
- About the Journal
- Editorial Board
- Review Process
- Author Guidelines
- Article Processing Charges
- Special Issues
- Current Issue
- Past Issue
 Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour
Journal of Mental Health and Social Behaviour Volume 4 (2022), Article ID: JMHSB-159
https://doi.org/10.33790/jmhsb1100159Research Article
Depression among Healthcare Workers During COVID-19 Pandemic in Hulu Langat District, Selangor, Malaysia: A Cross-sectional Study
Hadita Sapari1, Mohamad-Ikhsan Selamat1, Salina Mohamed2,3, Zailiza Suli 4, & Mohamad-Rodi Isa1*
1*Department of Public Health Medicine, Faculty of Medicine, Universiti Teknologi MARA, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
2Department of Psychological Medicine, Faculty of Medicine, Universiti Teknologi MARA, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
3Department of Psychological Medicine, Hospital Universiti Teknologi MARA, 42300 Bandar Puncak Alam, Selangor, Malaysia.
4Hulu Langat District Office, Lot 7253, Jalan Hentian Kajang 1C, Pusat Hentian Kajang Jalan Reko, 43000 Kajang, Selangor, Malaysia.
Corresponding Author Details: Mohamad Rodi Isa, MBBS, DAP&E, MPH, DrPH, Department of Public Health Medicine., Faculty of Medicine, Universiti Teknologi MARA, Jalan Hospital, 47000 Sungai Buloh, Selangor, Malaysia.
Received date: 14th April, 2022
Accepted date: 16th May, 2022
Published date: 18th May, 2022
Citation: Sapari, H., Selamat, M.I., Mohamed, S., Suli, Z., & Isa, M.R., (2022). Depression among Healthcare Workers During COVID-19 Pandemic in Hulu Langat District, Selangor, Malaysia: A Cross-sectional Study. J Ment Health Soc Behav 4(1):159.
Copyright: ©2022, This is an open-access article distributed under the terms of the Creative Commons Attribution License 4.0, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: COVID-19 is a serious threat to the global, not only to health, economy and society but also is a great challenge to HCW’s mental health. A lot of studies were carried out and found HCW’s psychological well-being has been severely affected, especially those in the hospital setting. This study aims to determine the prevalence of depression and the factors associated with depression among HCWs in public health settings during the COVID-19 pandemic.
Methods: A cross-sectional study was conducted at 13 health clinics and one District Health Office in Hulu Langat District. This study was conducted from February 2021 to Mei 2021. A self-administered questionnaire was distributed consisting of three sections (sociodemographic, job characteristics and depression assessment using validated PHQ-9 tool). Descriptive statistics were used to describe the sociodemographic, and multiple logistic regression was used to determine the factors associated with depression.
Result: A total of 291 HCWs were involved in this study. The prevalence of depression among HCWs was 22.7 (95%CI: 22.65, 22.98). Female (Adj. OR=2.01, 95% CI: 1.016, 3.55), stress at work (Adj. OR=3.22, 95% CI: 1.48, 7.02), conflict among colleague (Adj. OR=3.33, 95% CI: 1.72, 6.34) and never attended training or orientation related COVID-19 management (Adj. OR=2.30, 95% CI=1.13, 4.70) were associated with depression.
Conclusion: The prevalence of depression in this study was comparable with international studies conducted during pandemic COVID-19, but was lower than the local prevalence of depression conducted pre-pandemic. A healthy working environment needs to be conducted to ensure psychological well-being and hence alleviate the depression among HCWs.
Conclusion: The prevalence of depression in this study was comparable with international studies conducted during pandemic COVID-19, but was lower than the local prevalence of depression conducted pre-pandemic. A healthy working environment needs to be conducted to ensure psychological well-being and hence alleviate the depression among HCWs.
Keywords: Depression, Psychological Impact, Public Health Care Worker
Introduction
The World was shocked by the emergence of a new mystery virus at the end of 2019 in Hubei Wuhan, China. COVID-19, a novel coronavirus, has spread from the People's Republic of China to 20 other countries in the first six weeks of the new decade. As a consequence, on 30th January 2020, the Director-General of the World Health Organization (WHO) declared the outbreak a Public Health Emergency of International Concern (PHEIC) [1].
Following this, healthcare workers (HCW) in both divisions (either in public health or clinical) play a crucial role in diagnosing, treating COVID-19 patients, controlling and planning mitigation plans to contain the disease. Moreover, it’s been almost two years since the HCW worldwide struggled to manage the COVID-19 outbreak and thus exposed to highly stressful levels and traumatic events. During the peak of COVID-19 in China and Italy, a rapid systemic review done by Muller, Hafstad [2] showed the prevalence of depression was 21%. WHO has highlighted the exceptionally high load on healthcare workers and has asked for prompt action to address the urgent needs and actions required to save lives and avert a serious impact on healthcare workers' physical and mental health [3]. According to Chew, Ngiam [4], all HCWs are vulnerable to suffering psychological impacts regardless of the volume of confirmed COVID-19 cases. Moreover, Wu, Fang [5] emphasize that individuals exposed directly or indirectly to a life-threatening situation may experience a high risk of psychological morbidities.
Malaysia reported the first case in January 2020 and subsequently there were two waves reported in Malaysia that were handled well. The confirmed cases continue to decline and even recorded zero cases on 1st July 2020 [6,7]. It was such a relief for HCW who had been handling the ongoing cases for 5 months. Unfortunately, this was not last long as Malaysia was hit by the third wave again which began on the 8th of September 2020 [8]. The confirmed cases continue to soar since then and even worse in 2021 with the emergence of a new variant of COVID-19 and variant of concern (VOCs) which are highly infectious compared to the variant before [9]. Ultimately, HCW was facing a tougher task compared to previous waves. A lot of local newspapers already highlighted that Malaysian HCW was already overwhelmed, stressed, frustrated as well as emotionally and physically drained [10].
In 2020, a study done involving Asian Pacific countries by Chew, Ngiam [4] revealed that Malaysia’s healthcare workers from medical and non-medical categories suffered the highest prevalence of depression at 14.3%. Furthermore, Mohd-Fauzi M.F., Mohd-Yusoff H. [11] has carried out a study on doctors’ mental health in all health facilities in Selangor including one state health office, 12 public hospitals, and 11 district health offices and found that HCW suffered severe depression (10%).
In view of the prolonged situation of pandemic COVID-19, WHO has produced interim guidelines detailing the strategies to address mental health and psychosocial support (MHPSS) to all layers of the population including HCW [12]. In Malaysia, MHPSS guidelines were developed in 2020 and have been carried out at the national, state and district levels [13,14]. Its establishment aimed to protect or promote psychosocial well-being or prevent or treat mental disorders such as depression, anxiety and post-traumatic stress disorder. The psychological impact in this study was referred to as depression and anxiety.
Although there were a lot of studies had been done before focusing on the psychological impact among HCWs in a hospital setting, the magnitude of psychological impact among HCWs in a public health setting is still lacking and questionable. Health systems preparedness is not only ensuring enough hospital beds, ventilators and intensive care unit (ICU) capacity, but the ability of the health systems to quickly detect new COVID-19 cases and curb the spread of the highly contagious disease is equally or perhaps more important than the prior. Therefore, this study was conducted to determine the factor associated with depression among HCWs during the COVID-19 Pandemic in Hulu Langat district in Selangor, Malaysia.
Material and methods
Study design and location of study
A cross-sectional study was conducted at 13 government health clinics and one District Health Office in Hulu Langat district in Selangor, Malaysia. The health clinics namely Sungai Chua Health Clinic, Bandar Baru Bangi Health Clinic, Batu 9 Health Clinic, Batu 14 Health Clinic, Semenyih Health Clinic, Beranang Health Clinic, Sungai Sekamat Health Clinic, Rinching Tengah Health Clinic, Kajang Health Clinic, Ampang Health Clinic, Bandar Seri Putra Health Clinic, Balakong Health Clinic, Bandar Tun Hussein Onn Health Clinic and Hulu Langat District Health Office. The study was conducted from October 2020 to May 2021.
Study population
The study population was all the HCWs working in public health settings who are registered under Hulu Langat Health District Office and Health Clinics in Hulu Langat. The inclusion criteria were HCW who were literate in either English or Malay, at least aged 18 years old and consented to participate in the study and the exclusion criteria were HCW who has a premorbid psychiatric disease diagnosed by a psychiatrist, on prolonged leave or medical certificate and pregnant regardless weeks of pregnancy.
Stratified proportionate sampling was done to select the number of participants in this study. The location of health facilities in Hulu Langat was stratified into 14 categories which were 13 health clinics and 1 district health office. After the number of participants needed for each stratum was calculated, a simple random sampling was done using computer-generated Statrek software to select the participants based on the name list of HCW in each clinic and health district office. Each participant was given coding to ensure anonymity throughout the study period.
Study instruments
A set of self-administered questionnaires with a written consent form was given to selected respondents. The questionnaire was developed in bilingual. All the given information in the questionnaire would be kept strictly confidential. The respondents also were informed that they could withdraw at any time from the study. The questionnaire was divided into three sections.
Section one comprises 12 items which consist of age, gender, marital status, race, religion, profession category, profession grade, educational level, total household income, living arrangement and pre-morbid illness.
Section two comprises 19 items which consist of workplace area, job position, frequency of contact with suspected or confirmed COVID-19 patient, average working hour per week, Personal history of COVID-19 infection, history of family members infected with COVID-19, history of a colleague infected with COVID-19, ever attended training or orientation related to COVID-19 management, awareness the existence of PPE guidelines produced by MOH, conflict among colleagues, feel stress at work, had to do work that does not usually do, increase workload, ever thought of resigning due to COVID-19 outbreak, awareness the existence of MHPSS, the usage of MHPSS service and action taken when feeling depressed.
Section three covered the assessment for depression using Patient Health Questionnaire 9 (PHQ-9) questionnaire
Patient Health Questionnaire-9 (PHQ-9) (9 items)
This tool offers psychologists concise for assessing depression and incorporates the DSM-IV depression criteria. The diagnostic validity of the 9-item PHQ-9 was established in studies involving eight primary care and seven obstetrical clinics. The PHQ-9 scores were more than 10, the sensitivity was 88% and the specificity was 88% for Major Depressive Disorder. Internal consistency was shown to be high and the internal reliability with a Cronbach’s α of 0.89 in the PHQ Primary Care Study and 0.86 in the PHQ Ob-Gyn Study [15]. This study used the translated Malay version of PHQ by Azah, Shah [16], which has good internal reliability with Cronbach’s α of 0.67, good test retest reliability Cronbach’s α of 0.73 with the best cut-off score of 5 with the sensitivity of 69% and specificity of 60.5%. The total scores are categorized as follow: minimal/no depression (0-4), mild depression (5-9), moderate depression (10-14) and severe depression (15-21). In this study, mild, moderate and severe were classified as having depression.
Method of data collection
There were two methods of data collection which were face to face interviews using administered questionnaires to collect primary data for sections one and two, and a self-administered questionnaire to collect data for depression.
Informed Consent
Consent was taken with the selected participants prior to enrolment into the study. A session in a group with the selected participants was carried out for each clinic. Those who consented were continuing to answer the questionnaire in another room. Only those who agreed to participate in this study were entitled to answer the questionnaire. In addition, the participant was allowed to withdraw at any time from the study.
Ethical considerations
Ethical approval was obtained from Universiti Teknologi MARA Research Ethics Committee and Medical Research Ethics Committee (UiTM Research Ethics Committee: REC/04/2021 (MR/260); Medical Research & Ethics Committee MOH: NMRR-21-144- 58117 (IIR)). Approval for data collection was also obtained from the Selangor Health State Department before the data collection was conducted (Ref: JKNS/KA/Q-712/04-01 Jld 14 (55)).
Statistical Analysis
The data was entered and analyzed using Statistical Package for Social Science (SPSS) version 26.0 (SPSS Inc, Chicago, IL). Descriptive statistics were used to describe the sociodemographic distribution, job characteristics and job position of HCW in Hulu Langat. Normality of the continuous data was checked using central tendency, histogram, skewness and kurtosis. Subsequently, categorical data were presented in frequency and percentage, while continuous data were presented in median and interquartile range (IQR) due to not normally distributed data.
Factors associated with depression were analyzed using binary logistic regression. Simple logistic regression was first conducted to determine the factors and significant value associated with depression and anxiety. The crude odds ratio (OR) and 95% confidence interval (CI) were estimated. Then, significant variables in SLogR and those variables with less than 0.25 were also chosen for the multiple logistic regression (MLogR) to adjust for the confounding factors using the backward method of analyses. The Cox & Snell square and Nagelkerke R square in the model summary was used to conclude the variance of psychological impact with the significant factors in the model. The interaction and fitness of the model using the Hosmer-Lemeshow and receiver operating characteristic (ROC) curve were also checked. A p-value of less than 0.05 was considered significant. The adjusted odds ratio (Adj. OR) and 95% confidence interval (CI) were estimated.
Results
A total of 291 HCWs were involved in this study giving a response rate of 87.0%. The prevalence of depression among HCWs was 22.7 (95%CI: 22.65, 22.98). The sociodemographic characteristics of the respondents are shown in Table 1. The age of the participants ranges from 23 to 58 years old. The median age was 41 (IQR: 9.0). Slightly more than half of the participants were from 31-to 40 years old, majority of the participants were female (68.7%), married (73.5%), Malays (86.3%), from the support group I (44%), and profession as nurses (30.9%) followed by doctors (20.3%).

Table 1: The sociodemographic characteristics of the respondents (N=291)
The job characteristic of the participants is shown in Table 2. 75.6% of the participants work in health clinics with the majority have been working less than 60 hours per week (85.6%). 60.1% of the participants gave a history of their colleague had been infected with COVID-19. Almost three quarter has attended training or orientation related to COVID-19 and is aware of the existence of the MHPSS program meanwhile 98.6% of them aware of the existence of PPE guidelines by MOH
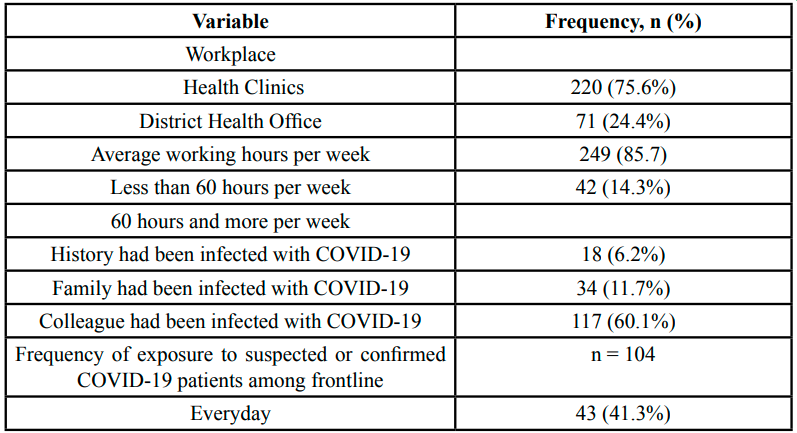
Table 2: Job Characteristics and Position Distribution of the respondents (n=291)
The univariate analysis of the factor associated with depression is shown in Table 3. The significant associated factors for depression in this analysis were gender (female) (p=0.028), feeling more stress at work (p<0.001), conflict among colleagues (p<0.001), had to do work that they usually don’t do (p=0.004) and ever thought of resigning because of COVID-19 (p=0.001). The factors with p-value less than 0.25 were workplace (p=0.110), family had been infected with COVID-19 (p=0.110), training or orientation related COVID-19 management (p=0.094), had increase workload (p=0.094) and awareness the existence of MHPSS program (p=0.090) and ever use MHPSS (p=0.060).
All significant variable and variables with a p-value less than 0.25 was proceeded to multivariable logistic regression to determine the significant associated factors adjusted for confounding factors.
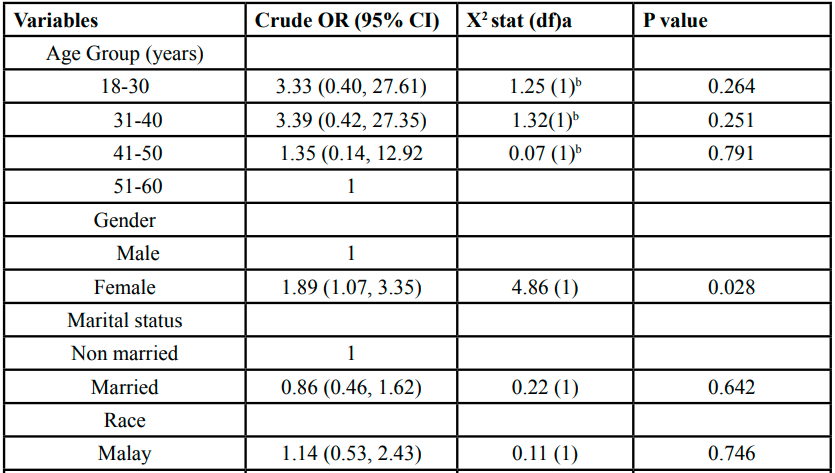
Table 3: Sociodemographic, job characteristics and job position factors associated with depression among HCW from simple logistic regression analysis (n=291)
Table 4 shows the multivariable analysis of the factors associated with depression among HCWs during the COVID-19 pandemic in Hulu Langat District. Females are having 1.01 times the odds of depression compared to males (adj. OR: 1.10 (95%CI: 1.02, 3.55)). Those who stress at work are having 3.22 times the odds of depression compared to those without having stress at work (Adj. OR: 3.22 (95%CI: 1.48, 7.02)). Those who are not having training or orientation related to COVID-19 management are having 2.30 times the odds of depression compared to those who attended the training or orientation (Adj. OR: 2.30 (95%CI: 1.13, 4.70). Those who had conflict among colleagues are having 3.33 times the odds of depression compared to those without any conflict among colleagues (Adj. OR: 3.33 (95%CI: 1.72, 6.34)). All these four factors can discriminate 70.1% of those having depression and not having depression (AUC: 0.701 (95%CI: 0.626, 0.775).
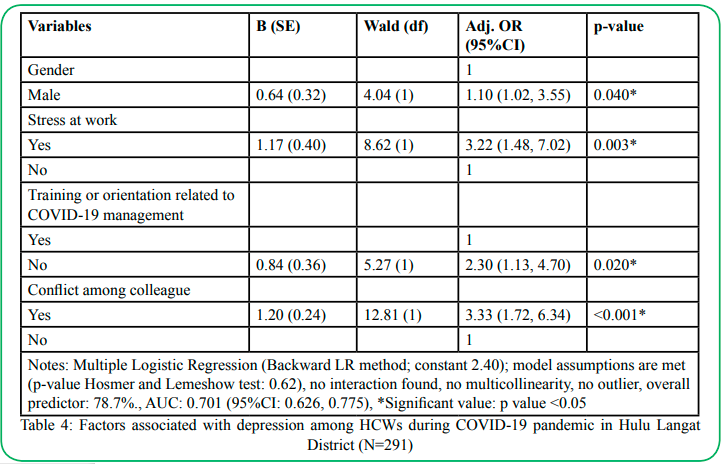
Table 4: Factors associated with depression among HCWs during COVID-19 pandemic in Hulu Langat District (N=291)
Discussion
From this study, the prevalence of depression among HCWs was 22.7% (95%CI: 22.65, 22.98). Similar findings for depression were seen in a systemic review by Muller, Hafstad [2] and Pappa, Ntella [17] which was 21% and 22.8%, respectively. Another study carried out in the Asia Pacific using the DASS-21 assessment revealed that the prevalence of depression among HCW was 14.3% [4]. The result in this study also was the opposite compared to a study done in our neighbourhood country in Singapore which found the prevalence of depression was 8.9% [18]. In Malaysia setting, this study finding was almost similar to a study done among university HCW in Malaysia which also found 29.5% of depression with higher compared to this present study [19].
HCW were already overwhelmed with high workload, heavier psychological work demands, higher job control and long working hours even before the pandemic [20]. Interestingly, even though the prevalence of depression in this study was on par with some international studies, however when compared with a local study done during pre-pandemic, the prevalence of depression was indeed higher than the finding in this study. A study involving HCW in the government university hospital and several health clinics in Kuala Langat also showed that the prevalence of depression was 38.5% [21]. On the other dimension, when comparing the general population's psychological well-being during COVID-19, the general population suffered slightly higher depression (23.9%) compared to HCW. This is probably because a lot of initiatives and interventions have been done by MOH, Malaysia including the MHPSS program, good coping skills among HCW and good preparedness phase by the country [13,19,22]. Furthermore, even this finding showed that the prevalence of depression was low compared to pre-pandemic studies done in Malaysia, this should not be ignored as it indicates that depression have been chronic problem among HCW and should be tackled urgently.
In this study, being a female is a predictor of depression and was associated with 2 times the odds of depression compared to males. Previous studies also revealed that female was a significant factor in psychological impact [23,24]. The possible reason for this is that disparities in biological, psychological, and sociological features contributed to the vulnerability of females suffering psychological impact more common compared to males [25].
HCW who never attended training and orientation related to COVID-19 management appears to be a significant factor for depression. Attending training was proved to alleviate the confidence among HCW in infection control procedures, hence alleviating the psychological health concerns of depression [16]. This finding was consistent with a study done in Bangladesh which revealed that lack of information and access to the latest information; and not updating knowledge on COVID-19 was recognized as a significant factor for depression [27]. Furthermore, the deployment of a new HCW who lacked training or never attended training and had insufficient abilities in an overburdened setting to deliver health care might also contribute to the development of depression.
Stress at work was found as a significant predictor. Xing, Xu [28] in their study conducted in hospitals in China also found that more than two-thirds of the total HCWs in the study felt stress at work. Although HCW in health clinics were not associated with critically sick patients as in that trial, the HCW in health clinics were required to involve patients who were suspected of having COVID-19 and this could contribute to stress. Besides that, other factors that may add to stress include lack of human resources, mobilization to other places, tight scheduling, inadequate logistic support and lack of support measures such as a proper place for physical rest and toiletries [26]. The organizational leader and administrative staff should also proactively ensure that all equipment is appropriate and that employees have access to free healthy food and drinking water throughout working hours, especially during lockdown periods when food and water are scarce. Furthermore, for the HCW to perform their duties smoothly and with less stress, they must have adequate access to the internet, computers and laptops, printers, and charging stations [29].
This study also demonstrated that conflict among colleagues was significantly associated with depression. A similar finding was reported by Lasalvia, Bonetto [30]. In facing this extraordinary outbreak, HCW had to perform a slew of new activities in addition to their regular duties. According to one online survey that was conducted in 2020, only 47% of HCW received a clear action plan for COVID-19 78% of HCW claimed that COVID-19 gave rise to a negative impact on the workplace [31]. It is the responsibility of everyone in the organization, from top management and supervisors to HCW, to ensure that clear orders are issued. Effective communication, empathy, a strong support system, strong soft skills, and teamwork are all critical components of a healthy and harmonious working environment [32].
Strength and limitations of the study
This study was carried out to fill in the gap and investigate the psychological well-being among HCW in the Public Health setting generally and Hulu Langat District specifically as one of the busiest Health districts in Selangor. Moreover, this study was conducted when Malaysia was at the peak of the COVID-19 outbreak and Hulu Langat was categorized as a red zone since the second wave of COVID-19, which might help in portraying the magnitude of psychological wellbeing during an outbreak.
However, there were some limitations in this study. There was no baseline data for mental health status among HCWs screened using PHQ-9 before in Hulu Langat. The existing mental health data were screened using the DASS screening tool. Hence, a better comparison of psychological well-being before and during the outbreak cannot be determined. This study required the participants to a self-administered questionnaire, hence the findings have fully relied on a self-reported survey which may question the authenticity of responses and recall bias. Thirdly, this study was a cross-sectional study and hence cannot be used to infer causality between the independent variables with depression and anxiety. Lastly, this study was done in a single centre of the health district, hence rendering the result from this study less generalizable.
Recommendation for program and policy
There are some recommendations for improvement that can be done by the organization. Firstly, the organization should arrange strategies to ensure all layers of HCW attended training courses mainly regarding COVID-19 especially those who never attended. Secondly, health campaigns such as promoting mental health awareness and encouraging the usage of the MHPSS program should be bolstered. HCW also should be educated on mental illness-related stigma as this possibly could be one of the driving factors that cause low utilisation of the MHPSS program among HCW. Apart from that, providing a nice, healthy and harmonious working environment is vital. This can be done through good communication between top management, supervisors, and the staff in order for them to execute their work efficiently, effectively, and happily, thereby reducing the psychological burden on HCW. Finally, top management must ensure the needs of HCW are well-taken care of especially during a lockdown, in terms of food and drinks accessibility, resting area and other needs such as computers, laptops, internet, manpower as well as to establish nurseries and place for staff’s children to stay while their parent is working.
Conclusion
Stress at work, did not receive training or orientation related to COVID-19 management and conflict among colleagues were among the significant modifiable factors associated with depression. The top management and managers in the organization play a critical role in fostering a healthy working environment, and good teamwork, as well as increasing the awareness among HCW to participate more actively in the district’s MHPSS program.
Conflict of interest:
The author hereby declares there was no conflict of interest in any form.
Abbreviations:
COVID-19: Coronavirus disease; HCW: Healthcare workers; ICU: Intensive Care Unit; MHPSS: Mental Health and Psychosocial Support; MLogR: Multiple Logistic Regression; MOH: Ministry of Health, Malaysia; SPSS: Statistical Package for Social Science; OR: Odds ratio; PHEIC: Public Health Emergency of International Concern; PHQ-9: Patient Health Questionnaire-9; PPE: Personal Protective Equipment; ROC: Receiver Operative Characteristics; SLogR: Simple Logistic Regression; VOC: Variant of concern; WHO: World Health Organization;
Acknowledgement
We would like to acknowledge the immense contribution of anybody for agreeing to be part of the study.
Funding
This is self-funded research and did not receive any funding.
References
World Health Organization (2020). COVID-19 Public Health Emergency of International Concern (PHEIC) Global research and innovation forum.View
Muller, A.E., et al., (2020). The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Research, 293: p. 113441.View
World Health Organization. (2020). Protecting health workers from COVID-19. [cited 2021 june 23]; Available from: https://www.who.int/westernpacific/news/feature-stories/detail/ protecting-health-workers-from-covid-19.View
Chew, N.W.S., et al., (2020). Asian-Pacific perspective on the psychological well-being of healthcare workers during the evolution of the COVID-19 pandemic. BJPsych Open, 6(6): p. e116.View
Wu, P., et al., (2009). The psychological impact of the SARS epidemic on hospital employees in China: exposure, risk perception, and altruistic acceptance of risk. Can J Psychiatry, 54(5): p. 302-11.View
Bernama, (2020). COVID-19 chronology in Malaysia, in Bernama. View
Tee, K., Dr Noor Hisham: Malaysia records zero local Covid-19 transmissions for the second time, three imported cases, in Malay Mail. 2020.View
Rampal, L. and B.S. Liew, (2021). Malaysia's third COVID-19 wave - a paradigm shift required. Med J Malaysia, 76(1): p. 1-4.View
Bernama., (2021). 23 cases involving Covid-19 variants of concern detected, says DG., in Malay Mail.View
Kwan, F. (2020). Covid-19 surge will impact mental health, warn experts. [cited 2021 june, 23]; Available from: https:// www.freemalaysiatoday.com/category/nation/2020/10/10/ covid-19-surge-will-impact-mental-health-warn-experts/.View
Mohd-Fauzi M.F., et al., (2020). Doctors' Mental Health in the Midst of COVID-19 Pandemic: The Roles of Work Demands and Recovery Experiences. International journal of environmental research and public health, 17(19): p. 7340.View
World Health Organization, (2020). Mental health and psychosocialsupport aspects of the COVID-19 response, W.P. Region, Editor. View
MOH, (2020). standard operating procedure (SOP) in providing mental health and psychosocial support services (MHPSS) for COVID-19 response in quarantine stations, s.a.a.v.i.p.s.M. mental health, disease control division, Editor.
MOH, (2020). Garis panduan Pengurusan COVID-19 di Malaysia.
Kroenke, K., R.L. Spitzer, and J.B. Williams, (2001). The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med, 16(9): p. 606-13.View
Azah, M.N., et al., (2005). Validation of the Malay version brief Patient Health Questionnaire (PHQ-9) among adult attending family medicine clinics. International Medical Journal Malaysia, 12: p. 259-263.View
Pappa, S., et al., (2020). Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain, behavior, and immunity, 88: p. 901-907.View
Tan, B.Y.Q., et al., (2020). Psychological Impact of the COVID-19 Pandemic on Health Care Workers in Singapore. Annals of Internal Medicine, 173(4): p. 317-320.View
Chow, S.K., et al., (2021). Religious Coping, Depression and Anxiety among Healthcare Workers during the COVID-19 Pandemic: A Malaysian Perspective. Healthcare (Basel), 9(1).View
Arnetz, B.B., (2001). Psychosocial challenges facing physicians of today. Soc Sci Med, 52(2): p. 203-13.View
Eusof Izzudin, M.P., ., et al., (2018). Prevalence and Related Factors of Depression among Healthcare Personnel at Primary Healthcare Centers. Malaysian Journal of Medicine and Health Sciences 14(SP2): p. 32-36.View
Alshekaili, M., et al., (2020). Factors associated with mental health outcomes across healthcare settings in Oman during COVID-19: frontline versus non-frontline healthcare workers. BMJ Open, 10(10): p. e042030.View
Lai, J., et al., (2020). Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Network Open, 3(3): p. e203976-e203976.View
Xiaoming, X., et al., (2020). The psychological status of 8817 hospital workers during COVID-19 Epidemic: A cross-sectional study in Chongqing. J Affect Disord, 276: p. 555-561.View
Joe Gramigna, M., (2021). Female health care workers at increased risk for mental health problems during pandemic, in Healio News. View
Zhu, Z., et al., (2020). COVID-19 in Wuhan: Sociodemographic characteristics and hospital support measures associated with the immediate psychological impact on healthcare workers. EClinicalMedicine, 24.View
Tasnim, R., et al., (2021). Prevalence and correlates of anxiety and depression in frontline healthcare workers treating people with COVID-19 in Bangladesh. BMC Psychiatry, 21(1): p. 271.View
Xing, L.-q., et al., (2020). Anxiety and depression in frontline health care workers during the outbreak of Covid-19. International Journal of Social Psychiatry, p. 0020764020968119.View
Khan, Y.H., et al., (2020). Work related stress factors among healthcare professionals during COVID-19 pandemic; a call for immediate action. Hospital Practice, 48(5): p. 244-245.
Lasalvia, A., et al., (2021). Psychological impact of COVID-19 pandemic on healthcare workers in a highly burdened area of north-east Italy. Epidemiology and Psychiatric Sciences, 30: p. e1.View
Vibhas Ratanjee, D.F. (2020). What Healthcare Workers Need From Leaders in COVID-19 Crisis. Available from: https:// www.gallup.com/workplace/308957/healthcare-workers-need-leaders-covid-crisis.aspx.View
Tannenbaum, S.I., et al., (2021). Managing teamwork in the face of pandemic: evidence-based tips. BMJ Quality & Safety, 30(1): p. 59View