INTRODUCTION
Meniscal injuries are diagnosed through clinical evaluation, magnetic resonance imaging (MRI), or diagnostic arthroscopy.1,2 Arthroscopy, which is reported to have an accuracy of 90-95% and has the benefit of immediate surgical correction being able to be performed, is considered the gold standard diagnostic technique; however, arthroscopy has drawbacks such as unnecessary surgical costs and risks.1,3 The reported diagnostic accuracy of MRI has been as high as 88%,4 but MRI also has drawbacks, such as high prevalence of findings in asymptomatic uninjured knees,5 increased healthcare costs,6 and challenges with accessing imaging.7 Thus, accurate diagnosis with a physical exam is valuable; comprehensive physical examination and testing batteries (i.e., positive McMurray’s, Thessaly’s, and Apley’s tests) have been associated with high diagnostic accuracies of 90% and 81%, respectively.8 Similarly, a clinical prediction rule of a history of catching or locking, pain with forced hyperextension, pain with maximum knee flexion, joint line tenderness, and pain or clicking while performing McMurry’s test has been reported to have a positive predictive value of 92.3% and a positive likelihood ratio of 11.45 when all five signs are present in a clinical exam.9
Once diagnosed, meniscal injuries are often treated surgically in combination with conservative therapy or after conservative therapy has failed to produce the desired improvement.2,10,11 In fact, arthroscopic partial meniscectomy (APM), which addresses meniscal injury by removing the damaged meniscal tissue, is one of the most commonly performed orthopedic surgeries.12,13 Surgical approaches, however, have often failed to have the desired result. For example, APM has not been found to outperform sham surgery or conservative management, and surgery has resulted in patients who were more susceptible to developing osteoarthritis.11,12,14 Arthroscopic repair, which has a reputation as the “gold standard” for meniscal injuries in cases where it is feasible to repair the specific meniscal tear present,10,15 has high rates of failure (e.g., patients often re-develop symptoms, patients require additional corrective operations, etc.).16,17 When patient history, physical examination, current pain, and dysfunction or mechanical symptoms indicate meniscal injury, non-operative or conservative treatment is recommended.2,18
Thus, there is a need to consider other treatment options for patients who present with the signs and symptoms of a meniscal pathology due to the prevalence of meniscal injuries, potential undesired surgical outcomes (e.g., adverse long-term outcomes), and recommendations for conservative care.2,12,19,20 The Mulligan Concept (MC), introduced by Brian Mulligan, is an innovative conservative treatment approach used to address common issues (e.g., joint pain, decreased ROM, movement dysfunction, etc.) associated with knee joint pathology.21,22 The MC incorporates movement with mobilization by combining the patient’s active range of motion (AROM) with a clinician’s joint glides to attempt to produce immediate changes in the patient’s complaints and impairment measures. While consensus on the mechanism of action has not been reached, application of the MC is thought to alter the mechanoreceptive and nociceptive responses to promote immediate improvements in the patient’s impairment.23,24
Specific MC mobilizations with movement (MWMs) techniques have been proposed as effective conservative non-surgical interventions for meniscal pathology.25 Researchers have recently begun to examine the effects of the proposed MC MWM techniques (i.e., ‘Squeeze’ technique, tibial IR, and tibial ER) in patients with clinically diagnosed meniscal lesions.24,26–29 A synthesis of the available literature to assess the effectiveness of the proposed meniscal MC MWM techniques in the treatment of clinically diagnosed meniscal lesions has not been conducted. Examining the effects of these MC MWMs in clinically diagnosed meniscal lesions would provide an update on the evidence and help inform practitioners on an evidence-based method for incorporating MC MWMs ‘Squeeze’, tibial IR, and tibial ER into clinical practice. Therefore, the purpose of this systematic review was to critically appraise the literature to investigate the effectiveness of MC MWMs for meniscal lesions on patient reported pain, function, and multi-dimensional health status in patients with clinically diagnosed meniscal pathologies.
METHODS
Study Design
The systematic review was registered on the International Prospective Register of Systematic Reviews (PROSPERO), a database for tracking the quality of systematic reviews in health professions (CRD42021278025). The 13-item PROSPERO checklist for the creation of systematic reviews was followed for accuracy of study design and reporting.30 The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 27 item checklist was also used in the creation of the systematic review to ensure the quality of the study design.31
Search Strategy
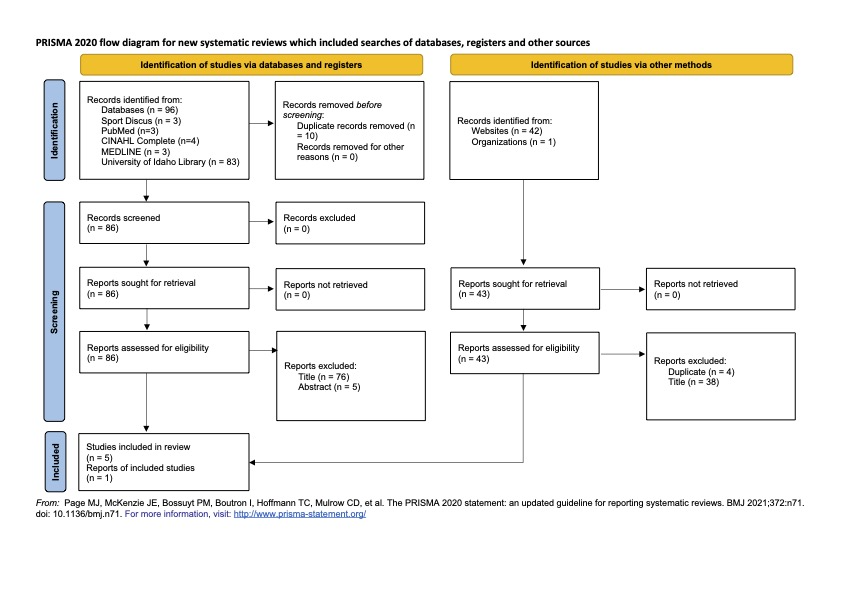
An electronic search of the literature was conducted in May 2022. The following databases were used for the literature search: PubMed, SportDiscus, CINHAL, MEDLINE, the University of Idaho library, and the indexed reference of published works listed on the Mulligan Concept website. The search was limited to the last ten years with an additional filter to specify academic articles or journal articles depending on the database. The search terms used were "menisc* AND mulligan AND pain (Figure 1). Other search terms (i.e., knee, function, mobilization with movement, MWM, mulligan concept, MC, meniscal pathology, meniscal derangement, and meniscal tear) were used to find additional studies, but no additional studies were identified with these terms. A hand search of the references of identified articles was also performed; however, no additional studies were identified with this process, while one additional study was identified on the Mulligan Concept website that was published in the Journal of Sports Medicine and Allied Health Sciences, which is the official journal of the Ohio Athletic Trainers Association.

Eligibility Criteria
Each study had to meet the following inclusion criteria to be eligible for this review. A clinical diagnosis of a meniscal pathology consisting of a minimum of three of the following items during the physical exam: 1) a positive test for McMurray’s, Thessaly’s, or Apley’s Compression tests; 2) pain at end range of knee flexion; 3) pain at end range of knee extension; 4) joint line tenderness; and 5) a history of painful popping or clicking (Table 1). Additionally, the use of the MC MWM ‘Squeeze’ technique, tibial IR, or tibial ER for treatment of clinically diagnosed meniscal pathologies had to be present. Finally, PRO measures had to be used in the assessment of knee pain or function. Studies were excluded if a non-MWM MC technique or alternative forms of manual therapy were utilized or if the included participants had any other clinically diagnosed knee pathology, hyperalgesia, or a previous history of knee surgery. Studies were also excluded if they were not published in English, not published within the last 10 years, or did not meet the expectations for blinded peer-review (e.g., dissertations, poster presentations,).
Study Selection
One author (NR) conducted the initial search, while a second author (SL) repeated the search to ensure the accuracy and repeatability of the search results (Figure 1). The two search authors (NR and SL) were blinded to the initial review of titles and abstracts and met to ensure final inclusion was consistent. Four of the authors (NR, SL, RH, and DB) independently completed a full text review of the studies that met inclusion and exclusion criteria and met to reach consensus for inclusion; a fifth author (RB) was consulted to confirm inclusion in the event of an impasse. All the authors agreed that the studies selected met the criteria for inclusion after review (Table 2).
Data Collected
The studies included were graded with the following scales to assess and measure the study quality (e.g., study type, internal validity, level of evidence; (Table 3). The PEDro scale was used to assess the internal validity of the randomized control trials (RCTs); scores of seven or higher were considered high methodological quality, five to six were fair quality, and zero to four were poor quality.32 The Downs and Black (D&B) Checklist for randomized studies examining health care interventions was also utilized to evaluate included RCTs.33 The 27 item D&B Checklist was scored out of 32 total points where ranges of corresponding scores were given: excellent (26-32); good (20-25); fair (15-19); and poor (≤ 14).34 Any identified case series was assessed with the Joanna Briggs Institute (JBI) checklist for case series. A 6/10 or greater indicated a low risk of bias.35 Identified case studies were assessed with the CARES checklist and were scored out of twelve.36 The CARES checklist was scored on a 0-12 scale by giving a point to any question within a category when answered “yes” by the reviewer. The last question (Question 13) was not scored because it is intended for the completion of a case study by the original author and is not always reported in the study. Each study was assigned a level of evidence in accordance with the Oxford Center of Evidence-Based Medicine.37 This system of assessment was designed to quickly assess the best literature based on the study’s design. Each study design falls within a specific level that can be graded up or down based on the quality of the study.37
Data Extraction
The total number of participants and general demographic information were extracted from each qualified study. The primary data extracted from each article were study characteristics (e.g., publication data, study design, etc.), methodology (e.g., treatment protocol, inclusion/exclusion criteria, etc.), and results. Patient reported pain was assessed by the Numeric Pain Rating Scale (NRS). Patient-reported function was assessed by the Patient-Specific Functional Scale (PSFS), while multi-dimensional (e.g., impairment, quality of life, etc.) patient-reported assessment of health status was assessed with the Disablement in the Physically Active (DPA) and Knee Osteoarthritis Outcome Score (KOOS). The Lower Extremity Functional Scale (LEFS), Global Rating of Change (GRoC), Range of motion (ROM), and Client Specific Impairment Measures (CSIM) were assessed as secondary outcomes when reported. Lastly, follow-up results were collected to determine the long-term effectiveness of the treatment intervention.
Primary Outcomes
Pain
The NRS is an outcome measure designed to assess pain intensity.38 All six studies utilized the NRS, which is a single-item measure that ranges from 0 (no pain) to 10 (most severe pain) and is used to assess the best, current, and worst pain the patient has experienced over the past 24 hours.38,39 The minimal clinically important difference (MCID) on the NRS is 2 points or a 33% reduction indicating a “much better” improvement in symptoms.40
Function
The PSFS was used to assess function. All six studies utilized the PSFS, where patients choose and rate functional or personally important tasks from 0 (unable to perform activity) to 10 (able to perform activity at pre-injury level).34,35,41 The MCID for the PSFS is 3 points in orthopedic knee conditions.41
Multi-dimensional Health Status
Five studies used the DPA scale to assess the patient’s perception of disablement as a result of their injury.42 The DPA scale consists of 16 items scored from 1 (no problem) to 5 (the problem(s) severely affect me).42,43 The scores for each item are totaled and then 16 is subtracted from the total score to provide the DPA score; scores range from 0-64, with high scores indicating more severe disablement.42 The MCID value for the DPA scale is a change of 9 points in acute injuries and a change of 6 points in chronic injuries.42
Two studies used the KOOS, which is a self-administered outcome measure used to assess a patient’s perception of their knee injury and ability to complete usual activities.44 The KOOS assesses five different subscales specific to knee injury: pain, symptoms, activities of daily living, sport and recreational function, and knee-related quality of life over the past week.44 The KOOS includes 42 items across the five subscales with each item scored on a Likert scale from 0 (no problem or never) to 4 (extreme problem or always); the score is then converted to a 0-100 scale with a lower score representing more severe problems.44
Secondary Outcomes
One study used the LEFS to assess a patient’s perceived disablement with a 20-item questionnaire designed to assess a patient’s perceived level of difficulty completing different activities due to lower extremity injury.45 The LEFS items are scored on a Likert scale from 0 (extreme difficulty or unable to perform) to 4 (no difficulty) and the score for each is summed together for a total score; the maximum score on the LEFS is 80 points and indicates no functional limitations.45
One study used the GRoC which is a single-item measure to assess the patient’s perceptions of their overall improvement since the initial treatment.46 The GRoC is scored on a 15-point Likert Scale ranging from -7 (a very great deal worse) to +7 (a very great deal better).47 A change in score of 5 points or greater on the 15-point GRoC scale represents a clinically meaningful change.48
Three studies used range of motion (ROM) as a clinician-reported outcome measure used to assess joint motion. The normative ROM for knee flexion and extension ranges from 132.9° to 142.3° and 0.5° to 2.4° respectively.49
One study used the CSIM, which is a specific movement or muscle contraction that causes pain or is difficult for a patient to perform; the CSIM is rated on a scale from 0 (no difficulty or pain) to 10 (maximum difficulty or pain).50 The CSIM is used in the Mulligan Concept to identify what is painful for the patient and help the clincian use the appropriate directional force or glide to relieve pain throughout the previously painful movement. No validation of the CSIM has been done to date.
RESULTS
A total of 139 articles were initially identified from the search and 133 articles were excluded due to either being duplicates or not meeting the inclusion and exclusion criteria (Figure 1). A total of six articles met the inclusion and exclusion criteria for full-text review and were included in the analysis (Table 2). All eligible articles yielded a total of 72 subjects (Male=48, Female=24) ranging in age from 14-62 years. All patients were clinically diagnosed with a meniscal pathology through a physical exam; participant demographics and physical exam diagnostic criteria are presented in Table 1.
Quality Assessment
Six studies were included in the final analysis covering multiple designs and levels of evidence.21,24,26–29 Two RCTs, two case series, and two case studies were evaluated for quality using the appropriate measurements (Table 3). The two RCTs were graded down to Level 2 because of quality: both were scored as six or less on the PEDro scale indicating concerns with methodological quality. However, in the D&B checklist the Hudson RCT21 fell in the “excellent” range (26/32) while Kasturi28 fell in the “good” range (22/32). The case series were graded above a 6/10 demonstrating low risk of bias. Both case studies were assessed with the CARES checklist used for the reporting of a case study; both were able to answer “yes” to 75% or higher of the questions in the checklist. Table 1 details the assessment of each article included.
Intervention Protocol and General Findings Assessment
The total number of treatments used varied between studies. Kasturi28 was the only study without the total number of treatments reported; however, data was reported at three time points during the study. The number of treatments reported in the other studies varied between two and six.21,24,26,27,29 The time between treatments varied across all six studies ranging from 24 hours to 14 days.21,26 The specific intervention protocols and study timelines are described in Table 4.
Some of the patients were allowed to continue participation during treatment while other authors did not specify the amount of participation or restriction during treatment. Kasturi28 did not report on the level of activity before, during, or after treatment. Hudson et al21 only reported on discharge criteria and did not specify participation parameters. Sanchez24 reported that all the patients returned to participation but did not describe participation during the intervention. In the case series, Hudson et al27 reported that the patients were able to continue participation throughout treatment and returned to previous levels of activity. Brody et al26 and Rhinehart29 only reported that patients were able to return to previous levels of participation following the MC MWM treatment. No researcher reported any adverse reaction to the treatment or worsening of the symptoms following treatment.
Similar results were reported across the two RCTs.21,28 Kasturi28 reported both groups improved with rehabilitation; however, the treatment group with MC MWM had a statistically significant improvement in comparison to the control group consisting of conventional rehabilitation. Hudson et al21 also demonstrated statistically significant results for those in the treatment group and crossover group compared to the sham treatment.
Primary Outcomes
Pain
In the six included papers, the researchers reported decreases in pain that were either statistically significant or met the MCID of a two-point change on the NRS21,24,26–29,40All of the participants who received MC MWMs had a complete or near-complete resolution of pain (Table 5). Kasturi28 reported no significant difference after day one of treatment (p = 0.698) but a significant difference in NRS scores between the control group and the intervention group at four weeks with a mean difference of 1.65 (p = < 0.001), six weeks post intervention with a mean difference of 1.95 (p = < 0.001). Both groups had a reduction in pain on the NRS that exceeded the MCID. In their RCT, Hudson et al.21 did not report a statistically significant difference between the sham-control group and the intervention group after the final treatment for pain; however, the intervention group had over a two-point average reduction on the NRS and met the MCID, while the sham-control group did not meet the MCID for the NRS after the final treatment. Additionally, all the participants in the intervention group scored a two or less on the NRS scale following the final treatment.21
In the two included case series26,27 the researchers reported decreases in pain in as little as two treatments26 to an average of five treatments.27 In both cases, pain was reduced to near zero at discharge on the NRS.26,27 The total number of patients treated between the two-case series was seven with five of them from the Hudson et al.27 study. Two additional patients have been reported in the literature through two case studies.27,29 Both patients reported decreased pain in as few as three treatments.27,29 Both studies met the MCID with a greater than two-point change at discharge.27,29 In addition, both authors reported that the patients had less than 1/10 on the NRS at discharge.27,29
Function
Patient reported improvement in function was found on the PSFS (Table 6) in all six studies and the results were either statistically significant or met the MCID.21,24,26–29 In both RCTs,21,28 a statistically significant difference in the PSFS scores of the participants in the intervention group compared to the control group were found across each of the measured time points.21,28
Additionally, in a case series by Hudson et al.,27 each of the participants had an increase of at least 3 points on their PSFS by the time of discharge, meeting the MCID of 3.27,51 Furthermore, changes in patient reported function were reported to be statistically significant (p = 0.003) and a large effect size (d = 3.01) was reported.27,52 The other case series by Brody et al26 did not include inferential statistical analysis; however, both patients reported PSFS improvements which met the MCID value for the PSFS.
In a case study by Rhinehart,29 the participant had an increase in their average PSFS score by 4.75 points from initial visit to discharge (nine days), which also met the MCID for the PSFS. In another case study,24 the participant improved 2 points on their PSFS to reach the maximum 10 points from initial visit to discharge.
Multidimensional Health Status
Disablement in the Physically Active Scale (DPA)
In each of the five studies that reported on the DPA scale, either the MCID was met or a statistically significant change in DPA scores was reported (Table 7) indicating the patient’s perceived disability improved with treatment.21,24,26,27,29 The DPA scale was utilized in one RCT and a statistically significant difference (mean difference of 8.78 points; p = 0.013) was found between the MC MWM treatment group and the sham group.21 In the case series by Hudson et al.,27 each of the five participants had an improvement in their DPA scale at discharge: three of the five participants reported changes exceeding the MCID criterion, while the other two participants reported DPA scale scores within the reported ranges of healthy people prior to starting treatment.27,42 Brody et al.26 reported that the DPA score increased from intake to discharge for one participant and noted that the increase was due to increased life stress. In the two case studies, both patients reported a decrease in their DPA score with each visit.24,29
Knee Injury and Osteoarthritis Outcome Score
Two of the studies included the KOOS outcome measure to assess the patient’s perception of their knee injury and dysfunction.21,27 In a case series, Hudson et al.27 found the average change on the KOOS across participants was a 28.56 ± 5.68 point increase (i.e., improvement) from the initial exam to discharge, which was an average of 14.2 days across the five participants. In a randomized controlled trial, Hudson et al.21 observed an average increase (i.e., improvement) of 13.82 ± 10.94 points on the KOOS in participants in the MC ‘Squeeze’ treatment group, while there was only a 9.07 ± 11.13 average increase in the sham group. Five participants crossed over and completed the MC ‘Squeeze’ treatment and reported a mean increase of 21.28 ± 11.38 from completion of sham trial to completion of MC ‘Squeeze’ trial.
Secondary Outcomes
Lower Extremity Functional Scale
The LEFS was included as an outcome measure in a single case report.29 Researchers reported the patient had an initial score of 55. After four treatment sessions over the course of 9 days, the patient had attained a score of 80 points, which is the highest score possible indicating no perceived functional limitations were identified by the patient on the LEFS.29 Additionally, this patient maintained this score at both the one-week and one-month follow up after discharge.29
Global Rating of Change
The GRoC was used as an outcome measure in the case report by Rhinehart.29 The patient reported a score of +6 (A great deal better) following the first treatment session.29 The discharge exam for this patient occurred nine days after initial treatment, and a GRoC score of +7 (A very great deal better) was reported. The GRoC score was maintained at both the one-week and one-month follow-up appointments.29
Range of Motion
Three of the studies included knee ROM as an outcome measure (Table 8).26,28,29 In two of the studies, the patients had full knee range of motion by discharge.26,29 Additionally, in their case report, Rhinehart29 found improvements in ROM were maintained through the one-month follow-up. In an RCT, the researchers found a statistically significant mean difference of 7.5 (p = < 0.001) in ROM in the intervention group compared to the control group.28
Client Specific Impairment Measure
The Client Specific Impairment Measure (CSIM) outcome was included in a case report29 where the patient identified a body-weight squat and forward lunge as the motions causing pain and reported a 4 out of 10 for the squat and a 6 out of 10 for the lunge before treatment for pain/difficulty.29 Following the first treatment session, the CSIM scores improved to a 2; after the second treatment session, the reported CSIM scores were a 0 indicating no pain or difficulty with a body-weight squat or forward lunge. Scores of 0 on the CSIM were maintained through discharge, one-week, and one-month follow up.29
Follow-up Results
Follow-up data collection post-discharge (Table 9) was only conducted in two26,29 of the included studies. In the case report by Rhinehart,29 the patient completed four treatment sessions over the course of nine days and results were maintained or improved at follow-up. Brody et al26 obtained follow-up results from one participant, 21 weeks (~5 months) post discharge. The participant received two treatment sessions and was discharged three weeks after their initial evaluation, also reporting maintained or improved scores at follow-up.26
DISCUSSION
Researchers have reported that appropriate physical examination procedures can result in accurate diagnosis of meniscal pathology.6,7 Accurate identification of the condition, as well as determining if the patient will respond to conservative therapy, is important for healthcare professionals and researchers. The MC includes MWMs such as the ‘Squeeze’ technique, tibial IR, and tibial ER proposed to rapidly restore pain-free, functional ROM for patients with suspected meniscal injury which could enhance conservative care protocols and outcomes. The MWM techniques, however, have not been critically appraised via a systematic review. The purpose of this study was to evaluate the effectiveness of MC MWMs on patient-reported pain, function, and multi-dimensional health status in patients with clinically diagnosed meniscus pathologies.
Pain
Pain severity was assessed using the NRS in each of the included studies21,24,26–29 The application of MWMs in cases of clinically diagnosed meniscal pathology produced substantial improvements in pain severity. Improvements included complete or near-complete resolution of pain in as little as one week of treatment26 or in as few as one or two treatment sessions.24,26 Asymptomatic meniscal tears are common among healthy people indicating that the damaged meniscus may not need to be removed; thus, when pain is a primary complaint, conservative pain reduction therapies that successfully resolve this complaint may be sufficient.53 The use of MC MWMs, and specifically the MC ‘Squeeze’ technique, were found to be effective interventions for pain reduction in clinically diagnosed meniscal pathology over shorter durations (e.g., one month-follow-up) in the included literature. The included studies did not identify evidence to support the long-term effects of these interventions (e.g., length of pain resolution, relationship to OA development, etc.), patient-applied application of the techniques for symptom management, or outcomes of the techniques being applied as multimodal rehabilitation protocols. Thus, clinicians and researchers should consider measuring and assessing longer-term outcomes of these technique, outcomes from patient-application of the techniques, and how the incorporation of other intervention or exercise protocols may influence patient outcomes.
Function
The PSFS was used in all studies to assess patient-perceived functional improvements. The reported PSFS changes met the MCID and were statistically significant indicating the technique not only provided a reduction in pain but also restored function, as defined by the patient. The findings are valuable because pain and function are the primary symptoms for which patients seek treatment.11 In Kise et al,11 patients were divided into two groups following diagnosis of meniscal injury where one group was given exercise therapy alone while the other group received surgery alone. The exercise therapy group and those who underwent meniscal repair showed no significant difference after two years indicating a need for a treatment that will restore function and allow continued activity for otherwise healthy patients. While the MC ‘Squeeze’ technique seems promising to restore function in the short term, only two of the studies included any long-term follow-up26,29 with the longest follow-up point being 21 weeks post-discharge.26 Neither of the RCT’s21,28 did any long-term follow-up with the patients to see how long the treatment result lasted. The gold standard of surgical repair is not necessarily a long-term solution for the treatment of meniscal pathologies as some patients who have had surgery have needed additional surgery in as few as two years, and in the event of a failed repair that is asymptomatic, it is advisable to leave the meniscus alone instead of performing resection or another repair.16 Therefore, alternative treatment approaches are needed, and the MC ‘Squeeze’ technique could be a valuable tool for the mitigation of symptoms to restore function when a meniscal pathology is suspected.
Multidimensional Health Status
The DPA scale assesses physical impairment (e.g., pain, function) and quality of life in unique constructs. The included studies provide evidence that the MC ‘Squeeze’ technique improved multidimensional health status as measured by the DPA scale. Four of the studies21,24,27,29 found a statistically significant change (i.e., improvement) in DPA scores following treatment. Brody,26 however, identified impaired quality of life (QOL) score on this outcome measure in her case study through the course of treatment. The case report design allowed patient questioning that revealed the QOL impairment was perceived to be due to other life-related stress independent of knee pain. The implications of catching a change in life stress related to or independent of presenting pathologies could have long-term- treatment implications by informing future care decisions.54 Overall, the MC ‘Squeeze’ technique restored physical and QOL impairments as measured by the DPA scale, which is expected because physical improvements (e.g., pain reduction, increased function) are likely to correlate with improved QOL.55
The use of the KOOS could have addressed the lack of long-term follow-up data as it has been recommended as a long-term outcome measure for three months, six months, and a year.44 However, the researchers who included the KOOS did not collect discharge data further than 14 days after intake. The studies21,27 that used the KOOS revealed meaningful improvement in KOOS scores; however, KOOS data collected at wider intervals over a longer duration would have provided greater insight into long-term intervention effectiveness.
Secondary Outcomes
The secondary outcome measures included in the different studies were the LEFS, GRoC, ROM, CSIM, and follow-up treatment. Only Rhinehart29 reported on the LEFS and GRoC, and both measurements revealed patient improvement during the study. These results were corroborated with other scales (e.g., DPA KOOS) also used in the study and revealed improvement in pain, function, and QOL. The Rhinehart29 study was the only study to include the CSIM; the CSIM data collected supported the PSFS and NRS data corroborating increased function and decreased pain following treatment. It is not known, however, if CSIM data provides unique or redundant information compared to other measures (e.g., NRS, PSFS).
Joint ROM was assessed in three of the articles26,28,29 included in this review and was found to have increased following treatment. The increase in ROM was supported by patient-reported information found in other measures (e.g., NRS, PSFS, DPA scale) providing disease-oriented evidence supporting the patient-reported evidence. An advantage of assessing ROM in addition to patient reported outcomes is ROM provides quantifiable disease-oriented evidence supporting improvement. The collection of disease-oriented outcomes, in addition to patient-oriented outcomes, should be considered for future studies to further understand the effects of the MC ‘Squeeze’ technique along with tibial IR and ER MWM’s.
Limitations
Limitations are present in this review. While all studies found positive findings for patients treated using the MC techniques, the quality of evidence should be considered. Only two RCTs were identified,21,28 and case reports and case series made up two-thirds of the studies included in this review. A meta-analysis was unable to be conducted due to the limited number of published studies and the heterogeneity of the included studies. The lack of long-term follow-up in the included studies is also a limitation, as only two studies26,29 included follow up visits with participants’ post-discharge. The collection of longer-term outcomes, including patient-oriented and disease-oriented, would be valuable in redetermining the effectiveness of MC MWM for the treatment of meniscal pathologies. Thus, further high-quality RCTs are needed. The included studies generally lacked comparison to sham treatments, multimodal conservative treatment, diagnostic imaging, or surgical intervention. Finally, the included studies generally included adolescent through middle aged adults of a physically active population. While other studies have successfully used the MC for other knee pathologies (e.g., osteoarthritis) in older populations,56 the findings of the systematic review should be applied with caution across all populations.
Recommendations for Future Research
Future research is needed on the MC ‘Squeeze’ technique along with other MC techniques as indicated by the patient case and their effectiveness in the treatment of clinically diagnosed meniscal pathologies. Long-term follow-up with patients from six months to three years would be helpful in better understanding how effective the treatment is at reducing the need for surgery. Higher level RCTs with a control or sham treatment group assessing a wider age range would also be beneficial. Lastly, studies using diagnostic imaging (e.g., MRI) or surgery to confirm the presence, type, and location of a meniscal pathology would help to further assess the effectiveness of the MC treatment for meniscal lesions and provide insight on types of meniscal pathology that may not respond to MC intervention.26,29
CONCLUSION
The results of this systematic review provide initial support for the use of MC MWM techniques for conservative treatment of patients with a clinically diagnosed meniscal pathology. The MC MWMs reduced pain, increased function, increased knee range of motion, while decreasing patient reported symptoms of multidimensional health status impairment related to meniscus pathology. Future research should focus on using the MC MWM techniques as adjunct or stand-alone interventions, in more diverse patient populations, in imaging confirmed meniscal pathology, and with longer-term follow-up to better understand the effectiveness of the intervention.
Conflicts of interest
All authors declare that they do not have any conflict of interests with any of the topics discussed in this manuscript.