Introduction
Disorders of the long head of the biceps brachii tendon (LHBT) are a commonly recognized source of shoulder pain.1–5 it is not unusual to have LHB pathology associated with rotator cuff tears and subacromial impingement.6,7 Rotator cuff deficiency increases superior translation of the humeral head in relation to the glenoid fossa, causing the LHBT, a humeral head depressor, to be subject to overuse injury. Clinical success is always predicated upon an accurate diagnosis and understanding of the pathological process. While a careful history and a thorough physical examination are important steps in the assessment of LHBT pathology, it is still difficult to differentiate the type and severity of the pathology. Musculoskeletal ultrasound (MSK US) imaging has become an established tool to assist in and optimize the diagnostic process. While MSK US is very accurate in the diagnosis of rotator cuff tears, there is moderate to strong evidence to support the use of MSK US in diagnosis of LHBT pathology.8 MSK US can accurately help to diagnose partial and full-thickness tears, LHBT subluxation/dislocation, and LHB tendinopathy.8
At times, MSK US can be a difficult diagnostic tool to use clinically and interpret the results. However, when used correctly, MSK US is a valuable tool to accurately diagnose a variety of LHBT pathologies. Therefore, its use should help to facilitate diagnosis and treatment of patients with shoulder pain due to suspected biceps tendon pathologies. The goal of this article is to provide a few tips and tricks to assist in using MSK US as a diagnostic tool for the assessment of the LHBT.
Patient Position

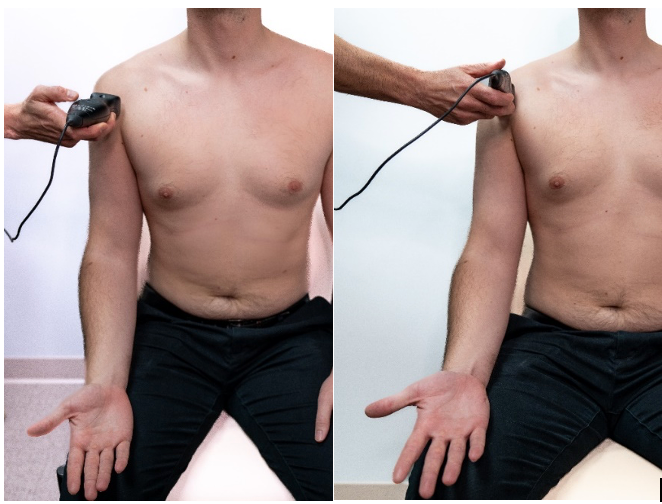
Figure 1.
1a: Patient is seated with shoulder and elbow relaxed. Shoulder at 0 degrees of abduction, neutral rotation, elbow flexed and resting on leg or pillow with forearm supinated.
Transducer Placement: Short Axis (SAX)
Probe placed transversely on the proximal anterior aspect of the shoulder, over the LHB.
1b: Patient is seated with shoulder and elbow relaxed. Shoulder at 0 degrees of abduction, neutral rotation, elbow flexed and resting on leg or pillow with forearm supinated
Transducer Placement: Long Axis View (LAX)
Probe placed longitudinally on the proximal anterior aspect of the shoulder, over the LHB.
Normal Tendon

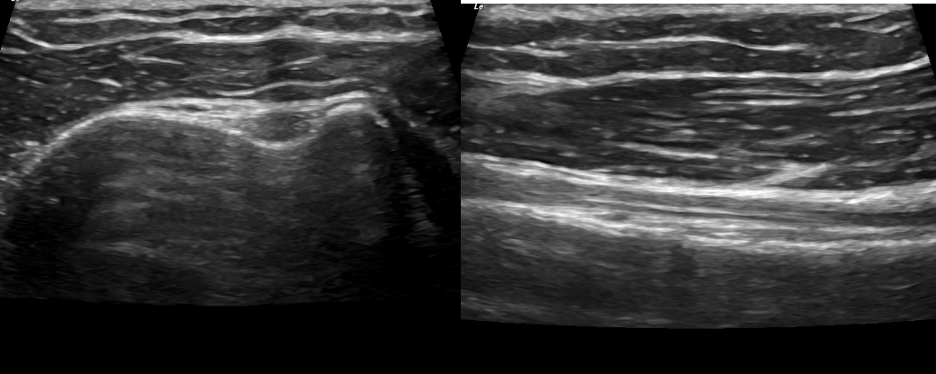
Figure 2.
2a: Normal Tendon-Short Axis View
LHB tendon is located deep within the inter-tubercular groove and viewed as a bright hyperechoic defined tendon. It is easily seen see between the bony greater and lesser tubercles. The thin band of bright tissue overlying the top of the
2b: Normal Tendon-Long Axis View
LHB tendon is seen running parallel along the image running proximal to distal from left to right. It should be seen as a bright hyperechoic fibrous band of tissue. The deltoid is seen above as a linear tissue with darker muscle bundles.
LHB Tendon Pathology

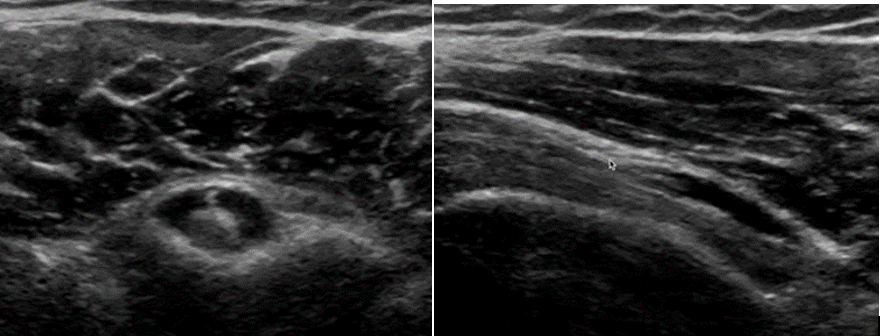
Figure 3.
3a: Effusion and edema are seen as an area of hypoechoic signal within the tendon sheath surrounding the LHB tendon. The anechoic ring is known as a “halo sign” on a SAX view. This edema could be either a tenosynovitis or a capsulitis. The LAX will be the differential view.
3b: Joint effusion within the tendon sheath seen here on the LAX. On the LAX views, it reveals presence of fluid distally indicating a tenosynovitis. A capsulitis would not show effusion in the biceps tendon sheath distally on the LAX view.