INTRODUCTION
Anterior Cruciate Ligament reconstruction (ACL-R) is typically recommended following ACL injury for patients planning to return to running, jumping, or cutting activities. ACL-R is thought to help improve excessive anterior tibial translation, improve rotational stability and restore proper joint kinematics resulting in improved pain, instability, and function.1–3 While ACL-R remains the gold standard for the management of ACL injuries, recent reviews examining the short- and long-term outcomes following reconstruction demonstrate that outcomes may not be as favorable as previously thought.4–8
Patients have high expectations following ACL-R with 91% expecting to return to the same level of sport/activity.9 Unfortunately, the results for return to sport (RTS) do not match these expectations with only 81% of people returning to any sport, 65% returning to their preinjury level of sport and 55% returning to competitive level sport.4 Of those who do return to sports, up to 20-30% sustain a contralateral ACL tear or graft re-rupture.7,8 Furthermore, approximately 50% of athletes who suffer an ACL injury will develop knee joint osteoarthritis (OA) in the 5-15 years following the initial injury.10–12
Weakness of the quadriceps following ACL-R has been directly linked to the development of patient dysfunction,5,13 knee osteoarthritis3,11 and lower likelihood of returning to same level of sport.14,15 Following ACL-R, patients can have diminished quadriceps strength long after expected time of RTS with average side to side quadriceps strength deficits of 23% and 14% at 6 and 12 months respectively.16 The diminished quadriceps strength following ACL-R may be related to several factors including graft site morbidity, post-operative swelling and pain,17,18 decreased knee extension range of motion,19 quadriceps atrophy20 and neural changes in the sensory and motor pathways.18,21–23 Quadriceps strength deficits cannot be solely attributed to graft site morbidity because patients with hamstring autografts also display quadriceps weakness, although to a lesser degree.24 Studies continue to demonstrate the prevalence of quadriceps strength deficits following ACL-R despite evidence showing the importance of restoring quadriceps strength.16
There is a recent renewed interest in the ACL repair (ACL-r) procedure as a potentially more joint friendly procedure, with less surgical trauma and preservation of the native ACL. ACL repair was previously abandoned following the study by Feigen et al. in 1976 which showed poor mid-term outcomes with nearly a 50% re-tear rate.25 However, several limitations exist in these older studies including the use of an open technique, repair of all tear types, use of antiquated techniques with absorbable sutures and cast immobilization for up to six weeks following surgery, all of which may have contributed to poor outcomes.25–27 On reanalysis of these results, proximal ACL tear types performed better compared to midsubstance tears.25 Newer early to midterm data on ACL repair demonstrates that ACL repair re-tear rates may be similar to ACL reconstruction in select patients and tear types.28 More recently, in several animal models and in human clinical data, ACL remnant preservation and ACL entire ligament repair/preservation has been shown to benefit knee biomechanics, proprioception, and clinical outcomes.24,26,28,29 However, there is limited data on the newer ACL-r techniques and further study is needed to validate the efficacy of this procedure.
Therefore, the purpose of this study was to assess for differences in metrics of knee joint loading during a single limb squat task between individuals following a primary ACL-r versus those who underwent a standard ACL-R with a patella bone-tendon-bone autograft. The single leg squat task was chosen as this is a movement readily implemented throughout the rehabilitation process. The single leg squat is utilized as both an exercise to improve lower extremity strength and neuromuscular control, and as a screening tool to assess readiness for return to running and sport.30–32 The authors hypothesized that there would be improved surgical limb knee loading in ACL-r compared to ACL-R at the three-month post-operative time point.
METHODS
Participants
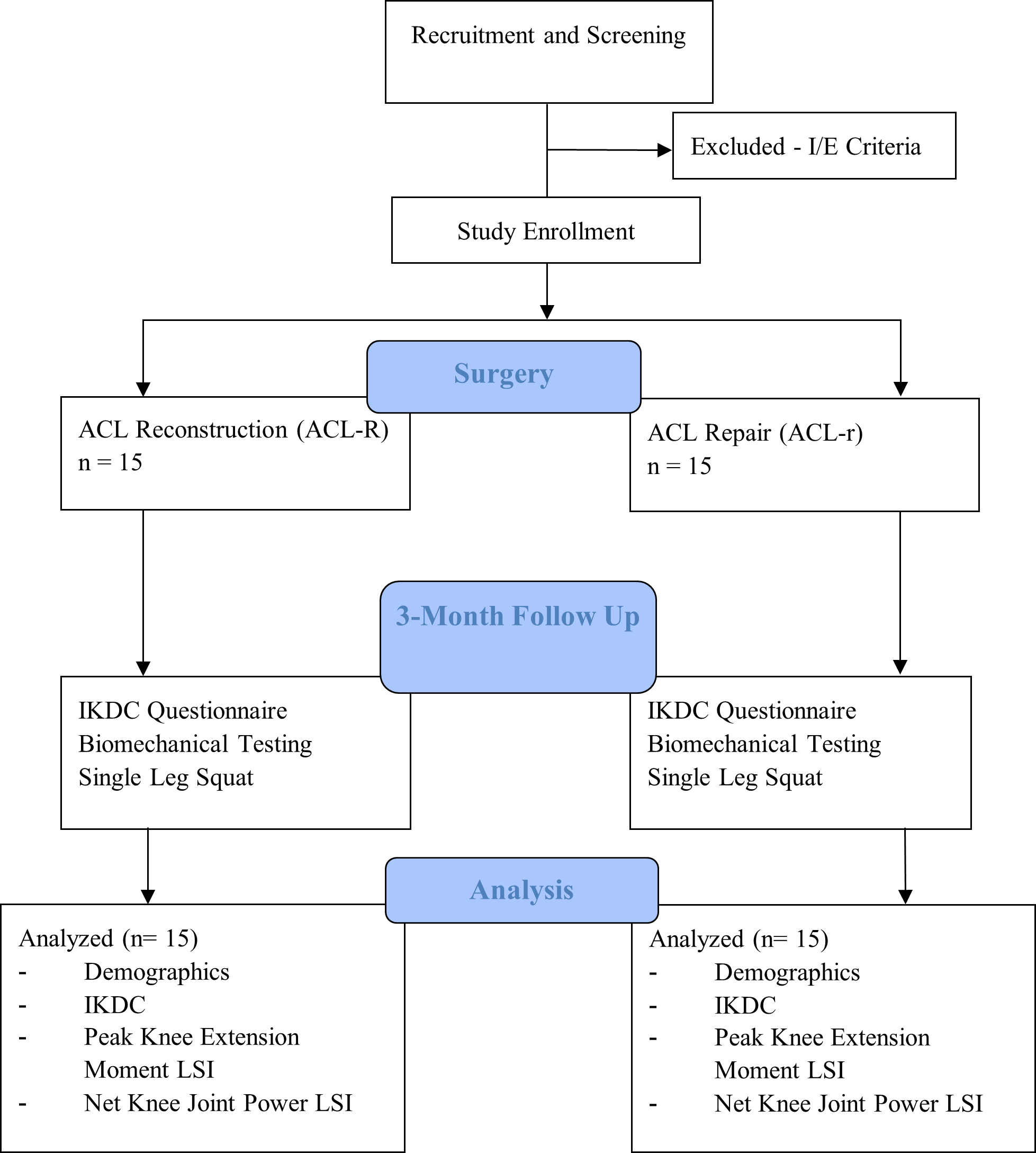
A total of 30 individuals who met the inclusion criteria were included in this study. All participants were tested at three months following surgery as part of a larger ongoing ACL study examining biomechanical and clinical outcomes across the continuum of care (Figure 1). Participants were considered eligible for the study if they were between the ages of twelve and sixty years old, sustained a primary ACL injury, elected to undergo either an ACL-R or ACL-r procedure, were considered a recreational or professional athlete participating in sport at least 50 hours/year and were attempting to return to their activity. All surgeries were performed by a single surgeon.

Participants did not complete formal pre-rehabilitation with a physical therapist or athletic trainer; rather, pre-rehabilitation education was completed by the treating surgeon. Participants in the ACL-r group all sustained a proximal ACL disruption (Sherman Classification Type 1 or 2) that was amenable to repair and underwent primary ACL repair with suture fixation.33 Participants in the ACL-R group all underwent a primary ACL-R with patella bone-tendon-bone autograft. Participants were excluded from the study if they had previously injured their ACL, had full thickness chondral injuries, had a grade II or III injury of the medial collateral ligament (MCL), lateral collateral ligament (LCL), posterior collateral ligament (PCL) injuries, or simultaneous fracture with ACL tear. Meniscal pathology was treated as deemed appropriate by the treating surgeon. There was no significant meniscal pathology in either group that necessitated altering the post operative rehabilitation protocol. Following surgery all participants completed formal physical therapy guided by the rehabilitation protocol of the surgeon. The rehabilitation protocol can be seen in Appendix 1 and further described by Bousquet et al.34
Following the screening process, if the subjects were eligible, they were invited to participate in the study. All participants gave informed consent to participate and the rights of each person were protected. If the participants were a minor, parental consent and child assent were attained. The Institutional Review Board of Texas Health Resources approved the research procedures. Following enrollment of the study, demographic information, injury history, sports participation, and International Knee Documentation Committee (IKDC) Subjective Knee Form scores were collected from each participant.
ACL-r Surgical Technique
ACL-r was performed under arthroscopic visualization with two or three standard portals in a technique similar to that described by DiFelice et al,26 but modified by the senior author to include only one 4.75mm SwiveLock (Arthrex, Naples, FL) secured in the anterior aspect of the native footprint on the medial wall of the lateral femoral condyle. Indications for repair were similar to that described by DiFelice et al.26
ACL-R Surgical Technique
Participants in the ACL-R group all underwent a primary ACL-R with patella bone-tendon-bone autograft. The autograft bone blocks were crimped to 9mm and then two 10mm femoral and tibial tunnels created for the graft. An independent tunnel technique, utilizing the medial portal for creation of the femoral socket within the native ACL femoral attachment site, was performed in all ACL-R patients.
Biomechanical Instrumentation
A 10-camera Motion Capture System (Qualisys AB, Göteborg, Sweden) with a sampling rate of 120Hz was used to capture joint motions in all three planes during the single limb squat. Thirty-three reflective markers were adhered to each participant’s skin/clothing with double-sided tape. Retroreflective markers were attached to the spinous process of the seventh cervical vertebra, twelfth thoracic vertebra, between the fourth and fifth lumbar vertebrae, sternum, bilateral acromion process, anterior superior iliac spine, posterior superior iliac spine, greater trochanter, anterior thigh, medial and lateral epicondyles of the femur, anterior shank, medial and lateral malleoli, calcaneus, and first and fifth metatarsal heads. Three additional retroreflective markers were attached on the sacrum as a cluster. Two ATMI force plates capturing at 1200Hz (Advanced Mechanical Technology, Inc., Watertown, MA) collected ground reaction force data utilized to calculate joint kinetics and were synchronized to the cameras allowing accurate time sequencing during data collection and data processing.
Single Limb Squat
The single limb squat task was chosen as it has been utilized throughout the literature to look at sagittal, frontal, and transverse plane kinematics in both healthy and injured cohorts to help assess movement quality.35,36 The single limb squat task is a foundational movement pattern in rehabilitation following ACL injury and performance during a single limb squat is used as a proxy to assess lower extremity strength and readiness to return to running.30,37,38 Participants were allowed to warm up until they felt comfortable with the given activity. Participants were asked to stand on one foot with their toes facing straight forward with their hands on their waist with their contralateral hip and knee flexed to 90 degrees. They were instructed to perform five consecutive single limb squats. A metronome set at 60 bpm was used to ensure consistent pace across testing as participants completed the five single limb squats. Participants were asked to squat to their best possible depth without losing balance but squat depth was not normalized. If a participant experienced a loss of balance, then the capture period was repeated until five consecutive single limb squats could be completed. The mean of the middle three squats was used for data analysis. All participants completed testing on their non-surgical limb followed by their surgical limbs.
Isokinetic Quadriceps Strength Testing
The Biodex Multi-Joint Testing and Rehabilitation System (Biodex Medical Systems, Shirley, NY) was used for testing concentric extensor peak torque. For the purpose of this study, extensor peak torque will be referred to throughout the manuscript as quadriceps strength. Quadriceps strength was measured at 60°/s and the protocol used has previously been described in the literature.39,40 All subjects completed testing on their non-surgical limb followed by their surgical limb.
Data Processing and Reduction
Peak quadriceps strength (Nm) was averaged across five trials and were normalized to body mass (Nm Kg-1). Three-dimensional joint coordinates were estimated from the trajectories of the reflective markers. All kinematic and force data were exported into Visual3D software (C-Motion, Inc. Germantown, MD) to process and reduce data. The markers and force data were filtered via a fourth-order low-pass Butterworth filter with a zero- phase lag at 12 Hz. Peak knee extension moment (Nm BW*Ht -1) was calculated using inverse dynamic approach during the descent phase of the single limb squat. Knee energy absorption (J BW*Ht-1) was calculated as an integration of the negative area of the knee joint power curve as a measure of eccentric loading (contraction) during the descent phase of a single limb squat which may be able to show greater differences in knee loading between groups compared to concentric contraction. Both variables were collected from surgical and non-surgical limbs during middle three trials of the five squats and normalized to height and body weight of the participants. A limb symmetry index (LSI) (surgical/non-surgical X 100) was calculated for all dependent variables.
Statistical Analyses
Independent t-tests were used to compare between group differences in demographic variables. Variables with significant difference would be used as covariate for the analyses. For the three variables of interest an analysis of covariance (ANCOVA) with a p-value set at p<0.05 was used for analysis, Bonferroni adjustment was included for adjustment of multiple comparisons. Partial Eta Squared effect sizes were calculated with standard thresholds used for strength of effect.
RESULTS
There were no differences in height (p=0.996), mass (p=0.996), IKDC score (p=0.886) or time between injury and surgery dates (p=0.912) between the groups. There was a significant difference in age (ACL-r: 38.87 ±13.9, ACL-R: 25.60±11.78; p=0.009) with the ACL-r being significantly older. (Table 1)
There were significant between group differences in all variables of interest while controlling for age (Table 2). The ACL-r had a significantly greater peak knee extension moment LSI (ACL-r: 78.46±5.79%; ACL-R: 56.86±5.79%; p=0.019, ηp2=.186 and net knee joint power LSI (ACL-r: 72.47±7.39%; ACL-R: 39.70±7.39%; p=0.006, ηp2=.245) than the ACL-R group during the single limb squat. The ACL-r also had a significantly greater quadriceps LSI than the ACL-R group (ACL-r: 66.318±4.61%, ACL-R: 48.03±4.61%; p=0.013, ηp2=.206). No patients experienced any major complications at final follow up including hospitalization, DVT or infection.
DISCUSSION
The results of this study indicate that individuals following ACL-r demonstrate differing loading strategies during a single leg squat and greater quadriceps strength symmetry in isokinetic testing compared to those who undergo ACL-R. The ACL-r group demonstrated greater limb symmetry in peak knee extension moment, quadriceps strength and knee energy absorption than the ACL-R group during a single limb squat. These measures are related but different and contribute to changes in both peak joint loading (knee extension moment) and loading over the entire movement (energy absorption), both of which may be important for joint health and function. These outcomes are unique and to our knowledge this study is the first to compare kinetics between ACL-r and ACL-R cohorts at the three-month time point.
Quadriceps deficits at three months following ACL-R have been associated with continued quadriceps deficits at time of return to sport.40 Persistent quadriceps strength deficits are associated with poor self-reported outcomes, altered biomechanics and increased risk of secondary injury.7,41 It is worth noting that the magnitude of difference in joint loading was large with knee joint power LSI of 72% vs 39% and quadriceps strength LSI of 66% vs 48% in the repair vs reconstruction group respectively. This was despite the fact that the repair group was significantly older compared to the reconstruction group which we expected to have a slower recovery of strength. Based on previous studies that demonstrates long term quadriceps strength deficits following ACL reconstruction, the authors expect this gap in loading and strength between the two cohorts to diminish but persist at longer term follow up.16 Prior studies have also demonstrated faster recovery of objective measures in ACL-r vs ACL-R. Van der list et al. demonstrated ACL-r patient had faster return of normal knee ROM with a trend towards decreased complications in the repair group (2% vs 9%).42
The strength symmetry data in the ACL-r group is significantly greater than previous work following ACL-R at three months after surgery in which the LSI reached 55% and was directly related to the ability to load the surgical limb knee.39 This improvement in strength may simply be related to the less traumatic nature of the ACL-r procedure resulting in less post-operative swelling, edema, and no associated graft site morbidity. Graft site morbidity is likely not the only contributing factors as previous studies have demonstrated decreased quadriceps strength following ACL-R with hamstring autograft and allograft.16,24 Other factors that warrant further investigation are potential differences between the two procedures in resultant arthrogenic muscle inhibition and differences in afferent signaling from the knee joint because of leaving the native ACL in place (during the ACL-r procedure).
Lee et al. reported on 26 subjects who underwent ACL-R with remnant tibial stump preservation compared to 22 subjects who underwent standard ACL-R without remnant preservation. They found that at approximately 2 years following surgery, those in the remnant preservation group had significantly better results on tests of proprioception (reproduction of passive positioning and threshold to detection of passive motion) compared to the standard group.24 If the findings of remnant preservation are extrapolated to leaving the entire native ACL in place, as is done in the ACL-r procedure, it may be plausible that there would similarly be an improved proprioceptive response in ACL-r patients compared to ACL-R.
Efferent signaling to the quadriceps muscle has been shown to be modulated by afferent input from the joint. The changes in afferent signaling from the joint and surrounding tissues contribute to the known mechanisms of arthrogenic muscle inhibition including alterations in muscle resting motor thresholds, changes in the discharge of articular sensory receptors, altered spinal reflex excitability (affecting the group I non-reciprocal (Ib) inhibitory pathway, the flexion reflex and the gamma loop) and abnormal cortical activity (intracortical inhibition and a requirement for greater frontal cortex theta power in basic movement and joint position sense tasks).18 With less overall trauma to the knee joint, it is possible that those individuals who received an ACL-r were better able to restore joint homeostasis, and thus maintain better afferent and efferent signaling in the respective joint.
Prior research has established that greater peak joint loading is related to decreased collagen turnover in individuals following ACL-R. In a total of 19 subjects who were on average three years post-operative ACL-R, greater peak vGRF during gait was associated with lower type II collagen breakdown.41 Similarly, Wellstandt et al. reported on frontal plane joint kinetics in 22 individuals (15-without OA, 7- with OA) five years following primary ACL-R which found that decreased surgical limb knee joint loading during walking was associated with early OA.8 Both of these studies support the notion that decreased knee joint loading is associated with OA following ACL-R during walking. Although the current study only examines joint loading at three months post operatively, quadriceps deficits could have an effect on long term joint health if weakness persists.
This study is not without limitations. A relatively small sample was examined with short term follow up. Longer term follow-up on this cohort is needed to examine if these loading differences persist. There is also a difference in age between the two patient groups which could bias the results. It is possible that the younger patient population could have a more robust inflammatory response leading to a greater degree of quadriceps deactivation. Given the study design the authors cannot determine a direct relationship between ACL-r and improved joint loading. Further work is needed to better elucidate the risks and benefits of performing ACL-r vs ACL-R.
CONCLUSION
The results of this study indicate that individuals following ACL-r demonstrate increased knee joint loading symmetry during a single leg squat task and greater quadriceps strength symmetry at 12 weeks post-surgery compared to those who underwent ACL-R. ACL-r may result in improved early knee joint loading and proprioception compared to ACL-R.
Conflicts of interest
The authors have no relevant conflicts of interest to disclosure.