The causal relationship between risk of developing bronchial asthma and frailty: a bidirectional two-sample Mendelian randomization study
 Xiao Ma
Xiao Ma Haoran Xu1
Haoran Xu1  Jinghui Xie
Jinghui Xie Lu Zhang
Lu Zhang Zegeng Li
Zegeng Li- 1Anhui University of Chinese Medicine, Hefei, China
- 2Department of Respiration, Wuhu Traditional Chinese Medicine Hospital, Wuhu, China
- 3The First Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, China
Background: A potential link between asthma and frailty has been suggested in previous studies. However, the nature of the causal relationship between these two conditions warrants further investigation. Therefore, this study assessed the bidirectional causality between asthma and frailty risk using two-sample Mendelian randomization (MR).
Methods: The study data were obtained from the genome-wide association study (GWAS) dataset, with 337,159 samples representing asthma data and 175,226 samples representing frailty. The causal relationship between the two disorders was assessed by selecting the single nucleotide polymorphisms (SNPs), significantly associated with both asthma and frailty. The inverse variance weighting (IVW) method was used as the main analytical method to estimate the possible influence of causality. Sensitivity analysis was also performed using Mr-Egger intercept, funnel plot, “leave-one-out,” and Cochran Q test. In addition, potential mediators were investigated by risk factor analysis.
Result: The IVW method showed an increased risk of frailty due to increased genetic susceptibility factors and the number of to asthma (OR = 2.325, 95%CI:1.958–2.761; p = 6.527498e-22), while no horizontal pleiotropy was observed for the Mr-Egger intercept (p = 0.609) and the funnel plot. The Cochran Q value was 72.858, p = 0.024, and there was heterogeneity in the Cochran Q-value. No single SNP was observed for “leave-one-out” that had a biasing effect on the instrumental variables. In addition, genetic susceptibility to frailty was associated with asthma (OR = 1.088, 95%CI:1.058–1.119; p = 4.815589e-09). In the causal relationship described above, several risk factors for frailty are complex, with asthma leading to a significant reduction in physical activity endurance.
Conclusion: Our findings suggest a probable positive causal effect of asthma on the risk of developing frailty, potentially mediated by reduced physical activity endurance. At the same time, a causal relationship exists between frailty and asthma. Therefore, assessment strategies for frailty should include asthma and vice versa.
1 Introduction
The Global Asthma Initiative (GINA) defines asthma as a heterogeneous disease caused by chronic airway inflammation (1) due to complex gene–environment interactions. Chronic inflammation causes variable airway obstruction and increased responsiveness, resulting in recurrent symptoms of episodic chest tightness, wheezing, shortness of breath, and/or cough (2). Asthma is a prevalent chronic respiratory condition significantly impacting global health. Globally, asthma affects an estimated 300 million people and causes nearly 250,000 deaths each year (3). Projections indicated that by 2025, the number of individuals with asthma could increase by nearly 100 million (4), with older adults experiencing higher morbidity and mortality rates compared to the younger population (5), contributing substantially to the global disease burden. The presentation, diagnosis, and treatment of asthma in the older adults are further complicated by age-related changes in physiological function and immunology. As with asthma, frailty is recognized as a major public health problem. Frailty is a complex clinical condition associated with aging, prevalent across various demographics. As the physiological capacity of multiple organ systems declines due to population aging (6), the homeostatic reserves of individuals are reduced, leading to increased vulnerability to endogenous and/or exogenous stressors (7). In older adults, frailty increases the risk of progressive decline in several systems and adverse clinical outcomes (8). The increasing prevalence of asthma and frailty markedly impairs the quality of life and exacerbates the burden on healthcare systems due to the associated decline in patient productivity. Thus, both are attracting increasing attention.
The causal linkage between asthma and the condition of frailty has garnered considerable academic scrutiny yet remains a matter of debate. Previous studies conclude (9) that asthma is associated with an increased risk of frailty. In a cross-sectional observational study of older adults asthmatics with frailty (10), the investigators performed the Kihon Frailty Screening Inventory as well as the SF-36 scale, the Hyland scale, the Asthma Quality of Life Questionnaire (AQLQ), the Asthma Control Test (ACT), and the Asthma Control Questionnaire (ACQ). Among 69 outpatient participants with asthma aged over 65, 52 (75.4%) were classified as frail. Kihon Frailty Inventory was significantly associated with all scores obtained on the SF-36, Hyland Scale, AQLQ, ACT, and ACQ, and asthma and frailty were associated. In another study from China (11), 9,416 older adults asthma patients were included in a cross-sectional survey of the epidemiologic status and risk factors of frailty and pre-frailty. In this study, a high prevalence of frailty and pre-frailty was observed among older adults Chinese patients with asthma, suggesting that routine frailty assessment could benefit the management of asthma in this population. Evidence also supports the role of frailty as a significant risk factor for the development and progression of asthma (12). These findings underscore the potential for a bidirectional causal association between asthma and frailty, emphasizing the need to clarify this relationship to inform prevention and treatment strategies for both conditions. Nonetheless, observational studies are prone to confounders and reverse causality, making their results difficult to control (13), thus limiting our understanding of the relationship between the two diseases.
Mendelian randomization (MR) is an emerging statistical approach in epidemiological research that employs genetic variants [single nucleotide polymorphisms (SNPs)] as instrumental variables (IVs) to assess the observed causal relationships between exposure factors and clinical outcomes (14). Genetic variation follows the principle of random assignment of alleles to offspring and the natural causal effect of genetic variation on phenotype (15); hence, SNPs are not subject to potential confounders and are strongly correlated with exposure factors, making MR analyses less susceptible to confounders and reverse causation bias in observational studies (16). The two-sample MR estimates causal relationships, referring to data that measures exposure and outcomes in different datasets typically collected from genome-wide association studies (GWAS). Until now, two-sample MRs have been widely used to explore the causal relationship between different exposures and asthma (17, 18); however, no study has assessed the bidirectional causality between asthma and frailty.
Therefore, this study explored the potential causal relationship between asthma and frailty via a bidirectional two-sample MR study to provide a relevant theoretical basis for the relationship between asthma and frailty development.
2 Materials and methods
2.1 Study design
In this study, a bidirectional two-sample MR analysis was performed to test the bidirectional causality between asthma and frailty using a publicly available GWAS pooled dataset, wherein no raw data were collected; therefore, no additional ethics committee approval or informed consent was required. Further sensitivity analyses were performed to test the reliability of the results. Furthermore, to investigate the potential genetic mechanisms underlying the combination of asthma and frailty, we considered several potential modifiers: body mass index (BMI), vitamin D,triglyceride, smoking, and physical activity (19–21). Here, all MR analyses were required to meet the three basic assumptions: association, independence, and exclusivity (22). Figure 1 presents a brief overview of the bidirectional MR analysis. This study complies with the STROBE-MR guidelines (23).
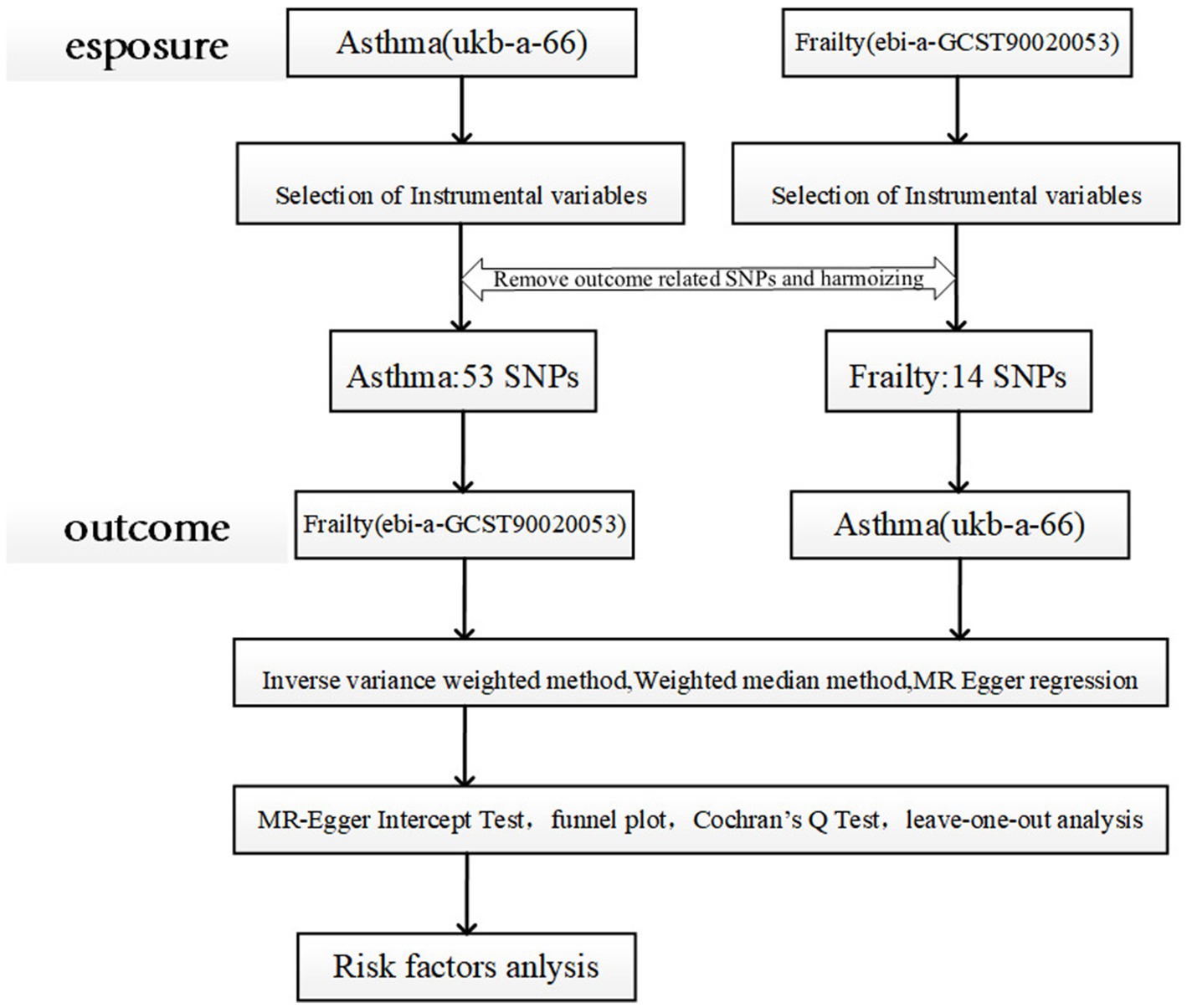
Figure 1. Schematic representation of the two-sample Mendelian randomization study design. MR analyses are required to meet the following criteria: (1) the instrumental variable must be strongly correlated with the exposure factor (assumption of correlation); (2) the instrumental variable must not be correlated with any confounders associated with the “exposure-outcome” association (assumption of independence); and (3) the instrumental variable affects the outcome variable only through the degree of exposure (assumption of exclusivity, also known as “no pleiotropy”). (3) the instrumental variable affects the outcome variable only through the degree of exposure (exclusivity assumption, also known as “no pleiotropy”) (22).ukb-a-66:UK Biobank-a-66.
2.2 Data sources
The study data were mainly extracted from the Integrative Epidemiology Unit Open GWAS project website sample repository.1 The asthma dataset was derived from the UK Biobank, includes 337,159 individuals of European ancestry, and contains 39,049 cases and 298,110 controls. The frailty dataset was obtained from a dataset of 175,226 cases of European ancestry. The two-sample MR assumes independence between exposure data and outcome data. Therefore, data from asthma, having a significant overlap cohort with frailty, were excluded. The GWAS data corresponding to asthma were selected for analysis based on these criteria. Detailed information is shown in Table 1.

Table 1. Extraction of relevant data information from the Genome-Wide Association Studies database.
2.3 Selection of instrumental variables
The first hypothesis of MR was that instrumental variables needed to be highly correlated with exposure factors; therefore, SNPs reaching the GWAS threshold (p < 5 × 10-8) were selected as preliminary results (24). The PLINK software was then employed to exclude SNPs in linkage disequilibrium (r2<0.001, genetic distance = 10,000 KB) (25). The selected instrumental variables were tested for weak instrumental variable bias by calculating the F-value; when the F-value was >10, the instrumental variables could be recognized as sufficient to overcome the weak instrumental tendency (26), further validating the hypothesis of the association between genetic variation and exposure factors, calculated as F = R2(N-2)/(1-R2) (27), where N is the sample size of the exposure factor, and R2 is the instrumental variable explaining the proportion of variance in the exposure factor.
Second, to satisfy the second MR hypothesis of no association of genetic variants with potential confounders, a query was performed using PhenoScanner (28),2 a comprehensive web-based database of genotype–phenotype associations, to determine whether there was no association between the screened SNPs and known confounders. We further investigated whether these SNPs were associated with potential risk factors such as BMI, vitamin D, triglycerides, smoking, and decreased exercise capacity. If SNPs associated with these potential confounders were found at the genome-wide significance level (p < 5 × 10−8), MR-presso analysis was performed to identify outliers. Finally, the remaining SNPs were extracted from the outcome data, ensuring that the effects of instrumental variables on exposure and outcome corresponded to the alleles with the same effects (29).
2.4 Mendelian randomization analysis
To avoid potential pleiotropic effects, three different MR methods (IVW, weighted median, and Mr-Egger) were used to assess the bidirectional causality between asthma and frailty. The primary analytical method to detect possible causality effects was IVW, and the results were supplemented by applying weighted median and Mr-Egger to assess the causal relationship between asthma and frailty in terms of OR values. Applying the MR-Egger method in this analysis yielded wider confidence intervals and non-significant p-values (30). However, the IVW method exhibited higher statistical efficacy than other MR methods and can provide robust results under a wider range of conditions (31). Should there be inconsistencies between the results of various MR analyses and prior research, it would necessitate a careful examination of the p-threshold for selecting instrumental variables, potentially leading to a reanalysis of the data (14).
Sensitivity analyses were performed to assess the reliability of the analyzed results, and potential heterogeneity and horizontal pleiotropy (influencing results through causal pathways rather than exposure) were observed. The Mr-Egger intercept test and funnel plots were used in this study to detect horizontal pleiotropy for all outcomes (p < 0.05 was considered to be horizontal pleiotropy) (32). Subsequently, the results’ stability was assessed using Cochran’s Q-test to test heterogeneity for statistically significant results. Heterogeneity was deemed present in the analysis at p < 0.05 (33). A “leave-one-out” was conducted to evaluate whether the observed causality was reliant upon or unduly influenced by a single SNP within the relationship (34).
2.5 Risk factors
The potential genetic mechanisms underlying the comorbidity of asthma and frailty were explored by analyzing several risk factors, including BMI, vitamin D, triglyceride levels, cigarette smoking, and decreased exercise capacity. Genetic information for BMI was obtained from the Genetic Investigation of Anthropomorphic Traits (GIANT) Consortium (35). The vitamin D dataset was retrieved from the UK Biospecimen Bank (UK Biobank) (36). For lipid metabolism, triglyceride data were collected from the UK Biobank (37). The dataset on smoking was extracted from the Gene Sequencing Consortium (GSCAN) (38). The physical activity datasets were obtained from the UK Biobank (UK Biobank) (39). Table 2 presents details of each dataset. Mendelian randomization was conducted with asthma as the exposure and the aforementioned risk factors as outcomes. IVW was used as the primary analysis method, and a statistically significant difference was p < 0.05.
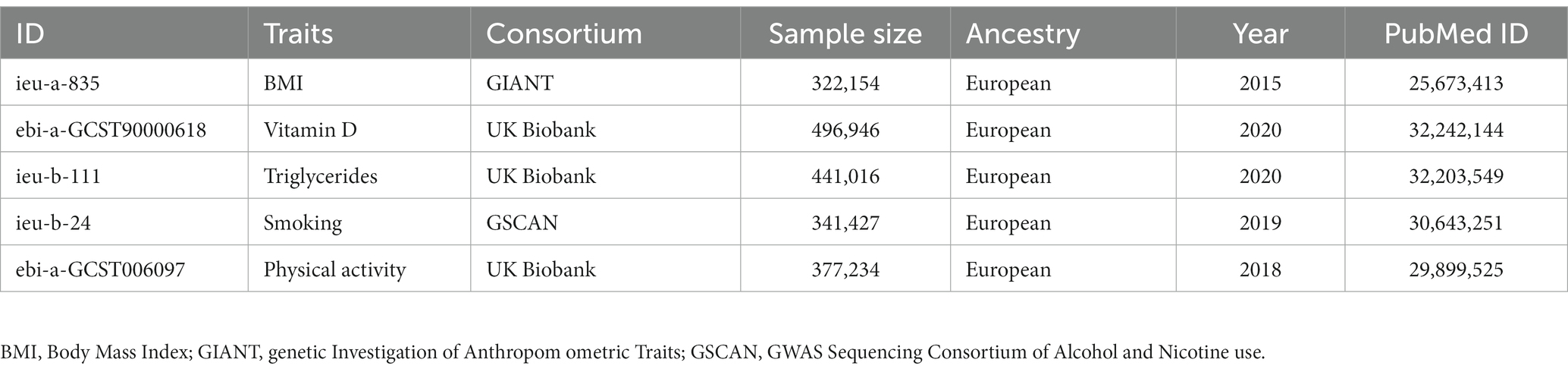
Table 2. Data sources for frailty-related risk factors.
2.6 Statistical analysis
The results of MR analysis are expressed as effect estimates (OR) and 95% confidence intervals (CI) that directly reflect the causal relationship between asthma and frailty, with a statistically significant p < 0.05. All analyses were executed with the two-sample MR package (version 0.5.7) and ggplot2 (version 3.4.2) in R (version 4.1.2).
3 Results
3.1 Identification of genetic instrumental variables
Instrumental variables exhibiting linkage disequilibrium, which could introduce bias, were excluded. Subsequently, 71 asthma-related SNPs meeting stringent selection criteria (genome-wide significance with p < 5 × 10−8 and low linkage disequilibrium with r2 < 0.001) were retrieved from the GWAS database. After data concordance and querying with PhenoScanner (see text footnote 2), confounders were excluded. Eighteen SNPs were detected as confounders and excluded. Finally, 53 SNPs were retained as valid instrumental variables for asthma, of which 12 were also associated with frailty (Table 3). The F statistics of all SNPs were > 10, indicating the absence of any weak bias in the study results and confirming the reliability of statistical test efficacy (Table 4).
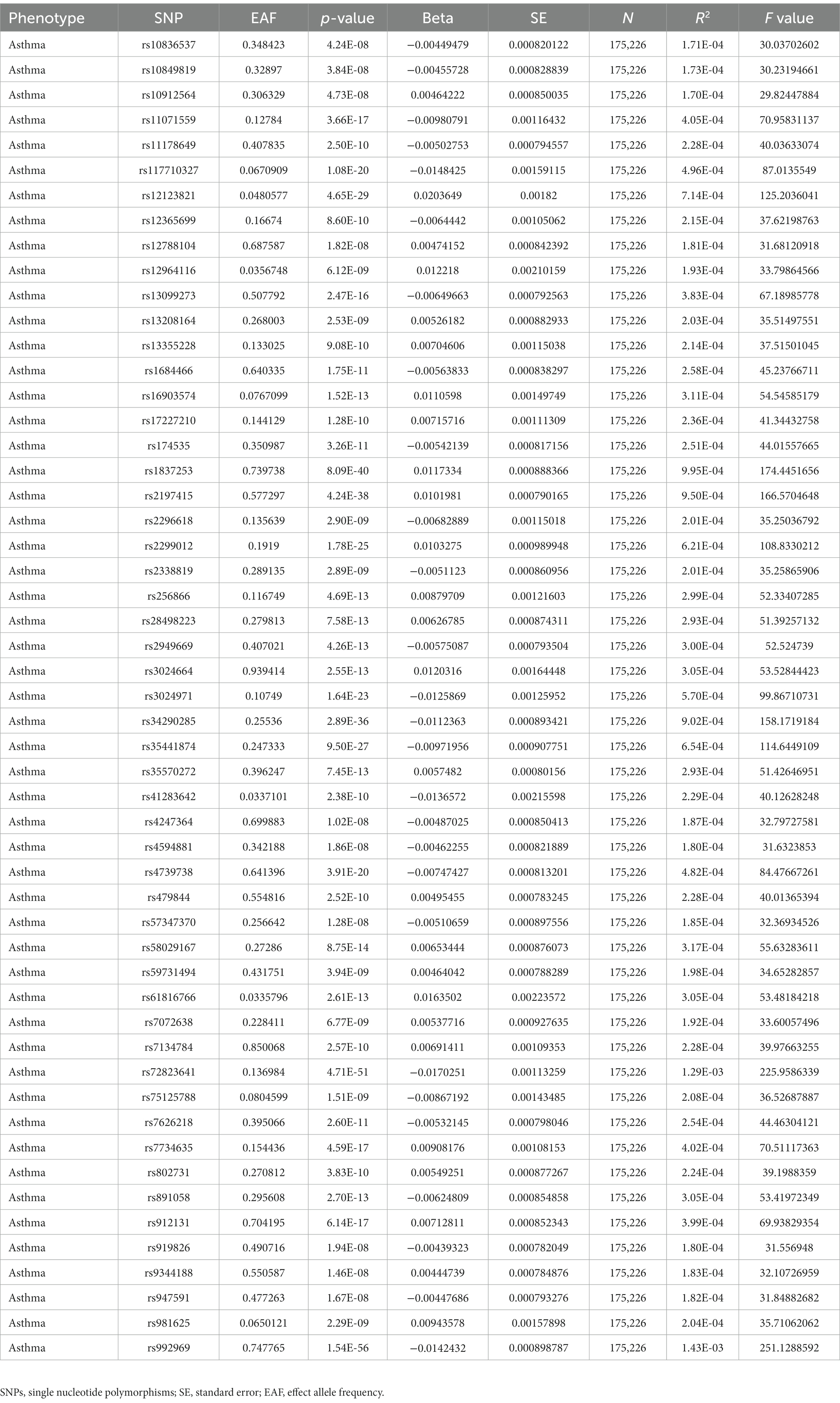
Table 3. Extraction of Single Nucleotide Polymorphisms and F-values for instrumental variables of the asthma genes from the Genome-Wide Association Studies database.
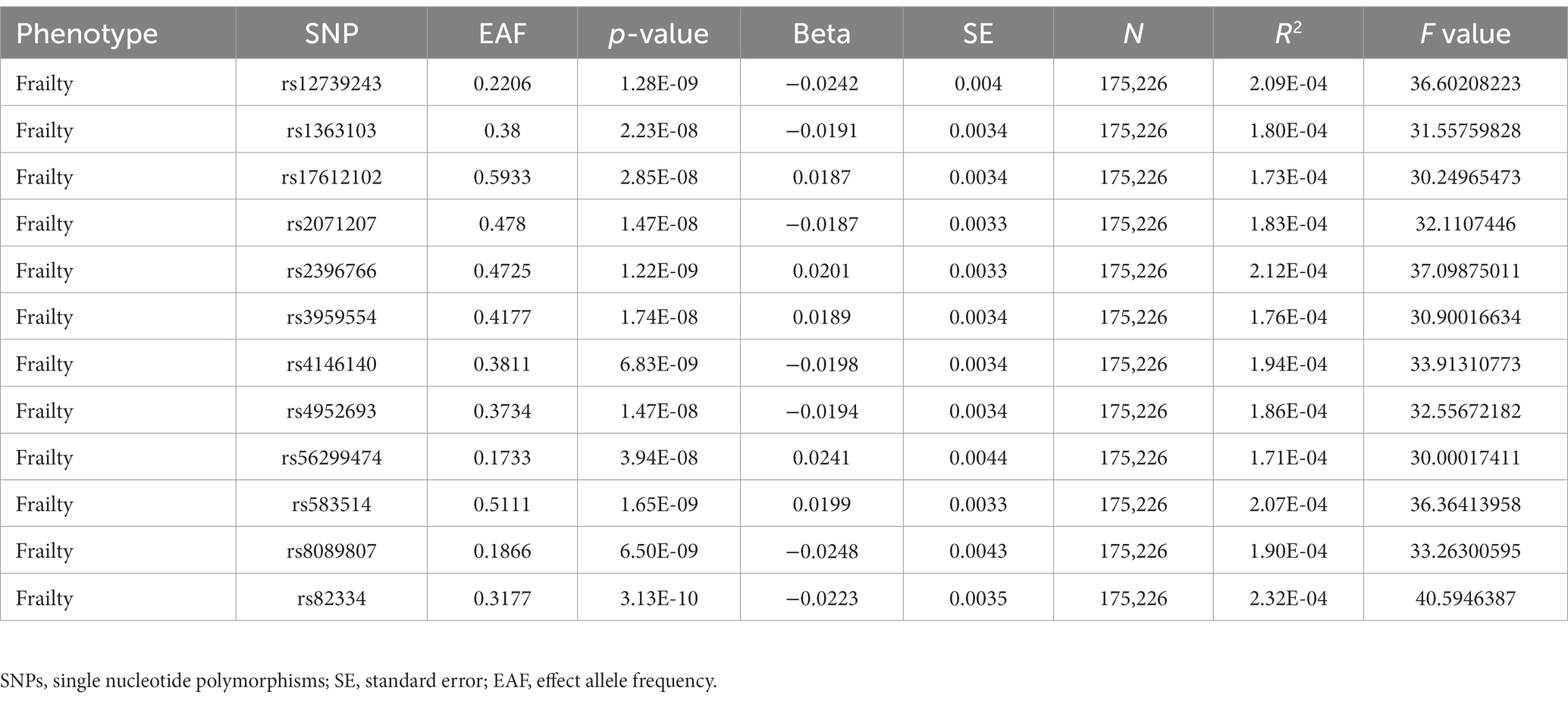
Table 4. Extraction of Single Nucleotide Polymorphisms and F-values for instrumental variables of the frailty genes from the Genome-Wide Association Studies database.
3.2 Mendelian randomization analysis
The analysis examined the genetic susceptibility to asthma as a potential causal factor in frailty development, revealing a strong and positive association (Figure 2). The IVW method revealed that genetic predisposition to asthma increased the risk of developing frailty (OR = 2.325, 95% CI: 1.958–2.761; p = 6.527498e-22) (Table 5), and the same estimate was observed in the weighted median analysis (OR = 1.943, 95% CI: 1.533–2.462; p = 3.921789e-08). In the Mr-Egger analysis (OR = 2.095, 95% CI: 1.358–3.232; p = 1.580040e-03), a consistent direction of effect was observed (see Figure 3 for details), in line with the results of previous studies (40).
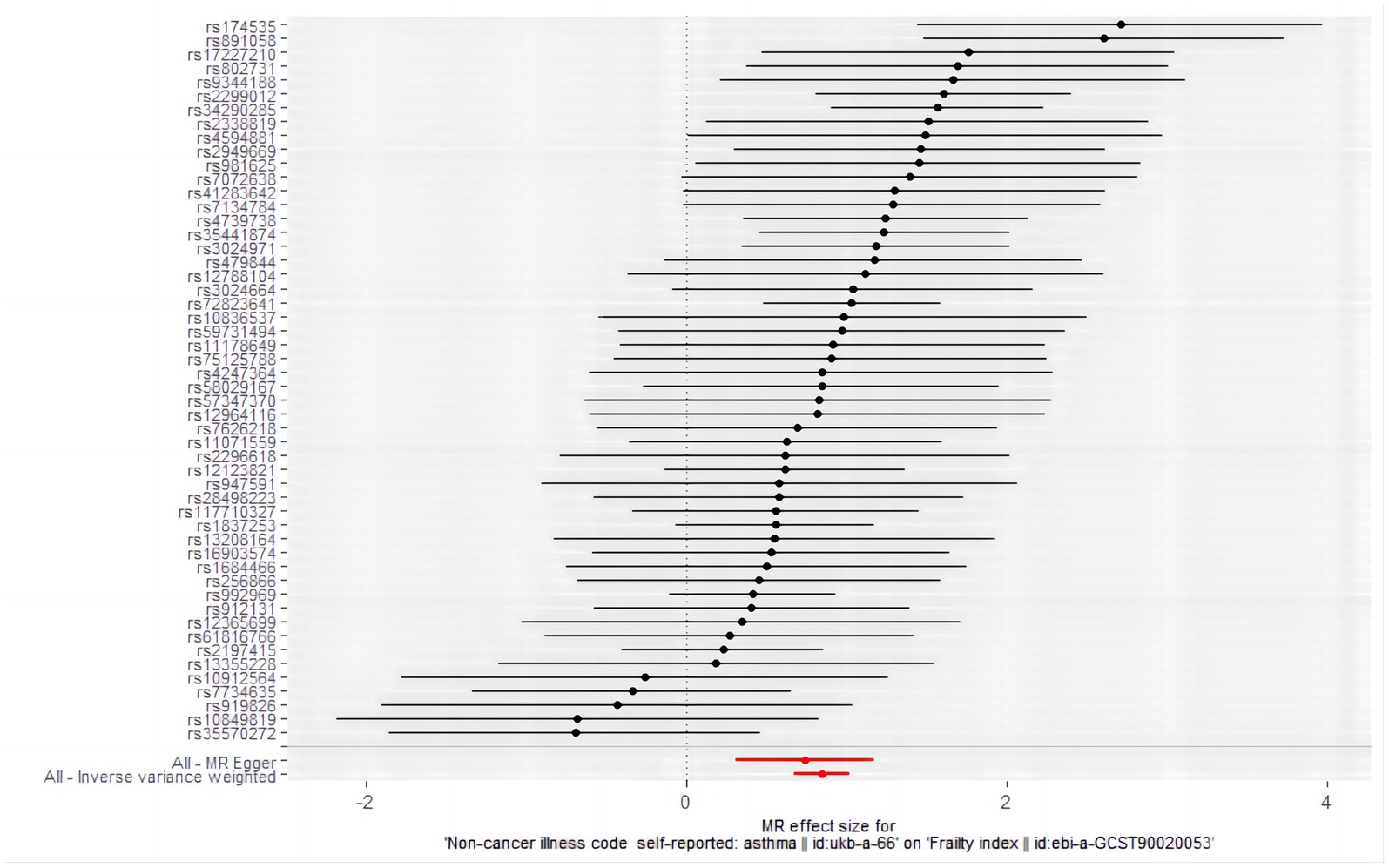
Figure 2. Forest plot of the causal effects of single nucleotide polymorphisms associated with asthma on frailty. Mendelian randomization estimates the effect size and data are expressed as effect values with 95% CI. The significance of red lines are MR results of MR-Egger test and IVW method.
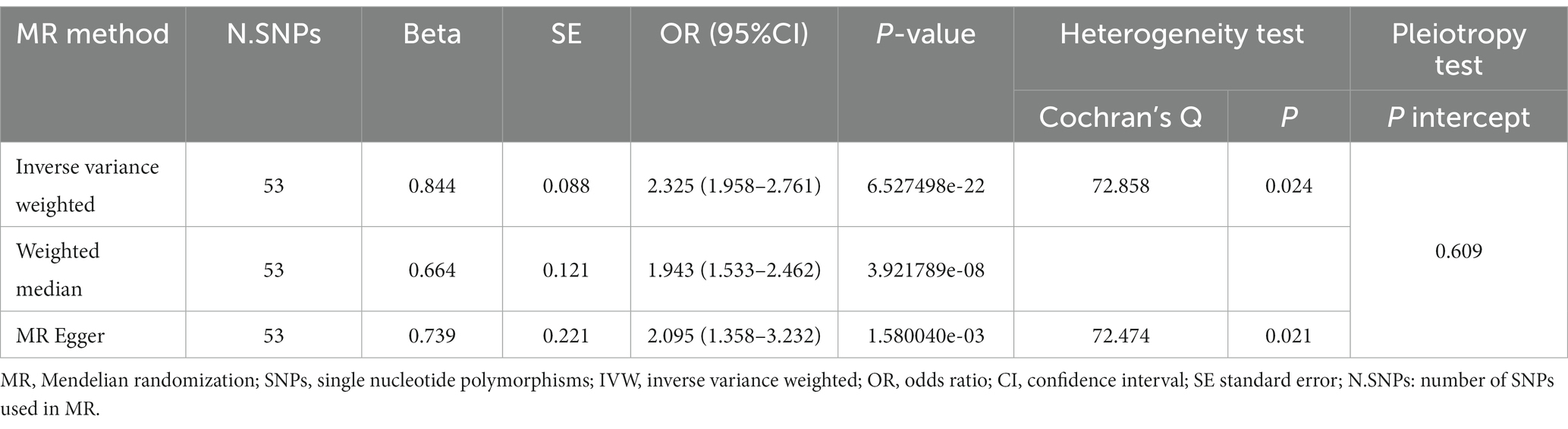
Table 5. Results of MR analysis for the effect of asthma on frailty.
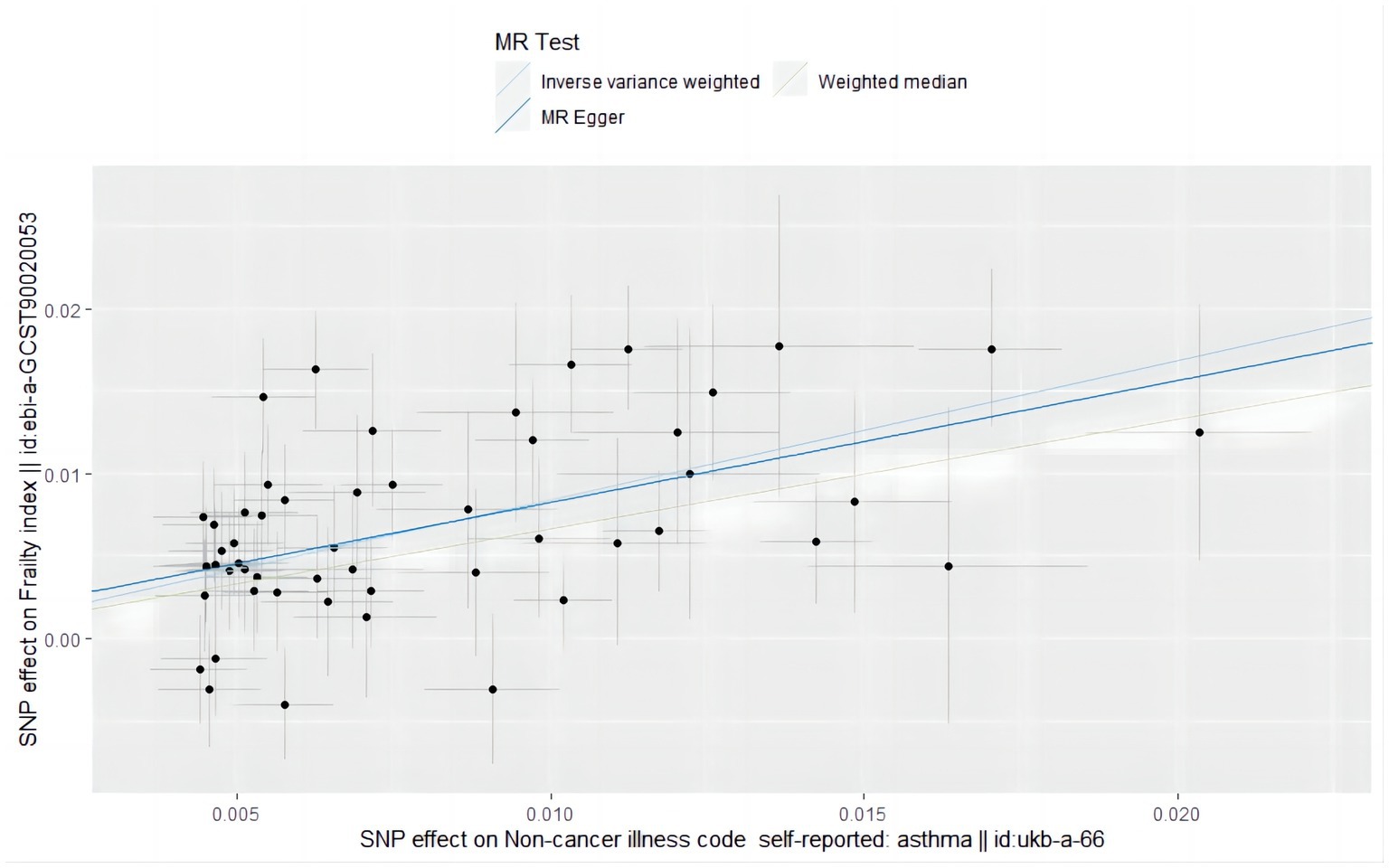
Figure 3. Scatter plot of the causal effect of single nucleotide polymorphisms associated with asthma on frailty in a Mendelian randomization study.
According to the IVW analysis under the random-effects model with frailty as the exposure factor and asthma as the outcome factor, a causal relationship was observed between frailty and asthma (OR = 1.088, 95% CI: 1.058–1.119; p = 4.815589e-09) (Figure 4). Weighted median analysis revealed the same estimate (OR = 1.095, 95% CI: 1.057–1.135; p = 4.723029e-07) (Table 6). The results of the Mr-Egger analysis (OR = 0.889, 95% CI: 0.677–1.166; p = 4.154820e-01) were not statistically significant, probably due to the large Mr-Egger’s confidence interval and lower effectiveness (Figure 5), suggesting a causal relationship between genetic susceptibility to frailty and asthma.
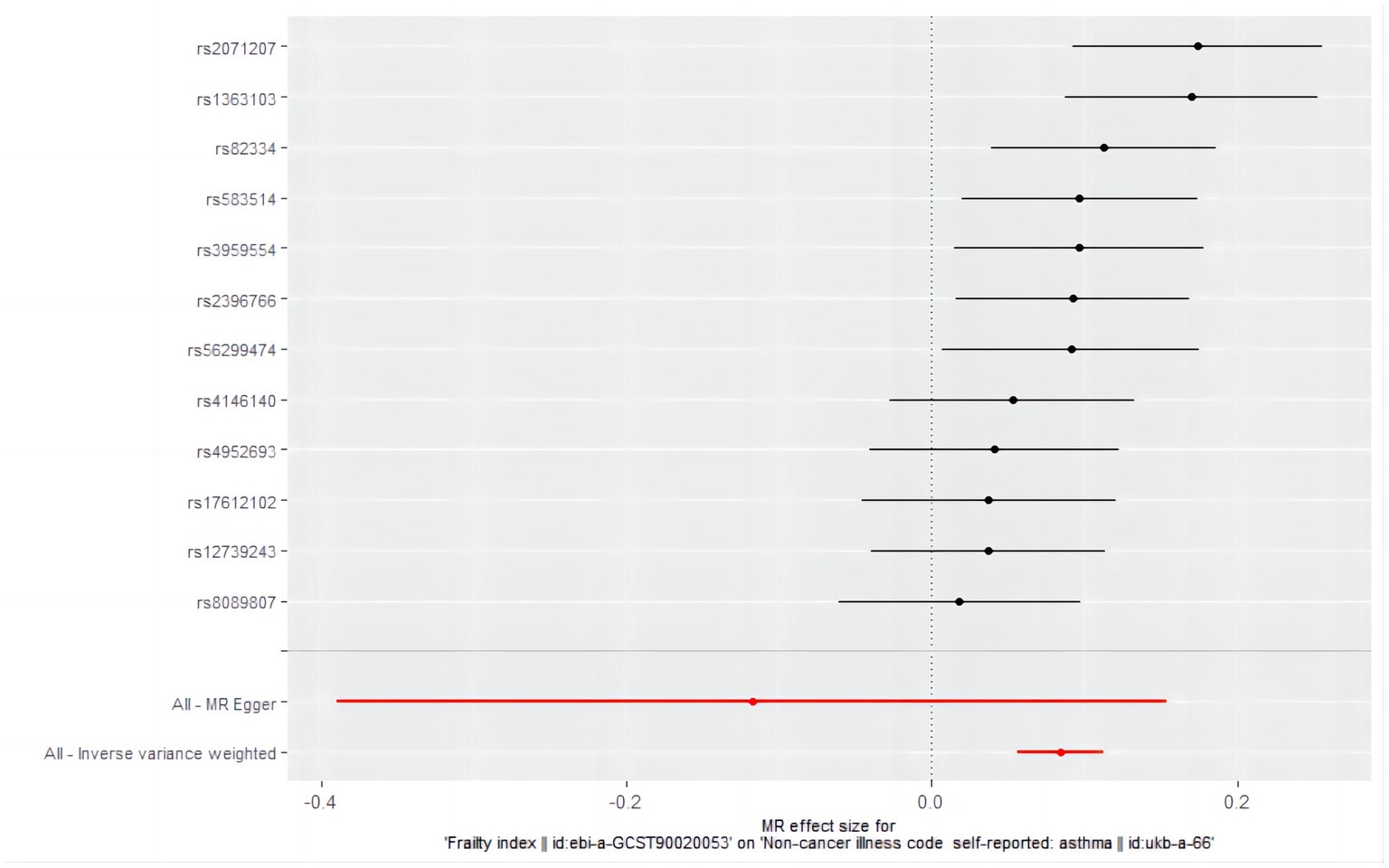
Figure 4. Forest plot of the causal effects of single nucleotide polymorphisms associated with frailty on asthma. Mendelian randomization estimates the effect size and data are expressed as effect values with 95% CI. The significance of red lines are MR results of MR-Egger test and IVW method.

Table 6. Results of MR analysis for the effect of frailty on asthma.
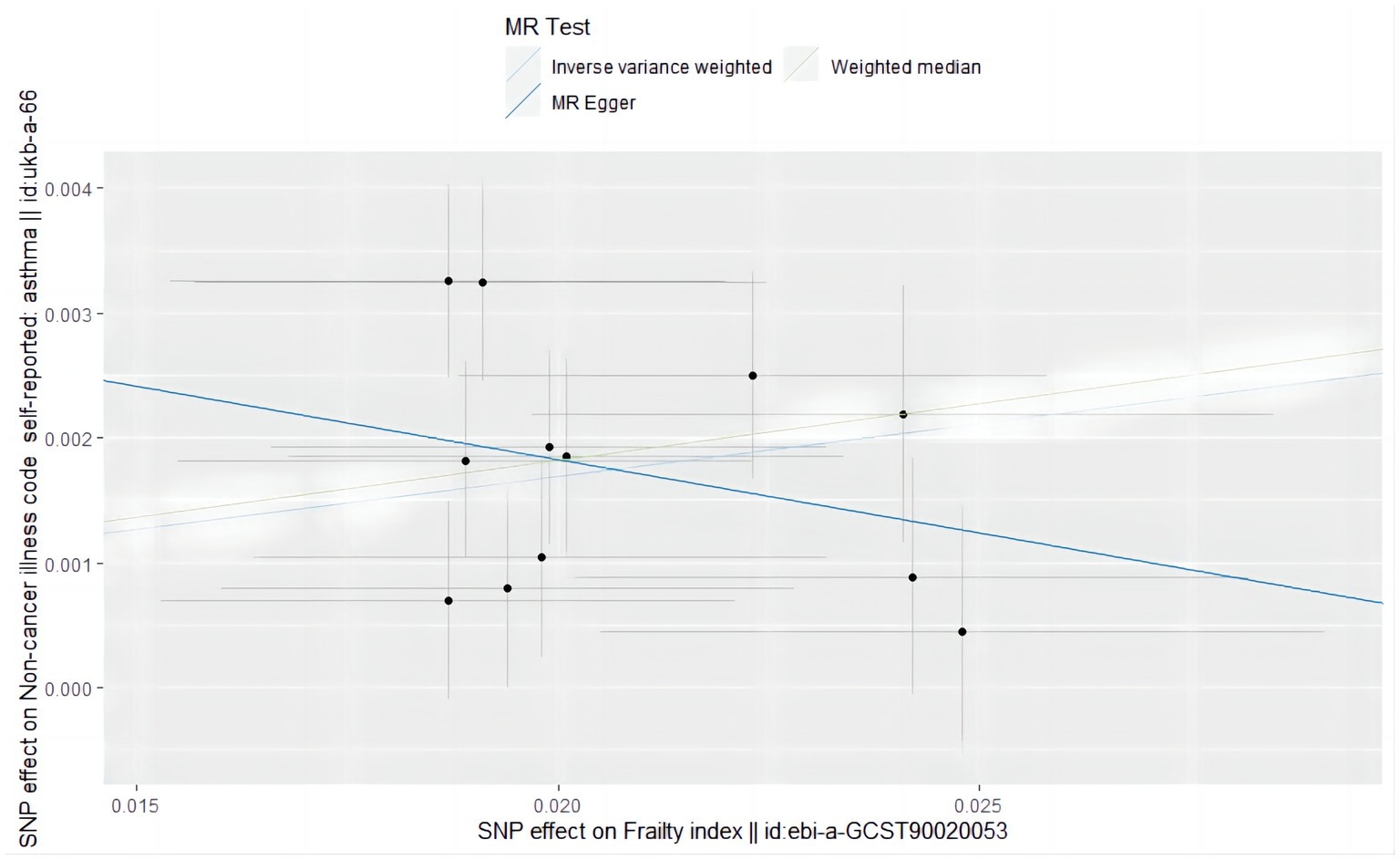
Figure 5. Scatter plot of the causal effect of single nucleotide polymorphisms associated with frailty on asthma in a Mendelian randomization study.
3.3 Sensitivity analysis
A series of sensitivity tests, including Mr-Egger intercept, funnel plot, Mr-PRESSO detection, Cochran Q test, and leave-on-out analysis, were conducted to evaluate the accuracy of the positive results. In the MR analysis with asthma as the exposure factor, the p-value of the Mr-Egger intercept was 0.609. The MR-PRESSO test (p = 0.734) and the symmetric funnel plot (Figure 6) indicated no evidence of horizontal pleiotropy, which might otherwise suggest bias in the asthma-related findings. For further analysis, we used Cochran’s Q test, and the included SNPs showed heterogeneity in the results (Q value 72.858, p = 0.024) (Table 5). Despite the observed heterogeneity (Q value 72.858, p = 0.024, Table 5), the stability of the MR findings remains robust, supported by applying an IVW analysis within a random-effects model that accounts for this variability. In addition, the “leave one out” confirmed the robustness of our results, demonstrating that no individual SNP disproportionately influenced the causal estimates, proving that the effect used to evaluate causality is not dependent on any single genetic instrument variable to drive the results, indicating that the results were reliable (Figure 7).
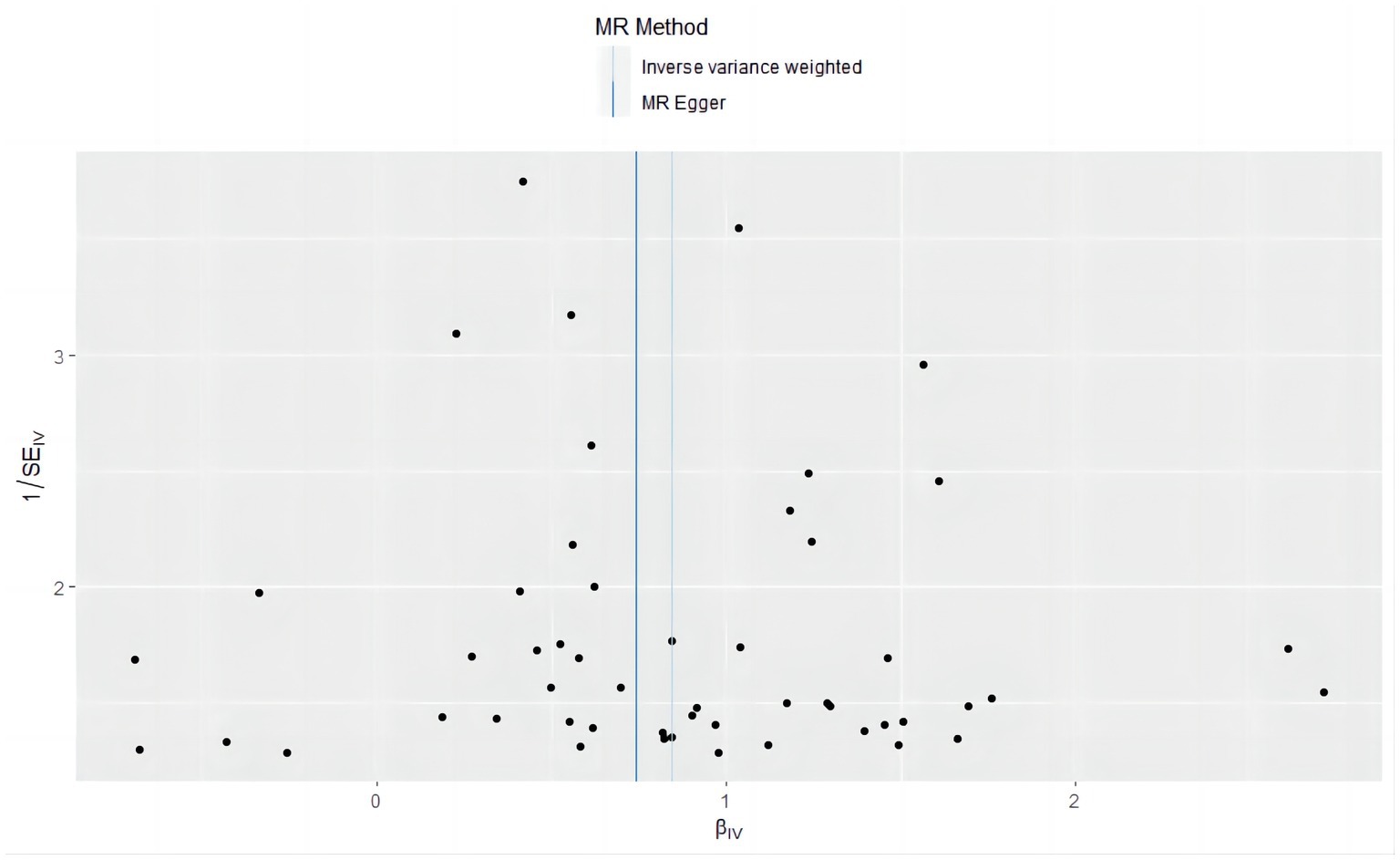
Figure 6. Funnel plot of causal effects in a Mendelian randomization study of asthma as an exposure factor versus frailty as an outcome factor.
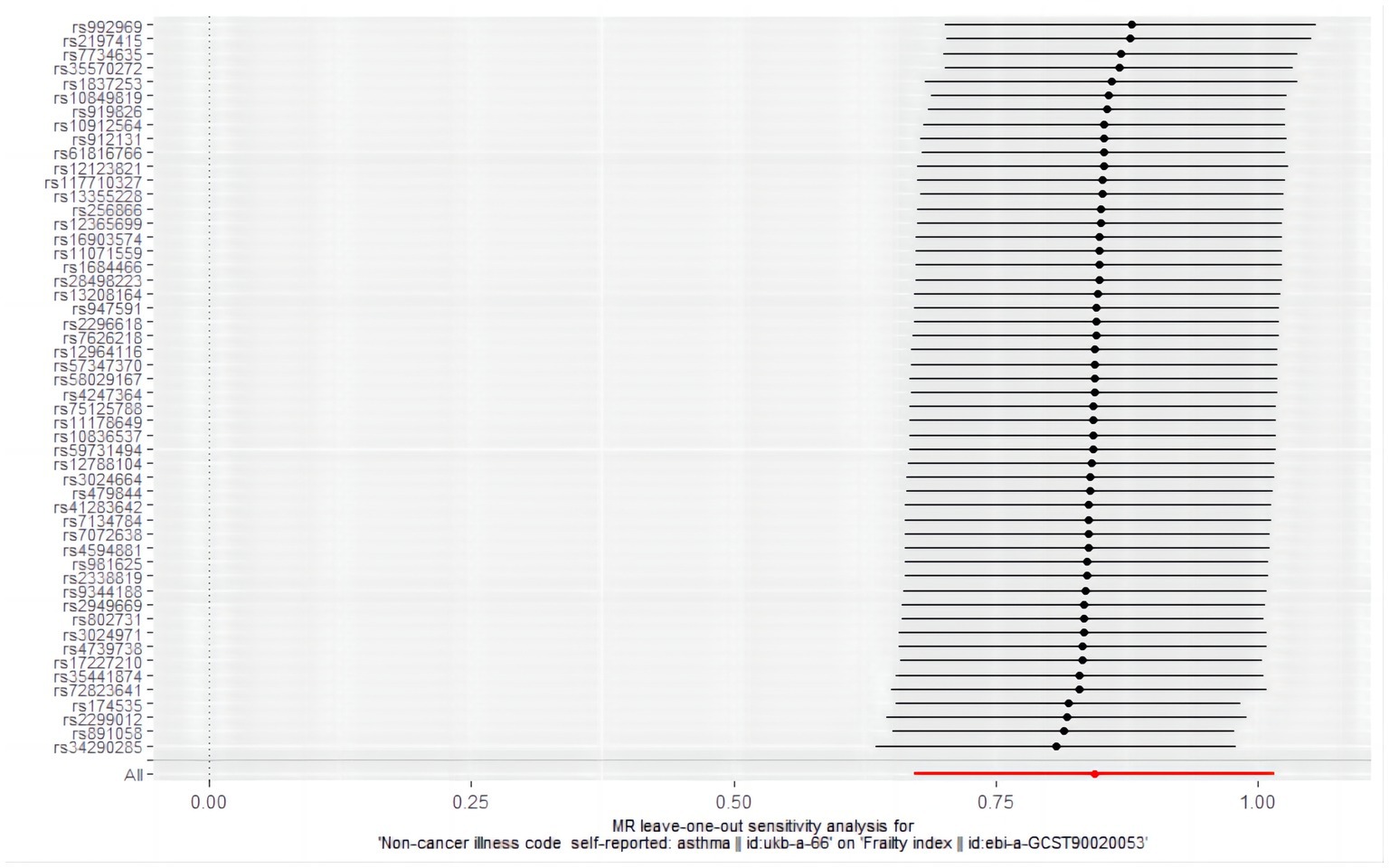
Figure 7. Results of sensitivity analysis of “leave-one-out” in a Mendelian randomized study of asthma-induced frailty.
In the MR analysis with frailty as the exposure factor, the p value of the Mr-Egger intercept was 0.173. The included SNPs were detected by Mr-PRESSO (p = 0.223), so there was no level of pleiotropy. Cochran’s Q test showed no heterogeneity between the two diseases (Q value 16.681, p = 0.118) (Table 6).
3.4 Risk factor analysis
MR analysis was used to further investigate the causal relationship between asthma and the common risk factors, including BMI, Vitamin D, Triglycerides, Smoking, and physical activity for frailty. Table 7 and Figure 8 show a negative causal association between the genetic susceptibility to asthma with physical activity (OR = 0.866, 95% CI: 0.788–0.953; p = 0.003) and asthma resulted in a significant reduction in physical activity endurance (Figure 9). Overall, the risk factor analysis shows that decreased physical activity endurance may be responsible for the increased risk of frailty due to asthma. However, the results of the analysis concluded that genetic susceptibility to asthma was not associated with BMI (OR = 0.960, 95% CI: 0.809–1.138; p = 0.635), Vitamin D (OR = 1.061, 95% CI: 0.927–1.216; p = 0.390), Triglycerides (OR = 0.808, 95% CI: 0.635–1.030; p = 0.085), Smoking (OR = 0.988, 95% CI: 0.867–1.125; p = 0.856).
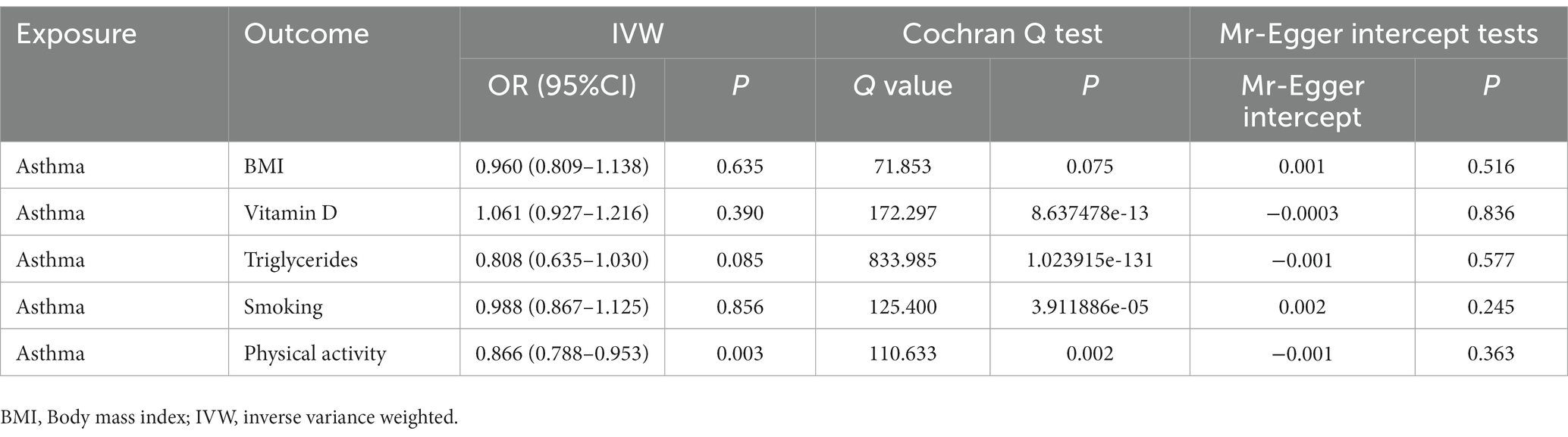
Table 7. Results of the analysis of common risk factors for asthma and frailty.
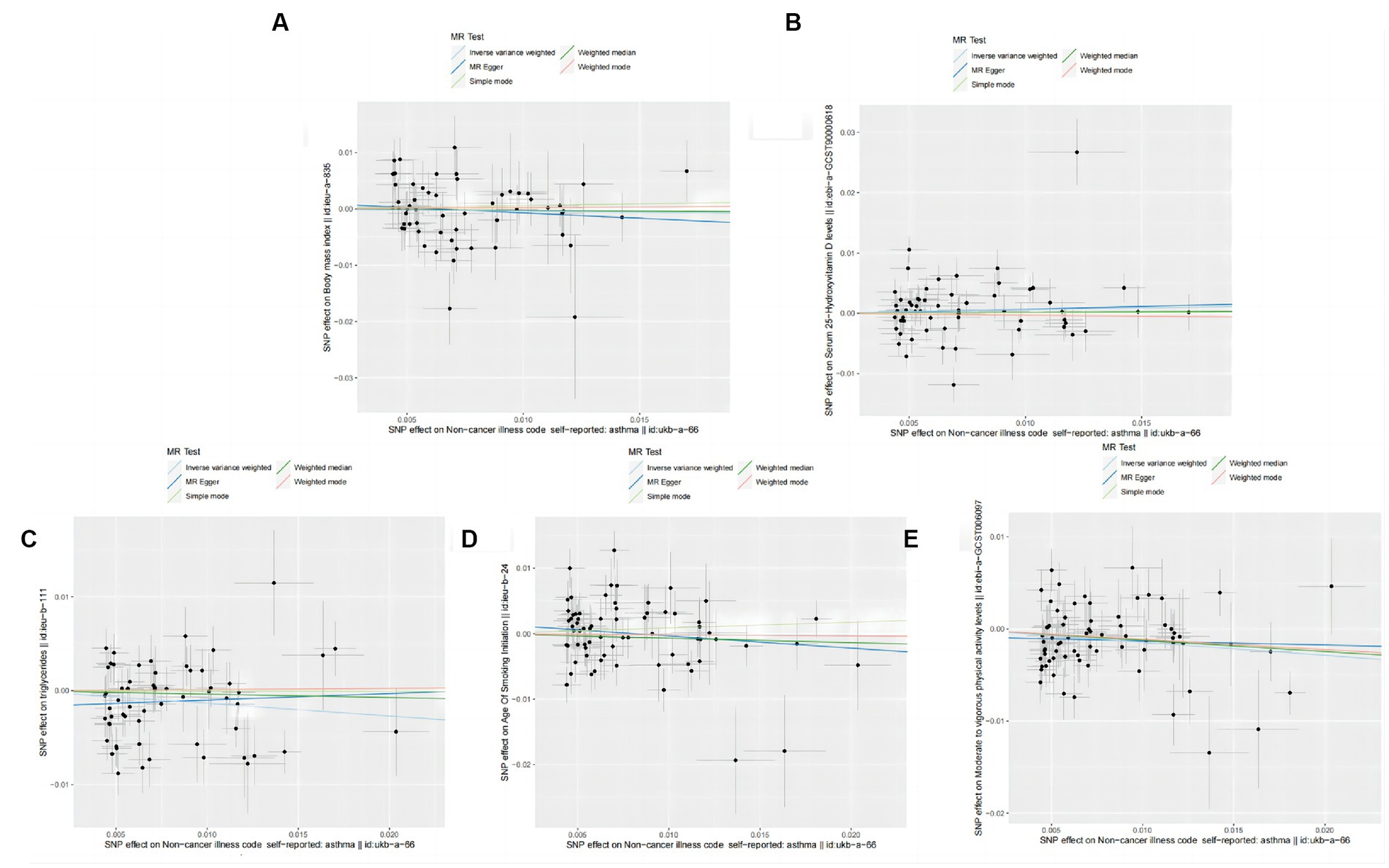
Figure 8. Scatter plot of the causal effect of single nucleotide polymorphisms associated with asthma on risk factors for frailty in the Mendelian randomization study. (A) Forest plot of the causal effect of single nucleotide polymorphisms associated with asthma on BMI. (B) Forest plot of the causal effect of single nucleotide polymorphisms associated with asthma on Vitamin D. (C) Forest plot of the causal effect of single nucleotide polymorphisms associated with asthma on Triglycerides. (D) Forest plot of the causal effect of single nucleotide polymorphisms associated with asthma on Smoking. (E) Forest plot of the causal effect of single nucleotide polymorphisms associated with asthma on physical activity.
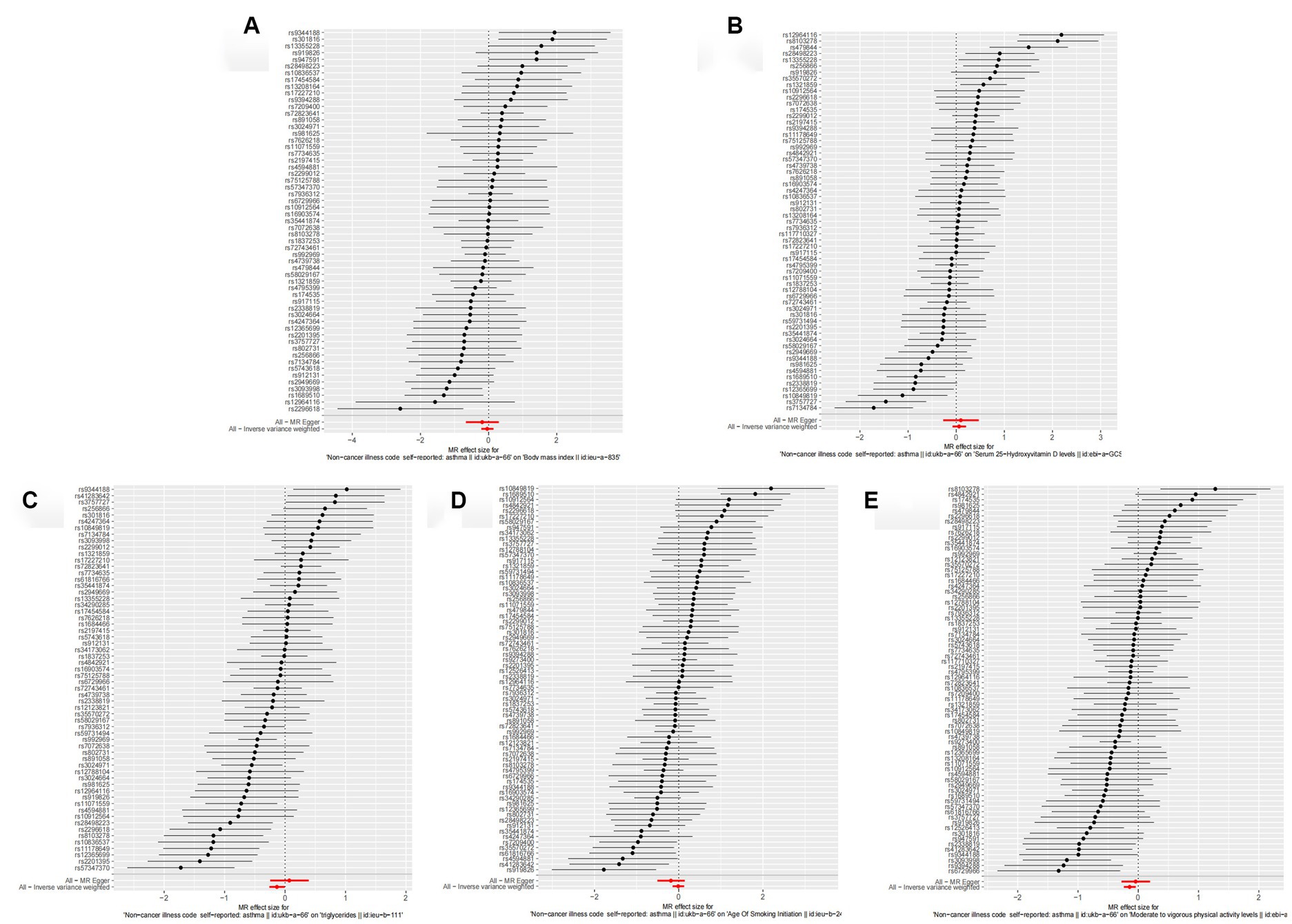
Figure 9. Forest plot of the causal effect of single nucleotide polymorphisms associated with asthma on risk factors for frailty. Mendelian randomization estimated the effect size and the data are expressed as effect values with 95% CI. The significance of the red line is the Mr-Egger test and the MR results of the IVW method. (A) Scatter plot of the causal effect of single nucleotide polymorphisms associated with asthma on BMI. (B) Scatter plot of the causal effect of single nucleotide polymorphisms associated with asthma on Vitamin D. (C) Scatter plot of the causal effect of single nucleotide polymorphisms associated with asthma on Triglycerides. (D) Scatter plot of the causal effect of single nucleotide polymorphisms associated with asthma on Smoking. (E) Scatter plot of the causal effect of single nucleotide polymorphisms associated with asthma on Smoking physical activity.
4 Discussion
The rapid rise in the prevalence of asthma and frailty has led to an increasing overlap between patients with asthma and those with frailty (41). The quality of life of many such patients is severely affected by these comorbid conditions, necessitating a clearer understanding of their causal relationship to improve prevention and treatment strategies. The results of observational studies in clinical research can easily be confounded by factors that are difficult to control, resulting in a lack of established causality. Randomization in randomized controlled trials (RCTs) avoids confounding and minimizes selection bias, representing the highest level of evidence, yet RCTs are also constrained by practical limitations. First, RCTs are financially costly and time-consuming, particularly for rare outcomes or conditions requiring long-term follow-up. Second, RCTs may not always yield therapies that selectively affect the intended risk factors, and crucially, random assignment of many risk factors is often not feasible due to practical or ethical constraints (42). MR offers a time-and cost-effective alternative for uncovering causal relationships (43). This bidirectional two-sample MR analysis utilized datasets from the GWAS database and employed multiple methods to examine the possible causal relationship between asthma and frailty systematically. Our observations indicate a significant association between genetic susceptibility to asthma and frailty, with reverse MR analysis supporting a causal link from frailty to genetic predisposition for asthma. To our knowledge, this is the first study to apply an MR framework to ascertain a causal link between asthma and frailty.
Asthma ranks as the second most prevalent chronic respiratory disease in the older adults, following COPD, and is also the second leading cause of death from chronic respiratory conditions (44). Scant observational clinical studies addressed asthma and frailty, yet our findings concur with these earlier studies (10). In an observational clinical study from Japan (45), 37% of the 203 older adults asthmatic patients (60 years or older) attending an outpatient clinic had comorbid conditions. Another cross-sectional study analyzing 34,403 eligible participants (aged ≥40 years) from the 1999–2018 National Health and Nutrition Examination Survey cycles found a 32.3% prevalence of concurrent asthma and frailty (46). This study identified an increased risk of frailty among patients with asthma, which may be partly ascribed to the inherent disease characteristics of asthma. Since asthma involves chronic airway inflammation, the airway epithelium acts as both a mediator and target, leading to airway remodeling and obstruction (47). Furthermore, the chronic inflammation observed in asthmatic patients is present in the respiratory tract and also manifests as systemic inflammation. Inflammation causes the increase in the levels of peripheral blood eosinophils, total blood IgE, and type 2 cytokines by regulating growth factors and increasing catabolism (48). Frailty is a state of diminished physiological reserves with a manifestation of aging in an aging population. Aging alters the immune response, leading to a chronic proinflammatory state and increased susceptibility to airway infection (49). As epigenetics change, airway epithelial dysfunction and inflammatory cytokine activity are more pronounced in immunosenescent, older patients with asthma, who are at higher risk for poor clinical outcomes (50). Thus, chronic systemic inflammation may be an important cause of frailty in older adults with asthma. This study also explored potential risk factors associated with the combined presence of asthma and frailty, such as BMI, vitamin D levels, triglycerides, smoking habits, and physical activity. It was found that decreased physical activity endurance may play a moderating role (Table 6), consistent with several observational studies (51), which reported that physical activity levels are negatively correlated with asthma severity. Since decreased physical activity endurance is a recognized cause of frailty, physical activity may play a key intermediate role in the asthma-frailty pathway.
To summarize, frailty, as a multi-comorbid and chronic disease, places a heavy burden on patients and their families and poses challenges to health systems worldwide. For patients with established asthma, attention should be paid to the changes in their ability to perform physical activity, adopt a more rigorous assessment method, formulate appropriate public health prevention strategies, and reduce asthma patients’ frailty burden to prevent asthma patients from becoming weaker and disabled.
Reverse MR analysis confirmed a possible causal relationship between frailty and asthma, suggesting that these conditions may share similar pathophysiological mechanisms. Definitions of frailty are often associated with aging and chronic disease, strongly influencing health and function in later life (52). Frail older adults may experience swallowing dysfunction, increasing the risk of aspiration and choking, potentially leading to respiratory disease. However, the complex interplay regulating asthma in frail patients is not fully understood, and only some research has been published in this area over the past few years. A cross-sectional clinical study (12) is underway in patients over 60 to assess the multidimensional relationship between frailty phenotypes and asthma. In another cross-sectional study from South Korea (53), the researchers examined frailty-related diseases among the older adults in the community. They found a close relationship between frailty and hypertension, diabetes, arthritis, asthma, and other diseases. It is necessary to study the mechanism of frailty and asthma further to identify, manage, and prevent the occurrence and development of asthma and achieve healthy aging.
However, this study also had some limitations. First, it was based on European populations, and whether there are genetic differences among other ethnic groups, countries, and regions cannot be determined. Second, this study only analyzed the relationship between asthma and frailty. The absence of comprehensive clinical information precluded further subgroup analyses on pre-frailty and frailty, thereby limiting the ability to delineate their precise causal relationships. Third is the limitation of GWAS data; more SNPs are needed as variable tools to repeat MR research, improve test efficiency, and present more data to explore potential mechanisms and provide practical means of preventing and treating frailty.
5 Conclusion
This investigation, employing a bidirectional two-sample MR approach, has established a causal link between asthma and frailty. Therefore, it is imperative to enhance the assessment and management of frailty among patients with asthma to mitigate the incidence of adverse outcomes. Furthermore, this research contributes novel insights into the investigation and prevention of frailty in the context of asthma and proposes viable evaluation methodologies for forthcoming studies, thereby facilitating the early identification, diagnosis, and management of these conditions.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: this study is based on the IEU Open GWAS project website summary data sample repository (https://gwas.mrcieu.ac.uk/), which are derived from publicly available studies. Ethical approval was obtained for all origin studies. The frailty dataset was obtained from https://gwas.mrcieu.ac.uk/datasets/ebi-a-GCST90020053. The Asthma dataset was obtained from https://gwas.mrcieu.ac.uk/datasets/ukb-a-66/.
Ethics statement
This study was analyzed using the publicly available GWAS pooled dataset, and in accordance with legal and institutional requirements, human participant studies do not require ethical review and approval nor written informed consent.
Author contributions
XM: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Software, Validation, Writing – original draft, Writing – review & editing. HX: Investigation, Software, Writing – review & editing. JX: Data curation, Investigation, Methodology, Writing – review & editing. LZ: Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. MS: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. ZL: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Resources, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Natural Science Foundation of China (U20A20398) and Wuhu Hua Tuo Plan for High-level Backbone Talents in Health.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Romaszko-Wojtowicz, A, Cymes, I, Draganska, E, Doboszynska, A, Romaszko, J, and Glinska-Lewczuk, K. Relationship between biometeorological factors and the number of hospitalizations due to asthma. Sci Rep. (2020) 10:9593. doi: 10.1038/s41598-020-66746-8
2. Mims, JW . Asthma: definitions and pathophysiology. Int Forum Allergy Rhinol. (2015) 5:S2–6. doi: 10.1002/alr.21609
3. Fahy, JV . Type 2 inflammation in asthma--present in most, absent in many. Nat Rev Immunol. (2015) 15:57–65. doi: 10.1038/nri3786
4. GBD 2015 Mortality and Causes of Death Collaborators . Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet. (2016) 388:1459–544. doi: 10.1016/S0140-6736(16)31012-1
5. Dunn, RM, Busse, PJ, and Wechsler, ME. Asthma in the elderly and late-onset adult asthma. Allergy. (2018) 73:284–94. doi: 10.1111/all.13258
6. Dent, E, Martin, FC, Bergman, H, Woo, J, Romero-Ortuno, R, and Walston, JD. Management of frailty: opportunities, challenges, and future directions. Lancet. (2019) 394:1376–86. doi: 10.1016/S0140-6736(19)31785-4
7. Cesari, M, Calvani, R, and Marzetti, E. Frailty in older persons. Clin Geriatr Med. (2017) 33:293–303. doi: 10.1016/j.cger.2017.02.002
8. Park, C, and Ko, FC. The science of frailty: sex differences. Clin Geriatr Med. (2021) 37:625–38. doi: 10.1016/j.cger.2021.05.008
9. Landre, B, Nadif, R, Goldberg, M, Gourmelen, J, Zins, M, Ankri, J, et al. Asthma is associated with frailty among community-dwelling adults: the GAZEL cohort. BMJ open. Respir Res. (2020) 7:e000526. doi: 10.1136/bmjresp-2019-000526
10. Kusunose, M, Sanda, R, Mori, M, Narita, A, and Nishimura, K. Are frailty and patient-reported outcomes independent in subjects with asthma? A cross-sectional observational study. Clin Respir J. (2021) 15:216–24. doi: 10.1111/crj.13287
11. Zeng, XZ, Meng, LB, Jia, N, Shi, J, Zhang, C, Li, YY, et al. Epidemiological status and associated factors of frailty and pre-frailty in older adults with asthma in China: a national cross-sectional study. Front Public Health. (2023) 11:1136135. doi: 10.3389/fpubh.2023.1136135
12. Figueiredo, RG, Pinheiro, GP, Arata, V, Leal, MFM, Santana, CVN, Tiraboschi, TL, et al. Impact of frailty in elderly patients with moderate to severe asthma. PLoS One. (2022) 17:e0270921. doi: 10.1371/journal.pone.0270921
13. Maners, J, Gill, D, Pankratz, N, Laffan, MA, Wolberg, AS, de Maat, MPM, et al. A Mendelian randomization of gamma' and total fibrinogen levels in relation to venous thromboembolism and ischemic stroke. Blood. (2020) 136:3062–9. doi: 10.1182/blood.2019004781
14. Bowden, J, and Holmes, MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. (2019) 10:486–96. doi: 10.1002/jrsm.1346
15. Smith, GD, and Ebrahim, S. 'Mendelian randomization': can genetic epidemiology contribute to understanding environmental determinants of disease? Int J Epidemiol. (2003) 32:1–22. doi: 10.1093/ije/dyg070
16. Sekula, P, Del Greco, MF, Pattaro, C, and Kottgen, A. Mendelian randomization as an approach to assess causality using observational data. J Am Soc Nephrol. (2016) 27:3253–65. doi: 10.1681/ASN.2016010098
17. Ahn, K, Penn, RB, Rattan, S, Panettieri, RA Jr, Voight, BF, and An, SS. Mendelian randomization analysis reveals a complex genetic interplay among atopic dermatitis, asthma, and gastroesophageal reflux disease. Am J Respir Crit Care Med. (2023) 207:130–7. doi: 10.1164/rccm.202205-0951OC
18. Freuer, D, Linseisen, J, and Meisinger, C. Asthma and the risk of gastrointestinal disorders: a Mendelian randomization study. BMC Med. (2022) 20:82. doi: 10.1186/s12916-022-02283-7
19. Stern, J, Pier, J, and Litonjua, AA. Asthma epidemiology and risk factors. Semin Immunopathol. (2020) 42:5–15. doi: 10.1007/s00281-020-00785-1
20. Wang, X, Hu, J, and Wu, D. Risk factors for frailty in older adults. Medicine. (2022) 101:e30169. doi: 10.1097/MD.0000000000030169
21. Yuan, L, Chang, M, and Wang, J. Abdominal obesity, body mass index and the risk of frailty in community-dwelling older adults: a systematic review and meta-analysis. Age Ageing. (2021) 50:1118–28. doi: 10.1093/ageing/afab039
22. Emdin, CA, Khera, AV, and Kathiresan, S. Mendelian Randomization. JAMA. (2017) 318:1925–6. doi: 10.1001/jama.2017.17219
23. Skrivankova, VW, Richmond, RC, Woolf, BAR, Yarmolinsky, J, Davies, NM, Swanson, SA, et al. Strengthening the reporting of observational studies in epidemiology using Mendelian randomization: the STROBE-MR statement. JAMA. (2021) 326:1614–21. doi: 10.1001/jama.2021.18236
24. Yang, W, Yang, Y, He, L, Zhang, M, Sun, S, Wang, F, et al. Dietary factors and risk for asthma: a Mendelian randomization analysis. Front Immunol. (2023) 14:1126457. doi: 10.3389/fimmu.2023.1126457
25. Zhu, X, Huang, S, Kang, W, Chen, P, and Liu, J. Associations between polyunsaturated fatty acid concentrations and Parkinson's disease: a two-sample Mendelian randomization study. Front Aging Neurosci. (2023) 15:1123239. doi: 10.3389/fnagi.2023.1123239
26. Burgess, S, and Thompson, SG, CRP CHD Genetics Collaboration. Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. (2011) 40:755–64. doi: 10.1093/ije/dyr036
27. Bottigliengo, D, Foco, L, Seibler, P, Klein, C, Konig, IR, and Del Greco, MF. A Mendelian randomization study investigating the causal role of inflammation on Parkinson's disease. Brain. (2022) 145:3444–53. doi: 10.1093/brain/awac193
28. Zhou, J, Lin, J, and Zheng, Y. Association of cardiovascular risk factors and lifestyle behaviors with aortic aneurysm: a Mendelian randomization study. Front Genet. (2022) 13:925874. doi: 10.3389/fgene.2022.925874
29. Tao, H, Fan, S, Zhu, T, You, L, Zheng, D, Yan, L, et al. Psychiatric disorders and type 2 diabetes mellitus: a bidirectional Mendelian randomization. Eur J Clin Investig. (2023) 53:e13893. doi: 10.1111/eci.13893
30. Burgess, S, and Thompson, SG. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. (2017) 32:377–89. doi: 10.1007/s10654-017-0255-x
31. Liu, K, Zou, J, Fan, H, Hu, H, and You, Z. Causal effects of gut microbiota on diabetic retinopathy: a Mendelian randomization study. Front Immunol. (2022) 13:930318. doi: 10.3389/fimmu.2022.930318
32. Li, P, Wang, H, Guo, L, Gou, X, Chen, G, Lin, D, et al. Association between gut microbiota and preeclampsia-eclampsia: a two-sample Mendelian randomization study. BMC Med. (2022) 20:443. doi: 10.1186/s12916-022-02657-x
33. Wu, F, Huang, Y, Hu, J, and Shao, Z. Mendelian randomization study of inflammatory bowel disease and bone mineral density. BMC Med. (2020) 18:312. doi: 10.1186/s12916-020-01778-5
34. Chen, X, Hong, X, Gao, W, Luo, S, Cai, J, Liu, G, et al. Causal relationship between physical activity, leisure sedentary behaviors and COVID-19 risk: a Mendelian randomization study. J Transl Med. (2022) 20:216. doi: 10.1186/s12967-022-03407-6
35. Locke, AE, Kahali, B, Berndt, SI, Justice, AE, Pers, TH, Day, FR, et al. Genetic studies of body mass index yield new insights for obesity biology. Nature. (2015) 518:197–206. doi: 10.1038/nature14177
36. Revez, JA, Lin, T, Qiao, Z, Xue, A, Holtz, Y, Zhu, Z, et al. Genome-wide association study identifies 143 loci associated with 25 hydroxyvitamin D concentration. Nat Commun. (2020) 11:1647. doi: 10.1038/s41467-020-15421-7
37. Richardson, TG, Sanderson, E, Palmer, TM, Ala-Korpela, M, Ference, BA, Davey Smith, G, et al. Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: a multivariable Mendelian randomisation analysis. PLoS Med. (2020) 17:e1003062. doi: 10.1371/journal.pmed.1003062
38. Liu, M, Jiang, Y, Wedow, R, Li, Y, Brazel, DM, Chen, F, et al. Association studies of up to 1.2 million individuals yield new insights into the genetic etiology of tobacco and alcohol use. Nat Genet. (2019) 51:237–44. doi: 10.1038/s41588-018-0307-5
39. Klimentidis, YC, Raichlen, DA, Bea, J, Garcia, DO, Wineinger, NE, Mandarino, LJ, et al. Genome-wide association study of habitual physical activity in over 377,000 UK Biobank participants identifies multiple variants including CADM2 and APOE. Int J Obes. (2018) 42:1161–76. doi: 10.1038/s41366-018-0120-3
40. Symvoulakis, EK, Kamekis, A, Drakonaki, E, Mastrodemou, S, Ryerson, CJ, and Antoniou, K. Frailty and chronic respiratory disease: the need for a multidisciplinary care model. Sarcoidosis Vasc Diffuse Lung Dis. (2021) 38:e2021031. doi: 10.36141/svdld.v38i3.11599
41. Chen, X, Zhang, Z, Yang, H, Qiu, P, Wang, H, Wang, F, et al. Consumption of ultra-processed foods and health outcomes: a systematic review of epidemiological studies. Nutr J. (2020) 19:86. doi: 10.1186/s12937-020-00604-1
42. Chatburn, RL . Basics of study design: practical considerations (from the "biostatistics and epidemiology lecture series, part 1"). Cleve Clin J Med. (2017) 84:e10–9. doi: 10.3949/ccjm.84.s2.03
43. Plotnikov, D, and Guggenheim, JA. Mendelian randomisation and the goal of inferring causation from observational studies in the vision sciences. Ophthalmic Physiol Opt. (2019) 39:11–25. doi: 10.1111/opo.12596
44. GBD Chronic Respiratory Disease Collaborators . Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. (2020) 8:585–96. doi: 10.1016/S2213-2600(20)30105-3
45. Ryu, K, Fukutomi, Y, Nakatani, E, Iwata, M, Nagayama, K, Yano, K, et al. Frailty and muscle weakness in elderly patients with asthma and their association with cumulative lifetime oral corticosteroid exposure. Allergol Int. (2023) 72:252–61. doi: 10.1016/j.alit.2022.10.005
46. Wang, X, Wen, J, Gu, S, Zhang, L, and Qi, X. Frailty in asthma-COPD overlap: a cross-sectional study of association and risk factors in the NHANES database. BMJ Open Respir Res. (2023) 10:e001713. doi: 10.1136/bmjresp-2023-001713
47. Banno, A, Reddy, AT, Lakshmi, SP, and Reddy, RC. Bidirectional interaction of airway epithelial remodeling and inflammation in asthma. Clin Sci. (2020) 134:1063–79. doi: 10.1042/CS20191309
48. Andrea, M, Susanna, B, Francesca, N, Enrico, M, and Alessandra, V. The emerging role of type 2 inflammation in asthma. Expert Rev Clin Immunol. (2021) 17:63–71. doi: 10.1080/1744666X.2020.1860755
49. Ebersole, JL, Graves, CL, Gonzalez, OA, Dawson, D 3rd, Morford, LA, Huja, PE, et al. Aging, inflammation, immunity and periodontal disease. Periodontol. (2016) 72:54–75. doi: 10.1111/prd.12135
50. Nanda, A, Baptist, AP, Divekar, R, Parikh, N, Seggev, JS, Yusin, JS, et al. Asthma in the older adult. J Asthma. (2020) 57:241–52. doi: 10.1080/02770903.2019.1565828
51. Ding, S, and Zhong, C. Exercise and asthma. Adv Exp Med Biol. (2020) 1228:369–80. doi: 10.1007/978-981-15-1792-1_25
52. Zazzara, MB, Vetrano, DL, Carfi, A, and Onder, G. Frailty and chronic disease. Panminerva Med. (2019) 61:486–92. doi: 10.23736/S0031-0808.19.03731-5
Keywords: asthma, frailty, Mendelian randomization analysis, causality, SNP, risk factor
Citation: Ma X, Xu H, Xie J, Zhang L, Shi M and Li Z (2023) The causal relationship between risk of developing bronchial asthma and frailty: a bidirectional two-sample Mendelian randomization study. Front. Med. 10:1289026. doi: 10.3389/fmed.2023.1289026
Edited by:
Clara Bonanad Lozano, Hospital Clínico Universitario de Valencia, SpainReviewed by:
Jose Francisco Parodi, University of San Martín de Porres, PeruBao-ping Tian, Zhejiang University School of Medicine, China
Copyright © 2023 Ma, Xu, Xie, Zhang, Shi and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zegeng Li, lizegeng6609@163.com