Abstract
Background
The World Health Organization defines suicide as the act of deliberately killing oneself. It is the second leading cause of death among 15-29 year olds globally.
Objective
To analyze the epidemiological profile and the spatial distribution of suicide deaths in the state of Sergipe.
Methods
We performed an ecological time-series study with data from the Brazilian Mortality Information System (Sistema de Informações sobre Mortalidade – SIM) about deaths by suicide occurring between 2000 and 2015. We considered as suicide deaths cases recorded as voluntary self-inflicted injuries. Suicide rates were estimated and age-adjusted in the population above 9 years. We analyzed temporal trends by sex and age groups using the simple linear regression model. For the spatial analysis, we performed Kernel density estimation with the software TerraView version 4.2.2.
Results
We identified 1,560 suicide cases in the state of Sergipe between 2000 and 2015, with a mean of 97.5 cases per year. We also observed that suicide rates in the state increased 102.3% (from 2.69/100,000 population in 2000 to 5.44 in 2015). Suicides occurred predominantly among males (1,160 cases; 74.35%), single people (1,010 cases; 64.7%), and brown-skinned people (1,039 cases; 66.6%). We observed significantly growing temporal trends in the general population, especially among male adults. Spatial analysis allowed us to draw a map that showed the regions with the highest occurrence of suicide.
Conclusion
We observed growing suicide trends in the state of Sergipe and the spatial analysis was an important tool that showed the areas with higher incidences of suicide.
Suicide; epidemiology; time-series studies; spatial analysis
Resumo
Introduçao
A Organização Mundial da Saúde define o suicídio como o ato de se matar deliberadamente. É a segunda principal causa de morte entre jovens de 15 a 29 anos no mundo.
Objetivo
Analisar o perfil epidemiológico e a distribuição espacial dos óbitos por suicídio no estado de Sergipe.
Métodos
Foi realizado estudo ecológico e de série temporal com dados do Sistema de Informações sobre Mortalidade (SIM) dos óbitos por suicídio ocorridos entre 2000 e 2015. Foram considerados suicídio os casos de mortes registrados como lesões voluntárias autoinfligidas. As taxas de suicídio foram estimadas e ajustadas por idade na população acima de 9 anos. Foram analisadas as tendências temporais por sexo e grupos etários usando o modelo de regressão linear simples. Para a análise espacial, foi realizada a estimativa de Kernel com o software TerraView 4.2.2.
Resultados
Foram identificados 1.560 casos de suicídio no estado de Sergipe entre 2000 e 2015, com média de 97,5 casos por ano. Observou-se um aumento de 102,3% das taxas de suicídio no estado (de 2,69/100.000 habitantes em 2000 para 5,44 em 2015). Os suicídios ocorreram predominantemente no sexo masculino (1.160 casos; 74,35%), em solteiros (1.010 casos; 64,7%) e pardos (1.039 casos; 66,6%). Foram observadas tendências temporais crescentes na população geral, especialmente entre adultos do sexo masculino. A análise espacial permitiu a construção de mapas exibindo as regiões com maiores concentrações de suicídio.
Conclusão
Observaram-se tendências crescentes de suicídio no estado de Sergipe e a análise espacial foi uma importante ferramenta ao mostrar áreas com maiores incidências de suicídio.
Suicídio; epidemiologia; estudos de séries temporais; análise espacial
Introduction
The World Health Organization (WHO) defines suicide as the act of deliberately killing oneself. It is the second leading cause of death among 15-29 year olds globally. Even though suicide rates have increased exponentially in recent years,11. World Health Organization, Department of Mental Health. Prevention of suicidal behaviors: a task for all. In: Mental and behavioral disorders. Geneva: WHO; 2000 this practice has been a common phenomenon throughout history among different peoples and cultures. It is a behavior with multifactorial determinants that can be triggered by a complex interaction of psychological and biological factors including genetic, cultural, social, and environmental elements.11. World Health Organization, Department of Mental Health. Prevention of suicidal behaviors: a task for all. In: Mental and behavioral disorders. Geneva: WHO; 2000,22. Skogman K, Alsén M, Öjehagen A. Sex differences in risk factors for suicide after attempted suicide: a follow-up study of 1052 suicide attempters. Soc Psychiatry Pschiatr Epidemiol. 2004;39:113-20. The WHO estimates that about 800,000 people commit suicide every year in the world (1 suicide every 40 seconds). It is thus among the world’s top 10 leading causes of death. The WHO also estimates that, until 2020, more than 1.5 million people will commit suicide.11. World Health Organization, Department of Mental Health. Prevention of suicidal behaviors: a task for all. In: Mental and behavioral disorders. Geneva: WHO; 2000,33. Bertolote JM, Fleischmann A. A global perspective in the epidemiology of suicide. Suicidologi. 2002;7:6-8.
The main factors associated with suicide are mental illness (mainly depression), alcohol/drug abuse or dependence, absence of social and familiar support, family suicide history, stressful events, and social and demographic characteristics (such as poverty, unemployment, and low educational levels).44. Fleischmann A, Bertolote JM, De Leo D, Botega N, Phillips M, Sisask M, et al. Characteristics of attempted suicides seen in emergency-care settings of general hospitals in eight low- and middle-income countries. Psychol Med. 2005;35:1467-74.,55. Botega NJ. Comportamento suicida: epidemiologia. Psico USP. 2014;25:231-6.
Brazil is the eighth country in the world regarding the absolute number of suicides. In 2012, 11,821 deaths by suicide were reported (30 per day), mostly committed by men (77.8%). Furthermore, from 2000 to 2012, an increase of 10.4% in suicide cases was observed. Among young people, suicide cases grew more than 30%.66. Waiselfisz JJ. Mapa da violência 2014. Rio de Janeiro: CEBELA-FLACSO; 2014.
In Brazil, deaths due to external causes are growing in contrast to deaths caused by infectious and parasitic diseases. Within these trends, suicide is the third cause of death due to external factors (6.8%), following homicides (36.4%) and traffic accidents (29.3%).77. Reichenheim ME, Souza ER, Moraes CL, Mello Jorge MH, Silva CM, Souza Minayo MC, et al. Violence and injuries in Brazil: the effect, progress made, and challenges ahead. Lancet. 2011;377:1962-75.
Several studies have reported an increase in suicide rates in Brazil.88. Lovisi GM, Santos SA, Legay L, Abelha L, Valencia E. Epidemiological analysis of suicide in Brazil from 1980 to 2006. Rev Bras Psiquiatr. 2009;31(suppl. 2):S86-94. The understanding of these epidemiological scenarios may support the elaboration, planning, and implementation of public policies and intervention strategies. Therefore, the objective of this study was to analyze the epidemiological profile and spatial distribution of suicide cases in the state of Sergipe (from 2000 to 2015) and to describe the temporal trends of specific mortality rates according to gender and age group.
Methods
Design and study area
We performed an ecological time-series study using secondary data. We obtained mortality data from the Mortality Information System (Sistema de Informações sobre Mortalidade – SIM) of the Department of Informatics of the Brazilian Unified Health System (DATASUS) in the Sergipe State Health Department. We analyzed the historical data on suicide – codes X60 to X84 according to the International Classification of Diseases, 10th revision (ICD-10)99. World Health Organization. International statistical classification of diseases, injuries, and causes of death. 10th ed. Geneva: WHO; 1992. – from 2000 to 2015 in the municipalities of the state of Sergipe. We also evaluated the social and demographic characteristics of the study subjects, such as age, ethnicity, gender, municipality of residence, death rate by suicide, place of suicide, and type of suicide.
The state of Sergipe is located in the northeastern Atlantic coast of Brazil and comprises 75 municipalities (Figure 1). It has a population of 2,068,017 inhabitants and an area of 21,910,354 km2, equivalent to 0.26% of the Brazilian territory.1010. Instituto Brasileiro de Geografia e Estatística (IBGE). IBGE Cidades. 2010 [Internet]. [cited 2017 Jan 5]. http://www.ibge.gov.br
http://www.ibge.gov.br...
Statistical analyses
Suicide mortality rates were calculated for each year (2000-2015). To investigate the presence of factors associated with suicide, we compared social and demographic variables with absolute and relative frequencies (proportions, ratios, and rates). We used the population count provided by the Brazilian Institute for Geography and Statistics (Instituto Brasileiro de Geografia e Estatística – IBGE) for those years.
We analyzed annual suicide trends according to gender and age group using linear regression. For this, we used the formula , where y refers to the annual rate of suicide deaths and (x) refers to the respective year. The annual percentage change (APC) for suicide mortality in the period under study was calculated according to the formula below1111. Antunes JLF, Waldman EA. Trends and spatial distribution of deaths of children aged 12-60 months in São Paulo, Brazil, 1980-98. Bull World Health Organ. 2002;80:391-8.:
Statistical analyses were performed with GraphPad Prism version 5.01 and Microsoft Office Excel 2010 software. We used the G test to analyze differences among the genders (male and female) according to age, ethnicity, marital status, suicide method and place of occurrence. We used the G test because it is recommended to compare multiples variables. Results were considered statistically significant when p < 0.05.
According to these classification parameters, suicide mortality was classified as low (< 5 deaths/100,000 population), medium (5-15 deaths/100,000 population), high (15-30 deaths/100,000 population), and very high (≥ 30 deaths/100,000 population).1212. Diekstra RFW, Gulbinat W. The epidemiology of suicidal behaviour: a review of three continents. World Health Stat Q. 1993;46:52-68.
Spatial analyses
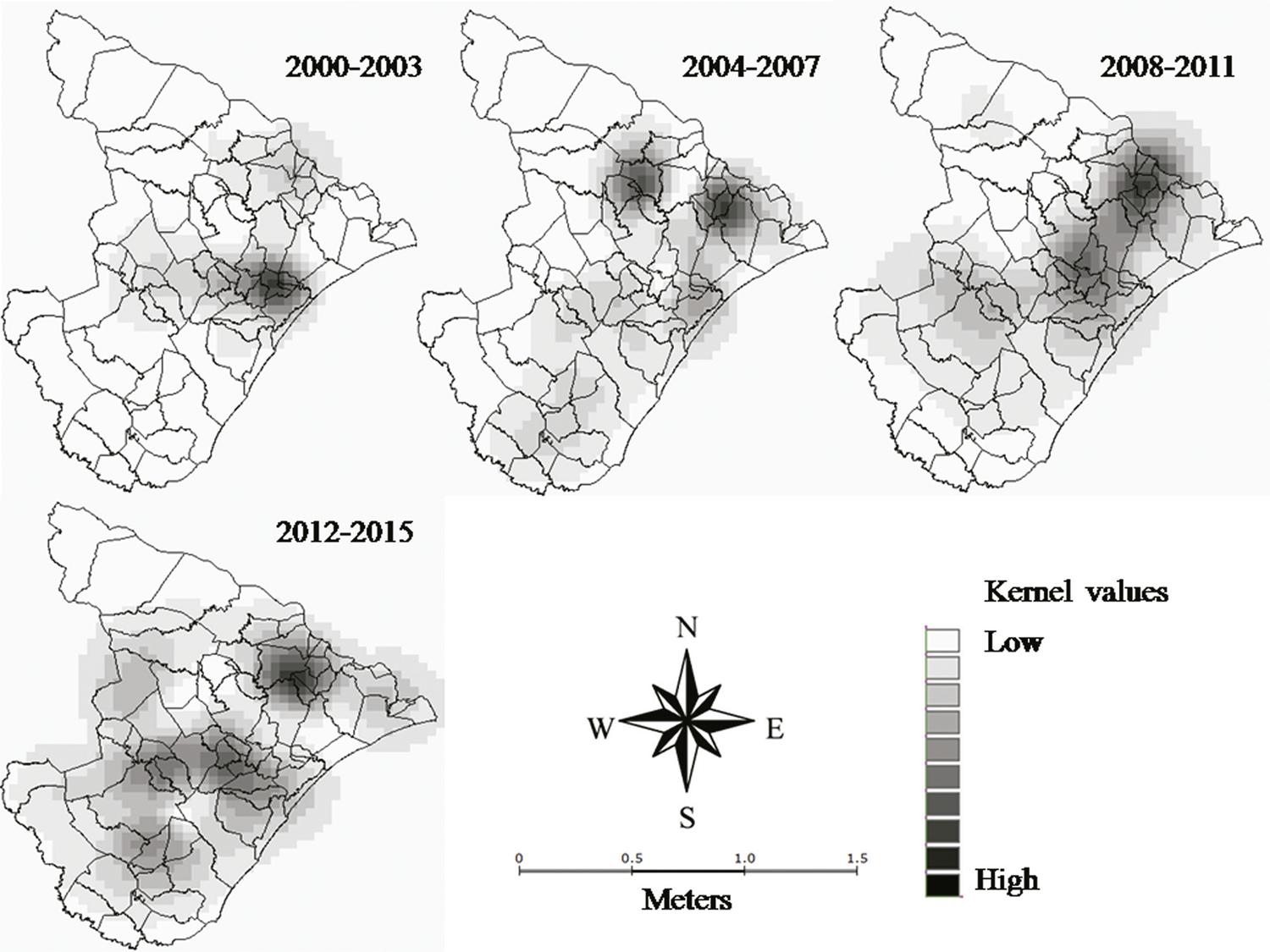
We built thematic maps according to suicide rates by municipality in each year using Kernel intensity estimators. The Kernel analysis generated a smooth density surface for the visual detection of hot spots, indicating agglomeration in a spatial distribution and continuous surface of data points and areas.1313. Bailey T, Gatrell AC. Interactive spatial data analysis. New York: Longman Scientific & Technical; 1995. We designed choropleth maps using the incidence rates from four time periods (2000-2003, 2004-2007, 2008-2011, and 2012-2015). We used the Quartz function to identify surfaces according to case density. Spatial analyses were performed using TerraView software version 4.2.2.1414. TerraView version 4.2.2. São José dos Campos: INPE; 2010. We also used the cartographic base of the state of Sergipe (available in digital format from IBGE) to design the maps.1010. Instituto Brasileiro de Geografia e Estatística (IBGE). IBGE Cidades. 2010 [Internet]. [cited 2017 Jan 5]. http://www.ibge.gov.br
http://www.ibge.gov.br...
Ethical considerations
This research involved human subjects and adhered to the protocols of Resolution 466/2012 from the Brazilian Committee for Ethics in Research (Comissão Nacional de Ética em Pesquisa – CONEP). Ethics committee approval was replaced with a term for the use for secondary data signed by the State Director of Health Surveillance. The authors have complied with the ethical principles contained in the Helsinki Declaration.
Results
We observed that suicide rates in the state of Sergipe increased linearly from 2000 to 2015 (2.69/100,000 population to 5.44/100,000 population, respectively; Table 1). These data represented a growth percentage of 102.3%. The mean coefficient of suicide mortality in that period was 4.8/100,000 population, considered low.1212. Diekstra RFW, Gulbinat W. The epidemiology of suicidal behaviour: a review of three continents. World Health Stat Q. 1993;46:52-68. The mean coefficient of mortality was higher among males (7.33) than among females (2.44).
Number of suicide deaths, estimated population and specific mortality rate in the state of Sergipe, Brazil, 2000-2015
We identified 1,560 cases of suicide (mean ± standard deviation = 100.8±19.2 per year). Regarding gender, we observed a higher percentage of cases in males (1,160; 74.4%) than in females (400; 25.6%; Table 2). In addition, the highest percentage of suicide deaths occurred among young adults and adults (76.6% in 20-59 year olds). We also analyzed social and demographic characteristics according to gender and observed that, among men, the highest percentage of deaths occurred in the age groups of 20-29 (25.4%) and 30-39 (24.7%) years. Similarly, we observed a greater percentage of deaths among women aged 20-29 (24.5%) and 30-39 (19.3%) years. Finally, we also observed a higher prevalence of suicide among single people – both male (65.9%) and female (61.3%; p < 0.0001) – when compared to other marital status groups. Regarding ethnicity, the highest percentage of cases of suicide was reported among brown-skinned people (male 69.1%, female 59.5%; p < 0.0001). The most common suicide methods included hanging (54.7%), poisoning (28.7%), and firearm use (7.7%). The main method used by males was hanging (60.9%), while females preferred poisoning (47.8%). Most of them committed suicide at home (55.2%).
Our data revealed that suicide rates showed a general rising trend from 2000 to 2015 (Figure 2). Trend model equations showed a rising pattern and statistically significant results for the overall suicide mortality rate in the state of Sergipe (p = 0.0003; Table 3) and for suicide rates among men (p = 0.0003). Regarding age, we observed a significant increasing trend among adults only (p = 0.05).
In agreement with the spatial data analysis, the occurrence of suicides followed a random, heterogeneous pattern, with annual variations (Figure 3) related to both the size of the territory and the concentration of cases in certain regions. The Kernel density estimator showed the areas with the highest suicide rates (darker areas represent higher clusters of cases) through data interpolation.
Discussion
Our results showed that the mean suicide rate in the state of Sergipe over the 2000-2015 period was 4.8 cases/100,000 population, which indicates that the state has a low level of suicide mortality according to WHO parameters (< 5 deaths/100,000 population).1212. Diekstra RFW, Gulbinat W. The epidemiology of suicidal behaviour: a review of three continents. World Health Stat Q. 1993;46:52-68. However, suicide rates according to gender indicated that men showed a medium level of suicide, while women had a low classification. In addition, we observed a growing trend of suicide rates in Sergipe, which is considered a serious public health problem. Moreover, the male-to-female morality ratio was approximately 3:1. Similar results were observed in other localities, with ratios ranging from 3:1 to 7.5:1, corroborating our findings that show significantly higher suicide rates among men.1515. Marín-León L, Barros MB. Suicide mortality: gender and socioeconomic differences. Rev Saude Publica. 2003;37:357-63.
16. Macente LB, Zandonade E. A study of the historic series on mortality per suicide in Espírito Santo, Brazil (from 1980 to 2006). J Bras Psiquiatr. 2011;60:151-7.-1717. Machado DB, Santos DN, Machado DB, Santos DN. Suicídio no Brasil, de 2000 a 2012. J Bras Psiquiatr. 2015;64:45-54.
The high rate of suicide among men is related to behavioral trends that include competitiveness, impulsivity, and difficulty expressing their feelings due to social and family pressure. Moreover, men would also be more susceptible when they are unable to fulfill traditional gender roles, being more sensitive to situations such as unemployment, impoverishment or failure to perform as a provider.1212. Diekstra RFW, Gulbinat W. The epidemiology of suicidal behaviour: a review of three continents. World Health Stat Q. 1993;46:52-68.,1717. Machado DB, Santos DN, Machado DB, Santos DN. Suicídio no Brasil, de 2000 a 2012. J Bras Psiquiatr. 2015;64:45-54.,1818. Leal OF. Suicídio, honra e masculinidade na cultura gaúcha. Cad Antropol UFRGS. 1992;6:7-21. In turn, among women, the lower incidence of suicide has been associated with a lower prevalence of alcoholism, stronger religious beliefs, and more flexible attitudes toward social skills. In addition, women recognize early signs and risk factors for depression, suicide, and mental illness, seeking help in times of crisis.1919. Minayo MC. A autoviolência, objeto da sociologia e problema de saúde pública. Cad Saude Publica. 1998;14:421-8.
20. Serrano AI. Impactos da modernidade sobre as pulsões autodestrutivas: ciências sociais e intervenção psiquiátrica [dissertation]. Florianópolis: Universidade Federal de Santa Catarina; 2003.
21. Meneghel SN, Victora CG, Faria NM, Carvalho LA, Falk JW. Epidemiological aspects of suicide in Rio Grande do Sul, Brazil. Rev Saude Publica. 2004;38:804-10.-2222. Stallones L, Beseler C, Hayes A, Wise R, Weir F, Mearns J, et al. Pesticide poisoning and depressive symptoms among farm residents. Ann Epidemiol. 2002;12:389-94.
The lethality of suicide methods is not directly related to the intention of death, but rather to the methods preferred according to gender. For example, among women, the use of medication as a suicide method is more common than among men.2323. Canetto SS, Sakinofsky I. The gender paradox in suicide. Suicide Life Threat Behav. 1998;28:1-23. The opposite is observed in relation to firearm use. It is also known that, although the prevalence of suicide attempts among women is higher, men have more success in their attempts. That is because men tend to choose more violent and fatal methods.2424. Souza ER, Minayo MC, Malaquias JV. Suicide among young people in selected Brazilian state capitals. Cad Saude Publica. 2002;18:673-83. Among men, the main suicide method in Sergipe was hanging. This was the method used in about half of the deaths. Similar data were reported in other studies.1515. Marín-León L, Barros MB. Suicide mortality: gender and socioeconomic differences. Rev Saude Publica. 2003;37:357-63.,2121. Meneghel SN, Victora CG, Faria NM, Carvalho LA, Falk JW. Epidemiological aspects of suicide in Rio Grande do Sul, Brazil. Rev Saude Publica. 2004;38:804-10.,2525. Vidal CEL, Gomes CB, Mariano CA, Leite LMR, Silva RA, Lasmar SC. Perfil epidemiológico do suicídio na microrregião de Barbacena, Minas Gerais, no período de 1997 a 2012. Cad Saude Coletiva. 2014;22:158-64.
In relation to the high percentage of suicide by poisoning, especially among women, it is important to highlight the easy access, in Brazil, to toxic and illegal substances such as aldicarb, pesticides, domestic class rodenticides, medicines, unspecified harmful substances, narcotics, and hallucinogens.1717. Machado DB, Santos DN, Machado DB, Santos DN. Suicídio no Brasil, de 2000 a 2012. J Bras Psiquiatr. 2015;64:45-54.,2626. Hawton K, van Heeringen K. Suicide. Lancet. 2009;373:1372-81
Regarding age, we observed an increasing and significant suicide trend among adults. The trend exhibited by our data corroborates the results reported in other studies.2727. Brzozowski FS, Soares GB, Benedet J, Boing AF, Peres MA. Suicide time trends in Brazil from 1980 to 2005. Cad Saude Publica. 2010;26:1293-302. Among the elderly, the increasing rate may be associated with classical reasons such as comorbidities and end-of-life depression.2828. Bando DH, Brunoni AR, Fernandes TG, Benseñor IM, Lotufo PA. Suicide rates and trends in São Paulo, Brazil, according to gender, age and demographic aspects: a joinpoint regression analysis. Rev Bras Psiquiatr. 2012;34:286-93. Conversely, high suicide rates among young people may be associated with lower religious support,2929. Stack S. Suicide: a 15-year review of the sociological literature. Part I: cultural and economic factors. Suicide Life Threat Behav. 2000;30:145-62. living with stepparents or single parents,3030. Gunnell D, Middleton N, Whitley E, Dorling D, Frankel S. Why are suicide rates rising in young men but falling in the elderly? A time-series analysis of trends in England and Wales 1950-1998. Soc Sci Med. 2003;57:595-611. high unemployment rates,2121. Meneghel SN, Victora CG, Faria NM, Carvalho LA, Falk JW. Epidemiological aspects of suicide in Rio Grande do Sul, Brazil. Rev Saude Publica. 2004;38:804-10. and alcohol or drug abuse.44. Fleischmann A, Bertolote JM, De Leo D, Botega N, Phillips M, Sisask M, et al. Characteristics of attempted suicides seen in emergency-care settings of general hospitals in eight low- and middle-income countries. Psychol Med. 2005;35:1467-74. Even though we have observed differences between the variables analyzed according to the gender of the person who committed suicide, the statistical test used (G test) does not allow to identify in which groups specifically there are differences. Unfortunately the non-use of a post-hoc test is a limitation of our work.
The spatial analysis of the cases allowed us to identify the areas with the highest suicide rates in the state of Sergipe. Our maps revealed clusters in the north region and along the east coast of the state. Moreover, Kernel density analysis showed that the central-eastern region of the state is the area at the highest risk of suicide (areas with clusters in all temporalities analyzed). The lowest occurrences were observed on the west coast and in the northwest region (areas without clusters in all analyzed periods).
Underreporting of cases is one of the limitations of the present study. It may be related to the incorrect completion of death certificates or to the deliberate omission of the actual cause of death, as a result of sociocultural factors or family prejudice. Frequently, in cases of suicide, family members try to hide the real cause of death or to negotiate it with those who notify the death. This reveals the difficulties that many families have in accepting suicide.1515. Marín-León L, Barros MB. Suicide mortality: gender and socioeconomic differences. Rev Saude Publica. 2003;37:357-63.,1919. Minayo MC. A autoviolência, objeto da sociologia e problema de saúde pública. Cad Saude Publica. 1998;14:421-8. Another limitation of our study was the temporal trend analysis performed using a simple linear regression model. Even though this test is not the gold standard, it was possible to observe an increasing tendency of mortality by suicide in Sergipe. Future studies could pursue more robust statistical analyses of these data.
Knowledge about suicide trends, its main causes, methods employed, and risk scenarios are of great importance to the formulation and structuring of prevention programs and the consequent elaboration of more specific and effective prevention strategies. Furthermore, the early identification of people at risk is crucial for the adoption of preventive measures. In this context, health professionals play an important role in identifying crucial emergency moments and advising relatives or friends to provide better support.1717. Machado DB, Santos DN, Machado DB, Santos DN. Suicídio no Brasil, de 2000 a 2012. J Bras Psiquiatr. 2015;64:45-54.
In summary, our data reveal an increase in the general suicide trend in the state of Sergipe, which represents an important public health problem. Our study also revealed that men show higher suicide rates than women. The issue of suicide demands attention from professionals from different areas who can deal with the risks and possibilities of prevention.
Acknowledgements
The authors would like to thank the Divisão de Vigilância Epidemiológica (DIVEP), Secretaria de Saúde do Estado de Sergipe (SES), and the board of Instituto de Medicina Legal do Estado de Sergipe for providing information. This study did not receive financial support.
References
-
1World Health Organization, Department of Mental Health. Prevention of suicidal behaviors: a task for all. In: Mental and behavioral disorders. Geneva: WHO; 2000
-
2Skogman K, Alsén M, Öjehagen A. Sex differences in risk factors for suicide after attempted suicide: a follow-up study of 1052 suicide attempters. Soc Psychiatry Pschiatr Epidemiol. 2004;39:113-20.
-
3Bertolote JM, Fleischmann A. A global perspective in the epidemiology of suicide. Suicidologi. 2002;7:6-8.
-
4Fleischmann A, Bertolote JM, De Leo D, Botega N, Phillips M, Sisask M, et al. Characteristics of attempted suicides seen in emergency-care settings of general hospitals in eight low- and middle-income countries. Psychol Med. 2005;35:1467-74.
-
5Botega NJ. Comportamento suicida: epidemiologia. Psico USP. 2014;25:231-6.
-
6Waiselfisz JJ. Mapa da violência 2014. Rio de Janeiro: CEBELA-FLACSO; 2014.
-
7Reichenheim ME, Souza ER, Moraes CL, Mello Jorge MH, Silva CM, Souza Minayo MC, et al. Violence and injuries in Brazil: the effect, progress made, and challenges ahead. Lancet. 2011;377:1962-75.
-
8Lovisi GM, Santos SA, Legay L, Abelha L, Valencia E. Epidemiological analysis of suicide in Brazil from 1980 to 2006. Rev Bras Psiquiatr. 2009;31(suppl. 2):S86-94.
-
9World Health Organization. International statistical classification of diseases, injuries, and causes of death. 10th ed. Geneva: WHO; 1992.
-
10Instituto Brasileiro de Geografia e Estatística (IBGE). IBGE Cidades. 2010 [Internet]. [cited 2017 Jan 5]. http://www.ibge.gov.br
» http://www.ibge.gov.br -
11Antunes JLF, Waldman EA. Trends and spatial distribution of deaths of children aged 12-60 months in São Paulo, Brazil, 1980-98. Bull World Health Organ. 2002;80:391-8.
-
12Diekstra RFW, Gulbinat W. The epidemiology of suicidal behaviour: a review of three continents. World Health Stat Q. 1993;46:52-68.
-
13Bailey T, Gatrell AC. Interactive spatial data analysis. New York: Longman Scientific & Technical; 1995.
-
14TerraView version 4.2.2. São José dos Campos: INPE; 2010.
-
15Marín-León L, Barros MB. Suicide mortality: gender and socioeconomic differences. Rev Saude Publica. 2003;37:357-63.
-
16Macente LB, Zandonade E. A study of the historic series on mortality per suicide in Espírito Santo, Brazil (from 1980 to 2006). J Bras Psiquiatr. 2011;60:151-7.
-
17Machado DB, Santos DN, Machado DB, Santos DN. Suicídio no Brasil, de 2000 a 2012. J Bras Psiquiatr. 2015;64:45-54.
-
18Leal OF. Suicídio, honra e masculinidade na cultura gaúcha. Cad Antropol UFRGS. 1992;6:7-21.
-
19Minayo MC. A autoviolência, objeto da sociologia e problema de saúde pública. Cad Saude Publica. 1998;14:421-8.
-
20Serrano AI. Impactos da modernidade sobre as pulsões autodestrutivas: ciências sociais e intervenção psiquiátrica [dissertation]. Florianópolis: Universidade Federal de Santa Catarina; 2003.
-
21Meneghel SN, Victora CG, Faria NM, Carvalho LA, Falk JW. Epidemiological aspects of suicide in Rio Grande do Sul, Brazil. Rev Saude Publica. 2004;38:804-10.
-
22Stallones L, Beseler C, Hayes A, Wise R, Weir F, Mearns J, et al. Pesticide poisoning and depressive symptoms among farm residents. Ann Epidemiol. 2002;12:389-94.
-
23Canetto SS, Sakinofsky I. The gender paradox in suicide. Suicide Life Threat Behav. 1998;28:1-23.
-
24Souza ER, Minayo MC, Malaquias JV. Suicide among young people in selected Brazilian state capitals. Cad Saude Publica. 2002;18:673-83.
-
25Vidal CEL, Gomes CB, Mariano CA, Leite LMR, Silva RA, Lasmar SC. Perfil epidemiológico do suicídio na microrregião de Barbacena, Minas Gerais, no período de 1997 a 2012. Cad Saude Coletiva. 2014;22:158-64.
-
26Hawton K, van Heeringen K. Suicide. Lancet. 2009;373:1372-81
-
27Brzozowski FS, Soares GB, Benedet J, Boing AF, Peres MA. Suicide time trends in Brazil from 1980 to 2005. Cad Saude Publica. 2010;26:1293-302.
-
28Bando DH, Brunoni AR, Fernandes TG, Benseñor IM, Lotufo PA. Suicide rates and trends in São Paulo, Brazil, according to gender, age and demographic aspects: a joinpoint regression analysis. Rev Bras Psiquiatr. 2012;34:286-93.
-
29Stack S. Suicide: a 15-year review of the sociological literature. Part I: cultural and economic factors. Suicide Life Threat Behav. 2000;30:145-62.
-
30Gunnell D, Middleton N, Whitley E, Dorling D, Frankel S. Why are suicide rates rising in young men but falling in the elderly? A time-series analysis of trends in England and Wales 1950-1998. Soc Sci Med. 2003;57:595-611.
Publication Dates
-
Publication in this collection
23 Aug 2018 -
Date of issue
Oct-Dec 2018
History
-
Received
17 May 2017 -
Accepted
08 Jan 2018