 Linghuan Wang
Linghuan Wang Binqi Li
Binqi Li He Zhao1
He Zhao1 Yiming Mu
Yiming Mu- 1Medicine School of Nankai University, Tianjin, China
- 2Department of Endocrinology, Chinese People’s Liberation Army (PLA) General Hospital, Beijing, China
Objectives: To perform a systematic review and meta-analysis of interferon and endocrine side effects, including their incidence, evaluation, and management.
Methods: PubMed was searched through March 7th, 2021, by 2 authors independently (LH Wang and H Zhao). Early phase I/II, phase III experimental trials, prospective and retrospective observational studies were included. Stata 16.0 (StataCorp LLC, 16.0) was the main statistical software for meta-analysis. The weighted incidence and risk ratio were estimated for primary thyroid disease and diabetes mellitus.
Results: A total of 108 studies involving 46265 patients were included. Hypothyroidism was the most common thyroid disorder, followed by hyperthyroidism. IFN α+RBV treated patients experienced hypothyroidism in 7.8% (95%CI, 5.9-9.9), which was higher than IFN α (5.2%; 95%CI, 3.7-6.8) and IFN β (7.0%; 95%CI, 0.06-23.92). IFN α+RBV treated patients experienced hyperthyroidism in 5.0% (95%CI, 3.6-6.5), which was higher than IFN α (3.5%; 95%CI, 2.5-4.8) and IFN β (3.4%; 95%CI, 0.9-7.5). The summary estimated incidence of painless thyroiditis was 5.8% (95%CI, 2.8-9.8) for IFN α, and 3.5% (95%CI,1.9-5.5) for IFN α+RBV. The summary estimated incidence of diabetes was 1.4% (95%CI, 0.3-3.1) for IFN, 0.55% (95%CI, 0.05-1.57) for IFN α, 3.3% (95%CI,1.1-6.6) for IFN α+RBV.
Conclusions: Our meta-analysis shows a high incidence of endocrine adverse events provoked by IFN, further reinforced by combined RBV treatment.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42022334131.
Introduction
Interferon (IFN) is a broad-spectrum antiviral agent that activates cell surface receptors and causes cells to produce antiviral proteins, thereby inhibiting viral replication and interferon use has long been associated with endocrine-related adverse events (1). About 0.1 to 1% of patients suffered severe and even life-threatening side effects, including thyroid, visual, hearing, kidney, and heart damage, and pulmonary interstitial fibrosis (2, 3), in which, thyroid disorders have been reported in up to 20% of the patients during IFN-based therapies (4). Besides, cases of diabetes mellitus associated with interferon have also been reported. The present study aims to perform a systematic review and meta-analysis of interferon and endocrine side effects, including their incidence, evaluation, and management.
Materials and methods
Study registration
The review has been registered with the International Prospective Systems Review Registry (PROSPERO ID: CRD42022334131).
Literature search
Two independent authors (LH Wang and H Zhao) searched PubMed database for relevant articles on the subject of endocrinopathies and interferon until March 7th, 2021. Search terms were included for the various endocrinopathies, adverse events, interferon, IFN, hypothyroidism, hyperthyroidism, thyroiditis, hypophysitis, primary adrenal insufficiency, diabetes, Graves’ disease, primary thyroid disease, thyroid dysfunction, secondary hypogonadotropic hypogonadism, primary hypoparathyroidism, primary hypoparathyroidism. Combine these terms with the Boolean logic operator AND/OR.
Study selection
Study design types included early phase I/II, phase III experimental trials, prospective, and retrospective observational studies. The subjects were adults treated with interferon. Studies of interferon combined with radiotherapy, cellular vaccines, small molecule inhibitors, immune checkpoint inhibitors (ICI), or interleukin-2 therapy regimen were excluded. The language was limited to English or Chinese. A preliminary selection of manuscripts was made by title and abstract. Then, studies that did not report adverse endocrine events or had inadequate data were excluded by reading the full text. In addition, duplicate studies were excluded. If there was any disagreement, it would be discussed by all authors and resolved by consensus.
Data analysis and extraction
Each included study included the following elements: author and year of publication, study design, median follow-up time, therapy, dosing of drug administration, endocrine adverse events (hypothyroidism, hyperthyroidism, thyroiditis, and diabetes mellitus). Supplementary data and appendices were also methodically explored if available.
Outcome
The outcome was the occurrence of endocrine adverse events (such as hypothyroidism, hyperthyroidism, and diabetes mellitus).
Definition of hypothyroidism, hyperthyroidism, painless thyroiditis and diabetes
Hypothyroidism was defined as an elevated TSH with a decreased fT4 and/or fT3 level. Hyperthyroidism was defined as a suppressed TSH with an elevated fT4 and/or fT3 level. Painless thyroiditis was defined as hyperthyroidism or hypothyroidism secondary to thyrotoxicosis, with negative TRAb, reduced or absent uptake of technetium scan tracer, and/or increased 18 fluorodeoxyglucose uptake of positron emission tomography (18FDG-PET) tracer (5). Thyroid biopsy was a better way to diagnose painless thyroiditis but it was invasive. Therefore, PET was used to help diagnose painless thyroiditis. Diabetes was defined as FBG ≥ 7.0 mmol/L, and/or PBG ≥ 11.1 mmol/L.
Statistical analysis
Stata 16.0 (StataCorp LLC, 16.0) was the main statistical software for meta-analysis. A meta-analysis of incidence estimates was performed using an inverse sine transformation method to weigh the studies. Summary estimates of incidence were reported with a 95% confidence interval (CI). For randomized controlled trials, relative risk and 95% CI were calculated using the number of adverse events observed and the number of patients who did not experience an adverse event in each group. In addition, we conducted a combination of the relative risks from individual trials for the same adverse event in a meta-analysis. Heterogeneity was assessed using the Q and I² statistics. Where there was significant statistical heterogeneity, we reported risk ratios (RRs) using the random-effects model. For other outcomes, we used the fixed-effect model. P<0.05 was considered statistically significant.
Results
Study characteristics
Our search identified a total of 1074 articles, of which 898 were excluded based on title and abstract. Of the 176 full texts that were reviewed, 108 were finally included (Figure 1) (2, 6–89). These included 1 phase I, 6 phase III randomized trials, 75 prospective, and 26 retrospective studies. A total of 119 study arms were identified. The main diseases were chronic hepatitis C (CHC) (82/119, 68.9%), chronic hepatitis B (CHB) (13/119, 10.9%), CHB+CHC (2/119, 1.7%), chronic hepatitis D (2/119, 1.7%), multiple sclerosis (7/119, 5.9%), malignant tumor (9/119, 7.6%) and blood disease (4/119, 3.4%). A total of 46265 patients were analyzed (IFN α, n=21344; IFN β, n=1625; IFN α+RBV, n=11937; placebo, n=10204). The regimens were classified as monotherapy with IFN α (70/119, 58.8%), IFN β (7/119, 5.9%), and IFN α+RBV (43/119, 36.1%).
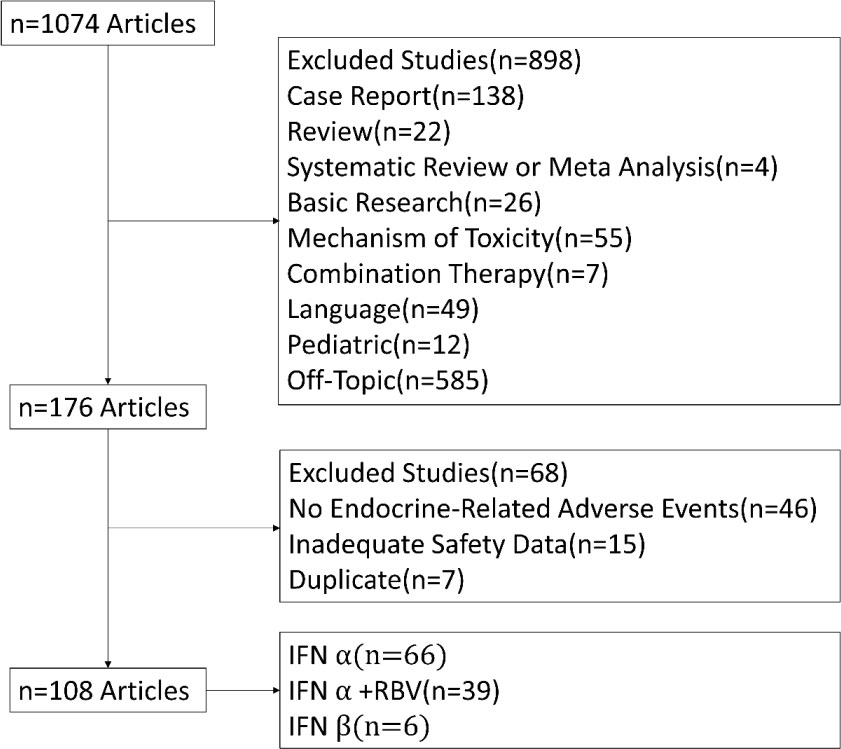
Figure 1 Flow chart of study selection.
Incidence of endocrine adverse events
The summary estimated incidence of endocrine adverse events was 9.1% (95%CI, 8.7-10.7) for IFN, 8.3% (95%CI, 6.4-10.4) for IFN α, 8.3% (95%CI,2.9-16.2) for IFN β, 12.7% (95%CI,10-15.7) for IFN α+RBV (Table 1).
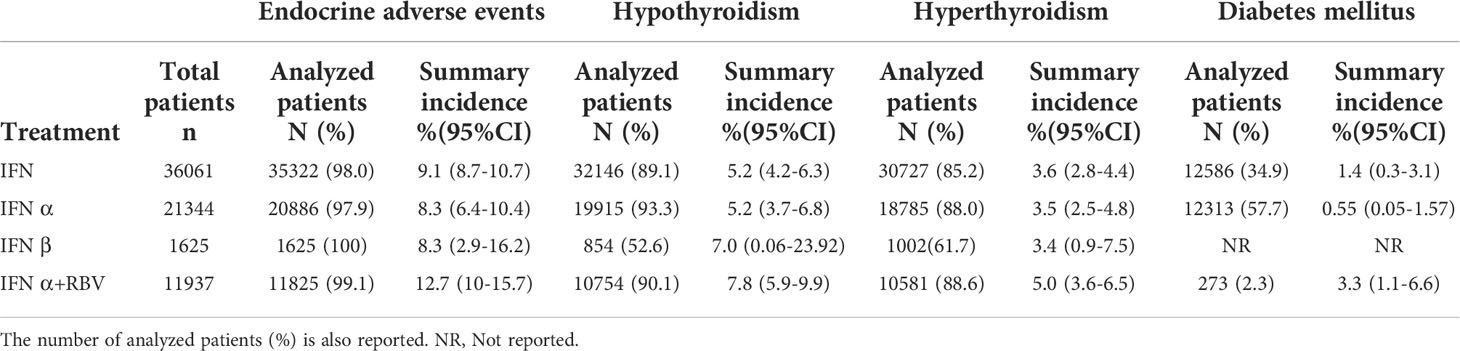
Table 1 Summary estimated incidence of endocrine adverse events on interferon.
Incidence of hypothyroidism
Hypothyroidism was the most common thyroid disorder. The summary estimated incidence of hypothyroidism was 5.2% (95%CI, 4.2-6.3) for IFN, 5.2% (95%CI, 3.7-6.8) for IFN α, 7.0% (95%CI,0.06-23.92) for IFN β, 7.8% (95%CI,5.9-9.9) for IFN α+RBV. Compared to placebo, the risk of hypothyroidism was significantly increased by IFN (RR, 1.999; 95% CI, 1.043–3.831; p =0.037). However, there was no difference between IFN α (RR, 2.634; 95% CI, 0.559–11.588; p >0.05)/IFN α+RBV (RR, 1.861; 95% CI, 0.647–5.350; p >0.05) and placebo (Tables 1, 2).

Table 2 Summary of relative risk for endocrine adverse events.
Incidence of hyperthyroidism
Predictions for hyperthyroidism were lower with a combined incidence of 3.6% (95%CI, 2.8-4.4) for IFN, 3.5% (95%CI, 2.5-4.8) for IFN α, 3.4% (95%CI, 0.9-7.5) for IFN β, 5.0% (95%CI, 3.6-6.5) for IFN α+RBV. Compared to placebo, the risk of hyperthyroidism was significantly increased by IFN (RR, 2.329; 95% CI, 1.667–3.253; p <0.001). The IFN α+RBV (RR, 2.319; 95% CI, 1.647–3.266; p < 0.001) had a high risk of hyperthyroidism compared to the placebo. However, there was no difference between IFN α (RR, 2.145; 95% CI, 0.348–13.216; p >0.05) and placebo (Tables 1, 2).
Incidence of painless thyroiditis
The summary estimated incidence of painless thyroiditis was 3.7% (95%CI, 2.3-5.3) for IFN, 5.8% (95%CI, 2.8-9.8) for IFN α, 3.5% (95%CI, 1.9-5.5) for IFN α+RBV. Compared to placebo, the risk of painless thyroiditis was significantly increased by IFN (RR, 1.854; 95% CI, 1.270–2.707; p=0.001). The IFN α+RBV (RR, 1.875; 95% CI, 1.281–2.745; p = 0.001) had a high risk of painless thyroiditis compared to the placebo. Patients with painless thyroiditis can be detected both in the phase of hyperthyroidism or hypothyroidism, further complicating correct reporting. It was not appropriate to put painless thyroiditis and other endocrine adverse events in one table. Therefore, painless thyroiditis was analyzed separately (Tables S1, S2).
Incidence of diabetes mellitus
The summary estimated incidence of diabetes mellitus was 1.4% (95%CI, 0.3-3.1) for IFN, 0.55% (95%CI, 0.05-1.57) for IFN α, 3.3% (95%CI,1.1-6.6) for IFN α+RBV. Further analysis was not possible due to the rarity of interferon-associated diabetes (Table 1).
Discussion
Our meta-analysis shows a high incidence of endocrine adverse events related to interferon therapy, which is further enhanced by combined therapy. Hypothyroidism is the most common thyroid disorder, followed by hyperthyroidism. The highest incidence of hypothyroidism on monotherapy is noted on IFN β. The incidence of hyperthyroidism during monotherapy is higher for IFN α. Diabetes mellitus are less frequent, with no cases of diabetes mellitus reported on IFN β therapy. IFN α+RBV shows a remarkably higher incidence of hypothyroidism, hyperthyroidism, and diabetes mellitus. However, IFN α+RBV shows a lower incidence of painless thyroiditis than IFN α.
Thyroid dysfunction
Interferon is a broad-spectrum antiviral drug, which is widely used in the treatment of viral hepatitis and neoplastic diseases. Interferon therapy is closely associated with the occurrence of thyroid dysfunction (TD).
The reported incidence of interferon-associated thyroid dysfunction ranged from 2.5% to 34.3% (9, 14–16, 18, 76, 90, 91, 40, 69, 92–94). In addition, the incidence of interferon-associated TD was correlated with the duration of treatment. Cumulative incidence increased with the duration of interferon therapy, with 6.6%, 10.1%, and 11.5% cumulative incidence at 3, 6, and 12 months after initiation of interferon treatment, respectively (69).
Different treatments had different effects on the incidence of thyroid dysfunction. The incidence of thyroid dysfunction during IFN α combined with RBV was reported to be 4.7 to 27.8% (14–16, 93, 95). The incidence of thyroid dysfunction during INF α monotherapy was 2.5%.-34.3% (14, 40, 94). Besides, studies found that patients treated with interferon α and ribavirin had a higher mean incidence of TD (12.1%) than patients treated with interferon α alone (6.6%) (96).
The incidence of hypothyroidism, hyperthyroidism, and thyroiditis during interferon-α therapy was 4.2 - 6.4%, 1.0 - 5.1%, and 1.7 - 3.4% respectively (14, 69). Previous studies have shown varying timing of onset of thyroid dysfunction during interferon therapy. The mean time to onset of thyroid dysfunction after interferon treatment was 5-6 months (14, 69), among which, the average onset time of hypothyroidism was 5.1 weeks to 6 months (3, 14), the average onset time of hyperthyroidism was 6.8 weeks to 4 months (3, 14), and the average onset time of thyroiditis was 18 weeks to 4 months (3, 14).
However, the long-term outcome of these patients who suffered interferon-associated thyroid dysfunction remains unknown. Most prospective studies were limited to 6 months after the end of IFN α therapy (92). Most TD patients presented with subclinical thyroid disease, which spontaneously recovered after interferon treatment, and only a few patients had persistent symptoms that required medication (3, 14, 69, 95). However, Vasiliadis et al. reported that 57.69% of patients displayed permanent thyroid disease (22). Besides, thyroid disease may even persist in some patients, requiring long-term treatment (18, 23, 94).
The incidence of IFN α associated with TD also differed significantly between countries. In two studies of adult subjects, Brazil had the lowest incidence and Poland had the highest (25, 97).
In our study, the proportion of hypothyroidism was higher than that of hyperthyroidism, as in most studies (9, 14, 22, 92). Contrary to our results, a study in southern Taiwan found that hyperthyroidism was most common in interferon alpha-based therapy (23).
So why are there differences in the incidence of interferon-associated TD reported by different studies? First, difference in genetic susceptibility was one of the leading factors of TD incidence variability. Studies showed that Asian ethnicity was an independent risk factor for IFN-associated TD development, with a higher incidence than other ethnic groups (27, 76). Second, iodine status also played an important role in TD variation. A diet high in iodine was prone to hypothyroidism, and a diet high in iodine was prone to hyperthyroidism. Third, different definitions of TD may overestimate or underestimate the true prevalence of TD.
IFN caused disorders of the immune system, and it had a direct toxic effect on thyroid cells. IFN induced cytotoxicity by upregulating perforin expression in peripheral natural killer cells and T cells, especially T helper cells (Th). It suppressed Th2 and enhanced Th1 immune response (91). Besides, interferon also activated lymphocytes and made cytokine and thyroid antibody production increase (91). IFN directly disrupted the thyroid. IFN inhibited hormone production, secretion, and metabolism, and lead to abnormal expression of major histocompatibility antigens on thyroid cells (29, 98). In addition to IFN α, ribavirin also had immunomodulatory effects on the thyroid (99). What’s more, HCV itself also induced thyroid autoantibodies (100, 101).
Previous studies showed that gender was an independent factor in predicting the occurrence of TD, and females had an increased risk for the development of IFN associated TD (9, 18, 23, 27, 76, 102). We believed that the hormonal status of women was one of the reasons why women were more susceptible to IFN-α related TD than men. The immune reactivity of females was higher than that of males, and sex hormones affected the occurrence and severity of immune-mediated pathological states. In addition, studies found that pretreatment of TPOAb was an independent factor associated with TD occurrence, and patients with positive pretreatment of TPOAb had a higher risk of TD occurrence (22, 35, 36, 38, 76). What’s more, ATA positive rate also predict TD (35, 40). Studies showed that HCV patients with positive ATA had an 80% chance of developing TD during or after interferon therapy. The prevalence of ATA in patients with hepatitis C was significantly higher than that in healthy people (22, 35, 90, 101, 103).
Diabetes mellitus
Interferon-related diabetes was also a major endocrine adverse event. Although the incidence was not high, the presentation was usually severe and irreversible, with fulminant diabetes and ketoacidosis (104, 105). In one of our previous reviews, we found that interferon therapy shortened the incubation period of T2DM, turning the original T2DM into T1DM (106). The onset of interferon-associated type 1 diabetes [0.50 (0.55) years] required longer periods of IFN treatment than interferon-associated type 2 diabetes [0.19 (0.28) years] (106). The incidence of T1DM in hepatitis C patients treated with interferon was 10-18 times that of the general population (2, 43, 104). It was worth noting that interferon-induced diabetes may be accompanied by the occurrence of autoimmune thyroid disease or changes in immune indicators (107–117).
IFN was significantly overexpressed in islet cells of T1DM patients (118–120). Interferon may contribute to diabetes in several ways. First, IFN α lead to apoptosis by activating oligosadenosine synthase-ribonuclease L and protein kinase R pathways (121). Second, Interferon-alpha increased membrane known major histocompatibility complexIclass antigen expression and activated T cells and natural killer cells causingβ-cell injury (122). Third, Th1 multiactivity induced by IFN α therapy enhanced the autoimmune response to β cells and accelerated the destruction of β cells (123). Compared with non-peg-IFN, patients receiving the combination of peg-IFN and ribavirin had a shorter time to develop IFN-induced T1DM (124). The incidence of diabetes mellitus was higher for IFN α+RBV than for IFN α in our study. Ribavirin was a guanosine analog that had an immune effect on TH1-like activation (125), which further enhanced the autoimmune response to interferon. On the one hand, Th1 cytokines expressed Fas antigen on the surface of β cells and induced T-cell mediated apoptosis (68, 126). On the other hand, as a Th1 cytokine, IFN γ directly damaged β cells by synergistic action with TFN α (127).
Other endocrine events
Few data are available on thyroid cancer and gonadal function during interferon therapy. In one prospective review, one interferon-alpha-treated patient was identified with papillary thyroid carcinoma (71). Besides, a prospective study of interferon therapy for hepatitis from China reported a case of gonadal dysfunction.
Precision medicine and future directions
Interferon can also cause other autoimmune diseases, including optic neuromyelitis (128), Sjogren’s syndrome (114), severe insulin resistance against insulin receptor antibodies (109, 113), and stiff-man syndrome, in addition to causing endocrine adverse events. However, unlike targeted therapies (129), reports of interferon-related adverse events toward the skin and mucous manifestations were rare. Some interferon-associated adverse endocrine events were severe and irreversible, such as type 1 diabetes and stiff-man syndrome. Therefore, it was necessary to strengthen the monitoring of high risk factors (e.g., thyroid related antibodies, diabetes related antibodies, other autoimmune antibodies) during interferon therapy. Aggressive treatment was also necessary for interferon-associated endocrine adverse events to avoid more serious consequences.
Currently, the main treatment drugs for chronic viral hepatitis include nucleoside/nucleotide analogue (NUC) drugs and immune stimulants such as interferon α (IFN α) or PEG-IFN α. However, more advanced treatments such as gene therapy, targeted immune therapy (130) and modern vaccination are now emerging rapidly (131). In addition, precision medicine is picking up pace. Pharmacogenomics Studies such as Human Genome Project, genome-wide association studies (GWAS) and other pharmacogenomics studies (132), Next-Generation Gene Sequencing and Mass Spectrometric Studies (133) are the main content of precision medicine. In addition, the design and creation of advanced diagnostic tools and nanomedicine Precision Therapy (PTAs) maximizes the detection, treatment and monitoring of chronic viral hepatitis (134, 135).
Study design and limitations
This is a comprehensive analysis of endocrine adverse events on interferon. Because adverse events are often underestimated in randomized clinical trials, our meta-analysis includes retrospective, prospective studies, and randomized clinical trials. Differences in the definition of thyroid disease such as hypothyroidism, hyperthyroidism, and thyroiditis in each study may lead to differences in its incidence. Besides, subclinical thyroid disease has been reported as an adverse event in some studies and not in others, which may have a great impact on morbidity. In addition, our analysis was conducted at the study level and did not include data from individual patients. Human error can’t be excluded in the screening of included studies. Finally, the trial will be excluded if endocrine adverse events are not reported, which may overestimate our final results.
Conclusions
Thyroid diseases are frequent endocrine adverse events triggered by interferon, and hypothyroidism is most common. Combined ribavirin shows a remarkably higher incidence. Besides, interferon-related diabetes is also a major endocrine adverse event. Although the incidence is not high, the presentation is usually severe. Therefore, clinically, a high suspicion of adverse endocrine events is necessary. Timely diagnosis and treatment of adverse endocrine events can avoid life-threatening complications. Precision medicine will be an advanced treatment for chronic viral hepatitis.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Author contributions
LW performed the statistical analysis and interpreted the data, drafted and revised the manuscript. LW, KC, and YM contributed to design the conception of the manuscript. BL, HZ, PW, QW, KC, and YM revised the manuscript. Every author contributed in the final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
Funding resources was provided by the Beijing Municipal Science & Technology Commission (Project No. D141107005314004) and the Beijing Municipal Science & Technology Commission (Project No.Z201100005520014).
Acknowledgments
We thank Professor Yiming Mu and Professor Kang Chen for their direction on this analysis.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2022.949003/full#supplementary-material
References
1. Russo M, Fried M. Side effects of therapy for chronic hepatitis c. Gastroenterology (2003) 124(6):1711–9. doi: 10.1016/S0016-5085(03)00394-9
2. Fattovich G, Giustina G, Favarato S, Ruol A. A survey of adverse events in 11,241 patients with chronic viral hepatitis treated with alfa interferon. J Hepatol (1996) 24(1):38–47. doi: 10.1016/S0168-8278(96)80184-X
3. Tran HA, Malcolm Reeves GE, Gibson R, Attia JR. Development of thyroid diseases in the treatment of chronic hepatitis c with alpha-interferon may be a good prognosticator in achieving a sustained virological response: a meta-analysis. J Gastroenterol Hepatol (2009) 24(7):1163–8. doi: 10.1111/j.1440-1746.2009.05874.x
4. Manns M, Wedemeyer H, Cornberg M. Treating viral hepatitis c: efficacy, side effects, and complications. Gut (2006) 55(9):1350–9. doi: 10.1136/gut.2005.076646
5. de Filette J, Andreescu C, Cools F, Bravenboer B, Velkeniers B. A systematic review and meta-analysis of endocrine-related adverse events associated with immune checkpoint inhibitors. Hormone Metab Res (2019) 51(3):145–56. doi: 10.1055/a-0843-3366
6. Abdel-Kader ME, Azmy MK, Hassan MA, Ahmad YK, El-Dahshan T, Houssein MA. Thyroid function in patients with chronic hepatitis c virus infection under interferon therapy. J Egyptian Soc Parasitol (2012) 42(3):761–8. doi: 10.12816/0006360
7. Amenomori M, Mori T, Fukuda Y, Sugawa H, Nishida N, Furukawa M, et al. Incidence and characteristics of thyroid dysfunction following interferon therapy in patients with chronic hepatitis c. Internal Med (Tokyo Japan) (1998) 37(3):246–52. doi: 10.2169/internalmedicine.37.246
8. Andrade LJ, Atta AM, Atta ML, Mangabeira CN, Parana R. Thyroid disorders in patients with chronic hepatitis c using interferon-alpha and ribavirin therapy. Braz J Infect Dis (2011) 15(4):377–81. doi: 10.1590/S1413-86702011000400013
9. Kee KM, Lee CM, Wang JH, Tung HD, Changchien CS, Lu SN, et al. Thyroid dysfunction in patients with chronic hepatitis c receiving a combined therapy of interferon and ribavirin: incidence, associated factors and prognosis. J Gastroenterol Hepatol (2006) 21(Pt 2):319–26. doi: 10.1111/j.1440-1746.2005.03947.x
10. Benaiges D, Garcia-Retortillo M, Mas A, Canete N, Broquetas T, Puigvehi M, et al. Clinical value of thyrotropin receptor antibodies for the differential diagnosis of interferon induced thyroiditis. Exp Clin Endocrinol Diabetes (2016) 124(1):39–44. doi: 10.1055/s-0035-1565071
11. Burman P, Totterman TH, Oberg K, Karlsson FA. Thyroid autoimmunity in patients on long term therapy with leukocyte-derived interferon. J Clin Endocrinol Metab (1986) 63(5):1086–90. doi: 10.1210/jcem-63-5-1086
12. Caraccio N, Dardano A, Manfredonia F, Manca L, Pasquali L, Iudice A, et al. Long-term follow-up of 106 multiple sclerosis patients undergoing interferon-beta 1a or 1b therapy: predictive factors of thyroid disease development and duration. J Clin Endocrinol Metab (2005) 90(7):4133–7. doi: 10.1210/jc.2004-2326
13. Chang YK, Tseng YT, Chen KH, Chen KT. Long-term outcomes and risk factors of thyroid dysfunction during pegylated interferon and ribavirin treatment in patients with chronic hepatitis c infection in Taiwan. BMC Endocrine Disord (2019) 19(1):36. doi: 10.1186/s12902-019-0362-7
14. Kabbaj N, Guedira MM, El Atmani H, El Alaoui M, Mohammadi M, Benabed K, et al. Thyroid disorders during interferon alpha therapy in 625 patients with chronic hepatitis c: a prospective cohort study. Annales d'endocrinologie (2006) 67(4):343–7. doi: 10.1016/S0003-4266(06)72609-9
15. Baudin E, Marcellin P, Pouteau M, Colas-Linhart N, Le Floch JP, Lemmonier C, et al. Reversibility of thyroid dysfunction induced by recombinant alpha interferon in chronic hepatitis c. Clin Endocrinol (1993) 39(6):657–61. doi: 10.1111/j.1365-2265.1993.tb02423.x
16. Marazuela M, Garcia-Buey L, Gonzalez-Fernandez B, Garcia-Monzon C, Arranz A, Borque MJ, et al. Thyroid autoimmune disorders in patients with chronic hepatitis c before and during interferon-alpha therapy. Clin Endocrinol (1996) 44(6):635–42. doi: 10.1046/j.1365-2265.1996.751768.x
17. Custro N, Montalto G, Scafidi V, Soresi M, Gallo S, Tripi S, et al. Prospective study on thyroid autoimmunity and dysfunction related to chronic hepatitis c and interferon therapy. J Endocrinol Invest (1997) 20(7):374–80. doi: 10.1007/BF03347987
18. Dalgard O, Bjoro K, Hellum K, Myrvang B, Bjoro T, Haug E, et al. Thyroid dysfunction during treatment of chronic hepatitis c with interferon alpha: no association with either interferon dosage or efficacy of therapy. J Internal Med (2002) 251(5):400–6. doi: 10.1046/j.1365-2796.2002.00974.x
19. Danilovic DL, Mendes-Correa MC, Chammas MC, Zambrini H, Marui S. Thyroid hormonal disturbances related to treatment of hepatitis c with interferon-alpha and ribavirin. Clinics (Sao Paulo Brazil) (2011) 66(10):1757–63. doi: 10.1590/S1807-59322011001000014
20. Deutsch M, Dourakis S, Manesis EK, Gioustozi A, Hess G, Horsch A, et al. Thyroid abnormalities in chronic viral hepatitis and their relationship to interferon alfa therapy. Hepatol (Baltimore Md) (1997) 26(1):206–10. doi: 10.1002/hep.510260127
21. Durelli L, Bongioanni MR, Ferrero B, Imperiale D, Verdun E, Oggero A, et al. Long term recombinant interferon alpha treatment in MS with special emphasis to side effects. Multiple Sclerosis (Houndmills Basingstoke England) (1996) 1(6):366–71. doi: 10.1177/135245859600100617
22. Vasiliadis T, Anagnostis P, Nalmpantidis G, Soufleris K, Patsiaoura K, Grammatikos N, et al. Thyroid dysfunction and long-term outcome during and after interferon-alpha therapy in patients with chronic hepatitis c. Ann Acad Med Singapore (2011) 40(9):394–400.
23. Hsieh MC, Yu ML, Chuang WL, Shin SJ, Dai CY, Chen SC, et al. Virologic factors related to interferon-alpha-induced thyroid dysfunction in patients with chronic hepatitis c. Eur J Endocrinol (2000) 142(5):431–7. doi: 10.1530/eje.0.1420431
24. Durelli L, Ferrero B, Oggero A, Verdun E, Ghezzi A, Montanari E, et al. Liver and thyroid function and autoimmunity during interferon-beta 1b treatment for MS. Neurology (2001) 57(8):1363–70. doi: 10.1212/WNL.57.8.1363
25. Parana R, Cruz M, Santos-Jesus R, Ferreira K, Codes L, Cruz T. Thyroid disease in HCV carriers undergoing antiviral therapy with interferon plus ribavirin. Braz J Infect Dis (2000) 4(6):284–90.
26. Fentiman IS, Balkwill FR, Thomas BS, Russell MJ, Todd I, Bottazzo GF. An autoimmune aetiology for hypothyroidism following interferon therapy for breast cancer. Eur J Cancer Clin Oncol (1988) 24(8):1299–303. doi: 10.1016/0277-5379(88)90219-2
27. Jamil KM, Leedman PJ, Kontorinis N, Tarquinio L, Nazareth S, McInerney M, et al. Interferon-induced thyroid dysfunction in chronic hepatitis c. J Gastroenterol Hepatol (2009) 24(6):1017–23. doi: 10.1111/j.1440-1746.2008.05690.x
28. Friedrich-Rust M, Theobald J, Zeuzem S, Bojunga J. Thyroid function and changes in ultrasound morphology during antiviral therapy with pegylated interferon and ribavirin in patients with chronic hepatitis c. J Viral Hepatitis (2009) 16(3):168–77. doi: 10.1111/j.1365-2893.2008.01059.x
29. Roti E, Minelli R, Giuberti T, Marchelli S, Schianchi C, Gardini E, et al. Multiple changes in thyroid function in patients with chronic active HCV hepatitis treated with recombinant interferon-alpha. Am J Med (1996) 101(5):482–7. doi: 10.1016/S0002-9343(96)00259-8
30. Frisullo G, Calabrese M, Tortorella C, Paolicelli D, Ragonese P, Annovazzi P, et al. Thyroid autoimmunity and dysfunction in multiple sclerosis patients during long-term treatment with interferon beta or glatiramer acetate: an Italian multicenter study. Multiple Sclerosis (Houndmills Basingstoke England) (2014) 20(9):1265–8. doi: 10.1177/1352458514521311
31. Gisslinger H, Gilly B, Woloszczuk W, Mayr WR, Havelec L, Linkesch W, et al. Thyroid autoimmunity and hypothyroidism during long-term treatment with recombinant interferon-alpha. Clin Exp Immunol (1992) 90(3):363–7. doi: 10.1111/j.1365-2249.1992.tb05852.x
32. Goldberg JS, Vargas M, Rosmarin AS, Milowsky MI, Papanicoloau N, Gudas LJ, et al. Phase I trial of interferon alpha2b and liposome-encapsulated all-trans retinoic acid in the treatment of patients with advanced renal cell carcinoma. Cancer (2002) 95(6):1220–7. doi: 10.1002/cncr.10809
33. Goyal G, Panag K, Garg R. Prevalence of thyroid disorders in hepatitis c virus positive patients on interferon and antiviral therapy. Int J Appl basic Med Res (2016) 6(4):245–8. doi: 10.4103/2229-516X.192587
34. Hameed MA, Mehmood A, Farooq MA, Tayyab GUN, Haq Toor IU. Hypothyroidism in hepatitis c patients on pegylated interferon therapy. J Ayub Med College Abbottabad JAMC (2016) 28(4):706–8.
35. Huang JF, Chuang WL, Dai CY, Chen SC, Lin ZY, Lee LP, et al. The role of thyroid autoantibodies in the development of thyroid dysfunction in Taiwanese chronic hepatitis c patients with interferon-alpha and ribavirin combination therapy. J Viral Hepatitis (2006) 13(6):396–401. doi: 10.1111/j.1365-2893.2005.00705.x
36. Carella C, Mazziotti G, Morisco F, Manganella G, Rotondi M, Tuccillo C, et al. Long-term outcome of interferon-alpha-induced thyroid autoimmunity and prognostic influence of thyroid autoantibody pattern at the end of treatment. J Clin Endocrinol Metab (2001) 86(5):1925–9. doi: 10.1210/jcem.86.5.7459
37. Hamza I, Eid Y, El-Sayed M, Marzaban R, Abdul-Kareem S. Thyroid dysfunction in chronic hepatitis c patients treated with the combined pegylated interferon-ribavirin therapy. J Interferon Cytokine Res (2016) 36(9):527–33. doi: 10.1089/jir.2016.0007
38. Gelu-Simeon M, Burlaud A, Young J, Pelletier G, Buffet C. Evolution and predictive factors of thyroid disorder due to interferon alpha in the treatment of hepatitis c. World J Gastroenterol (2009) 15(3):328–33. doi: 10.3748/wjg.15.328
39. Hass HG, Klein R, Nehls O, Kaiser S. Thyroid disorders and occurrence of nonorgan-specific autoantibodies (NOSA) in patients with chronic hepatitis c before and during antiviral induction therapy with consensus interferon (interferon alfacon-1). J Clin Gastroenterol (2009) 43(5):470–6. doi: 10.1097/MCG.0b013e318184a470
40. Bini EJ, Mehandru S. Incidence of thyroid dysfunction during interferon alfa-2b and ribavirin therapy in men with chronic hepatitis c: a prospective cohort study. Arch Internal Med (2004) 164(21):2371–6. doi: 10.1001/archinte.164.21.2371
41. Kalkner KM, Ronnblom L, Karlsson Parra AK, Bengtsson M, Olsson Y, Oberg K. Antibodies against double-stranded DNA and development of polymyositis during treatment with interferon. QJM monthly J Assoc Phys (1998) 91(6):393–9. doi: 10.1093/qjmed/91.6.393
42. Lisker-Melman M, Di Bisceglie AM, Usala SJ, Weintraub B, Murray LM, Hoofnagle JH. Development of thyroid disease during therapy of chronic viral hepatitis with interferon alfa. Gastroenterology (1992) 102(6):2155–60. doi: 10.1016/0016-5085(92)90348-3
43. Schreuder TC, Gelderblom HC, Weegink CJ, Hamann D, Reesink HW, Devries JH, et al. High incidence of type 1 diabetes mellitus during or shortly after treatment with pegylated interferon alpha for chronic hepatitis c virus infection. Liver Int (2008) 28(1):39–46. doi: 10.1111/j.1478-3231.2007.01610.x
44. Okanoue T, Sakamoto S, Itoh Y, Minami M, Yasui K, Sakamoto M, et al. Side effects of high-dose interferon therapy for chronic hepatitis c. J Hepatol (1996) 25(3):283–91. doi: 10.1016/S0168-8278(96)80113-9
45. Liu Y-H, Wu T, Sun N, Wang G-L, Yuan J-Z, Dai Y-R, et al. Combination therapy with pegylated interferon alpha-2b and adefovir dipivoxil in HBeAg-positive chronic hepatitis b versus interferon alone: a prospective, randomized study. J Huazhong Univ Sci Technol [Medical Sciences] (2014) 34(4):542–47. doi: 10.1007/s11596-014-1312-2
46. Loftis JM, Wall JM, Linardatos E, Benvenga S, Hauser P. A quantitative assessment of depression and thyroid dysfunction secondary to interferon-alpha therapy in patients with hepatitis c. J Endocrinol Invest (2004) 27(7):Rc16–20. doi: 10.1007/BF03347491
47. Obolonczyk L, Siekierska-Hellmann M, Wisniewski P, Lewczuk A, Berendt-Obolonczyk M, Lakomy A, et al. Epidemiology, risk factors and prognosis of interferon alpha induced thyroid disorders. a prospective clinical study. Postepy higieny i medycyny doswiadczalnej (Online) (2017) 71(0):842–9. doi: 10.1111/j.1478-3231.2007.01610.x
48. Mammen JS, Ghazarian SR, Pulkstenis E, Subramanian GM, Rosen A, Ladenson PW. Phenotypes of interferon-alpha-induced thyroid dysfunction among patients treated for hepatitis c are associated with pretreatment serum TSH and female sex. J Clin Endocrinol Metab (2012) 97(9):3270–6. doi: 10.1210/jc.2012-1026
49. Masood N, Ghori R, Memon A, Memon S, Memon KI, Memon I, et al. Frequency of thyroid disorders during interferon and ribavirin therapy in chronic hepatitis c infection. J Coll Phys Surgeons–Pakistan JCPSP (2008) 18(6):347–51. doi: 06.2008/JCPSP.347351
50. Mazziotti G, Sorvillo F, Stornaiuolo G, Rotondi M, Morisco F, Ruberto M, et al. Temporal relationship between the appearance of thyroid autoantibodies and development of destructive thyroiditis in patients undergoing treatment with two different type-1 interferons for HCV-related chronic hepatitis: a prospective study. J Endocrinol Invest (2002) 25(7):624–30. doi: 10.1007/BF03345087
51. Murakami T, Masumoto T, Michitaka K, Horiike N, Hino H, Okada S, et al. Prediction of interferon-alpha-induced thyroid dysfunction in patients with chronic hepatitis c. J Gastroenterol Hepatol (1995) 10(5):528–31. doi: 10.1111/j.1440-1746.1995.tb01342.x
52. Murdolo G, Francisci D, Forini F, Baldelli F, Angeletti G, Stagni G, et al. Expression of endocrine autoantibodies in chronic hepatitis c, before and after interferon-alpha therapy. J Endocrinol Invest (2002) 25(11):938–46. doi: 10.1007/BF03344065
53. Nadeem A, Aslam M. Association of interferon-alpha and ribavirin-induced thyroid dysfunction with severity of disease and response to treatment in pakistani asian patients of chronic hepatitis c. Hepatitis Res Treat (2012) 2012:864315. doi: 10.1155/2012/864315
54. Preziati D, La Rosa L, Covini G, Marcelli R, Rescalli S, Persani L, et al. Autoimmunity and thyroid function in patients with chronic active hepatitis treated with recombinant interferon alpha-2a. Eur J Endocrinol (1995) 132(5):587–93. doi: 10.1530/eje.0.1320587
55. Rahmani M, Toosi MN, Ghannadi K, Lari GR, Jazebi M, Rasoulzadegan M, et al. Clinical outcome of interferon and ribavirin combination treatment in hepatitis c virus infected patients with congenital bleeding disorders in Iran. Haemophilia (2009) 15(5):1097–103. doi: 10.1111/j.1365-2516.2009.02042.x
56. Rotondi M, Oliviero A, Profice P, Mone CM, Biondi B, Del Buono A, et al. Occurrence of thyroid autoimmunity and dysfunction throughout a nine-month follow-up in patients undergoing interferon-beta therapy for multiple sclerosis. J Endocrinol Invest (1998) 21(11):748–52. doi: 10.1007/BF03348040
57. Sacchi S, Kantarjian H, O'Brien S, Cohen PR, Pierce S, Talpaz M. Immune-mediated and unusual complications during interferon alfa therapy in chronic myelogenous leukemia. J Clin Oncol (1995) 13(9):2401–7. doi: 10.1200/JCO.1995.13.9.2401
58. Sachithanandan S, Clarke G, Crowe J, Fielding JF. Interferon-associated thyroid dysfunction in anti-d-related chronic hepatitis c. J Interferon Cytokine Res (1997) 17(7):409–11. doi: 10.1089/jir.1997.17.409
59. Satzger I, Meier A, Schenck F, Kapp A, Hauschild A, Gutzmer R. Autoimmunity as a prognostic factor in melanoma patients treated with adjuvant low-dose interferon alpha. Int J cancer (2007) 121(11):2562–6. doi: 10.1002/ijc.22951
60. Silvestri F, Virgolini L, Mazzolini A, Bertolissi F, Russo D, Fanin R, et al. Development of autoimmune thyroid diseases during long-term treatment of hematological malignancies with alpha-interferons. Haematologica (1994) 79(4):367–70.
61. Tran HA, Jones TL, Ianna EA, Reeves GE. The natural history of interferon-alpha induced thyroiditis in chronic hepatitis c patients: a long term study. Thyroid Res (2011) 4(1):2. doi: 10.1186/1756-6614-4-2
62. Tran HA, Reeves GE, Ianna EA, Leembruggen N. Thyroid function outcomes after pegylated interferon-alpha and ribavirin therapy for chronic hepatitis c. Endocrine practice (2010) 16(6):934–9. doi: 10.4158/EP10036.OR
63. Tsuboi K, Katayama M, Yuasa R, Matoba H, Nagayama T, Ihara F, et al. Interferon-alpha-induced thyroid dysfunction in patients with chronic active hepatitis c: a transient, reversible and self-limited dysfunction. Internal Med (Tokyo Japan) (1998) 37(1):27–31. doi: 10.2169/internalmedicine.37.27
64. Wada M, Kang KB, Kinugasa A, Shintani S, Sawada K, Nishigami T, et al. Does the presence of serum autoantibodies influence the responsiveness to interferon-alpha 2a treatment in chronic hepatitis c? Internal Med (Tokyo Japan) (1997) 36(4):248–54. doi: 10.2169/internalmedicine.36.248
65. Wesche B, Jaeckel E, Trautwein C, Wedemeyer H, Falorni A, Frank H, et al. Induction of autoantibodies to the adrenal cortex and pancreatic islet cells by interferon alpha therapy for chronic hepatitis c. Gut (2001) 48(3):378–83. doi: 10.1136/gut.48.3.378
66. Wong V, Fu AX, George J, Cheung NW. Thyrotoxicosis induced by alpha-interferon therapy in chronic viral hepatitis. Clin Endocrinol (2002) 56(6):793–8. doi: 10.1046/j.1365-2265.2002.01553.x
67. Yuen MF, Ooi CG, Hui CK, Wong WM, Wong BC, Chan AO, et al. A pilot study of transcatheter arterial interferon embolization for patients with hepatocellular carcinoma. Cancer (2003) 97(11):2776–82. doi: 10.1002/cncr.11400
68. Betterle C, Fabris P, Zanchetta R, Pedini B, Tositti G, Bosi E, et al. Autoimmunity against pancreatic islets and other tissues before and after interferon-alpha therapy in patients with hepatitis c virus chronic infection. Diabetes Care (2000) 23(8):1177–81. doi: 10.2337/diacare.23.8.1177
69. Yan Z, Fan K, Fan Y, Wang X, Mao Q, Deng G, et al. Thyroid dysfunction in chinese patients with chronic hepatitis c treated with interferon alpha: incidence, long-term outcome and predictive factors. Hepatitis Monthly (2012) 12(9):e6390. doi: 10.5812/hepatmon.6390
70. Kodama T, Katabami S, Kamijo K, Katanuma A, Yamashita K, Azuma N, et al. Development of transient thyroid disease and reaction during treatment of chronic hepatitis c with interferon. J gastroenterol (1994) 29(3):289–92. doi: 10.1007/BF02358367
71. Benelhadj S, Marcellin P, Castelnau C, Colas-Linhart N, Benhamou JP, Erlinger S, et al. Incidence of dysthyroidism during interferon therapy in chronic hepatitis c. Hormone Res (1997) 48(5):209–14. doi: 10.1159/000185517
72. Kozielewicz D, Zalesna A, Dybowska D. Can pegylated interferon alpha 2a cause development of thyroid disorders in patients with chronic hepatitis b? Expert Opin Drug Safety (2014) 13(8):1009–14. doi: 10.1517/14740338.2014.921156
73. Kozielewicz D, Wietlicka-Piszcz M, Halota W. Long-term outcomes of thyroid dysfunction in patients with chronic hepatitis c treated with pegylated interferon alpha and ribavirin. Przeglad Epidemiologiczny (2017) 71(4):555–69.
74. Tran A, Quaranta JF, Benzaken S, Thiers V, Chau HT, Hastier P, et al. High prevalence of thyroid autoantibodies in a prospective series of patients with chronic hepatitis c before interferon therapy. Hepatol (Baltimore Md) (1993) 18(2):253–7. doi: 10.1002/hep.1840180205
75. Tran HA, Jones TL, Batey RG. The spectrum of thyroid dysfunction in an Australian hepatitis c population treated with combination interferon-alpha2beta and ribavirin. BMC Endocrine Disord (2005) 5:8. doi: 10.1186/1472-6823-5-8
76. Costelloe SJ, Wassef N, Schulz J, Vaghijiani T, Morris C, Whiting S, et al. Thyroid dysfunction in a UK hepatitis c population treated with interferon-alpha and ribavirin combination therapy. Clin Endocrinol (2010) 73(2):249–56. doi: 10.1111/j.1365-2265.2010.03785.x
77. Imagawa A, Itoh N, Hanafusa T, Oda Y, Waguri M, Miyagawa J, et al. Autoimmune endocrine disease induced by recombinant interferon-alpha therapy for chronic active type c hepatitis. J Clin Endocrinol Metab (1995) 80(3):922–6. doi: 10.1210/jcem.80.3.7883851
78. Nadeem A, Aslam M, Khan DA, Hussain T, Khan SA. Effects of combined interferon alpha and ribavirin therapy on thyroid functions in patients with chronic hepatitis c. J Coll Phys Surgeons–Pakistan JCPSP (2009) 19(2):86–9. doi: 10.1210/jcem.80.3.7883851
79. Kakizaki S, Takagi H, Murakami M, Takayama H, Mori M. HLA antigens in patients with interferon-alpha-induced autoimmune thyroid disorders in chronic hepatitis c. J Hepatol (1999) 30(5):794–800. doi: 10.1016/S0168-8278(99)80131-7
80. Robson SC, Brice E, van Rensburg C, Kannemeyer J, Hift RJ, Kirsch RE. Safety and efficacy of interferon alpha-2b following prednisone withdrawal in the treatment of chronic viral hepatitis b. a case-controlled, randomised study. South Afr Med J = Suid-Afrikaanse tydskrif vir geneeskunde (1992) 82(5):317–20.
81. Durelli L, Ferrero B, Oggero A, Verdun E, Bongioanni MR, Gentile E, et al. Autoimmune events during interferon beta-1b treatment for multiple sclerosis. J Neurological Sci (1999) 162(1):74–83. doi: 10.1016/S0022-510X(98)00299-8
82. Kreisler A, de Seze J, Stojkovic T, Delisse B, Combelles M, Verier A, et al. Multiple sclerosis, interferon beta and clinical thyroid dysfunction. Acta Neurologica Scandinavica (2003) 107(2):154–7. doi: 10.1034/j.1600-0404.2003.02009.x
83. Ronnblom LE, Alm GV, Oberg K. Autoimmune phenomena in patients with malignant carcinoid tumors during interferon-alpha treatment. Acta Oncol (Stockholm Sweden) (1991) 30(4):537–40. doi: 10.3109/02841869109092414
84. Tothova E, Stecova N, Kafkova A, Fricova M, Svorcova E. [Occurrence of autoimmune complications in patients with chronic myelocytic leukemia during treatment with interferon alfa]. Vnitrni lekarstvi (2002) 48(5):380–3.
85. Teng ZL, Gong WJ, Zhang SQ, Sun YX, Ma XH. [Clinical observation of hashimoto thyroiditis in patients with chronic hepatitis c undergoing pegylated-interferon alpha-2a and ribavirin combination therapy]. Zhonghua gan zang bing za zhi = Zhonghua ganzangbing zazhi = Chin J Hepatol (2013) 21(2):101–4. doi: 10.3760/cma.j.issn.1007-3418.2013.02.007
86. Zantut-Wittmann DE, Pavan MH, Pavin EJ, Goncales FL Jr. Central hypothyroidism in patients with chronic hepatitis c and relation with interferon-alpha treatment. Endocrine regulations (2011) 45(3):157–61. doi: 10.4149/endo_2011_03_157
87. Rocco A, Gargano S, Provenzano A, Nardone M, De Sanctis GM, Altavilla N, et al. Incidence of autoimmune thyroiditis in interferon-alpha treated and untreated patients with chronic hepatitis c virus infection. Neuro Endocrinol letters (2001) 22(1):39–44. doi: 10.1159/000054622
88. Krupinska J, Wawrzynowicz-Syczewska M, Urbanowicz W, Poblocki J, Syrenicz A. The influence of interferon alpha on the induction of autoimmune thyroiditis in patients treated for chronic viral hepatitis type c. Endokrynologia Polska (2011) 62(6):517–22.
89. Rostaing L, Oksman F, Izopet J, Baron E, Cisterne JM, Hoff M, et al. Serological markers of autoimmunity in renal transplant patients before and after alpha-interferon therapy for chronic hepatitis c. Am J nephrology (1996) 16(6):478–83. doi: 10.1159/000169047
90. Prummel MF, Laurberg P. Interferon-alpha and autoimmune thyroid disease. Thyroid (2003) 13(6):547–51. doi: 10.1089/105072503322238809
91. Carella C, Mazziotti G, Amato G, Braverman L, Roti E. Clinical review 169: Interferon-alpha-related thyroid disease: pathophysiological, epidemiological, and clinical aspects. J Clin Endocrinol Metab (2004) 89(8):3656–61. doi: 10.1210/jc.2004-0627
92. Moncoucy X, Leymarie F, Delemer B, Lévy S, Bernard-Chabert B, Bouché O, et al. Risk factors and long-term course of thyroid dysfunction during antiviral treatments in 221 patients with chronic hepatitis c. Gastroenterologie clinique biologique (2005) 29(4):339–45. doi: 10.1016/S0399-8320(05)80778-X
93. Carella C, Mazziotti G, Morisco F, Rotondi M, Cioffi M, Tuccillo C, et al. The addition of ribavirin to interferon-alpha therapy in patients with hepatitis c virus-related chronic hepatitis does not modify the thyroid autoantibody pattern but increases the risk of developing hypothyroidism. Eur J Endocrinol (2002) 146(6):743–9. doi: 10.1530/eje.0.1460743
94. Morisco F, Mazziotti G, Rotondi M, Tuccillo C, Iasevoli P, Del Buono A, et al. Interferon-related thyroid autoimmunity and long-term clinical outcome of chronic hepatitis c. Digestive Liver Dis (2001) 33(3):247–53. doi: 10.1016/S1590-8658(01)80715-5
95. Hwang Y, Kim W, Kwon S, Yu H, Kim J, Choe W. Incidence of and risk factors for thyroid dysfunction during peginterferon α and ribavirin treatment in patients with chronic hepatitis c. Korean J Internal Med (2015) 30(6):792–800. doi: 10.3904/kjim.2015.30.6.792
96. Koh L, Greenspan F, Yeo P. Interferon-alpha induced thyroid dysfunction: three clinical presentations and a review of the literature. Thyroid (1997) 7(6):891–6. doi: 10.1089/thy.1997.7.891
97. Kryczka W, Brojer E, Kowalska A, Zarebska-Michaluk D. Thyroid gland dysfunctions during antiviral therapy of chronic hepatitis c. Med Sci Monitor Int Med J Exp Clin Res (2001), 221–5.
98. Berris B, Feinman SV. Thyroid dysfunction and liver injury following alpha-interferon treatment of chronic viral hepatitis. Digestive Dis Sci (1991) 36(11):1657–60. doi: 10.1007/BF01296413
99. Snell N. Ribavirin–current status of a broad spectrum antiviral agent. Expert Opin Pharmacother (2001) 2(8):1317–24. doi: 10.1517/14656566.2.8.1317
100. Vezali E, Elefsiniotis I, Mihas C, Konstantinou E, Saroglou G. Thyroid dysfunction in patients with chronic hepatitis c: virus- or therapy-related? J Gastroenterol Hepatol (2009) 24(6):1024–9. doi: 10.1111/j.1440-1746.2009.05812.x
101. Antonelli A, Ferri C, Fallahi P. Hepatitis c: thyroid dysfunction in patients with hepatitis c on IFN-alpha therapy. Nat Rev Gastroenterol Hepatol (2009) 6(11):633–5. doi: 10.1038/nrgastro.2009.168
102. Fernandez-Soto L, Gonzalez A, Escobar-Jimenez F, Vazquez R, Ocete E, Olea N, et al. Increased risk of autoimmune thyroid disease in hepatitis c vs hepatitis b before, during, and after discontinuing interferon therapy. Arch Internal Med (1998) 158(13):1445–8. doi: 10.1001/archinte.158.13.1445
103. Huang M, Tsai S, Huang B, Sheen I, Yeh C, Liaw Y. Prevalence and significance of thyroid autoantibodies in patients with chronic hepatitis c virus infection: a prospective controlled study. Clin Endocrinol (1999) 50(4):503–9. doi: 10.1046/j.1365-2265.1999.00686.x
104. Nakamura K, Kawasaki E, Imagawa A, Awata T, Ikegami H, Uchigata Y, et al. Type 1 diabetes and interferon therapy: A nationwide survey in Japan. Diabetes Care (2011) 34(9):2084–89. doi: 10.2337/dc10-2274
105. Muraishi K, Sasaki Y, Kato T, Inada C, Tajiri Y, Yamada K. Classification and characteristics of interferon-related diabetes mellitus in Japan. Hepatol Res (2011) 41(2):184–8. doi: 10.1111/j.1872-034X.2010.00753.x
106. Wang L, Chen K, Wang M, Lv Z, Gu W, Wang X, et al. Characteristics of interferon-associated diabetes mellitus in past 30 years: A review. Hormone Metab Res = Hormon- und Stoffwechselforschung = Hormones Metabolisme (2022) 54(3):145–52. doi: 10.1055/a-1749-5716
107. Fujioka T, Honda M, Yoshizaki T, Ogawa M, Matsuno H, Shimokawa K, et al. A case of type 1 diabetes onset and recurrence of graves' disease during pegylated interferon-alpha plus ribavirin treatment for chronic hepatitis c. Internal Med (Tokyo Japan) (2010) 49(18):1987–90. doi: 10.2169/internalmedicine.49.3831
108. Kose S, Gozaydin A, Akkoclu G, Ece G. Chronic hepatitis b with type I diabetes mellitus and autoimmune thyroiditis development during interferon alpha therapy. J Infection Developing Countries (2012) 6(4):364–8. doi: 10.3855/jidc.1632
109. Popescu C, Popescu GA, Arama V. Type 1 diabetes mellitus with dual autoimmune mechanism related to pegylated interferon and ribavirin treatment for chronic HCV hepatitis. J Gastrointestinal liver Dis JGLD (2013) 22(1):101–4.
110. Scavone G, Zaccardi F, Manto A, Caputo S, Pitocco D, Ghirlanda G. A case of chronic hepatitis c developing insulin-dependent diabetes, thyroid autoimmunity and stiff-person syndrome as complications of interferon therapy. Diabetes Res Clin Practice (2010) 89(2):e36–8. doi: 10.1016/j.diabres.2010.05.006
111. Soultati AS, Dourakis SP, Alexopoulou A, Deutsch M, Archimandritis AJ. Simultaneous development of diabetic ketoacidosis and hashitoxicosis in a patient treated with pegylated interferon-alpha for chronic hepatitis c. World J Gastroenterol (2007) 13(8):1292–4. doi: 10.3748/wjg.v13.i8.1292
112. Tosone G, Borgia G, Gentile I, Cerini R, Conte MCD, Orlando R, et al. A case of pegylated interferon alpha-related diabetic ketoacidosis: can this complication be avoided? Acta Diabetologica (2007) 44(3):167–69. doi: 10.1007/s00592-007-0259-1
113. Uto H, Matsuoka H, Murata M, Okamoto T, Miyata Y, Hori T, et al. A case of chronic hepatitis c developing insulin-dependent diabetes mellitus associated with various autoantibodies during interferon therapy. Diabetes Res Clin Practice (2000) 49(2-3):101–6. doi: 10.1016/S0168-8227(00)00143-1
114. Yamazaki M, Sato A, Takeda T, Komatsu M. Distinct clinical courses in type 1 diabetes mellitus induced by peg-interferon-alpha treatment for chronic hepatitis c. Internal Med (Tokyo Japan) (2010) 49(5):403–7. doi: 10.2169/internalmedicine.49.2656
115. Yagyu H, Okada K, Sato S, Yamashita Y, Okada N, Osuga J, et al. Pegylated interferon-alpha2b and ribavirin combination therapy induces hashitoxicosis followed by type 1 diabetes mellitus. Diabetes Res Clin Practice (2012) 95(3):e52–4. doi: 10.1016/j.diabres.2011.11.016
116. Zornitzki T, Malnick S, Lysyy L, Knobler H. Interferon therapy in hepatitis c leading to chronic type 1 diabetes. World J Gastroenterol (2015) 21(1):233–9. doi: 10.3748/wjg.v21.i1.233
117. Zheng Y, Wang Z, Xie Z, Dai R, Zhou Z. Fulminant type 1 diabetes caused by peginterferon α-2a therapy in hepatitis c. J Diabetes (2018) 10(5):419–20. doi: 10.1111/1753-0407.12636
118. Huang X, Yuang J, Goddard A, Foulis A, James R, Lernmark A, et al. Interferon expression in the pancreases of patients with type I diabetes. Diabetes (1995) 44(6):658–64. doi: 10.2337/diab.44.6.658
119. Foulis AK, Farquharson MA, Meager A. Immunoreactive alpha-interferon in insulin-secreting beta cells in type 1 diabetes mellitus. Lancet (London England) (1987) 2(8573):1423–7. doi: 10.1016/S0140-6736(87)91128-7
120. Chehadeh W, Weill J, Vantyghem MC, Alm G, Lefebvre J, Wattre P, et al. Increased level of interferon-alpha in blood of patients with insulin-dependent diabetes mellitus: relationship with coxsackievirus b infection. J Infect Dis (2000) 181(6):1929–39. doi: 10.1086/315516
121. Devendra D, Eisenbarth G. Interferon alpha–a potential link in the pathogenesis of viral-induced type 1 diabetes and autoimmunity. Clin Immunol (Orlando Fla) (2004) 111(3):225–33. doi: 10.1016/j.clim.2004.01.008
122. Foulis A, Farquharson M, Hardman R. Aberrant expression of class II major histocompatibility complex molecules by b cells and hyperexpression of class I major histocompatibility complex molecules by insulin containing islets in type 1 (insulin-dependent) diabetes mellitus. Diabetologia (1987) 30(5):333–43. doi: 10.1007/BF00299027
123. Ogawa K, Hige S, Nakanishi M, Yamamoto Y, Chuma M, Nagasaka A, et al. Immunological and mutagenic actions of ribavirin monotherapy preceding combination therapy with interferon for patients with chronic hepatitis c. Antiviral Ther (2009) 14(4):513–22. doi: 10.1177/135965350901400407
124. Ogihara T, Katagiri H, Yamada T, Kudo H, Imai J, Ishigaki Y, et al. Peginterferon (PEG-IFN) plus ribavirin combination therapy, but neither interferon nor PGE-IFN alone, induced type 1 diabetes in a patient with chronic hepatitis c. Internal Med (Tokyo Japan) (2009) 48(16):1387–90. doi: 10.2169/internalmedicine.48.2220
125. McHutchison J, Gordon S, Schiff E, Shiffman M, Lee W, Rustgi V, et al. Interferon alfa-2b alone or in combination with ribavirin as initial treatment for chronic hepatitis c. hepatitis interventional therapy group. New Engl J Med (1998) 339(21):1485–92. doi: 10.1056/NEJM199811193392101
126. Yamada K, Takane-Gyotoku N, Yuan X, Ichikawa F, Inada C, Nonaka K. Mouse islet cell lysis mediated by interleukin-1-induced fas. Diabetologia (1996) 39(11):1306–12. doi: 10.1007/s001250050574
127. Yamada K, Otabe S, Inada C, Takane N, Nonaka K. Nitric oxide and nitric oxide synthase mRNA induction in mouse islet cells by interferon-gamma plus tumor necrosis factor-alpha. Biochem Biophys Res Commun (1993) 197(1):22–7. doi: 10.1006/bbrc.1993.2435
128. Kawazoe T, Araki M, Lin Y, Ogawa M, Okamoto T, Yamamura T, et al. New-onset type 1 diabetes mellitus and anti-aquaporin-4 antibody positive optic neuritis associated with type 1 interferon therapy for chronic hepatitis c. Internal Med (Tokyo Japan) (2012) 51(18):2625–9. doi: 10.2169/internalmedicine.51.7771
129. Damiani G, Manganoni A, Cazzaniga S, Naldi L. Survey of cutaneous adverse reactions to targeted cancer therapies: value of dermatological advice. Giornale italiano di dermatologia e venereologia organo ufficiale Societa italiana di dermatologia e sifilografia (2020) 155(5):658–61. doi: 10.23736/S0392-0488.18.06033-9
130. Seto W, Yuen M. New pharmacological approaches to a functional cure of hepatitis b. Clin Liver Dis (2016) 8(4):83–8. doi: 10.1002/cld.577
131. Duraisamy G, Bhosale D, Lipenská I, Huvarova I, Růžek D, Windisch M, et al. Advanced therapeutics, vaccinations, and precision medicine in the treatment and management of chronic hepatitis b viral infections; where are we and where are we going? Viruses (2020) 12(9):998–1030. doi: 10.3390/v12090998
132. Akcay I, Katrinli S, Ozdil K, Doganay G, Doganay L. Host genetic factors affecting hepatitis b infection outcomes: Insights from genome-wide association studies. World J Gastroenterol (2018) 24(30):3347–60. doi: 10.3748/wjg.v24.i30.3347
133. Albalat A, Husi H, Stalmach A, Schanstra J, Mischak H. Classical MALDI-MS versus CE-based ESI-MS proteomic profiling in urine for clinical applications. Bioanalysis (2014) 6(2):247–66. doi: 10.4155/bio.13.313
134. Wang X, Li Y, Wang H, Fu Q, Peng J, Wang Y, et al. Gold nanorod-based localized surface plasmon resonance biosensor for sensitive detection of hepatitis b virus in buffer, blood serum and plasma. Biosensors Bioelectronics (2010) 26(2):404–10. doi: 10.1016/j.bios.2010.07.121
Keywords: interferon, endocrine adverse events, hypothyroidism, hyperthyroidism, thyroiditis
Citation: Wang L, Li B, Zhao H, Wu P, Wu Q, Chen K and Mu Y (2022) A systematic review and meta-analysis of endocrine-related adverse events associated with interferon. Front. Endocrinol. 13:949003. doi: 10.3389/fendo.2022.949003
Received: 20 May 2022; Accepted: 11 July 2022;
Published: 05 August 2022.
Edited by:
Bernadette Biondi, University of Naples Federico II, ItalyCopyright © 2022 Wang, Li, Zhao, Wu, Wu, Chen and Mu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kang Chen, cycon_ck@yeah.net; Yiming Mu, muyiming@301hospital.com.cn
†These authors have contributed equally to this work and share last authorship