
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research
Journal of Rehabilitation Practices and Research Volume 4 (2023), Article ID: JRPR-146
https://doi.org/10.33790/jrpr1100146Research Article
Transcending Trauma: Treatments’ Caveats, Construal, and Cultural Context
Luis A. Vega1*, Myrren Agabao1, Angelica Franco2, Zeltzin Estrada-Rodriguez1, Fernando Gomez3, Natasha Selene2, Yeunjoo Lee4, Addie Gonzales1, Kayla Wu5, and Andrea S. Niestas6
1 Department of Psychology, California State University, Bakersfield, CA 93311. United States.
2Program in Counseling Psychology, California State University, Bakersfield, CA 93311, United States.
3 Department of Social Work, California State University, Bakersfield, CA 93311. United States.
4 Department of Advanced Educational Studies, California State University, Bakersfield, CA 93311. United States.
5 Psychology Undergraduate Program, University of California, San Diego, La Jolla, CA 92093. United States.
6 Bakersfield College, Bakersfield, CA 93305. United States.
Corresponding Author Details: Luis A. Vega, Department of Psychology, California State University, Bakersfield, CA 93311. United States.
Received date: 18th June, 2023
Accepted date: 25th July, 2023
Published date: 27th July, 2023
Citation: Vega, L. A., Agabao, M., Franco, A., Estrada-Rodriguez, Z., Gomez, F., Selene, N., Lee, Y., Gonzales, A., Wu, K., and Niestas, A. S., (2023). Transcending Trauma: Treatments’ Caveats, Construal, and Cultural-Context.
Copyright: ©2023, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
We examined evidence for the view that trauma transcendence should be operationally defined as a process rather than an end goal and considered caveats in individual differences of construal and contextual-cultural influences. The focus was on the role of therapy treatments used in trauma transcendence and the extent to which evidence-based information, theory, and generalizability are—can/ should be—involved. Our methodological analysis and theoretical discussion of extant research evidence focused on (a) models of trauma transcendence, (b) the multivariate, scientific nature of evidence-based therapy treatments/outcomes, (c) the need to have tailor-made trauma treatments that allow for individualized patient variability, (d) therapists’ skill-limitations/strengths, and (e) the need for methodical, systematic approaches to trauma transcendence. Our conclusions show that evidence-based approaches are needed, but limits remain in generalizability of findings. We also recognize a need for multipronged approaches to trauma transcendence, from trauma-informed approaches, to reducing the shortage of therapists, increasing methodological-clinical sophistication in the public sphere, and addressing the multivariate nature of trauma. Finally, we suggest that navigating trauma transcendence should be a process that goes beyond the homeostatic state.
Keywords: Trauma-transcendence, Evidence-based therapy, Assessment-treatment validity, Trauma-informed approaches, Construal-and-context in therapy outcomes; Multicultural competence
Introduction
Transcending trauma is crucial today, considering catastrophic events ranging from the COVID-19 pandemic, natural disasters, human dislocations, the ubiquity of gun violence in many societies, to ongoing wars. In 2021 alone, the number of people seeking mental-health care in the United States was 42 million [1], or about 12 percent of the US population of 331.4 million [2]. To help with trauma transcendence, our research group has shown that we must first understand how a person’s affect, behavior, and cognition-also known as the ABC tripartite model in social psychology [3] need to be considered [4]. In specific, Zamora et al. showed that different types of trauma treatments, such as the 12-steps approach program used by Alcoholics’ Anonymous, Kübler-Ross [5] six-stages of grief, as well as the broaden-and-build theory of emotions [6], all involved aspects of Affect, Behavior, Cognition (ABC). Vega et al. [7] further extended Zamora et al.’s [4] work by showing that transcendence needed to not only involve all aspects of the ABC tripartite, but must also be a proactive approach, requiring monitoring of trauma through a 5Rs model (trauma -reduction of wellbeing, -relapse, -resiliency, -recovery, and -realization), as well as having a good definition of trauma, an opaque endeavor. In this paper we further offer clarifications to the 5Rs model, as well as review and propose continued improvements to trauma transcendence based on methodical, systematic approaches.
Transcendence Trauma Model: Methodical Refinements
We have argued that transcending trauma required a proactive approach, where the status of trauma could be monitored according to the 5Rs model, and that this required ongoing efforts of gradual improvements that went over and beyond the homeostatic state [7]. Also, we stated that trauma uniquely and differentially affected individuals—on a severity continuum of no- to high-harm trauma experience for a similar event across individuals. That is, an event that is traumatic for one person may not be for another. Furthermore, a person’s definition and experience of trauma is influenced by context and personal construal or interpretation. We offered that using standardized approaches and more scientific norming, when appropriate and available was a necessity. Here, we propose to embed our model in a more contextual setting, with varying paths to emulate how people may possibly navigate trauma. Figure 1 presents our modifications, with hyphenated arrows showing that transcendence can be nonlinear, and that context, circumstances, and culture, as examples, should be embedded through the system affecting trauma transcendence (shaded oval).
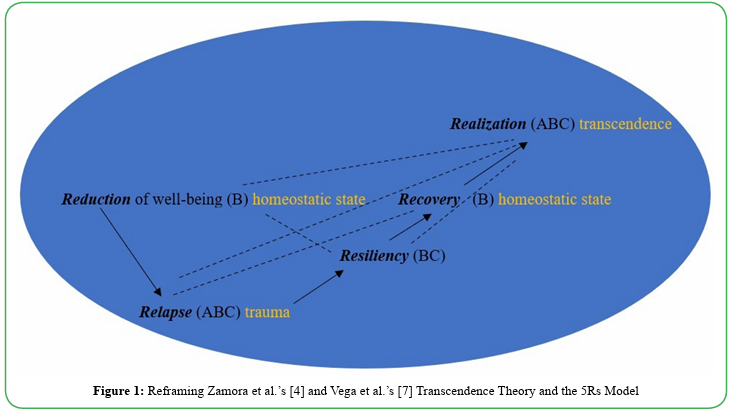
Figure 1: Reframing Zamora et al.’s [4] and Vega et al.’s [7] Transcendence Theory and the 5Rs Model
The main points of the model in Figure 1 are that transcending trauma requires attention to four foundations. First, trauma affects a person’s emotions, actions, and thinking, which are denoted as affect, behavior, and cognitions (i.e., ABC) at each step. Second, the 5Rs (trauma -reduction of wellbeing, -relapse, -resiliency, -recovery, and -realization) operationally define locations of trauma transcendence in relation to the homeostatic state. Thus, relapsed connotes a negative influence of trauma, whereas resiliency connotes a positive one. Third, how a person progresses through trauma transcendence, or each of the 5Rs, does not have to be in the outlined sequence, for it could be non-linear (dashed lines)—so some people who are not affected by a traumatic effect, may be able to access transcendence and wellness of positive emotions, thoughts, and actions (or positive outcomes of ABC). Finally, implicit in Figure 1 is that being in a homeostatic state, as one was before a traumatic event, is not as ideal as transcending into a higher state of wellbeing. Further, as Vega et al. [7] showed, trauma transcending is a process that requires ongoing, proactive effort to not re-live, or stagnate with negative effects of past trauma. Therapies and treatments may not be explicit in these foundations, but our research goal is that they should be if we are to rely on evidence-based analysis for the effectiveness of therapy.
It is important that we keep a holistic view of trauma transcendence, so that we can make processes, procedures, and practices of transcending trauma, transparent. For example, an individual’s cultural background needs to be considered in how that person will navigate trauma transcendence. This is essential because a person’s cultural background may be a strength in their journey to transcending trauma. Lilienfeld [8] has shown that psychological treatments at times can cause more harm than good, and this can be particularly the case in multicultural settings [9]. According to Sue et al. [10], this is especially true when we lack cultural humility to acknowledge issues of multicultural competence—costumes, language, values, world views and the intersectionality of issues of social justice which include historical oppression, discrimination, racism, sexism, and many other -isms. A more detailed account of how therapy may cause harm is offered by Curran et al. [11], who showed that in addition to a lack of cultural competence, a negative therapeutic process like unresolved alliance raptures [therapist-client], therapists’ practices of rigidity, over-control, lack of knowledge, can all derail trauma transcendence.
Thus, as Cronbach [12] once stated, understanding the full person within their psychology necessitates an account of explained- and unexplained-variance, experimental approaches that account for variance between treatments and within individuals, and putative multivariate (correctional) influences, identifiable or not. It is essential that we examine and meet both statistical/methodological assumptions of treatment validity and generalizability, as well as consider any omitted variable(s) and basic measurements of constructs. This is similar to data scientists worrying about violations of their models involving curvilinearity, existence of outliers, heteroscedasticity (unequal error residuals), and omitted X variables in their regression models [13]. Or, experimentalists, who must worry about demand characteristics, progressive error, experimenter biases, and even what to call the control group (baseline, comparison group, placebo;[14]). Hence, the importance for being methodical and systematic in treatments to trauma transcendence is of utmost importance for research on mental health treatments and outcomes as it is for data scientists and experimentalists obtaining valid results.
Evidence-Based Trauma Transcendence Treatments
That we must treat trauma is not debatable, but who can treat trauma has been the subject of scrutiny in public discourse and professional associations. Baker, McFall, and Shoham [15] published concerns that practitioners of psychological services often failed to base treatments on scientific evidence. They traced this issue to the training of doctoral students, with Philosophy Doctorates (PhD) trained in laboratories, research, and clinical practice settings perceived as more adept at applying scientific rigor and evidence based approaches. In contrast, the degree of Doctor of Psychology, with persons earning this degree known as PsyDs, are perceived to mostly be trained more for clinical practice and less for laboratory and research practice— more science-based approaches. Adding to this perception is the fact that many PsyD programs are for-profit programs, with Baker et al. [15] arguing that just like in medicine in the early 1900s, when personal experience was valued higher than scientific research, psychology must now adopt to scientific application in accreditation, as medicine once did.
One result of this debate is a bifurcation of accrediting bodies. The American Psychological Association (APA) used to be the sole body offering accreditation to clinical training institutions, with some PsyD graduate programs meeting their standards. Because the Association of Psychological Science (APS), which split from the APA in 1989, has focused on stricter scientific rigor, they now offer an accreditation to doctoral-level clinical programs, known as PCSAS (Psychological Clinical Science Accreditation System), and it excludes PsyD degree programs. This process of gatekeeping aims to infuse science into licensure of clinicians [16].
The aims of infusing science into clinical practice are important and it may lead to similar advances for mental health as medicine did for medical practice and treatment. However, it must be noted that the emergence of therapy is recent and ongoing, with Freud anticipating current debates. According to Dominus [1], writing in the New York Times on the effectiveness of therapy, Freud himself was “famously uninterested in submitting his innovation [psychoanalysis] to formal research.” Even though some of his findings were finding scientific support, Freud strongly believed that “…the wealth of reliable observations on which these assertions rest make them independent of experimental verification.” Thus, if we are to examine the record on the usefulness of therapy in helping the transcendence of trauma, reconciling scientific, political, and practical considerations need to be explicitly examined. We attempt to provide insight into this perspective by discussing issues of theory-making (inductive approach), and theory-testing (deductive approach) as these apply to trauma transcendence.
The Rise of Talk Therapy as an Inductive Approach to Trauma Transcendence
On the footsteps of Darwin’s [17] observational work and findings on natural selection, it is likely Freud may have sought to make similar inroads through observational inference into the psyche of fellow humans. Many of his observations on early parental experiences have passed scientific scrutiny, as psychoanalysis and associated talk-therapy has become less-libido-focused [1]. Others on his footsteps, such as Carl Jung’s [18] association method, and Carl Roger’s [19] client-centered approach have all been bottom-up approaches, demonstrating the usefulness of transcending trauma as part of the 5Rs (trauma - reduction of wellbeing, -relapse, -resiliency, -recovery, and -realization; [7]). These have all involved aspects of affective, behavioral, and cognitive (ABC) approaches. Expressive writing— a recent, behaviorally-primed approach to therapy— has also been a serendipitously bottom-up approach [20].
Interestingly, that talk-therapy works is supported in the literature [1,21] - with effect sizes measurable—and yet, unconventionally, therapy outcomes often lie on the skills of the therapist(s), and their techniques, as well as the patient-therapist bond [22]. This begs the question on the distinction of the effectiveness between PhD versus PsyD credentialed therapists. While (inductive) skills derived from practice and experience for PsyDs may be shown to be effective, qualitatively measuring these effects is not always done, and at times when it is done, the qualitative methodology—such as action research which investigates the issue as it is solved—is not acknowledged to have the same scientific rigor as evidence-based [deductive], experimental conclusions required of PhD programs. Moreover, outcome effectiveness due to patient differences such as gender, comorbidities, cultural background, and many others have not been fully examined [1]. Consequently, evidence-based data will be crucial as we form theories that are supported and valid, if we are to avoid the Dodo Bird effect1 in therapy [23], so that we do not fall into the trap of assuming therapies and patients are all the same.
Therapy is inductive in nature, with the therapist and even the patient, observing patterns, trends, and grouped characteristics that imply a diagnosis, or that lead to resiliencies and improvements. But to be able to generalize these observed outcomes, the purported trauma transcendence treatments must be tested methodically and systematically, so we do not start from ground zero with every patient. Testing our inductively derived theories will help us standardize our treatments, even if to the chagrin of the late Freud [1].
Directed and Deductive Approaches to Trauma Transcendence Therapy
Predicting trauma transcending therapeutic outcomes necessitates that we have good theories. One drawback is that if we only focus on metric outcomes, then we may over focus on the effects, not the causes. Caveats can be found in the medical model where “magic pills” have brought immediate relief with treatment, but not a cure, and where the roots of the ailment can remain. Mental health practitioners, with psychologists in specific and researchers too, have not been immune to the debate [24], of using magic pills or prescribing drugs for mental health ailments. To be fair, chronic problems can be true of mental health as they are of physical health, and pharmaceutical therapies may be required [25].
And yet, the pressing nature of mental health problems often requires reactive approaches, with a focus on symptoms rather than causes. The fact that trauma and mental health issues are imbued with myriad, multivariate causes, makes it difficult to distill and isolate individual variables for analysis. Still, Dominus [1] shows that causal variables can be of focus, through simple questions like, “is talk therapy better than no therapy?” which can be addressed using randomized studies. Glass and Smith [21] answered this question in the affirmative, showing that persons who suffer from neurosis and psychosis benefited from talk therapy. In their study, the researchers compared untreated to treated individuals. Their results showed that 75 percent of those treated with therapy manifested statistically significant improvement on the outcome measures, compared to no treatment individuals. In fact, to answer the question Glass and Smith had to create a new statistical technique called meta-analysis, which quantified impact, and answered the question of generalization across therapies—all worked regarding talk therapy. It should be noted that therapy having beneficial outcomes since Glass and Smith’s [21] study has been shown to be overall true for patients with anxiety, depression, and other psychological disorders [1].
Meta-analysis has been a gold standard to show if theoretical predictions hold across studies, using randomized sample designs. Predicted results are not always supported, however, as Cuijpers et al. [26] have found that psychotherapy studies focused on treating depression showed that half of the patients receiving therapy had little or no benefit, with one-third experiencing reduced symptoms to meet being diagnosed as not having depression. Even then, consensus on the value of treatment outcomes and subsequent generalization across populations from samples—even when randomized, and plausible omitted mediator/moderator variables are included-can impact the interpretation and importance of results [27,28]. This is reflected in a registered (predictions made a priory) meta-analysis of studies done in the last two years on the effectiveness of psychodynamic therapy by Leichsenring et al. [29], who showed that, “…no single therapeutic approach fits all psychiatric patients, as shown by the limited success rates across all evidence-based treatments” (p. 286).
Adding to the difficulties of assessing the effect of randomized, experimental studies on trauma transcending therapies is the replication crisis that has impacted psychology, and science in general. It is estimated that only 36 percent of psychological studies on average can be replicated [30]. Even highly established, empirically rooted findings that used meta-analysis have been the subject of suspicion under the replication crises [31]. And adding to the limitations of meta-analysis in what is called the file-drawer effect—where non-supporting findings are not published, the impact and effect of randomized studies might be more limited than research has shown. As well as data interpretation limitations, factors such as an appropriate control group, where half of the randomized group is put on a waiting list (no treatment), where being in a state of limbo has ethical implications of depriving patients of beneficial outcomes, if any, and where placebo effects—or nocebo effects, opposite effects/worsening symptoms [32], can alter or limit the findings.
Trauma Transcendence Tailored Therapy Treatments
The term trauma-transcendence implies being proactive if we are to treat trauma as a process or continuum. This approach seems right, as individuals will differ in their experiences navigating the 5Rs depicted in Figure 1. Advancing trauma transcendence research and practice must continue, as advocated by leaders of the PCSAS and NIMH (the National Institutes of Mental Health) [16], particularly where medical pharmaceutical interventions are needed. Scientific evidence in trauma transcendence requires that we navigate the inductive- (theory building; observations) and deductive- (theory -testing and -revisiting) research cycle that is true of all science [33]. Manifesting and applying evidence-based interventions in the form of norming, standardization of operational definitions, generalizations, and enhanced wellbeing to those experiencing trauma is an ongoing process [1]. Providing tailored therapy treatments is imperative for mental health professionals who must meet the distress demands of our times. If we are to avoid the pitfalls of therapy causing harm [8], we need to be methodical and systematic to narrow the variability where treatments work and are properly tailored to patients’ needs.
Extant research provides guidelines for potential ways to tailor therapy to those seeking trauma transcendence therapy. Sue et al. [10] overview issues in counseling the culturally diverse, in a seminal book now in the ninth edition. The myriad issues they discussed are copious, from therapists having cultural humility/competence, to individuals crisscrossing multiple social identities that make them vulnerable to stereotypes, stigmas, and scapegoating (ABC of social psychology). Would be therapists are warned and advised about their limitations or walking in blind when assisting clients in a trauma transcending state. The importance of having a diverse therapists’ workforce is also highlighted as important by Sue et al., and a need echoed by minority therapists [34]. Table 1 illustrates a few selected groups Sue et al. [10] cover in their book, with issues that may appear of most concern to the identity space of a group [35], and issues where uninformed therapists can commit malpractice and maligned outcomes [8,11].
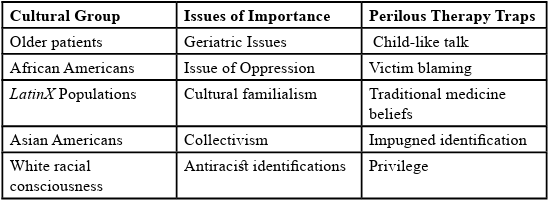
Table 1: Patient Subgroups, their Issues of Importance, and Perilous Therapy Traps in Selected Groups [10].
No matter how many evidence-based therapies we have, if there are not enough therapists to tackle the mental health crises of today [36], many individuals who can benefit from trauma transcendence will go unsupported. With millions of individuals in need of mental health care [1], and not enough mental health professionals to meet demand, it is imperative that support systems be in place—such as support groups used by alcoholic anonymous, extended families in many cultures, and community centers tailored to older adults. One effort involves trauma-informing procedures, processes, and programs that can be used by communities, agencies, universities, initiated by the United States Department of Health and Human Services. Their guide is available and accessible to the public [37].
As the above publication notes, a trauma-informed approach requires acknowledging collective trauma imposed not only on individuals, but families, and communities. Many communities have histories of trauma due to historical issues of oppression and discrimination that can cause re-traumatization [37]. One example is the amply demonstrated racial trauma that African Americans have suffered in American society, which according to Tatum [38] is manifested in through hurtful statements such as, why are all the black kids sitting together in the cafeteria? to endemic issues of exclusion in housing and employment, to police excessive use of force against this community, all leaving enduring trauma. Thus, not only are there not enough therapists, but victims of trauma involved individuals, families, and communities, which a trauma informed approach tries to bring into focus for trauma transcending interventions.
Briefly, SAMHSA’s [37] efforts are designed to infuse trauma informed approaches, asking all of us to be upstanders rather than bystanders to those living with trauma. This approach seeks to ingrain educational foundations in institutions and populations that are responsive to those in trauma-plight. It seeks to do this by helping potential responders (a) identify trauma conditions, (b) inform on trauma reduction pathways residing within institutional supports and control, (c) use established, proven principles that can be of guidance and application, (d) suggest guidance implementing programs that are trauma informed, and (e) consider trauma in the context and community of those affected.
In addition to the trauma-informed approaches discussed above, it is important to ensure that treatments be individualized for those trying to transcend trauma, depending on the trauma they have experienced. Deindividualization—losing track of the individual’s needs-is part of the trauma, and the reason the shaded area in Figure 1 is large. It is important that support systems to those in the process of transcending trauma allow for non-linear progress of the 5Rs model, that issues (or variables) affecting that person be acknowledged and monitored for progress—where evidence-based approaches can be applied. For example, Kaye [39] proposed a grief barometer, where those transcending trauma due to losing a loved one can measure their progress. In other instances, a relationship tree [40] has been shown to assess support systems as a person is to engage in trauma transcendence. Another example is Logotherapy, where seeking trauma transcendence is pursued through seeking purpose, meaning, and deliberate choice of a positive perspective and reflection. This approach was pioneered by Frankl [41] and is well demonstrated by Southwick et al. [42], who applied it to combat veterans experiencing post-traumatic stress disorder (PTSD). This approach of logotherapy is like expressive writing, which is also self-guided and works best with a supportive therapist [20].
Conclusion
As we stated earlier, the field of trauma transcendence is relatively new within Western historical standards. Psychoanalysis traces its roots to 1880-1882 [43], close to the formal establishment of the discipline of psychology in 1879 [44]. We can only hope that in time, trauma transcendence will be a science as medicine is today, and its accrued advances, even though the medical field can be traced back to the Greeks. The plight of those transcending trauma necessitates access to approaches that will work, and to the degree these are methodical and systematic, the better [45]. That more trauma transcending information needs to be made transparent and available to all, has amply been demonstrated in the discussion above. The science cycle of inductive- and deductive-approaches will continue to advance our knowledge. We hope that more methodological literacy approaches can become part of practitioners’ tools and treatment repertoires. For example, small N designs are not seen too often in the literature, but these could see more widespread adoption. Myers and Hansen [14] discussed how if we want to see the impact of a new therapy treatment for depression, not enough depressed individuals might be available for a randomized trial. An experiment could still be conducted in which the progress of one or a few individuals could be studied intensively using ABA (i.e., baseline-treatment-baseline progression) variation designs, which can have high internal validity, have baselines, and the individual serves as its own control group— obviating ethical concerns of treatment deprivation, as discussed above in between subjects randomized experiments. Finally, we remain hopeful that science will continue to make progress in attending to the alleviation of those navigating trauma transcendence beyond the homeostatic state and to do so by using the foundations of the 5Rs model covering the ABC tripartite for wellness and wellbeing [4,7].
Competing interests:
The author(s) declare that they have no competing interests and express gratitude to two anonymous reviewers whose comments greatly improved this manuscript.
References
Dominus, S. (2023, May 16). Does therapy really work? Let’s unpack that. New York Times.View
United States Census Bureau (2021). Historical population change data (1910-2020). Retrieved from https://www.census. gov/data/tables/time-series/dec/popchange-data-text.html.View
Jhangiani, R., & Tarry, H. (2022). Principles of social psychology (1st international H5P edition). BCcampus. https:// opentextbc.ca/socialpsychology/ View
Zamora, R., Morales, M., Estrada-Rodriguez, Z., Montano, S., Mun, T., Watson, J., & Vega, L. A. (2019). Mind-body and action in the face of calamity: The ABCs of transcendence. Paper presented at the 99th Annual Convention of the Western Psychological Association, April 27-29, Pasadena, California. Retrieved from https://drive.google.com/file/d/1Tmwof1Tu4hd D24o1J1O8PFQjy4KSWZTf/viewView
Kübler-Ross, E. (1969). On death and dying. New York: Scribner.View
Fredrickson, B. L. (1998). What good are positive emotions? Review of General Psychology, 2, 300–319. View
Vega, L. A., Zamora, R., Lee, Y., Estrada-Rodriguez, Z., Rhodes, S., Mun, T., & Watson, J., (2021). Using social psychology’s ABC Triad to transcend trauma: Improving on the homeostatic state. Journal of Rehabilitation Practices and Research, 2(2), 122-128. https://doi.org/10.33790/jrpr1100122View
Lilienfeld, S. O. (2007). Psychological treatments that cause harm. Perspectives in Psychological Science, 2(1), 53-70.View
Wendt, D. C., Gone, J. P., & Nagata, D. K. (2014). Potentially harmful therapy and multicultural counseling: Bridging two disciplinary discourses. The Counseling Psychologist 1-25, [online: 10.1177/0011000014548280.View
Sue, D. W., Sue, D., Neville, H. A., & Smith, L. (2022). Counseling the culturally diverse: Theory and practice (9th ed.). Hoboken, NJ: Wiley. View
Curran, J., Parry, G. D., Hardy, G. E., Darling, J., Mason, A., & Chambers, E. (2019). How does therapy harm? A model of adverse process using task analysis in the meta-synthesis of service users’ experience. Frontiers in Psychology, 1-13: online. https://doi.org/10.3389/fpsyg.2019.00347View
Cronbach, L. J. (1957). The two disciplines of scientific psychology. American Psychologist, 12, 671-684. View
Cohen, J., & Cohen, P. (1983). Applied multiple regression/ correlation analysis for the behavioral sciences. Hillsdale, NJ: Erlbaum.View
Myers, A., & Hansen, C. (2012). Experimental psychology (7th ed.). Belmont, CA: Cengage.View
Baker, T. B., McFall, R. M., & Shoham, V. (2008). Current status and future prospects of clinical psychology: Toward a scientifically principled approach to mental and behavioral health care. Psychological Interest in the Public Interest, 9(2), 67-103. DOI: 10.1111/j.1539-6053.2009.01036.xView
Jaffe, E. (2012, December). Clinical science accrediting system earns national recognition. Observer. Retrieved from, https:// www.psychologicalscience.org/observer/clinical-science accrediting-system-earns-national-recognition.View
Darwin, C. R. (1859). On the origin of species by means of natural selection, or the preservation of favoured races in the struggle for life. London: John Murray. View
Jung, C. G. (1910). The association method. American Journal of Psychology, 31, 219-269. View
Rogers, C. R. (1946). Significant aspects of client-centered therapy. American Psychologist, 1, 415-422.View
Pennebaker, J. W. (2018). Expressive writing in psychological science. Perspectives on Psychological Science, 13(2), 226 229.View
Glass, G. V., & Smith, M. L. (1977). Meta-analysis of psychotherapy outcome studies. American Psychologist, 32(9), 752-760. https://doi.org/10.1037/0003-066X.32.9.752View
Wampold, B. E. (2015). How important are the common factors in psychotherapy? An update. World Psychiatry, 14(3), 270 277. https://doi.org/10.1002/wps.20238View
Rosenzweig, S. (1936). Some implicit common factors in diverse methods of psychotherapy. American Journal of Orthopsychiatry, 6(3), 412–415. https://doi.org/10.1111/j.1939-0025.1936. tb05248.xView
Lavoie, K. L., & Barone, S. (2006). Prescription privileges for psychologists: a comprehensive review and critical analysis of current issues and controversies. CNS Drugs, 20, 51-66. https:// doi.org/10.2165/00023210-200620010-00005View
National Institute of Mental Health (2021). Chronic illness and mental health: Recognizing and treating depression. U.S. Department of Health and Human Services. Publication No. 21-MH-8015.View
Cuijpers, P., Quero, S., Noma, S., Ciharova, M., Miguek, C., Karyotaki, E., Cipriani, A., Cristea, I., & Furukawa, T. (2021). Psychotherapies for depression: a network meta-analysis covering efficacy, acceptability, and long-term outcomes of all main treatment types. World Psychiatry, 20(2), 283-293. https:// doi.org/10.1002/wps.20860View
Bollen, K. A. (1989). Structural equations with latent variables. New York: John Wiley & Sons.View
Rosenthal, R., & Rosnow, R. L. (1991). Essentials of behavioral research: Methods and data analysis (2nd ed.). New York: McGraw Hill.View
Leichsenring, F., Abbass, A., Heim, N., Keefe, J. R., Kisely, S., Luyten, P., Rabung, S., & Steinert, C. (2023). The status of psychodynamic psychotherapy as an empirically supported treatment for common mental disorders – an umbrella review based on updated criteria. World Psychiatry, 22(2), 286-304. https://doi.org/10.1002/wps.21104View
Diener, E. & Biswas-Diener, R. (2023). The replication crisis in psychology. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from, http://noba.to/q4cvydehView
Engber, D. (2016, March 6). Everything is crumbling: An influential psychological theory, borne out in hundreds of experiments, may have just been debunked. How can so many scientists have been so wrong? Slate.com. Retrieved from http://www.slate.com/articles/health_and_science/ cover_story/2016/03/ego_depleti on_an_influential_theory_in_ psychology_may_have_just_been_debunked.htmlView
Kennedy, W. P. (1961). The nocebo reaction. Med World, 95, 203–205. View
Bhattacherjee, A. (2012). Social sciences research: Principles, methods, and practices. Creative Commons License. Retrieved from https://open.umn.edu/opentextbooks/textbooks/social science-research-principles- methods-and-practices.View
Wu, J. (2022, October 6). How to cope with racism-induced stress: As an Asian therapist, I witnessed firsthand the effect of xenophobia and racism had on my on my community. WashingtonPost.com.View
Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: A black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. University of Chicago Legal Forum, 1, article 8. Retrieved from http:// chicagounbound.uchicago.edu/uclf/vol1989/iss1/8View
Phillips, L. (2023, May 8). A closer look at the mental health provider shortage. Counseling Today [A publication of the American Counseling Association]. Retrieved from https:// ct.counseling.org/2023/05/a-closer-look-at-the-mental-health provider-shortage/View
Substance Abuse and Mental Health Services Administration (2014). SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. HHS Publication No. (SMA) 14-4884. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from https://ncsacw.samhsa. gov/userfiles/files/SAMHSA_Trauma.pdfView
Tatum, B. D. (2017). Why are all the Black kids sitting together in the cafeteria?: And other conversations about race. New York: Basic Books.View
Kaye, D. (2023). Blame Gabriel: Acute grief following death of a loved one a study of self-empowerment therapy. International Journal of Psychiatry, 8(2), 21-27. View
Peterson, N. L., & Goldberg, R. M. (2016). Creating relationship trees with grieving clients: An experiential approach to grief counseling. Journal of Creativity in Mental Health, 11(2), 198 212. https://doi.org/10.1080/15401383.2016.1181597View
Frankl, V. E. (1963). Man’s search for meaning: An introduction to Logotherapy. New York: Washington Square Press.View
Southwick, S. M., Gilmartin, R., McDonough, P., & Morrisey, P. (2006). Logotherapy as an adjunctive treatment for chronic combat-related PTSD: a meaning-based intervention. American Journal of Psychotherapy, 60(2), 161-174. https://doi. org/10.1176/appi.psychotherapy.2006.60.2.161View
Freud, S. (1917). The history of the psychoanalytic movement (A. A. Brill, Trans.). Originally published in New York by the Nervous and Mental Disease Pub. Co. (Original German work published 1914.)View
Cattell, J. M. (1888). The psychological laboratory at Leipsic. Mind, 13, 37-51.View
Thambirajah, M. S. (2005). Psychological basis of psychiatry [Psychological measurements: their uses and misuses, chapter 8]. Edinburgh, NY: Churchill Livingston.View
Baumeister, R. F., & Vohs, K. D. (2018). Revisiting our reappraisal of the (surprisingly few) benefits of high self esteem. Perspectives on Psychological Science, 13(2), 137-140.View