The global incidence rate of cancer has risen from 12.7 million in 2008 to 19.3 million in 2020.1,2 Cancer causes significant morbidity and mortality worldwide, regardless of socioeconomic development.2 The majority of the deaths from cervical cancer occur in Sub-Saharan Africa, Melanesia, South America, and South-Eastern Asia.2–5 The age-standardised incidence rates ASR (25.6 per 100,000 population) and the cumulative risk (3.86%) of cervical cancer is highest in Africa compared to other continents.6 In 2020, the ASR per 100 000 women in Benin and Cameroon were 15.1 and 33.7 per 100 000 women respectively,7,8 and the cumulative risk of cervical cancer in ages 0-74 in both countries was 1.8% and 3.6% respectively.7,8 In 2018, cervical cancers attributable to Human Papilloma Virus (HPV) 16 and 18 accounted for an estimated 72% of cases globally.9,10
Cervical cancer can be prevented or detected early using the HPV vaccine and screening strategies. Indeed, the World Health Organisation (WHO) has a global strategy to eliminate cervical cancer.11 WHO’s target age for vaccination in girls is between the ages of 9-14 years, before the onset of sexual intercourse.12 A systematic review revealed that between 2006 and 2014, only 1% of low middle-income countries (LMICs) had HPV vaccination programs.13 Screening is recommended using cervical cytology alone every three years for women aged 21 to 29 years.14 For women aged 30 to 65 years, three-yearly cytology, five-yearly with high-risk human papillomavirus (hrHPV) testing, or both (co-testing) five yearly is recommended.14 Due to the difficulty in implementing screening programs because of poor infrastructures and funding in low-resource settings like Africa, the WHO recommends a screen-and-treat approach to allow for treatment based on the result of the screening test .15 Most African countries use visual inspection with acetic acid (VIA) and immediate treatment with cryotherapy, while some continue with the use of cytology-based screening or are examining HPV testing .15,16
Lifetime uptake data of cervical cancer screening in 55 LMICs countries (representing 72% of the world population), reveals that only 44% of women in the target age group have ever had the opportunity to get a cervical screening test, with values even lower in sub-Saharan Africa (country level median 16.9%; range 0.9% -50.8%) in contrast to more than 60% in High-Income Countries.17,18 WHO enjoins introducing HPV vaccination and expanding screening and treatment for effective cervical cancer prevention.19,20 Although cervical cancer incidence and mortality are high in low-resource settings including Africa, several potentially modifiable factors are implicated including a lack of awareness of the symptoms, and screening,21 poor communication, and inadequate media education.22 The present study explored levels of awareness of cervical cancer and cervical screening in two West African countries, Benin, and Cameroon. Awareness is an important first step in increasing engagement in screening and identifying characteristics of those with lower levels of awareness can assist in the development of targeted interventions.
Methods
Study design and setting
This study addressed the following research questions: (i) What is the level of awareness of cervical cancer in Benin and Cameroon? (ii) What is the level of awareness of cervical screening in Benin and Cameroon? (iii) Does the level of awareness of cervical cancer and cervical screening differ by demographic characteristics and engagement with media?
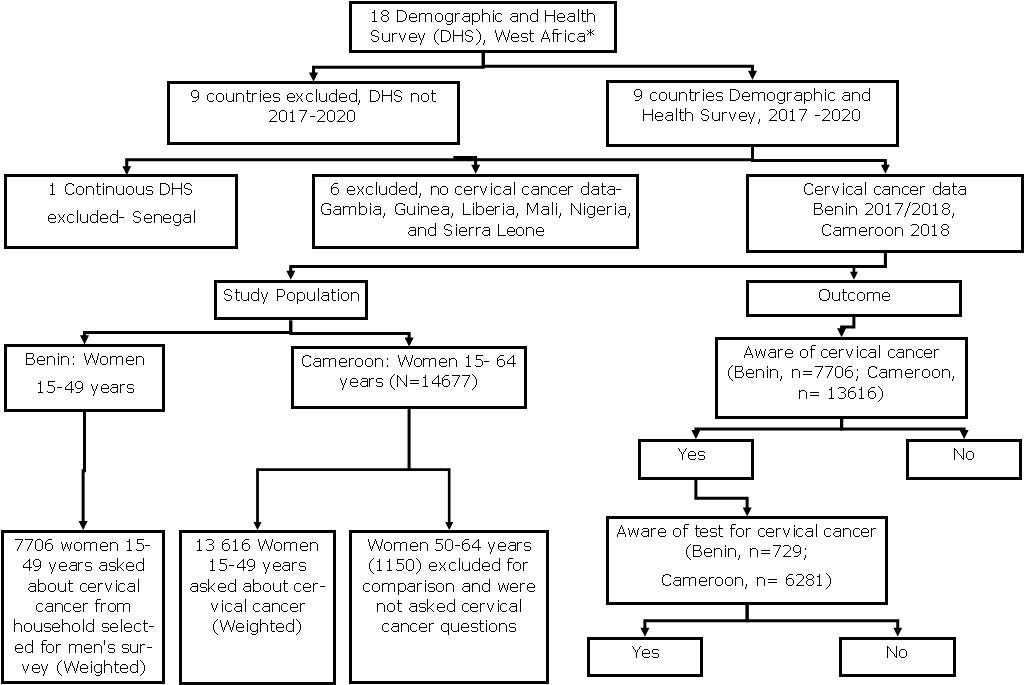
This study uses the Demographic and Health Survey (DHS) of two West African countries (Benin and Cameroon) conducted between 2017-2018 (Figure 1) (http://dhsprogram.com/).

Study population
We used the Encyclopaedia Britannica classification to define West Africa, with Cameroon included (https://www.britannica.com/place/western-Africa). This is also highlighted in the flow chart in Figure 1. The study used data from the Benin DHS 2017-18 and Cameroon DHS 2018. The surveys were conducted using a two-stage stratified cluster sampling method. Firstly, enumeration areas (EAs) in proportion to the size of the population or households using the latest census in the country were selected. Secondly, a new sample frame was created from the clusters, which were then stratified. Stratification was applied using urban and rural areas in both countries. Then household sampling is done to select eligible women, men, and children for the survey. The DHS office calculates the sample size for each country. Women of reproductive age (15-49 years) from Benin (15,928) and Cameroon (14,677) were surveyed. The response rate was 98.1% in Benin and 98.2% in Cameroon. In Benin, 7706 women 15- 49 years were asked questions on cervical cancer. A subgroup of women ages 50-64 years was also surveyed in Cameroon. These women were excluded from our study for the purpose of comparison and because they were not asked questions on cervical cancer.
Measures
Awareness of cervical cancer and screening
The outcomes of interest were whether women were aware of cervical cancer and cervical screening. The questionnaire was written in French. In both countries, the women were asked “Have you heard about cervical cancer?” and if ‘Yes’, they were then asked, “Have you heard of testing for cervical cancer of the uterus?” (https://translate.google.co.uk/). The responses were either ‘Yes’ or ‘No’ in both outcomes (Figure 1).
Demographic characteristics
We decided to use the 10-year age range as against the 5-year age range in the DHS study based on similar groupings in a Kenyan DHS analysis study,23 the low sample size of women with awareness of cervical cancer and screening and based on guidelines from the International Journal of Epidemiology on forming categories reported that "grouping should be mid-decade to mid-decade or in five-year age groups (e.g. 35–44 or 35–39, 40–44, etc., but not 20–29, 30–39 or other groupings) " - S A Reijneveld.24 The 10-year bands were from age 15 up to age 44 and then a 5-year age band up to age 49. Residential status was assessed as ‘urban’ or ‘rural’. For marital status, ‘never married’ were women who had never lived with a partner, the ‘currently married’ had married or were not formally married but were living with a partner, and the ‘formerly married’ women were widowed, divorced, or separated, or who had formerly lived with a partner. We grouped marital status as ‘never in a union’ and ‘currently/ formerly in a union’. Education assessed the highest achieved level and was grouped into four categories (no education, primary, secondary, higher) in line with the standard DHS report. The wealth quintile was measured as the relative wealth of the household based on ownership of assets such as radio, television, car, motorcycle, and materials for housing construction,25 and was divided into quintiles of poorest, poorer, middle, higher, and highest. The categories of religion were country-specific, but were broadly categorized as ‘Christians’, ‘Muslims’, ‘none’, and ‘others’. Occupation of the women were reported based on the standardized DHS format but were recategorized as ‘not working’, ‘non-professionals’, and ‘professionals’.
Media use
The frequency of reading the newspaper, watching television, listening to the radio, and using the internet in the last month was reported as, ‘not at all’, ‘less than once a week’, and ‘at least once a week’. For frequency of using the internet in the last month, women who use it almost every day were also included.
Ethics considerations
We obtained approval to use the data from the DHS program. The DHS program has ethical documentation on the privacy and confidentiality of all the respondents (http://dhsprogram.com/).
Statistical analysis
Univariate descriptive statistics were used to describe the demographic characteristics and media use. We summarised the categorical variables as weighted frequencies and percentages while the numerical variables were summarised as weighted means with a 95% Confidence Interval (CI). A Chi-square test was used to determine the association between demographic characteristics and the awareness of cervical cancer/screening. All variables were included in the multivariate analysis. Multivariate logistic regression was then used to determine the association between demographic characteristics and media use and awareness of cervical cancer and screening. The association was reported as odds ratio (OR), P values, and 95% CI.
We used the survey package in R version 4.1.1 (2021-08-10), to handle the survey design.26 Each country was analysed separately, and we applied sample weights for all the descriptive statistical analysis taking into consideration the weight variable (v005) after dividing it by 1,000,000: v005/1000000. The regression analysis considered the survey design by using the primary sampling unit (PSU), v021; secondary sampling unit (SSU), v002; sample strata, v025; and the weight.
The code used were:
Sample weight <- v005 (weight variable)/1000000
Survey design <- svydesign (ids = ~PSU+SSU, strata = ~v025, weights = ~sampleweight, data = data frame)
Results
A total of 21322 women of reproductive age were surveyed in Benin (n=7706) and Cameroon (n=13616) on awareness of cervical cancer and 7010 of these women were additionally asked about their awareness of cervical cancer screening. Table 1 shows the demographic characteristics of the women included in this study. The mean age was slightly lower in Cameroon (27.85 [95% CI 27.66-28.04]) than in Benin (28.39 [95% CI 28.15-28.62]). The majority of the women were within the age group 15 – 24 years in both countries, as high as 42.1% in Cameroon. Most women resided in a rural area, Benin (51.7%) and Cameroon (68.5%). More women in Benin (75.3%) than in Cameroon (54.8%) had either been married or were formerly married. More than half of the women (55.1%) in Benin had no education but 45.2% of women in Cameroon had secondary education. The richest wealth quintile had the highest proportion in Benin (22.5%) and Cameroon (23.8%). Most of the women were Christians, Benin (54.9%) and Cameroon (71.7%). The majority of the women were nonprofessionals, Benin (74.6%) and Cameroon (64.7%).
Most of the women in Benin did not read newspapers/magazines (90.4%; Table 2), watch television (62.5%), listen to the radio (42.8%), or use the internet (93.8%). Similarly, in Cameroon, the majority of the women did not read newspapers/magazines (80.5%), watch television (42.8%), listen to the radio (61.5%), or use the internet (73.5%; Table 2).
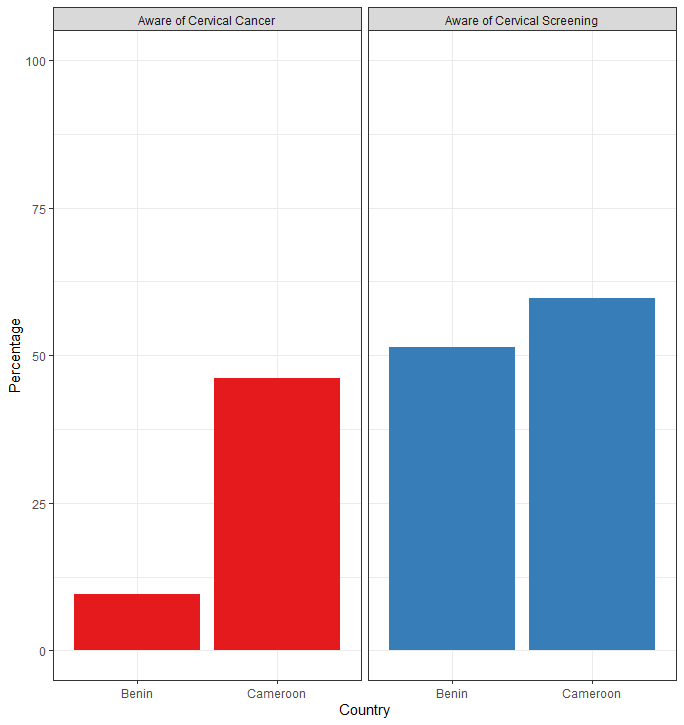
Figure 2 shows the awareness of cervical cancer and cervical screening among women. Only 9.5% of women in Benin were aware of cervical cancer but 46.1% were aware of cervical cancer in Cameroon. Around half of the women who were aware of cervical cancer in both countries were aware of cervical screening, Benin (51.4%) and Cameroon (59.7%).

In Benin awareness varied slightly by age but was very low (less than 11%), in Cameroon at least half of the women aged 25 and above were aware of cervical cancer. Awareness was higher among women in the urban areas in Benin (14.0%) and Cameroon (57.9%) (Table 1). Women who had never been in a union in Benin (10.5%) and Cameroon (47.9%) were more aware of cervical cancer than women who were currently/formerly married. Women with higher education in Benin (53.0%) and Cameroon (82.2%) were more aware of cervical cancer. Similar patterns were seen in the wealth quintiles in both countries, women in the richest wealth quintile had the highest proportion of awareness in Benin (20.8%) and Cameroon (71.0%). Christian women were more aware of cervical cancer in Cameroon (54.4%) than women following other religious faiths. Professional women were more aware of cervical cancer in both countries. Women who watch television (20.2%, 63.8%) and listen to the radio (14.0%, 64.2%) at least once a week and women who use the internet almost every day (47.9%, 77.2%) were more aware of cervical cancer in Benin and Cameroon respectively (Table 2). Overall, awareness of cervical cancer in Benin was very low compared with Cameroon.
In both countries, awareness of cervical screening slightly varied across the different age groups (Table 1). Women aged 25-34 years in Benin (58.4%) and women aged 45+ years in Cameroon (66.0%) had the highest level of awareness of cervical screening. Awareness of screening was higher in women in the urban areas of Benin (54.5%) and Cameroon (62.0%). Currently/formerly married women were more aware of screening than those who were never in a union in Benin (53.4%) and Cameroon (62.3%). Awareness of cervical screening increased with education level in both countries, women with higher education had greater awareness of cervical screening in Benin (71.6%) and Cameroon (74.4%). Awareness of cervical screening had no clear pattern of association with the wealth quintiles, but in both countries, women in the richest wealth quintile had the highest proportion of awareness in Benin (56.6%) and Cameroon (65.8%). Christian women in Benin (52.7%) were more aware of cervical screening but in Cameroon, women with other religions (68.9%) were more aware of screening. Professional women in both countries were more aware of cervical screening in Benin (63.5%) and Cameroon (65.9%).
Women in both countries who read newspapers/magazines, watched television, and listened to the radio at least once a week were more aware of cervical screening. The highest awareness was seen in women who read newspapers/magazines in Benin (65.7%) and Cameroon (67.7%). Women who used the internet almost every day in the last month were more aware of cervical screening in Benin (65.8%) and Cameroon (68.7%).
Univariate logistic regressions were conducted to provide a direct comparison with the multivariate logistic regressions (Table 3). In line with the results of the chi-square analysis (Tables 1 and 2), all the demographic characteristics and media use in both countries were significantly associated with awareness of cervical cancer except marital status. The results of the univariate analysis are shown in Table S1 in the online supplementary document. The multivariate logistic regression included the following variables in the adjusted model: age, residential status, marital status, education, wealth quintiles, religion, occupation, and frequencies of reading newspapers or magazines, watching television, listening to the radio, and using the internet in the last month.
In Benin, the odds of awareness of cervical cancer significantly increased from women aged 25-34 years (adjusted odds ratio, aOR=1.45, 95% confidence interval, CI=1.12-1.89) to women aged 45+ years (aOR=1.89, 95% CI=1.23-2.91) compared with women aged 15-24 (Table 3). The awareness of cervical cancer increased as the education levels increased in Benin, the odds were approximately 6 times higher ( OR = 6.04, 95% CI=3.34-10.91) in women with higher education than in women without education in the adjusted model. The middle and richest wealth quintiles in the adjusted model had significantly increased odds of awareness of cervical cancer (Table 3). Muslims in the adjusted model in Benin had significantly reduced odds of awareness (aOR=0.45, 95% CI=0.35-0.59,) than Christians. Being a professional woman in Benin increased the odds of awareness of cervical cancer (aOR=1.87, 95% CI=1.21-2.91). There was a significantly reduced odds ratio among women who read newspapers or magazines at least once a week (aOR=0.58, 95% CI=0.40-0.85). Benin women who watched television less than once a week had the highest odds (aOR=1.45, 95% CI=1.09-1.94) while women who listened to the radio at least once a week had the highest odds (aOR=1.31, 95% CI=1.02-1.68) than those who do not do that at all. There was a reduction in the odds among women who use the internet at least once a week, but the odds were significantly increased in women who used the internet almost every day, (aOR=3.61, 95% CI=2.45-5.32) (Table 3).
In Cameroon, the odds of awareness of cervical cancer increased as age increased in the adjusted models (Table 3). The odds were highest (aOR=2.91, 95% CI=2.36-3.60) among women aged 45+ years compared with women aged 15-24 years. Women who were currently /formerly married had a higher odd (aOR=1.25, 95% CI=1.10-1.43) than the unmarried in the adjusted model. Awareness of cervical cancer was approximately nine times higher (aOR=9.36, 95% CI=6.43-13.61) among women with higher education than women with no education. Similarly, awareness significantly increased as the wealth index increased in the adjusted model, approximately four times higher ( aOR=3.46, 95% CI=2.41-4.96) in the richest wealth quintile compared to women in the poorest wealth quintile. Muslims in the adjusted model had reduced odds of cervical cancer awareness (aOR=0.61, 95% CI=0.50-0.75) than Christians. The non-professional women had significantly increased odds in awareness (aOR=1.44 95% CI=1.27-1.63) compared with the not working women. There were significantly increased odds of cervical cancer awareness in Cameroon among women who read newspapers/magazines (aOR=1.27, 95% CI=1.09-1.48) and listened to the radio (aOR=1.21, 95% CI=1.06-1.39) less than once a week than those who did not. Also, among those that watch television at least once a week the odds increased (aOR=1.30, 95% CI=1.07-1.58). The odds were highest in those that used the internet almost every day (aOR=1.95, 95% CI=1.61-2.35).
In summary, older age, higher education levels, and frequent use of the internet in the last month were the factors with a clear significant association with increased cervical cancer awareness in the two countries (Table 3). Additionally in Cameroon, the wealth index had a clear significant association with awareness of cervical cancer.
In the chi-square analysis (Tables 1 and 2); age, education, wealth index, occupation, and media usage (television, radio, internet) were associated with awareness of cervical cancer screening in Benin whereas all the demographic characteristics and media use were associated with awareness of cervical cancer screening in Cameroon. The results of the univariate analysis are in Table S2 in the online supplementary document.
In Benin, the odds of cervical screening awareness were significantly higher (aOR=1.98, 95% CI=1.20-3.27) among women aged 25-34 years than aged 15-24 years in the adjusted model (Table 4). Women with higher education had four-fold increased odds of cervical screening awareness (aOR=4.42,95% CI=1.85-10.55) compared with women with no education in the adjusted model. Women who listened to the radio at least once a week in Benin had significantly increased odds of cervical screening awareness (aOR=1.73, 95% CI=1.04-2.88,) in the adjusted model.
In Cameroon, the odds of awareness of cervical screening significantly increased as age increased (Table 4). Women aged 45+ years had an increased odds of awareness compared with women aged 15-24 years (aOR=1.75, 95% CI=1.33-2.29). Women who were currently/formerly married had increased odds of cervical screening awareness (aOR=1.29, 95% CI=1.09-2.53) than women who had never been in a union in the adjusted model. The odds of cervical screening awareness significantly increased in women with secondary education (aOR=1.53, 95% CI=1.02-2.30,) to approximately three times higher (aOR=2.69, 95% CI=1.59-4.55) in women with higher education in the adjusted model. Using the internet almost every day in the last month significantly increased the odds of cervical screening awareness (aOR=1.35, 95% CI=1.10-1.67) in Cameroon.
In summary, older age, a higher level of educational achievement, and frequency of use of radio and the internet were significantly associated with the awareness of cervical screening.
Discussion
This study assessed the relationship between sociodemographic factors and awareness of cervical cancer and cervical screening in Benin and Cameroon, using the nationally representative DHS sample. Awareness of cervical cancer was significantly associated with older age, higher educational achievement, and frequent use of the internet in the last month in both countries, and with greater wealth quintiles in Cameroon. Awareness of cervical cancer screening was highest among women aged 25-34 years in Benin, women aged 45+ in Cameroon, and women with higher education in both countries. Age, education, and frequency of use of radio and the internet were also significantly associated with the awareness of cervical screening.
Awareness of cervical cancer varies across developing countries. In our study, awareness of cervical cancer was as low as 9.5% in Benin and 46.1% in Cameroon. In the Tanzania HIV and Malaria Indicators Survey, only 30.9% of women aged 15-49 years were unaware of cervical cancer, implying that more than 60% of the women were aware of cervical cancer in Tanzania.27 Predictors of cervical cancer awareness in that study included having more than secondary education, being affluent, having 1-4 children, and being aged 30-44 years.27 The risk of cervical cancer is increased in women with HIV; hence it is the most frequently detected cancer among women with HIV.28 Tanzania is one of the sub-Saharan African countries with higher prevalence of HIV compared to the prevalence of HIV worldwide.29 Therefore, women who participated in the Tanzania survey,27 could be more aware of cervical cancer because of the increased risk of cervical cancer associated with HIV . In a DHS analysis on the prevalence of awareness of cervical cancer in Zimbabwe (DHS 2015) and Benin (DHS 2017-18), awareness of cervical cancer in Zimbabwe was as high as 79.2%, much higher than our study and awareness in Benin (10.2%) was similar to our study.30 It appears the whole sample of women interviewed during the survey were used but, in our study, we analysed a sub-sample of women who were asked questions about cervical cancer. This is the reason a direct comparison cannot be made between our study and theirs. A population-based cross-sectional study of 1,090 women in Bangladesh, revealed an awareness of cervical cancer of 45.2% among women 15 to 75 years.31 This result is close to the prevalence in Cameroon in our study; although, the upper age limit in our study was only 49 years. Marital status, literacy, residential status, and socio-economic status were found to be associated with the level of knowledge of the women in the Bangladesh study.31 A nationally representative household survey that considered awareness of specific cervical screening tests such as smear tests among women also found low levels of awareness in Nepal (13%),32 and Indonesia (20%) .33 In our study, only women who were aware of cervical cancer were asked about awareness of cervical screening. Hence the reason why around half of the women in Benin (51.4%) and Cameroon (59.7%) were aware of cervical screening. Our study did not consider if the women were aware of the different methods of cervical screening. Cervical cancer screening programs in most African countries are less than the WHO target of 70% coverage, only 20% of the WHO countries in the African region have a national cervical cancer screening program which is mainly opportunistic.34 As of 2021, Benin and Cameroon had no national HPV vaccination program and no screening program for cervical cancer.7,8 The possibility that women will be aware of cervical cancer and screening is likely to be lower in countries without a national screening program. There is a need to increase the level of awareness of cervical cancer and screening among women in Benin and Cameroon through stakeholder involvement and the establishment of an implementable national cervical screening program.
The significant determinants of awareness of cervical cancer from our study included age, education, and frequency of using the internet in the last month in both countries and the wealth quintiles in Cameroon. Studies show that as a woman’s age increases she will possibly be more aware of the health issues that are associated with her reproductive health.30 Alongside advanced maternal age, studies show that having a formal education, using the internet, and having a professional/technical/managerial occupation significantly increased the odds of awareness of cervical cancer after adjusting for other confounders.30 Like our study, women aged over 45 years had the highest odds of cervical cancer awareness.30 Our study differs from Barrow et al30 in the forms of media used by women to get their information on health issues. In our study, women using the internet in the last month in both countries had better awareness of cervical cancer. Some previous studies did not specify the media use type, although some identified television as the best means of cervical cancer information delivery.35,36 Online social media platforms have been identified as a means for public health promotion but there is limited research on the effectiveness of social media in improving awareness of health topics.35 Inadequate information about cervical cancer could result in poor knowledge about the disease.36 It appears that studies agree that women get their health information from various forms of media, therefore, media use could improve awareness of cervical cancer.
Awareness of cervical cancer differed by wealth quintiles in Cameroon. In Ethiopia37 women with a higher average monthly income had better awareness of cervical cancer while in Kenya38 regional disparities in cancer awareness and screening utilization services are higher among the vulnerable regions with higher rural-urban wealth inequalities. Therefore, in most low-resource settings, age, education level, residential status, and socioeconomic status predict awareness of either cervical cancer or screening.27,30,31,33 There is a need to increase awareness among women of low socio-economic status to reduce the health inequalities that exist in their access to cervical cancer screening.
In Benin, an integrated strategic plan was developed to combat non-communicable diseases including cervical cancer.39 A similar plan was developed in Cameroon in 2020 for cancer control.16 As part of its primary prevention strategies, Cameroon employed awareness creation on special days and events, and in 2015 it completed a pilot phase to introduce the HPV vaccine for girls aged 9-13 years but the vaccine has not been added to the Expanded Program on Immunisation (EPI) since the pilot study.16 The cervical screening programs available in Cameroon are those organised by some public hospitals, faith-based organisations hospitals, National Committee for the Fight against Cancer (NACFAC), and Civil Society Organisations (CSOs).16 In both Benin and Cameroon, fewer than 1 in 10 women have had a cervical screening in the last 5 years.7,8 Awareness creation through active stakeholder participation is needed in both countries. Developing communication and behaviour change materials during the opportunistic program may help increase awareness in women.
Awareness of cervical screening affects recommendation. As observed in a Korean study where because of the low levels of cervical cancer prevention among mothers, they were unwilling to recommend screening and vaccination to their daughters.40 Secondly, accessibility and acceptability of cervical cancer prevention are affected by the level of knowledge and awareness. A study in Mali reported low levels of awareness but a high willingness to participate in screening programs.41 Even though one cannot ascertain that the high figures recorded for willingness results in actual participation in cervical screening. Among African women residing in the UK, awareness about cervical screening was reportedly low. Those born in the UK had significantly higher knowledge of cervical cancer risk factors with higher educational qualifications and older age.42 This may be due to the increased awareness creation that is in place in many high-income countries. An important barrier to participation in cervical screening is a lack of awareness about cervical cancer and screening.43,44 As seen in the literature, low levels of awareness of cervical cancer and screening affect the success of cervical screening implementation. Because low awareness affects recommendation, and willingness to participate in screening, there is a need to develop educational programs that will improve the knowledge of women about cervical cancer and screening. Healthcare providers should enlighten their patients on cervical cancer prevention because, in many African countries, they are usually the first point of call for most women attending the health facility.
Study Limitations
Our study used a large nationally representative sample, it is a cross-sectional study and causality cannot be established but the results are generalisable to women of reproductive age groups in the countries. We had results for only a small sub-sample, so findings may be subject to sampling bias. Data were collected through interviewer-assisted self-reporting and thus subject to recall bias. The disadvantages of using the pre-existing sample (that is the most recent census in most countries) includes the difficulty of adapting it to the DHS study requirements and conducting the same interviews with same household or person in different surveys which can result in respondent fatigue.45 Although to avoid respondent fatigue or contamination, the DHS separates the primary sampling units from the pre-existing sample and then reselects the household for survey.45 There is an inconsistency between the classification in Encyclopaedia Britannica of countries in West and Central Africa and the registered list of members of the Economic Community of West African States (ECOWAS) (https://ecowas.int/member-states/). Cameroon (as used in our study) though classified as a West African country in the Encyclopaedia, is not a member of the ECOWAS. Only two African countries (Benin and Cameroon) had data on cervical cancer among the 18 countries participating in the DHS. Our findings may therefore lack external validity for the countries we could not include. Another limitation of the data was that not all the women in Benin were asked questions on cervical cancer. Only women aged 15-49 years in households selected for the men’s survey answered questions on cervical cancer in Benin. This may have contributed to the low level of awareness in Benin. Only women of reproductive age (15-49 years) were included in the analysis. It is possible that awareness of cervical cancer and screening among women over 49 years may be slightly different from our findings. But since within our own analysis awareness increased with age, we don’t know if it would continue to do so with increasing age. However, it is important to note that exclusion bias is unlikely in our findings as neither of the two countries collected cervical cancer data for women over 49 years.
Conclusions
Data from this study will contribute to the existing literature on awareness of cervical cancer and screening, educate cervical cancer stakeholders, and inform future intervention research to help increase awareness of cervical cancer. Awareness of cervical cancer and screening in Benin and Cameroon is very low. There is a need to strengthen awareness programs through stakeholder engagement and public enlightenment. Media use, such as radio listening and internet use, may have a potential role in improving public enlightenment. In both countries, stakeholders need to implement the strategic plan for cervical cancer control and intensify awareness creation. Targeting younger women with age-appropriate cervical cancer information will help tackle the low level of awareness among young women. The inequality in awareness of cervical cancer and screening that exist between the poor and the rich in Cameroon needs to be tackled by investing in the education of the poor and ending residential segregation of access to health care. This will possibly allow free access to the required information on cervical cancer and screening.
Acknowledgments
We appreciate the women who participated in the survey and the DHS program team.
Funding
The study was conducted as part of the fulfilment of a Ph.D. funded by the Federal Government of Nigeria. The funder had no role in the study.
Authorship contributions
The study resulted from the first author’s PhD work. Two supervisors, Prof. KR and Dr BJ provided critical feedback, guidance during the analysis, and the interpretation of results. The two supervisors alongside Dr CJN and Dr CJ read through several drafts of the manuscripts before the final draft was submitted.
Competing interests
The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and declare no conflicts of interest.
Online Supplementary Document
Table S1. Univariate logistic regression of the demographic characteristics and media use associated with awareness of cervical cancer among women 15-49 years in Benin and Cameroon
Table S2. Univariate logistic regression of the demographic characteristics and media use associated with awareness of cervical cancer screening among women 15-49 years in Benin and Cameroon
Corresponding author:
Dr. Nike Olajide
MBBS, MPH
School of Health and Wellbeing
University of Glasgow
Clarice Pears Building
90 Byres Road
University of Glasgow
Glasgow G12 8TB.
[email protected], [email protected]