Article Text

Statistics from Altmetric.com
A 57 year old female non-smoker with no asbestos exposure was admitted with right chest pain and fever. Magnetic resonance imaging revealed a huge mass occupying the right hemithorax (fig 1). She underwent right posterolateral thoractomy following a negative bronchoscopic examination with transbronchial lung biopsy and transthoracic needle biopsy. A giant, well circumscribed, lobulated solitary tumour 13 cm in diameter attached with a pedicle to the visceral pleura was surgically removed (fig 2A). Macroscopically, the tumour was nearly protruding into the pleural space, compressing the right lower lobe upwards and presenting as a pleural mass. Histological examination showed poorly differentiated adenocarcinoma of the lung (fig 2B). A CT scan performed 12 months after surgery showed a well defined homogeneous mass abutting the pleura in the right lung. The most likely diagnosis was a local relapse of adenocarcinoma of the lung. She was treated with platinum-based chemotherapy and docetaxel and gefinitib. With no evidence of distant metastasis and no efficacy of chemotherapy, right lateral thoracotomy was performed. Pathological examination showed a recurrence of adenocarcinoma of the lung. The patient remains healthy 36 months after the initial diagnosis.

(A) T1-weighted coronal and (B) sagittal MR images showing a heterogeneous mass in the right lower hemithorax (curved arrows) associated with compression and displacement of the right lower lobe (straight arrow) and right hemidiaphragm.

{kind=link}
{kind=link}
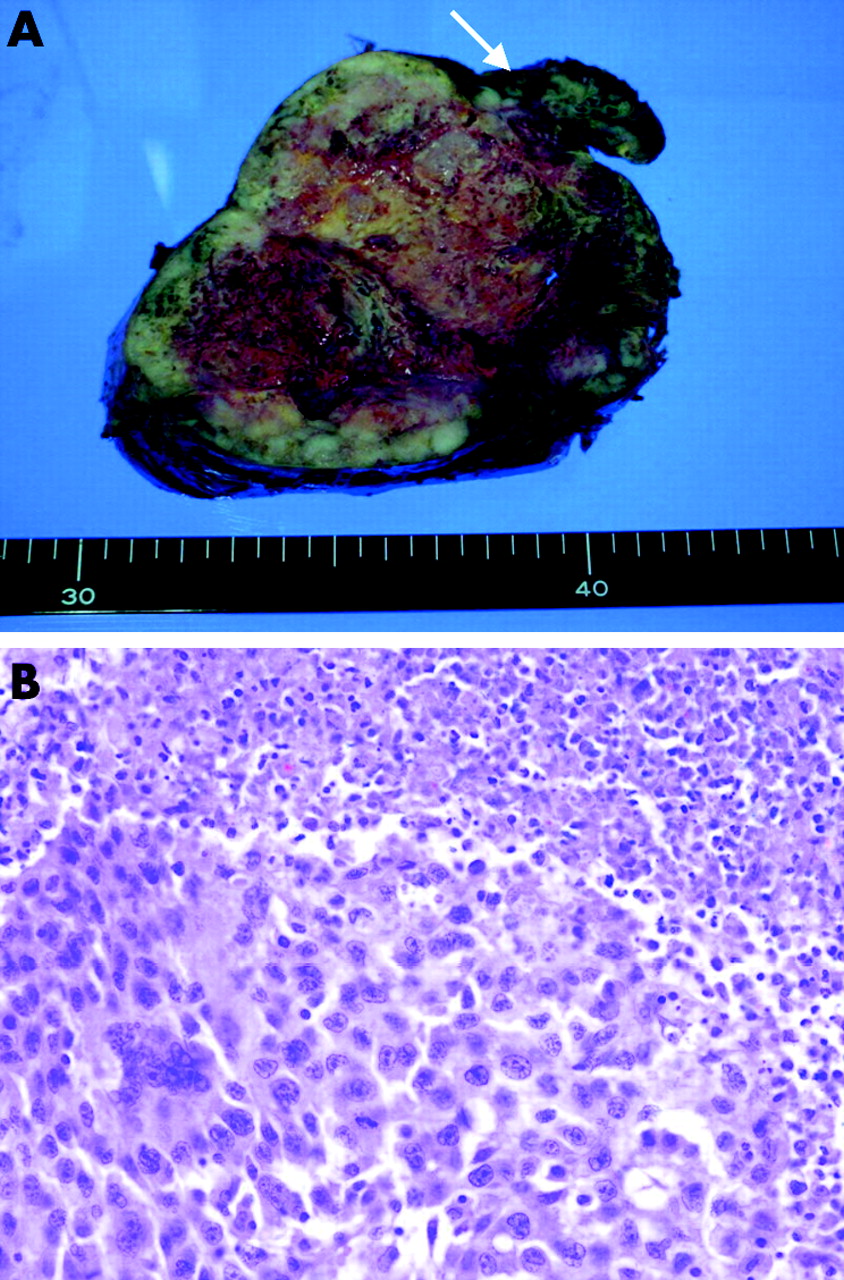
(A) Gross pathological specimen showing a yellowish encapsulated mass attached with a pedicle to the visceral pleura (arrow). (B) Histological section showing poorly differentiated adenocarcinoma.
Pulmonary adenocarcinoma with a localised extrapulmonary growth pattern presenting as a localised pleural tumour has not previously been described. Primary lung cancer mimicking pleural neoplasm—“pseudomesotheliomatous carcinoma”—is considered to represent a type of peripheral lung adenocarcinoma with a distinctive diffuse growth pattern.1 The clinical similarities between the present case and pseudomesotheliomatous carcinoma are the marked extrapulmonary growth and the presence of a small subpleural nodule. Although the pattern of recurrence also showed a localised pleural mass, surgery for metastases can improve survival.
Leaning points
-
Pulmonary adenocarcinoma with a localised extrapulmonary growth pattern presenting as a giant localised pleural mass is extremely rare.
-
The differential diagnosis of a large localised pleural tumour includes peripheral bronchial carcinoma.
-
Even if the pattern of recurrence reveals a localised mass, surgery for recurrence is controversial as there is a possibility of micrometastases, but it may improve survival in highly selected patients with lung cancer.