
Introduction
Soccer is unique among sports because it is the only sport that involves purposefully the use of the head to control, pass, or shoot the ball. The action of soccer heading has drawn considerable attention from policy makers, clinicians, researchers, parents, coaches, and athletes for its potential effects on the brain, particularly among younger players.1 The way soccer is played repeated impacts to the head (during headers) due to the high velocity at which the ball travels, reaching speeds up to 85 km/h (23.6 m/s). In fact, in response to a recent lawsuit and to minimize concussions that occur due to heading in youth soccer, U.S.A Soccer enacted guidelines restricting heading completely under the age of 11 and limiting it for players aged from 11 to 13 years.2 Many more institutions like the Football Association at UK follow similar guidelines for young footballers, males and females. Mild TBI is among the most common neurological conditions with an estimated annual incidence of 500/100,000 in the United States.3 One Canadian study examining both hospital-treated cases as well as those presenting to a family physician, calculated the incidence of mTBI in Ontario to lie between 493/100,000 and 653/100,000, depending on whether diagnosis was made by primary care physicians or a secondary reviewer.4
Concussions account for 5.8 per cent to 8.6 per cent of total injuries sustained during games.5 Swanik et al.6 found that 62.7% of varsity soccer players had suffered symptoms of a concussion during their playing careers, yet only 19.2% realized it. Gilbert et al.7 found that 81.8 per cent of athletes who had suffered a concussion had experienced two or more and that players with a history of concussion had 3.15 times greater odds of sustaining an additional concussion than those who had never had a concussion. Concussion/mild TBI can be described as the acute neurophysiological event related to blunt impact or other mechanical energy applied to the head, neck or body (with transmitting forces to the brain), such as from sudden acceleration, deceleration or rotational forces.8 Concussion can be sustained from a motor vehicle crash, sport or recreational injury, falls, workplace injury, assault or incident in the community.9
Over the previous five years, a relationship between lower extremity (LE) injury and sports related concussion (SRC) has been established in various sporting populations. Athletes at the high school, collegiate, and professional levels have demonstrated a greater risk for sustaining a LE injury post-SRC.10 The majority of the studies consist of retrospective injury surveillance data that monitored LE injury rates in concussed and non-concussed athletes for a specified time period surrounding the initial SRC event (both prior to- and post-SRC).11 All athletes diagnosed with SRC in these investigations were clinically cleared to play sports by sports medicine staff (athletic trainer, doctor, physiotherapist) and monitored for LE injury rates at various time points after the initial SRC. Of note, it is unclear if the individuals responsible for clearing athletes strictly adhered to all components related to the latest SRC consensus.12
A small number of studies examined the possible long-term effects of sub-concussive head impacts. While LE injury risk has been associated with SRC occurrence across multiple collegiate populations, previous investigations failed to control for LE injury history prior to an SRC, a potential confounding variable that may influence subsequent injury risk.13 Therefore, the purpose of this systematic review was to examine the relationship between SRC and LE musculoskeletal injuries.
Materials and Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines in the search strategy and reporting according to the PRISMA statement.
Information sources and Search Strategy
Keywords were selected (Lower limb injury, ball heading, neuromuscular control, concussion) by agreement of all authors and then submitted to a librarian with expertise in systematic reviews who developed a draft MEDLINE search strategy. This was reviewed by a second expert health sciences librarian using the CADTH Peer Review Checklist for Search Strategies according to the PRESS 2015 Guideline Statement. The draft search strategy was revised based on suggestions from the PRESS review, and then tested to be sure known key studies were retrieved. The MEDLINE search was adapted and translated for all other databases. The following 10 databases were searched: MEDLINE (Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R)), CINAHL Plus with Fulltext, EMBASE, PsycInfo, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Scopus, Web of Science, PsycARTICLES and SPORTDiscus. The search was limited to English-language and peer-reviewed publications with no date restriction. The search was conducted 12/11/ 2022.
Risk of Bias Assessment
The PEDro scale was used for the assessment of the risk of bias among the included studies. PEDro scale is a valid measure of methodological quality of clinical trials in rehabilitation. It consists of 11 items including external validity (item 1), internal validity (items 2–9), statistical reporting (items 10 and 11), and each one of them contributes one point to a total score of 10, except for one dichotomous item (yes/no). The PEDro scale is considered to meet interval level measurement, allowing score comparisons between studies. Scores of <4 are considered ‘poor’, 4–5 are considered ‘fair’, 6–8 are considered ‘good’, and 9–10 are considered ‘excellent’. Two reviewers assessed the risk of bias in each study independently and a third reviewer was recruited in case of any argument.
Eligibility criteria and data extraction
Studies were included if they (i) were original research; (ii) evaluated the incidence/prevalence, risk factors or causation related to neurodegenerative disease; (iii) included individuals who have suffered a sport-related concussion; (iv) evaluated athletes and/or retired athletes as the study subjects and (v) evaluated possible long-term sequelae defined as >10 years after sports-related injury. Studies were excluded from this review if they were published in a language other than English, studied animals, were review articles, case reports, book chapters, conference abstracts, editorials/commentaries/expert opinion, or theses or dissertations.
Citations were independently screened by pairs of authors. A third reviewer adjudicated disagreements between authors.
Study Selection Process
After duplicates and irrelevant records were removed, several relevant reports were sought for retrieval and assessed for eligibility through full-text screening by the two reviewers, independently. Two researchers searched independently all titles and abstracts from each search were screened to identify relevant studies. Subsequently, they excluded any reports with reasons, before ending up with the final studies of the review.All studies were imported, screened, and assessed through the EndNote software. (Clarivate, Philadelphia, PA, USA).
Data Items and Collection Process
The extracted data of the final studies included the characteristics of participants, the features of interventions, the outcome measures, and the main findings. The first reviewer sought and extracted these data, followed by the second reviewer checking the correctness of the data, and in case of disagreement, they were checked again. Reviewers worked independently during the process
Results
Study Selection
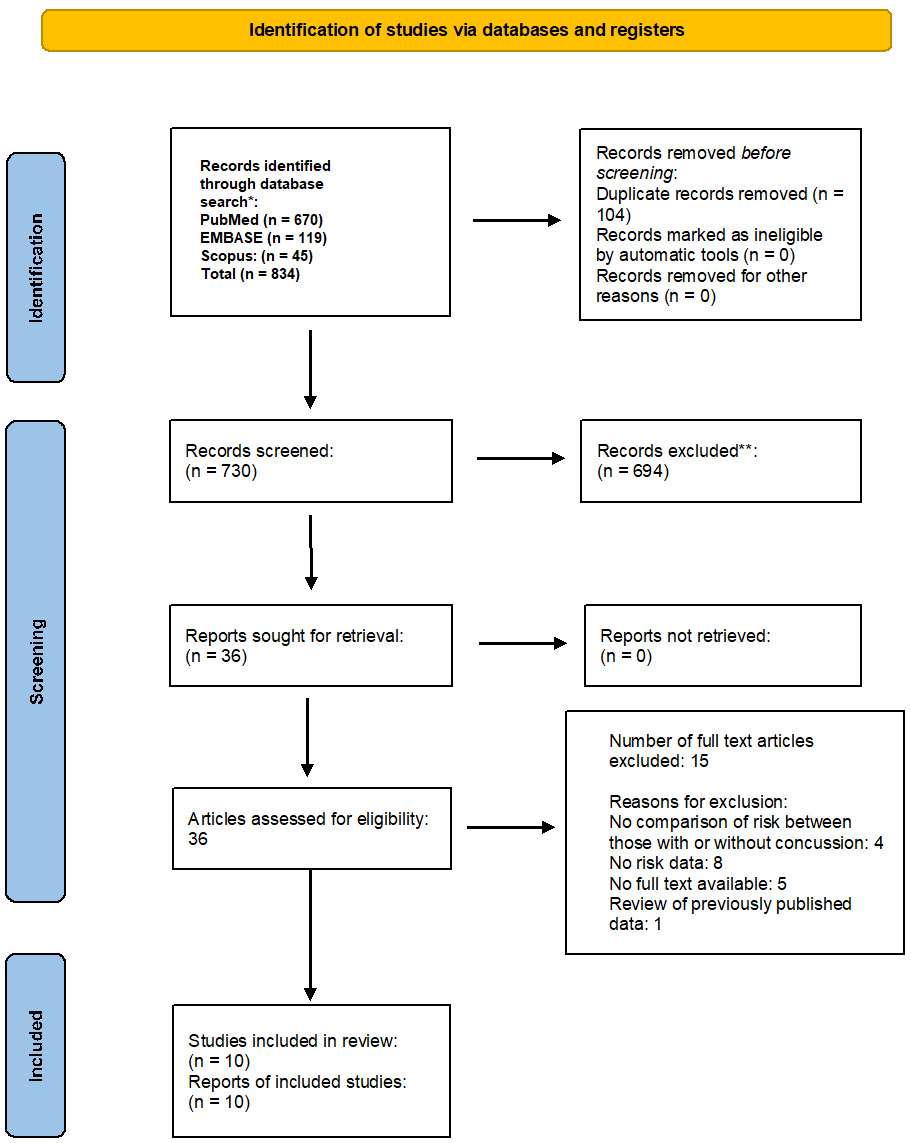
A total of 834 studies were identified from the databases and additional sources. Following the review of potential articles, 26 were full-text screened, of which 10 articles (four concussion-MSK biomechanics, six concussion-MSK injury) were included in the qualitative analyses. Due to the heterogeneous nature of the included study designs, this systematic review was unable to perform a quantitative meta-analysis for the present review. Therefore, our review presents a qualitative assessment of the available literature, as well as individual study characteristics and results. Included studies were prospective, retrospective, or cross-sectional designs, indicating that they were level 3 and 4 evidence studies. A comprehensive flowchart diagram of the study selection process is presented in Figure 1.
Risk of Bias in Studies
Table 1 shows the results of the methodological assessment based on the PEDro criteria. Out of 10 studies, five were rated as ‘high’, three were rated as ‘moderate’ and two were rated as ‘low quality’. Blinding therapists was not feasible in all trials due to the nature of the interventions. Four out of 10 studies did not ensure the blinding of the participants. One study included the blinding of outcome assessors. There was a low to no drop-out rate among the trials. Results were extracted by one author and reviewed by a second author to ensure accuracy and completeness. (Table 1)
Table 2 presents data extracted from all included studies.
All four of the included concussion-MSK biomechanics studies demonstrated, to some degree, that worse cognitive performance was associated with lower extremity MSK biomechanical patterns suggestive of greater risk for MSK injury. Among the six injury related studies, two investigations failed to determine group differences in cognitive performance between subsequently injured and non-injured athletes. The remaining four studies demonstrated that injured athletes significantly differed on baseline cognition measures versus matched controls, or that cognitive performance was a significant predictor for subsequent MSK injury.
Brooks et al14 found that the incidence of acute lower extremity musculoskeletal injury was higher among recently concussed athletes (15/87; 17%) compared with matched controls (17/182; 9%). The odds of sustaining an acute lower extremity musculoskeletal injury during the 90-day period after return to play were 2.48 times higher in concussed athletes than controls during the same 90-day period (odds ratio, 2.48; 95% CI, 1.04-5.91; p = 0.04). Also, Burman et al.15 stated that athletes with a concussion were more likely to sustain injuries compared with the control group, both before (OR 1.98. 95% CI 1.45 to 2.72) and after the concussion (OR 1.72. 95% CI 1.26 to 2.37). No increase in frequency of injury was found after a concussion compared with before. This was true for athletes in all four sports and for both sexes.
According to Cross et al.16 a total of 31,556 initial injuries were recorded soccer: 11,900; other sports: 19,656), which were followed by zero or one injury in the same season. Overall, first injury type was not a significant predictor of subsequent lower limb injury although certain contrasts yielded significant estimates. In soccer, the odds of sustaining a LE injury were higher after concussion than after upper extremity injury (UEMSKI; adjusted odds ratio [ORAdj], 1.56; 95% CI, 1.06-2.31). In football, the odds of TL LEMSKI were lower after concussion than after UEMSKI (ORAdj, 0.71; 95% CI, 0.51-0.99). No other significant effect estimates were observed for football or other sports.
Fino et al.17 found that concussion was associated with an increased instantaneous relative risk of LE injury when adjusting for LE injury history [hazard ratio (HR) = 1.67, 95% confidence interval (CI) = 1.11-2.53], agreeing with previous results. Among individuals who had a history of LE injuries before the concussion event, a nonsignificant yet moderate effect of concussion on the instantaneous relative risk of ipsilateral injuries was found after adjusting for the competing risk of contralateral injuries and censored values (HR = 1.85, 95% CI = 0.76-4.46). Similarly, Herman et al.18 found that lower extremity musculoskeletal injuries occurred at a higher rate in the concussed athletes (45/90 or 50%) than in the non-concussed athletes (30/148 or 20 %; p < 0.01). The odds of sustaining a lower limb musculoskeletal injury were 3.39 times higher in the concussed athletes (95 % confidence interval 1.90-6.05; p < 0.01). Overall, the number of days lost because of injury was similar between concussed and non-concussed athletes (median 9 versus 15; p = 0.41).
Lynall et al.19 stated that within one year after concussion, the group with concussion was 1.97 (95% confidence interval (CI), 1.19-3.28; P = 0.01) times more likely to experience a acute lower extremity musculoskeletal injury than before concussion and 1.64 times (95% CI, 1.07-2.51; p = 0.02) more likely to experience an acute lower extremity musculoskeletal injury than their matched non-concussed cohort over the same period. Up to 180 days after concussion, the group with concussion was 2.02 (95% CI, 1.08-3.78; p = 0.02) times more likely to experience an acute lower extremity musculoskeletal injury than before concussion.
Lynall et al.19 also found that Lower extremity injuries accounted for most injuries (56.3%), and concussions for 4.3% of total injuries. For every previous concussion, the odds of sustaining a subsequent time-loss lower extremity injury increased 34% (odds ratio [OR] = 1.34; 95% confidence interval [CI] = 1.13, 1.60). The number of previous concussions had no effect on the odds of sustaining any subsequent lower extremity injury (OR = 0.97; 95% CI = 0.89, 1.05) or a non–time-loss injury (OR = 1.01; 95% CI = 0.92, 1.10).
Makdissi et al.20 concluded that 199 concussive injuries were observed in 158 players. Sixty-one concussive injuries were excluded from analysis because of incomplete data (45 players) or presence of concurrent injury (16 players). Of the 138 concussive injuries assessed, 127 players returned to play without missing a game (92%). The remainder of concussed players returned to play after missing a single game (8%). Overall, there was no significant decline in concussed players on return to competition.
In soccer, Nordstrom et al.21 found during the follow-up period, 66 players sustained concussions and 1599 players sustained other injuries. Compared with the risk following other injuries, concussion was associated with a progressively increased risk of a subsequent LE injury in the first year (0 to <3 months, HR=1.56, 95% CI 1.09 to 2.23; 3 to <6 months, HR=2.78, 95% CI 1.58 to 4.89; 6-12 months, HR=4.07, 95% CI 2.14 to 7.76). In the second model, after adjustment for the number of injuries in the year preceding the concussion, this injury remained significantly associated with the risk of subsequent injury in the first year (HR=1.47, 95% CI 1.05 to 2.05).Finally, Nyberg et al.22 found that players who sustained a concussion did not have an increased risk for subsequent injuries compared with players who experienced a knee injury; however, concussed athletes experienced significantly more serious subsequent LE injuries (absence >28 days) within 21 days after return to play.
When accounting for previous LE injury, Fino et al.23 found college athletes post-SRC to be at a 67% greater risk for subsequent LE injury when matched to those of the same team. While the exact location of LE injury following SRC was unclear in the studies, determined significant associations between SRC (reported, unreported, and unrecognized) and lateral ankle sprain, knee injury, and LE muscle strain. This investigation consisted of 335 athletes (61% female) who completed a questionnaire pertaining to their injury history following the completion of their collegiate career. Although limitations exist due to self-reporting and an inability to determine order of injury occurrence, athletes with a stated SRC history were 1.6-2.9 times more likely to report a LE injury, findings similar to related retrospective data.24
Various authors have also suggested that collegiate athletes are at greater risk for LE injury at 90 days,25 180 days,26 and 365 days27 post-SRC. Collegiate male and female athletes across seven sports were 2.5 times more likely to sustain a LE musculoskeletal injury compared to matched counterparts 90 days after sustaining an SRC.28 It was determined that 17% of post-SRC athletes sustained a non-contact LE injury, while the incidence of similar injury was less (9%) in the matched control group.29 In a related study of collegiate basketball, soccer, and lacrosse athletes, LE musculoskeletal injury risk was 3.4 times greater in athletes who were previously concussed when matched to those of comparable athletic status during a 90 day follow-up period.30 Male soccer athletes with prior SRC were 3.7 times more likely to injure the LE, while female sport participants demonstrated a 2.8 times greater risk for LE injury after SRC.31These findings at 90 days post-SRC have not been observed in other collegiate cohorts,32 and it is presently unclear why these findings are equivocal. While Lynall et al. did not observe differences at 90 days, athletes were significantly more likely to sustain a LE injury at 180 days (2.02 times), and 365 days (1.97 times) post-SRC compared to pre-concussive injury rates.33 In addition to youth and collegiate athletes, professional athletes have demonstrated greater injury risk and frequencies following SRC.
Discussion
This systematic review and meta-analysis revealed that individuals appear to be at greater risk of sustaining a lower extremity musculoskeletal injury following a concussion compared to individuals without a history of concussion.34 Of the 10 included studies, some were of low quality which affects the strength of the conclusions of this systematic review.
Concussions can involve multiple and varied regions of the brain, including those associated with orienting and executive components of visuospatial attention and stimuli. When one suffers a concussion, these parts may become injured or impaired, which compromises the ability to process stimuli in terms of disengagement, movement, and re-engagement. Even after concusion symptoms resolve, there is a possibility that muscle strength and neuromuscular impairments are still present.35
There is ongoing research that has revealed that individuals continue to experience neuromuscular, neurocognitive, sensory processing, and balance deficits related to concussion well after RTP. While LE injury risk has been associated with SRC occurrence across multiple collegiate populations, previous investigations have failed to control for LE injury history prior to an SRC, a potential confounding variable that may influence subsequent injury risk.36 For example, athletes returning from ACL reconstruction are 15 times more likely to reinjure the ACL on the contralateral or ipsilateral limb.In addition to youth and collegiate athletes, professional athletes have demonstrated greater injury risk and frequencies following SRC.37 Elite male European soccer athletes were at greater risk for subsequent injury (combined lower and upper extremity) following SRC occurrence across three time periods (0–3 months, 3–6 months, and 6–12 months post-SRC with injury risk being greatest at 6–12 months after an SRC.38 Following 28 seasons of injury data in professional ice hockey players, researchers concluded that, in comparison to a knee injury, athletes post-SRC were more likely to sustain a subsequent severe LE injury (> 28 days recovery) within 21 days of returning to sport.39 However, no differences were reported at the seven and 42 day follow-up and the reported injury after the SRC or knee injury was not classified by location.40 Furthermore, no differences were observed in the frequency of subsequent injury between athletes who sustained an SRC or knee injury.41 Mounting evidence along with this systematic review suggests that athletes with a prior SRC history across all sporting populations are at greater risk for LE injury, although the mechanism for this relationship is presently unclear. Multiple theories have been postulated, such as impaired motor planning and coordination,42 reductions in cortical excitability,43 and neuromuscular alterations that persist far beyond resolution of traditional post-SRC measures It has been demonstrated through numerous studies that following a concussive event, the majority of athletes are able to return to baseline values relating to symptom reporting, performance, and balance/sway within a relatively short time period.44 However, subtle cognitive and physical deficiencies may persist, only to be revealed during a dynamic sporting environment that tasks performers with completing highly complex maneuvers.45
Recent evidence suggests that cognitive deficits related to dual tasking (which is very crucial in soccer), a hallmark of SRC, play a serious role in LE injury risk during sport.46 Examinations between musculoskeletal injury and cognition determined that collegiate athletes currently injured in the upper or lower extremity performed worse on matching tasks than healthy controls, and no statistical differences were found between athletes with a musculoskeletal injury or SRC on any neurocognitive metrics. Young adults classified as “low performers” on a NP test battery displayed biomechanical patterns suggesting a greater risk for ACL injury when performing dual-task drop landings.47 Compared to “high performing” individuals, those with a lower score completed landings with greater vertical ground reaction forces, anterior shear forces, knee abduction moment/angle, along with decreased trunk flexion angle.48,49 An athlete with deficiencies in processing environmental stimuli and task constraints (such as an athlete post-SRC), may have difficulty preplanning correct movement sequences, may not be able to produce protective muscular forces, which may lead to high impact loads on musculoskeletal components that result in injury.50
Limitations and Future Research
The results of the present systematic review should be interpreted carefully in light of its’ limitations. First, restricting the inclusion criteria to only English-language publications may have increased the risk of missing critical information published in other languages. Second, there were only a small number of well-designed studies included, however they may have been underpowered. Third. some of the included studies were of low quality.
Future Directions
Rehabilitation professionals should be aware that collegiate athletes may be at increased risk for lower extremity musculoskeletal injury following a sports related concussion, even after being cleared for return to play (RTP). Many of the RTP concussion protocol tests are important, but some are subjective, such as the symptom checklist and assessments. Research has suggested that current concussion testing methods may not possess sufficient sensitivity to detect any lingering concussion-related abnormalities that persist after symptom resolution which may in turn affect motor performance. Future research should attempt to identify new methods to evaluate athletes during the RTP concussion protocol to ensure that they are fully prepared to return to their sport and are not experiencing subtle or lingering deficits when returning to participation.
Conclusion
Mounting evidence indicates that athletes with a prior SRC history across all sporting populations may be at greater risk for LE injury, based on moderate to low quality evidence. The reasons for this relationship is presently unclear and needs more research to discern the underlying mechanisms.
Conflicts of Interest
The authors declare no conflict of interest.