Safae Ouma1,2, Maria Leyre Lavilla Lerma 3, Nabil Benomar3 and Nabila Rouahi4,*
1 Higher Institute of Nursing Professions and Technical Sciences, ISPITS, Boulevard Abdelkhalaq Torres, Route de Martil, 93100, Tetouan, Morocco. safaeouma21@gmail.com
2 PhD student, Faculty of Health Sciences, University of Jaen, Campus Las Lagunillas s/n, 23071 Jaén, Spain.
3 Faculty of Health Sciences, University of Jaen, Campus Las Lagunillas s/n, 23071 Jaén, Spain; llavilla@ujaen.es; nben@ujaen.es
4 Higher Institute of Nursing Professions and Technical Sciences ( ISPITS Annexe Kenitra), Route de Casablanca, 10120, Rabat, Morocco. rouahinbl@gmail.com
* Correspondence : Rouahi Nabila (Rouahi N), Professor at Higher Institute of Nursing Professions and Technical Sciences ( ISPITS Annexe Kenitra), Route de Casablanca, 10120, Rabat, Morocco.
e-mail : rouahinbl@gmail.com

Cite this article
Abstract
Background: Workplace violence (WPV) perpetrated against health professionals is a major problem in health sector. It affects health and performance of workers. The aims of this study were: 1) to assess WPV facing nurses in the northern region of Morocco and 2) to identify the related factors.
Methods: We conducted a cross-sectional study in the northern region of Morocco from October to December 2021. In total, 391 volunteer nurses working in 13 hospitals were enrolled. A self-reported questionnaire, ‘Violent Incident Form’ (VIF), was distributed to the participants. It assesses verbal and physical violence.
Results: We obtained 98% response rate and 97% of the respondent nurses faced at least one WPV episode the last year. Verbal violence is the most common type of violence. Significant factors as age of the victims (c2 = 15.34; p = 0.038) and the assaulters (c2 = 27.66; p <0.001), and mental condition of the assaulter (c2 = 28.27; p = 0.003) were obtained. According to post hoc residual z test, nurses aged between 40 and 49 and over 60 y.o were more exposed to physical violence than other groups, while the aggressors were younger aggressors (19-30 y.o.) and over 60 ; wherears significant less frequent were cases of aggressors aged between 31 and 50 y.o.
Conclusion: A high exposure of nurses to WPV in northern Moroccan hospitals is noted. The significant factors of violence obtained must be considered for the control and prevention of WPV among nurses in Moroccan hospitals.
Keywords: Morocco; nurses; hospital; verbal violence; physical violence; workplace violence; questionnaire
Introduction
The Workplace violence (WPV) is a worldwide problem within the healthcare sector. The effect of this phenomenon on the performance of an organization makes it a serious issue that we should study in all dimensions. The World Health Organization classifies workplace violence into physical and non-physical violence [1]. This publication specifies that these categories of WPV include physical assault, homicide, verbal abuse, bullying/mobbing, sexual/racial harassment, and threatening behavior. The National Institute for Occupational Safety and Health also defines it as a violent act, including physical assaults and threats of assault directed toward persons at work or on duty [2]. Other classifications, based on the relationship between the two parties involved in the incident, are also known [3, 4].
The notified incidence of violence in the health sector constitutes almost a quarter of all the incidents of WPV perpetrated in all the other sectors [5]. Consequently, WPV affects the work demand [6], the quality of healthcare, and the psychological state of the health workers [7].
In health facilities, 52.2% to 87.3% of health workers reported an experience of physical violence during their careers. Many more are threatened or exposed to verbal abuse. Patients and visitors are responsible for a great number of incidents [8]. Pich and Roche [8] confirmed that all the categories of health workers are concerned with WPV, but the highest rate of reported cases is observed among nurses and midwives in both public and private sectors and different geographic areas.
According to Cebrino et al, a worldwide bibliometric analysis reveals that the number of studies on WPV perpetrated against healthcare personnel grew between 1992 and 2019 [9]. Most reported WPV factors include psychological setting, illness of the perpetrators, miscommunication, younger nurse age, and alcohol use [10]. Chapman et al. [11] identified the predicting behaviors that must alert nurses on the occurrence of a WPV incident and then help them manage it. It was found that nurses suffer from WPV approximately two times more than physicians [12]. Despite the growing interest and the high number of studies published on WPV perpetrated against healthcare workers, this phenomenon is still underestimated. According to Kvas and Seljak, this is due to unreported cases and a large tolerance of WPV among health professionals [13].
In Morocco, non-medical health professionals represent 56% of health human resources; physicians represent 22% and administrates 22% [14]. The first category of health personnel includes Nurses (69%), Midwives (16%), Health technicians such as medical analysis laboratory and imagery personnel (11%), rehabilitation personnel (4%), and social worker (1%). According to the same document, 60% are female gender and 40% are male gender.
The first study conducted in Morocco on WPV in the healthcare sector was published in 2010 [15]. Moroccan healthcare workers are at high risk of exposure to WPV [16]. A report on the Moroccan working environment showed a higher workload and higher stress levels in the workplace [17]. Additionally, the same authors observed the absence of an ergonomic workplace, the non-availability of resources, and the ignorance of consequences of exposure to violence in the Moroccan healthcare sector. The reality is that few data are available and published on WPV in the Moroccan health sector.
For a better control and prevention of this phenomenon, it is important to know the occurrence and the factors associated with WPV perpetrated against nurses in Moroccan hospitals. To intervene and manage these incidents as quickly as possible, nurses need to be able to know and identify factors that can alert them to the possibility that a violent incident may occur [11]. This interest is in line with policies issued by Moroccan Health authorities. Additionally, Moroccan high governmental authorities and health authorities adopted laws and procedures to be applied in the case of any kind of aggression facing health professionals in their workplace. The authorities adopted this strategy during the year 2021.
The study questions are 1) What is the occurrence of the WPV in northern region hospitals of Morocco and 2) What are the factors related to WPV among nurses exposed to WPV in the hospitals of this area. Only 1 study has investigated this phenomenon in Morocco, specifically in the emergency unit of the national hospital located in Rabat city.
Objectives
The aims of this study were 1) to assess the WPV perpetrated against nurses in hospitals of the northern area of Morocco and 2) to identify the related factors.
Materials and Methods
Study area, study design and tool
We performed a cross-sectional field study. The study was conducted in a geographic area located in the north-west of Morocco (35.2630° N, 5.5617° W). Mediterranean Sea borders this area from the north and the Atlantic Ocean from the west. Rabat-Salé- Kénitra region and Fès-Meknès region border the area from the southeast and the east. A total of 12.5 million of inhabitants live in this area. The estimated number of non-medical health professionals working in the hospitals of this area was 1749.
To achieve the aims of our study, we adopted a self-reported questionnaire, Violent Incident Form (VIF). This questionnaire was initially developed by Arnetz [18], and used after that in several WPV survey studies [7, 19, 20]. The VIF assesses verbal violence and physical violence (spitting, biting, kicking, scratching/pinching, slapping/hitting punching, pushing, restraining, use of object or weapon, others). It reports also the circumstances, perpetrator, reactions and consequences of the violence. The questionnaire consists of 18 questions with binary (Yes/No) or multiple-choice responses. One section describes the characteristics of the victim and the aggressor. The other section describes the related factors of WPV experienced by nurses over the preceding 12 months.
Authorizations and ethical consideration
In accordance with the Declaration of Helsinki, we first obtained the authorization of the Regional Health Authorities and the approval of the Ethics Committee (protocol code 28/2021). Anonymous identification, data protection, and voluntary participation were ensured. Additionally, all the participants in the study gave their written agreement to participate in the survey by filling out a consent form.
Subjects, sampling, recruitment and data collection procedure
Participants were enrolled according to these inclusion criteria: being nurse and working for at least 2 years in the hospital as full-time worker. We excluded nursing students and nursing trainees. We unexpectedly visited the hospitals of the study area. The procedure to recruit the eligible subjects is the following. We went to each nurse’s supervisor in each hospital and asked him to distribute, among the eligible nurses, the pack of supports and tools of this survey. The individual pack contained the VIF questionnaire, along with a cover letter and a consent form. The sample size was estimated by Bernoulli sampling [21], according to the following formula.

We considered the central value of the prevalence interval as the representative value of the interval, i.e. 70%, IC=95%, Z-score 1.96 and a Δ=5%. In this way the minimum size was estimated equal to 323 nurses. We expanded the estimated sample up to 379 to reduce any statistical bias, due to any questionnaires not completed or with missing data. In this regard, we distributed 391 questionnaires. We recruited 387 volunteers and consenting nurses. The nurses were asked to describe the most significant WPV incident that they experienced during the 12 months preceding the study, as indicated in the VIF. Among the volunteers, 379 nurses experienced a WPV incident. They completed the questionnaire independently and anonymously. Afterwards, they deposited the completed questionnaires in a sealed box that we previously distributed in each hospital. Then, we collected the boxes 15 days after. The period of data collection lasted from October to December 2021.
Statistical analysis
We analyzed the data using the package IBM SPSS Statistics for Windows, version 21.0. Armonk, NY: IBM Corporation. Multiple responses were possible on the section of the checklist dealing with type of violence and other variables. The type of violence as dependent variable was categorized into verbal violence, physical violence (spitting, biting, kicking, scratching/pinching, slapping/hitting, punching, pushing, restraining, use of object or weapon) and Both, based on the approach of these authors [22]. Descriptive statistics were conducted to determine the characteristics of the study sample. Data were presented as frequencies and percentages. The multicomparison chi-square test was used to define significant differences among groups. Fisher’s exact test was used where the chi-square test was not appropriate. If the statistical test considering all options of responses for an item was positive (p-value <0.05), then the highest percentage value for an option was compared statistically to the sum of the percentages of all the other options, in order to point out probable triggers of WPV. Additionally, we performed a post hoc multiple chi-square test or multiple Fisher’s exact test (if the chi-square test or Fisher’s exact test were significant) to identify significantly more or less frequent categories. We applied the 2 tailed residual z test for significant variables. A value higher than +1.96 standard deviations is considered significant. The critical value is the same for each tail. All tests with p< 0.05 were considered significant.
Results
Demographic characteristics of the victims and the assaulters
We distributed the questionnaires to 391 nurses working in hospitals located in the study area. In total, 387 nurses informed the questionnaire with 98% response rate. Among the respondents, 97% of the nurses experienced at least one WPV episode during the preceding year. The demographic characteristics of the assaulted nurses and the assaulters are illustrated in Table 1.

Table 1. Demographic data of victims and WPV perpetrators in hospitals, northern region of Morocco, 2021.
Our data showed that the majority of the nurses (78%) aged less than 39 years old. The sex ratio (Male-to-Female) was 0.7. Most of the victims were females (60%), whereas most of the assaulters were male (70%). The majority of assaulters aged between 31 and 50 years old.
Violence pattern among nurses
The data on the type of violence facing nurses are presented in Table 2. The most common type of violence was verbal violence (70 %). The main forms of physical violence were Slapping/Hitting (29 %) and Kicking (26 %).

Table 2. Type of WPV facing nurses (n=379) in northern region hospitals of Morocco, 2021.
Profile of the victims and the aggressors
The data on the profile of the victims, aggressors and factors related to WPV are illustrated in Table 3.
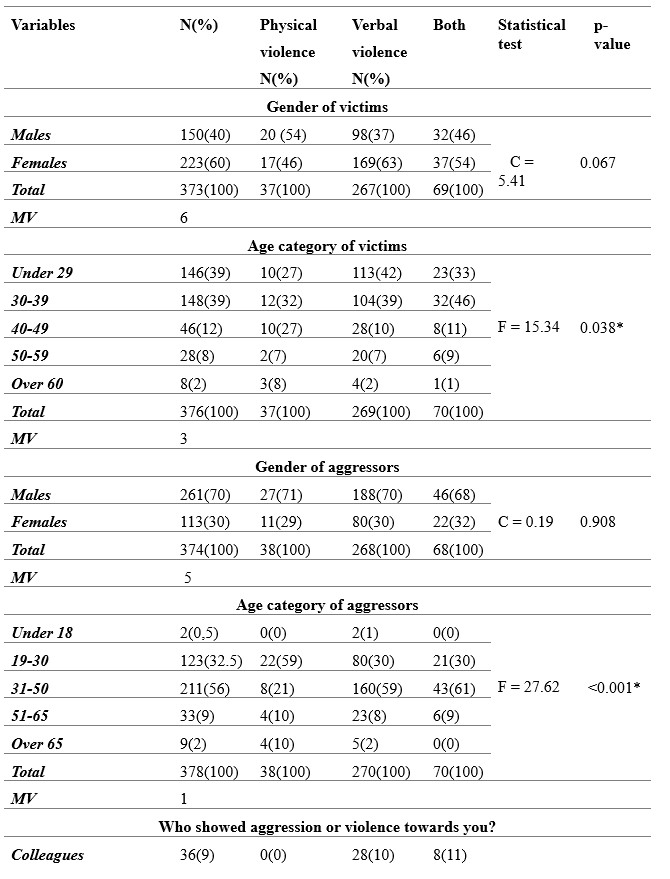

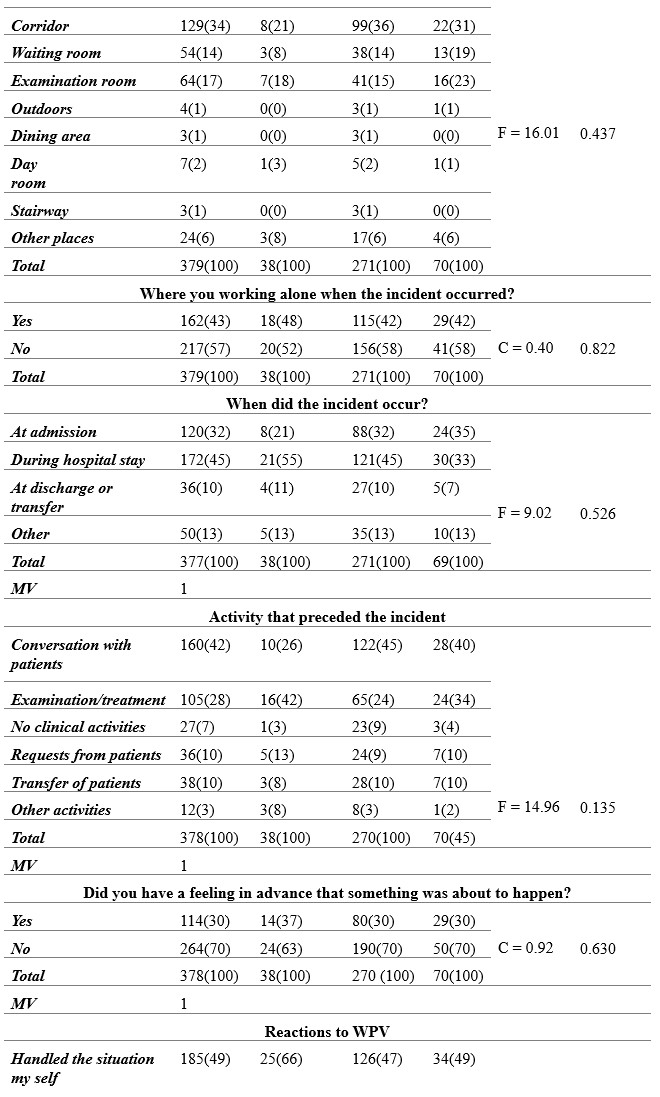
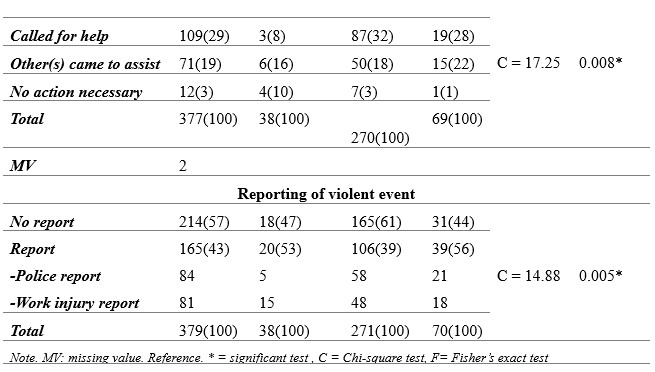
Table 3. Circumstances and factors associated with violence using VIF questionnaire among nurses, Morocco, 2021.
The data on the post hoc statistics, based on 2 tailes residual z test for significant variables previously obtained using Chi-square or Fisher tests, are reported in Table 4.
Considering the profile of the victims, our results indicated that nurses having less than 39 years old were significantly more exposed to WPV than the elders (c2 = 15.34; p = 0.038). Focusing on 40-49 and 60 or older age groups of the victims, the standardized residuals are significant for physical violence. This finding suggests a significant positive association between 40-49 (z = 2.6) and 60-older age groups (z = 2.5) and the physical violence.
Regarding the aggressors, we found that males perpetrate more violence than females. Neverthless, this result was not statistically significant. We observed that the age category of the aggressor was significantly associated with violence (c2 = 27.66; p < 0.001). The aggressors belonging to 31-50 years old age category perpetrated more WPV than other age categories. Comparing this age category to the others, we found that this interval can be considered as a trigger of WPV (p < 0.001).
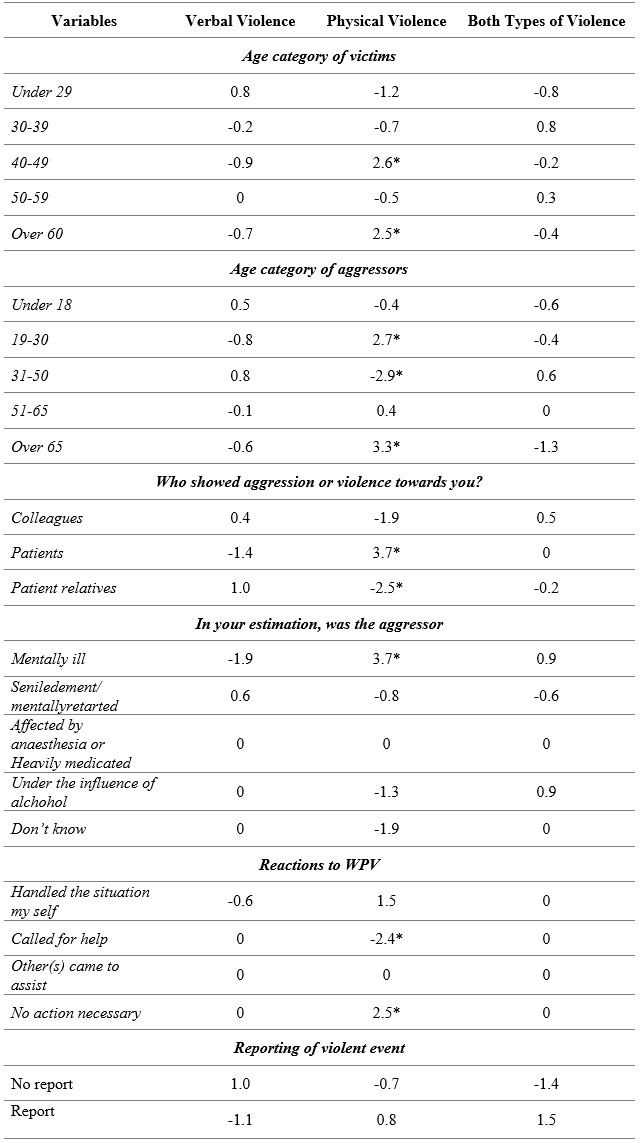
Table 4. Post hoc statistics, based on 2 tailes residual z test applied to significant risk factors of WPV experienced by nurses, Morocco 2021. Significant z values were marked with an asterisk.
Additionally, post hoc statistics based on residual standardized z test, were significant for 19-30 and over 65 age groups of the aggressors (z = 2.7 and z = 3.3 respectively) for physical violence. This result indicates a significant positive association between these age grousp and physical violence. At the opposite, we obtained a significant negative association between 31-50 age group and physical violence (z = – 2.9).
With regards to the nature of the relationship between the parties involved in the incident, the data showed that this factor was strongly and significantly associated with violence (c2 = 28.17; p < 0.001). The most frequently notified profile of the aggressor was the patient’s relatives (50%). Comparing this profile of the perpetrator to the others, we found that patient’s relatives is probably a trigger of WPV (p = 0.001). Moreover, according to post hoc statistics based on residual standardized z test, we obtained that the profile ‘Patients’ was positively associated with physical violence (z = 3.7) and ‘Patients relatives’ profile was negatively associated with physical violence (z = – 2.5).
Considering the emotional and psychological state of the aggressor, it was significantly associated with violence (c2 = 28.28; p = 0.003). Comparing the state of the aggressor ‘Mentally ill’ to the other states, we found that the mentally ill aggressor can be considered as a significant alerting factor of violence (p = 0.006). On the other hand, the standardized residual z test indicated that ‘Mentally ill’ aggressor’s state is positively associated with physical violence (z = 3.7). This finding suggest that mentally ill aggressors are more likely authors of physical violence than the aggressors with other mental and psychological disorders.
Circumstances and factors associated with WPV
Considering the circumstances of the violence, the time of violent incidents was not significantly associated with WPV. Nevertheless, we observed that aggressive episodes occurred with a high frequency throughout daily shift (68%). About the place of WPV occurrence, the corridors were the most frequently signalized place (34%) than other places. However, the result was not statistically significant. Regarding the situation if the victim was working alone or not, the frequency of violence was slightly high (57%) when the victim was not working alone.
Looking for which step during the patient journey the incidents occur mainly, we observed that most of the events occurred during the hospital stay (45%) and at admission (32 %). Nevertheless, the results were not statistically significant.
Considering the activities preceding the incident, we found that ‘Conversation with the patient’ was the most frequent (42%), followed by ‘Examination/treatment’ (28%).
Prediction, reactions and management of workplace violence
Considering the feeling in advance that something was about to happen, most of the victims (70%) responded by No. This result indicates that the great majority of the nurses were not able to identify suspicious behaviors.
Regarding the reactions to WPV, half of the victims opted for handling the situation themselves and this result was statistically significant (c2 = 17.96; p = 0.008). Comparing the option ‘Handled the situation my self’ to all the other options, we found that this option is a probable trigger of WPV (p = 0.088). Post hoc residual statistics showed a negative association of the option ‘Call for help with physical violence (z = -2.4). About the option ‘No action necessary’, residual statistics showed a positive association with physical violence. in general, the results on the reactivity of the nurses express a non-responsiveness.
Our data showed a low reporting level of the violence occurring in Moroccan hospitals. We observed that 57% of the nurses did not formally report the violence in a police report or a work injury report. This result was statistically significant (c2 = 14.9; p = 0.005). Finally, Data indicates that the most frequent negative effect of WPV on the nurses was the psychological problem (74%).
Discussion
In this study, we have explored the occurrence of workplace violence among nurses and the associated factors in northern region hospitals of Morocco. It presents the first data on occupational violence facing nurses in Morocco to our knowledge. We obtained a high exposure to WPV among nurses working in this area. This finding was similar to the data reported in these studies [6, 11, 23-28]. Moreover, comparing the WPV frequency between different studies is difficult [6, 20, 23]. This difficulty may be due to the different case definition of different categories of violence adopted by the authors, the use of different tools, and the application of different study designs. In addition, individual differences in perception of violence forms can lead to different results. Overall, verbal violence was more frequent than physical violence. In addition, Arnetz et al report that the violence pattern facing healthcare professionals is different between different health units providing different kind of healthcare [18].
Profile of the victims and the aggressors
Focusing on the age of the victims, we observed that younger nurses, i.e., under 39 years old, faced more workplace violence than elderly nurses. This finding is consistent with the literature [10, 29, 30]. We suggest the insertion of a training module on the management and prevention of WPV in the nursing academic course and the first years after employment in Moroccan health facilities.
Considering the gender of the aggressors, despite the fact that this factor was not statistically significant, but the proportion of male aggressors was very high (70%) compared to females (30%). This item was reported as a factor of violence in these studies [19, 31, 32]. Regarding the assaulter’s age, we found that it was a statistically significant factor of violence. This finding is consistent with the last cited studies.
The significantly most incriminated assaulters were the patients’ relatives. This result is supported by these studies [24, 26, 28, 32-35]. This finding may be linked to the fact that patients and their relatives have high expectations of healthcare professionals, and when they perceive that their needs are not satisfied, they may adopt aggressive attitudes [3, 36]. According to post hoc residual z test, significant statistics showed that nurses aged between 40 and 49 and over 60 y.o were more exposed to physical violence than other age categories, while the aggressors aged between (19-30 y.o.) and over 60. In addition, significant less frequent were cases of aggressors aged between 31 and 50 y.o.
These victims and aggressors age categories must be considered by the healthcare professionals in the management and the control of WPV.
Circumstances and factors associated with WPV
Despite the fact that our findings were not statistically significant, most of the incidents occurred during daily shifts. This finding is in accordance with these studies [37, 38]. Other authors obtained contradictory data [28, 32].
About WPV place, the most frequently signalized place was the corridors (35%). These data are consistent with these studies [29, 10]. The fact that the results on the circumstances were not statistically significant may be linked to the great number of the response options, the reduced number of the participants in each response option, and the limited sample size.
Prediction, reactions and management of workplace violence
Considering the feeling in advance that an incident will occur, the majority of the incidents were not expected by the nurses. This result is in accordance with the data found in the literature on the predictive factors of WPV [39]. This finding expresses a need to sensitize and inform the nurses about workplace violence. Regarding the consequences of WPV, the most negative effect was psychological problems. This result is in line with the findings of the previously cited study.
Beside this result, we obtained a low reporting of the violent incidents. This finding is in accordance with the results obtained by these authors [40, 41]. It is probably due to the lack of a notification system of WPV, the lack of information on how to report the incident, the ignorance of labor laws and rights, and the victims may believe that the reporting is useless or the act of violence is not considered a crime.
Conclusions
A high exposure of nurses to WPV in northern Moroccan hospitals is noted. Verbal violence is more predominant than physical violence. Considering the profile of the assaulters, the majority are male and the most incriminated are the patients’ families. Significant risk factors such as age of the victims and the assaulters were obtained. The mental condition of the assaulter is significantly associated to violence perpetrated against nurses. These results should alert policymakers about the violent workplace incidents committed in Moroccan hospitals. We recommend the conduction of large-scale studies to inform policymakers about the exact magnitude and factors of WPV in other hospitals and non-hospital settings in all regions of the kingdom. Then the implementation of a program on the prevention and management of WPV for nurses and other categories of healthcare professionals. Another preventive aspect is the setting of a WPV notification system in hospitals to help operative managers on time to address the factors that lead to workplace violence.
Limitations
Despite the fact that most of our findings are supported by the data published on workplace violence, our study has some limitations. The main limitation is that VIF asks about violence experienced the past year only. Another limitation about the severity of the violence is related to the fact that the VIF reports if the participant experienced a violent event or not, but the participant is not asked about how often he faced incidents during the year. Finally, since our study was conducted in the northern area only, our findings are not generalized to the whole population of nurses working in Moroccan hospitals or other healthcare facilities. In order to have representative results on the violence through all the country, further studies must be extended to a larger period of time and cover all the regions of Morocco.
Funding: This research received no external funding.
Institutional Review Board Statement: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of “Comithé d’Ethique pour la Recherche Biomédicale CERBO (protocol code 28/2021 and date of 11/10/2021).
Informed Consent Statement: Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement: Data is unavailable due to privacy and national restrictions.
Conflicts of Interest: The authors declare no conflict of interest.
Author Contributions: Conceptualization, S.O (Safae Ouma); N.B (Nabil Benomar) and N.R (Nabila Rouahi); Methods, S.O; N.B and N.R; Software, S.O and N.R; Validation, S.O; N.B; M.L.LL (Maria LeyreLavilla Lerma) and N.R; Formal analysis: MLLL; Investigation, S.O; Resources, S.O; N.B and N.R; Data curation, S.O; N.R and N.R; Writing—Original draft preparation, S.O and N.R; Writing—review and editing, S.O; N.B; MLLL and N.R; Visualization, S.O; N.B; MLLL and N.R; Supervision, N.B and N.R; Project administration, N.B and N.R; Funding acquisition, None. All authors have read and agreed to the published version of the manuscript.
Acknowledgments: We would like to thank the nurses who participated in this research and staff of the hospitals who facilitated the fluent conduction of the study for their efforts in the data collection.
References
- Krug, E. G., Dahlberg, L. L., Mercy, J. A., Zwi, A. B., Lozano, R. (2002). World report on violence and health. World Health organization. https://apps.who.int/iris/handle/10665/42495.
- National Institute for Occupational Safety and Health. (2002). Violence : Occupational hazards in hospitals. http://doi.org/10.26616/NIOSHPUB2002101.
- Phillips, J. P. (2016). Workplace Violence against Health Care Workers in the United States. New England Journal of Medicine, 374(17), 1661‑1669. https://doi.org/10.1056/NEJMra1501998.
- Wassell, J. T. (2009). Workplace violence intervention effectiveness : A systematic literature review. Safety Science, 47(8), 1049‑1055. https://doi.org/10.1016/j.ssci.2008.12.001.
- Tuncel, E. K., Dundar, C., Sunter, A. T., Canbaz, S., &Peksen, Y. (2009). Violence towards primary healthcare workers in Samsun, Turkey. 18.Conference: 12th World Congress on Public Health World Health Organization
- Park, M., Cho, S.-H., & Hong, H.-J. (2015). Prevalence and Perpetrators of Workplace Violence by Nursing Unit and the Relationship Between Violence and the Perceived Work Environment : Workplace violence against nurses. Journal of Nursing Scholarship, 47(1), 87‑95. https://doi.org/10.1111/jnu.12112.
- Khalil, M., &Alameddine, M. (2020). Recruitment and retention strategies, policies, and their barriers : A narrative review in the Eastern Mediterranean Region. Health Science Reports, 3(4). https://doi.org/10.1002/hsr2.192.
- Pich, J., & Roche, M. (2020). Violence on the Job: The Experiences of Nurses and Midwives with Violence from Patients and Their Friends and Relatives. Healthcare, 8(4). 522. http://doi.org/10.3390/healthcare8040522.
- Cebrino, J., &Portero de la Cruz, S. (2020). A worldwide bibliometric analysis of published literature on workplace violence in healthcare personnel. PLOS ONE, 15(11), e0242781. https://doi.org/10.1371/journal.pone.0242781.
- Kamchuchat, C., Chongsuvivatwong, V., Oncheunjit, S., Yip, T. W., &Sangthong, R. (2008). Workplace Violence Directed at Nursing Staff at a General Hospital in Southern Thailand. Journal of Occupational Health, 50(2), 201‑207. https://doi.org/10.1539/joh.O7001.
- Chapman R, Perry L, Styles I, Combs S. Predicting patient aggression against nurses in all hospital areas. British Journal o Nursing. 2009. 18(8) : 476 – 483.
- Partridge, B.; Affleck, J. Verbal abuse and physical assault in the emergency department: Rates of violence, perceptions of safety, and attitudes towards security. Australas. Emerg. Nurs. J. 2017, 20, 139–145. [CrossRef]
- Kvas, A., & Seljak, J. (2014). Unreported workplace violence in nursing : Unreported workplace violence in nursing. International NursingReview, 61(3), 344‑351. https://doi.org/10.1111/inr.12106.
- Human Resources report of the Ministry of Health, 2016.
- Belayachi, J., Berrechid, K., Amlaiky, F., Zekraoui, A., &Abouqal, R. (2010). Violence toward physicians in emergency departments of Morocco : Prevalence, predictive factors, and psychological impact. Journal of Occupational Medicine and Toxicology, 5(1), 27. https://doi.org/10.1186/1745-6673-5-27.
- Giurgiu DL., Jeoffrion C., Roland-Lévy C, Grasset B., Brigitte Dessomme BK., Moret L., Roquelaure Y., Caubet A., Verger C., El Houssine Laraqui C., Lombrai Pl., Geraut C, and Tripodi D. 2016. Wellbeing and occupational risk perception among health care workers: a multicenter study in Morocco and France. J.Occup Med Toxicol. 2016; 11: 20. http://doi.org/10.1186/s12995-016-0110-0.
- Semlali H. (2010). The Morocco Country Case Study: Positive Practice Environments. Morocco Case Study: Health Care Environments in Morocco. Global Health Workforce Alliance, WHO, Geneva. http://www.who.int/workforcealliance/knowlege/resources/ppemorocco/en/index.html
- Arnetz JE, Arnetz BB, Söderman E. Violence toward health care workers. Prevalence and incidence at a large, regional hospital in Sweden. AAOHN J. 1998 Mar;46(3):107-14. PMID: 9582726.
- Ferri, P., Silvestri, M., Artoni, C., & Di Lorenzo, R. (2016). Workplace violence in different settings and among various health professionals in an Italian general hospital : A cross-sectional study. Psychology Research and Behavior Management, 9, 263‑275. https://doi.org/10.2147/PRBM.S114870.
- Magnavita, N., &Heponiemi, T. (2012). Violence towards health care workers in a Public Health Care Facility in Italy: A repeated cross-sectional study. BMC Health Services Research, 12(1), 108. https://doi.org/10.1186/1472-6963-12-108.
- Strand, M. M., Estimation of a population total under a “Bernoulli sampling” procedure. The American Statistician, 1979. 33(2), 81-84.
- Khalid GM, Idris UI, Jatau AI, Wada YH, Adamu Y, Ungogo MA. Assessment of occupational violence towards pharmacists at practice settings in Nigeria. Pharmacy Practice. 2020 Oct-Dec;18(4):2080. https://doi.org/10.18549/PharmPract.2020.4.20.
- Ayranci, U., Yenilmez, C., Balci, Y., &Kaptanoglu, C. (2006). Identification of Violence in Turkish Health Care Settings. Journal of Interpersonal Violence, 21(2), 276‑296. https://doi.org/10.1177/0886260505282565.
- Kitaneh, M., &Hamdan, M. (2012). Workplace violence against physicians and nurses in Palestinian public hospitals : A cross-sectional study. BMC Health Services Research, 12(1), 469. https://doi.org/10.1186/1472-6963-12-469.
- Alsaleem, S., Alsabaani, A., Alamri, R., Hadi, R., Alkhayri, M., Badawi, K., Badawi, A., Alshehri, A., & Al-Bishi, A. (2018). Violence towards healthcare workers : A study conducted in Abha City, Saudi Arabia. Journal of Family & Community Medicine, 25, 188‑193. https://doi.org/10.4103/jfcm.JFCM_170_17.
- Hamdan, M., & Abu Hamra, A. (2015). Workplace violence towards workers in the emergency departments of Palestinian hospitals : A cross-sectional study. Human Resources for Health, 13(1), 28. https://doi.org/10.1186/s12960-015-0018-2.
- Rafeea, F., AlAnsari, A., Musbah Abbas, E., Elmusharaf, K & Abu Zeid, M. (2017). Violence toward health workers in Bahrain Defense Force Royal Medical Services´ emergency department. Open Access Emergency Medicine, 9, 113‑121. https://doi.org/10.2147/OAEM.S147982.
- Zafar, W., Siddiqui, E., Ejaz, K., Shehzad, M. U., Khan, U. R., Jamali, S., &Razzak, J. A. (2013). Health Care Personnel and Workplace Violence in the Emergency Departments of a Volatile Metropolis : Results from Karachi, Pakistan. The Journal of Emergency Medicine, 45(5), 761‑772. https://doi.org/10.1016/j.jemermed.2013.04.049.
- Adib, S. M., Al-Shatti, A. K., Kamal, S., El-Gerges, N., & Al-Raqem, M. (2002). Violence against nurses in healthcare facilities in Kuwait. International Journal of Nursing Studies, 39(4), 469‑478. https://doi.org/10.1016/S0020-7489(01)00050-5.
- Alameddine, M., Mourad, Y., &Dimassi, H. (2015). A National Study on Nurses’ Exposure to Occupational Violence in Lebanon : Prevalence, Consequences and Associated Factors. PLOS ONE, 10(9), e0137105. https://doi.org/10.1371/journal.pone.0137105.
- Gerberich, S. G. (2004). An epidemiological study of the magnitude and consequences of work related violence : The Minnesota Nurses’ Study. Occupational and Environmental Medicine, 61(6), 495‑503. https://doi.org/10.1136/oem.2003.007294.
- Lei, Z., Yan, S., Jiang, H., Feng, J., Han, S., Herath, C., Shen, X., Min, R., Lv, C., & Gan, Y. (2022). Prevalence and Risk Factors of Workplace Violence Against Emergency Department Nurses in China. International Journal of Public Health, 67, 1604912. https://doi.org/10.3389/ijph.2022.1604912.
- Algwaiz, W. M. (2012). Violence exposure among health care professionals in Saudi public hospitals. Saudi Med J. 2012. 7.
- Muñoz del Carpio-Toia, A., Begazo Muñoz del Carpio, L., Mayta-Tristan, P., Alarcón-Yaquetto, D. E., & Málaga, G. (2021). Workplace Violence Against Physicians Treating COVID-19 Patients in Peru : A Cross-Sectional Study. The Joint Commission Journal on Quality and Patient Safety, 47(10), 637‑645. https://doi.org/10.1016/j.jcjq.2021.06.002.
- Sachdeva, S., Jamshed, N., Aggarwal, P., & Kashyap, S. (2019). Perception of workplace violence in the emergency department. Journal of Emergencies, Trauma, and Shock, 12(3), 179. https://doi.org/10.4103/JETS.JETS_81_18.
- Usman, N., Dominic, B., Nwankwo, B., Nmadu, A., Omole, N., & Usman, O. (2022). Violence towards health workers in the workplace : Exploratory findings in secondary healthcare facilities in Kaduna metropolis, Northern Nigeria. Babcock University Medical Journal, 5(1). https://doi.org/10.38029/babcockunivmedj.v5i1.118.
- Albashtawy, M., Al-Azzam, M., Rawashda, A., Batiha, A.-M., Bashaireh, I., &Sulaiman, M. (2015). Workplace Violence Toward Emergency Department Staff in Jordanian Hospitals : A Cross-Sectional Study. Journal of Nursing Research, 23(1), 75‑81. https://doi.org/10.1097/jnr.0000000000000075.
- Fernandes, C. M. B., Raboud, J. M., Christenson, J. M., Bouthillette, F., Bullock, L., Ouellet, L., & Moore, C. F. (2002). The effect of an education program on violence in the emergency department. Annals of Emergency Medicine, 39(1), 47‑55. https://doi.org/10.1067/mem.2002.121202.
- Alshahrani, M., Alfaisal, R., Alshahrani, K., Alotaibi, L., Alghoraibi, H., Alghamdi, E., Almusallam, L., Saffarini, Z., Alessa, S., Alwayel, F., Saffarini, L., Alrawdhan, A., Mapusao, C., Asonto, L. P., Alsulaibikh, A., &Aljumaan, M. (2021). Incidence and prevalence of violence toward health care workers in emergency departments : A multicenter cross-sectional survey. International Journal of Emergency Medicine, 14(1), 71. https://doi.org/10.1186/s12245-021-00394-1.
- Garg, R., Garg, N., Sharma, D.K., Gupta, S. (2019). Low reporting of violence against health-care workers in India in spite of high prevalence. Medical Journal Armed Forces India. 75. 211-215. doi: 10.1016/j.mjafi.2018.11.011.
- Alfuqaha O., Albawati N., Alhiary S., Alhalaiqa F., Haha M., Musa S., Shunnar O and AL Thaher Y 5. (2022). Workplace Violence among Healthcare Providers during the COVID-19 Health Emergency: A Cross-Sectional Study. Behav. Sci. 2022, 12, 106. https://doi.org/10.3390/bs12040106.
![]() This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.