, Palace, Pandit, Peralta Uribe, Pittock, Ramanathan, Rattanathamsakul, Saiz, Samadzadeh, Sanchez-Dalmau, Saylor, Scheel, Schmitz-Hübsch, Shifa, Siritho, Sperber, Subramanian, Tiosano, Vaknin-Dembinsky, Mejia Vergara, Wilf-Yarkoni, Zarco, Zimmermann, Paul and Stiebel-Kalish. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanna Asseyer,  susanna.asseyer@charite.de
susanna.asseyer@charite.de
†These authors share last authorship