Article Text

Abstract
Objectives Although uric acid lowering therapies, including xanthine oxidase (XO) inhibition, may reduce the absolute level of blood pressure (BP), the effect of XO inhibition on BP variability is largely unknown. The aim of the present analysis was to evaluate the impact of febuxostat, an XO inhibitor, on BP variability in a randomised trial setting.
Methods This was a subanalysis of the PRIZE Study, a randomised trial to evaluate the potential effect of febuxostat on carotid intima–media thickness progression. Patients with hyperuricemia and carotid plaques were randomly assigned to the febuxostat or control group. During a 24-month period, office BP and pulse rate (PR) were measured ≥3 times. BP and PR variabilities were assessed with SD and coefficient of variation (CV). The effect of febuxostat on BP and PR variabilities was adjusted with age, sex and baseline BP or PR, expressed with 95% CIs.
Results A total of 472 patients were included into the present subanalysis. During the 24-month follow-up period, the febuxostat group had a significantly lower adjusted mean systolic BP (128.4 (126.8–130.0) vs 130.7 (129.1–132.2) mm Hg, p=0.04) and CV of systolic BP (7.4 (6.7–8.0) vs 8.2 (7.6–8.8), p=0.04) than the control group. Adjusted SD of PR was also lower in the febuxostat group than their counterpart (5.95 (4.93–6.97) vs 7.33 (6.32–8.33), p=0.04).
Conclusion XO inhibition with febuxostat was associated with reduced visit-to-visit BP variability as well as reduced PR variability in patients with hyperuricemia and carotid plaques.
Trial registration numbers University Hospital Medical Information Network Clinical Trial Registry (UMIN000012911 and UMIN000041322).
- hypertension
- gout
- cardiovascular diseases
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Uric acid lowering therapy with xanthine oxidase (XO) inhibition may reduce the absolute level of blood pressure (BP), although the effect on BP variability is unknown.
WHAT THIS STUDY ADDS
XO inhibition with febuxostat reduced visit-to-visit BP variability in patients with hyperuricemia and carotid plaques.
Febuxostat treatment was also associated with reduced PR variability.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
XO inhibition with febuxostat may have a potential benefit to reduce the absolute BP level and BP variability.
Introduction
Hyperuricemia is closely associated with hypertension, the most common treatable risk factor for cardiovascular disease.1 2 Given the high prevalence of hypertension in patients with hyperuricemia and gout, it is conceivable that hypertension treatment is essential in a setting of hyperuricemia. Systemic blood pressure (BP) has a dynamic nature and varies from beat to beat, day to day and clinic visit to visit. Absolute mean BP is important in the development of cardiovascular disease, but BP variability may also play a part. BP variability reflects atrial stiffness, endothelial function, sympathetic nerve activation and other intrinsic and social factors.3 Among various types of fluctuation, visit-to-visit BP variability has been well studied and is recognised as a predictor of dementia, end-stage renal disease, cardiovascular events, including coronary artery disease and stroke, and all-cause mortality.4 5 Despite the established prognostic impact of increased visit-to-visit BP variability, therapeutic implications and approaches for this phenomenon are unclear.6 It is well known that the effect of antihypertensive agents on reducing BP variability is not equivalent among different drug classes. In previous studies, calcium-channel blockers rather than β-blockers and ACE inhibitors were associated with reduced BP variability.7 8 In this context, uric acid lowering therapies, including xanthine oxidase (XO) inhibition, may reduce BP, especially in selected populations.1 9–11 For instance, XO inhibition with allopurinol has been shown to reduce absolute BP levels in previous randomised, double-blind, placebo-controlled studies. However, the sample size was small in the randomised studies,9 10 and the effect of XO inhibitor on BP variability is largely unknown. The aim of the present analysis was to evaluate the impact of febuxostat, an XO inhibitor, on BP and its variability in a randomised trial setting.
Methods
Study design and participants
This is a subanalysis of the PRIZE Study, a multicentre, prospective, randomised, open-label, blinded-endpoint trial to assess a hypothesis if febuxostat delays carotid intima–media thickness (IMT) progression in patients with hyperuricemia. The detailed study protocol and design are described in previous publications.12–16 Briefly, patients with hyperuricemia (serum uric acid (SUA) level>7.0 mg/dL) and carotid plaques (maximum IMT of the common carotid artery≥1.1 mm) at screening were enrolled. Major exclusion criteria included uric acid lowering medications within 8 weeks prior to assessment of eligibility and gouty tophus or symptoms of gout arthritis within 1 year. Patients who met the entry criteria were randomly assigned 1:1 in an open-label manner to either the febuxostat or control group. All participants in both groups underwent appropriate lifestyle modification for hyperuricemia. Patients in the febuxostat group received an initial dose of 10 mg/day, followed by 20 mg/day at 1 month and 40 mg/day at 2 months, if tolerated. Febuxostat 40 mg/day was targeted as the maintenance dose, but an increased dose up to 60 mg/day at 3 months or later was also permitted. In the PRIZE Study, office BP was recorded at baseline and at 6, 12 and 24 months. In patients who discontinued participation in the PRIZE Study during the follow-up period, office BP was also measured at the last study visit. Office BP and pulse were measured in a sitting position after at least 5 min at rest among study participating centres. BP measurement times were kept as constant as possible throughout the study period.13 In the present subanalysis, patients were considered eligible when office BP was evaluated at baseline and was measured ≥3 times during the study period. Thus, a total of 472 patients were included in this subanalysis (figure 1).
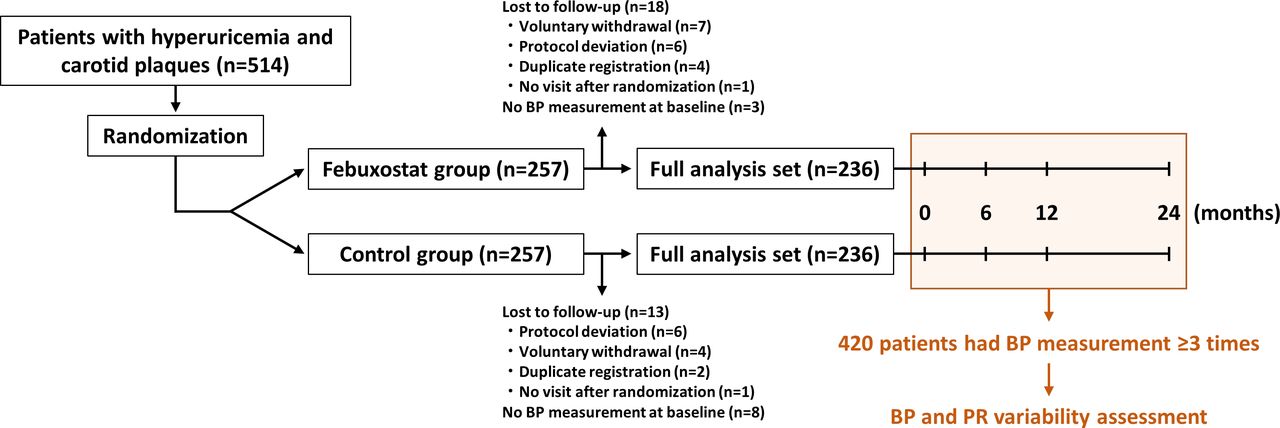
Study flow. A total of 16 out of 472 (3.4%) patients who discontinued participation in the study had additional BP and PR values at the last study visit. BP, blood pressure; PR, pulse rate.
BP measurement
BP was measured during outpatient clinical encounters in a routine clinical practice setting at baseline and at 6, 12 and 24 months, or at the last visit of discontinued study participants. BP was managed by treating physicians according to the guideline recommendations.17 Systolic and diastolic BP and pulse rate (PR) were recorded. In the present analysis, visit-to-visit BP variability was evaluated by SD and coefficient of variation (CV) of systolic BP. CV was defined as the within-subject SD×100 divided by the mean BP level.18–20 BP measurement≥3 times allowed us to evaluate visit-to-visit BP variability and to calculate SD and CV of systolic BP.21 22 Mean PR and SD and CV of PR were also assessed.
Study endpoint and statistical analysis
The primary endpoint of the present subanalysis was CV of systolic BP during the study period. SD of systolic BP and mean systolic BP during the study period, and at each timepoint, were also evaluated. As an exploratory analysis, mean PR and PR variability were investigated.
Statistical analysis was performed by an independent, professional biostatistician with R statistical software V.4.0.2 (R Foundation for Statistical Computing, Vienna, Austria) in a modified intention-to-treat manner.13 Data are expressed as median (IQR) or frequency (%). The distributions of baseline characteristics were evaluated with standardised mean difference. CV of systolic BP during the study period was calculated as abovementioned. Effect of febuxostat versus control in mean systolic BP and PR and SD and CV of systolic BP and PR were estimated using a linear regression model, adjusted with age, sex and a baseline systolic BP or PR value, and expressed with 95% CIs. A value of p<0.05 was considered statistically significant.
Results
Study participants
Between May 2014 and June 2016, a total of 514 patients were registered in the PRIZE Study and were randomised to either the febuxostat group (n=257) or the control group (n=257). Of the 514 patients, 472 (91.8%) were included into the present subanalysis (figure 1). Table 1 lists the baseline characteristics, which were balanced between the febuxostat and control groups. Overall, the median SUA level was 7.6 (7.1, 8.2) mg/dL at baseline, and a history of hypertension was found in 419 of 472 (88.8%) patients. At 24 months, febuxostat was prescribed at the median dose of 20 (10, 40) mg/day, and the median SUA levels were 4.6 (3.8, 5.5) and 7.4 (6.6, 8.0) mg/dL in the febuxostat and control groups. Trajectories of BP and PR at baseline and at 6, 12 and 24 months are shown in table 2. At each timepoint, the mode of use of antihypertensive medications was similar between the two groups (online supplemental table S1). During the study period, 103 of 472 (21.8%), 95 of 421 (22.6%), 102 of 403 (25.3%) and 81 of 376 (21.5%) patients had office systolic BP≥140 mm Hg at baseline and at 6, 12 and 24 months, respectively.
Supplemental material
Baseline characteristics
BP and PR parameters
BP and PR variability
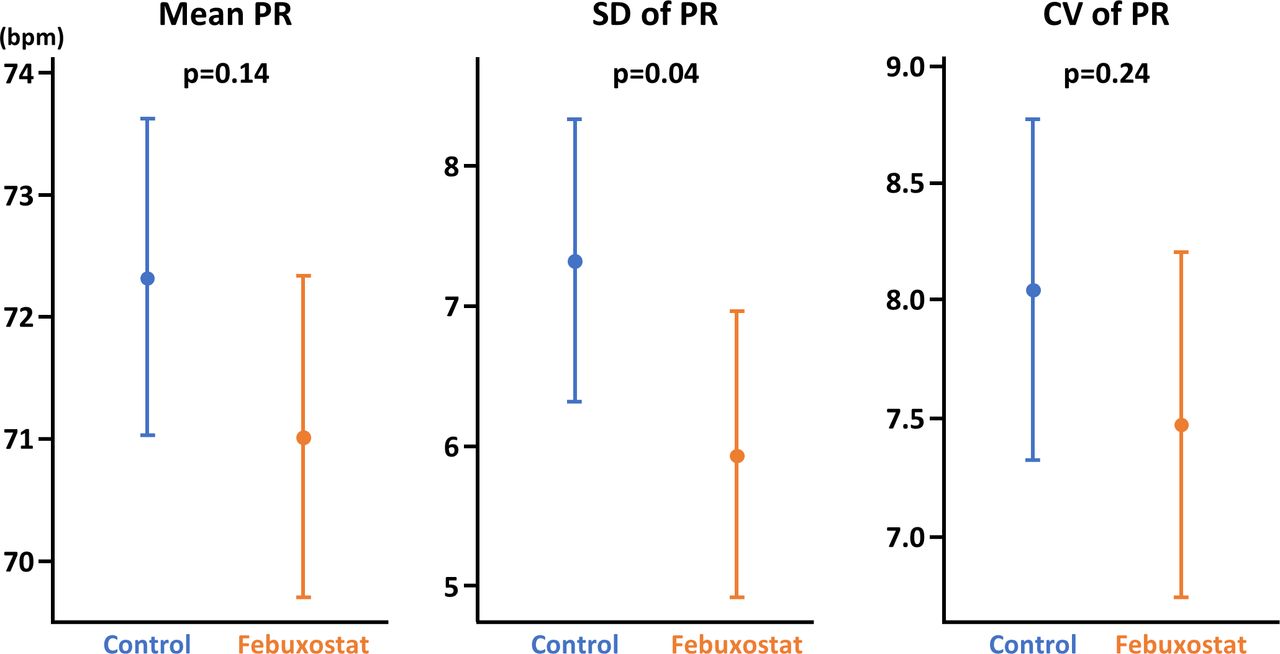
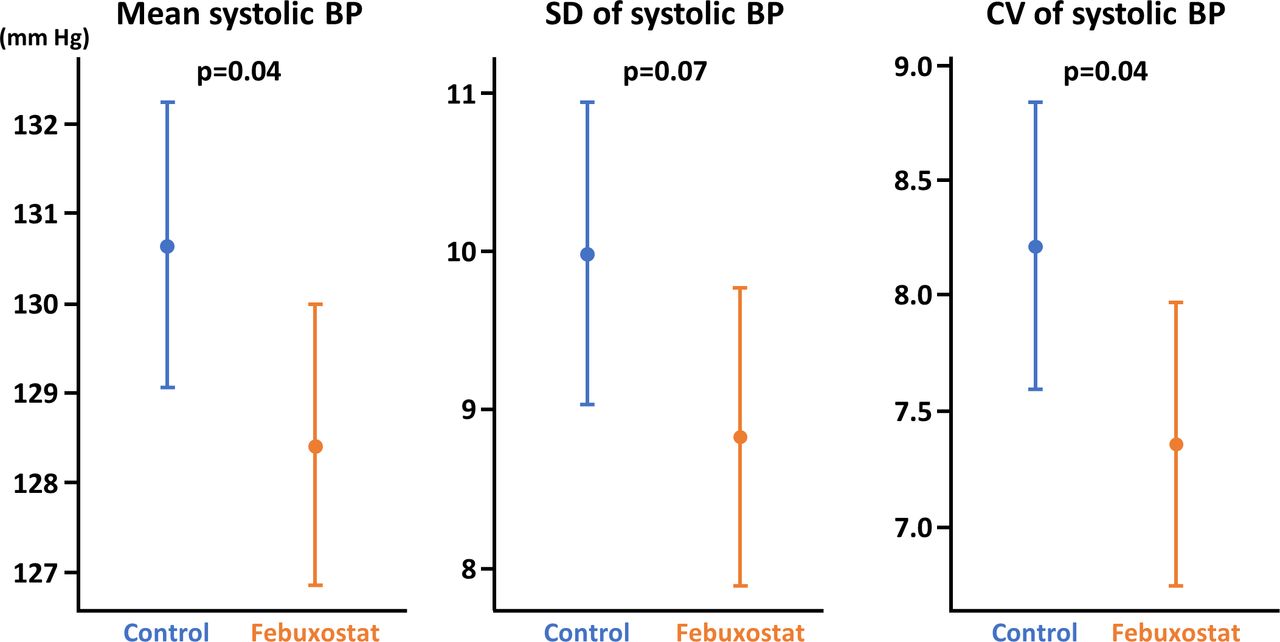
Of the 472 patients, 420 (89.0%) had systolic BP measurement≥3 times during the study period and were included to evaluate BP and PR variabilities (figure 1). Baseline characteristics remained well balanced between the two groups for the BP and PR variability assessment, with all standardised mean differences<0.10 (online supplemental table S2). During the 24-month follow-up period, the febuxostat group had a significantly lower adjusted mean systolic BP (128.4 (126.8–130.0) vs 130.7 (129.1–32.2) mm Hg, p=0.04) and CV of systolic BP (7.4 (6.7–8.0) vs 8.2 (7.6–8.8), p=0.04) than in the control group (figure 2 and table 3). SD of systolic BP also tended to be lower in the febuxostat group (8.8 (7.9–9.8) vs 10.0 (9.0–11.0), p=0.07) (figure 2). In terms of PR, the febuxostat group’s adjusted SD of PR was significantly lower than their counterpart (5.95 (4.93–6.97) vs 7.33 (6.32–8.33), p=0.04) (figure 3 and table 3). The febuxostat group had a numerically, but non-significantly, lower mean PR (71.0 (69.7–72.3) vs 72.3 (71.0–73.6) bpm, p=0.14) and CV of PR (9.1 (8.0–10.2) vs 10.0 (8.9–11.1), p=0.24) than in the control group (figure 3). Online supplemental figure S1 displays the associations of mean systolic BP and SD and CV of systolic BP with SUA levels achieved at 24 months in the febuxostat and control groups, showing no significant relations.

Mean systolic BP and SD and CV of systolic BP between the febuxostat and control groups. Variables are adjusted by age, sex and baseline systolic BP and are expressed with 95% CIs. BP, blood pressure; CV, coefficient of variation.
{kind=link}
{kind=link}
{kind=link}
Mean PR and SD and CV of PR between the febuxostat and control groups. Variables are adjusted with age, sex and baseline PR and are expressed with 95% CIs. CV, coefficient of variation; PR, pulse rate.
Effect on systolic BP and PR
Discussion
The present subanalysis of the randomised PRIZE Study demonstrated for the first time, to our knowledge, that XO inhibition with febuxostat was associated with reduced visit-to-visit BP variability in addition to the level of mean systolic BP. The febuxostat group also showed reduced office PR variability when compared with the control group. These findings illustrate the potential therapeutic effect of febuxostat in patients with hyperuricemia and carotid plaques.
It is well known that elevated BP and SUA levels are closely associated with each other.1 A longitudinal cohort study showed that among non-obese, normotensive males aged ≤50 years, at baseline, systolic BP increased during a 5-year follow-up period (from 123±8 to 130±7 mm Hg, p<0.05), and the increase in systolic BP was related to higher baseline BP and SUA levels.23 A meta-analysis of 25 observational studies (n=97 824) indicated that the risk of incident hypertension was increased by 13% for every 1 mg/dL increase in the SUA level.24 Thus, although controversial, an elevated SUA level may be causally associated with hypertension. An experimental study demonstrated that the administration of oxonic acid, an inhibitor of uricase, resulted in hyperuricemia and a subsequent increase in BP in a rat model.25 In this experimental study, elevated BP was reduced and counterbalanced by lowering uric acid with febuxostat.25 In humans, conflicting results of XO inhibition in lowering BP have been reported. In the single-centre, double-blind, placebo-control study, 60 prehypertensive obese adolescents were randomised to receive allopurinol, probenecid or a matching placebo. At 2 months, 24-hour systolic BP was significantly reduced in the allopurinol and probenecid groups.10 Even though a meta-analysis suggested the BP lowering effect of allopurinol,11 this therapeutic strategy has not been established because recent randomised control trials did not show such an effect on BP by lowering SUA levels in various groups of patients.1 In this context, patients treated with febuxostat had a lower mean office systolic BP during the follow-up period compared with their counterpart in the adjusted model in the present study. The magnitude of possible effect of febuxostat on lowering absolute systolic BP in this study (ie, −2.24 mm Hg) may be clinically relevant, because even a 2 mm Hg lower usual systolic BP would involve about 10% lower stroke mortality and about 7% lower mortality from ischaemic heart disease or other vascular causes as shown in a meta-analysis.26 Future studies are warranted to clarify the BP lowering effect of antihyperuricemic agents and to explore candidates to be treated.
Beyond the absolute BP level, BP variability has been recognised as a clinically relevant predictor of cardiovascular outcomes. Rothwell et al clearly demonstrated that visit-to-visit BP variability was strongly associated with increased risks of stroke and coronary events in patients with previous transient ischaemic attack.2 Multiple mechanisms link to BP variability, including atrial stiffness, endothelial function, sympathetic nerve activation and other intrinsic and social factors.3 An increased SUA level was also reportedly associated with greater visit-to-visit BP variability.27 It is known that the effect of antihypertensive agents on BP variability varies widely.7 8 Although a BP lowering effect of antihyperuricemic agents has been suggested as mentioned above, the effect on reducing BP variability remains uncertain. In the present study, febuxostat showed a significant reduction in visit-to-visit BP variability in patients who have hyperuricemia and carotid plaques. Our results may be robust because the primary endpoint of the BP variability metric (ie, CV of systolic BP) was adjusted on the randomised control setting. Given that the achieved uric acid concentration at 24 months was not significantly associated with reduction in absolute BP level and BP variability (online supplemental figure S1), the potential of febuxostat on reduced BP variability may be attributable to XO inhibiting effect rather than SUA lowering effect. Since the febuxostat groups showed lower PR variability than in the control group, sympathetic nerve activation may play a role in the underlying mechanism. The regulation of PR, a surrogate of heart rate (HR), depends on the influence of sympathetic activity as shown in several experimental studies, in which, for instance, HR was strongly correlated with cardiac norepinephrine spillover in unmedicated hypertensive patients, supporting the notion that HR is associated with the cardiac sympathetic drive.28 A previous cross-sectional study showed that elevated SUA levels were negatively correlated with time domain parameters of HR variability, largely reflecting parasympathetic cardiac modulation, and were positively correlated with low-frequency power of HR variability, indicating sympathetic activation.29 Given that a recent large-scale observational study (n=19 128) revealed that the prognostic impact of elevated SUA levels was enhanced especially when HR was elevated,30 the present study results may be relevant. In the proof-of-concept study by Rothwell et al, amlodipine treatment, rather than atenolol, was associated with reduced visit-to-visit BP variability with approximately −3.0 in SD and −1.8 in CV of systolic BP.2 Whether the effect of febuxostat in reducing BP variability observed in the present study (ie, −1.16 in SD and −0.9 in CV of systolic BP in the adjusted models) can be translated into significantly improving clinical outcomes deserves further investigations.
Limitations
The present study has several limitations. The PRIZE was a prospective, randomised control trial, but the present analysis was done in a post hoc manner. Hypertension treatment was done per local standard practice and BP medications were left to physicians’ discretion. Although the mode of use of antihypertensive medications was similar between the two study groups during the follow-up period (online supplemental table S1), data on the dosage and adverse events related to BP lowering were not available. BP measurement was defined in the study protocol but was not systematically audited. The open-label design might have affected the results. Despite being a randomised trial, the comparison of BP variability between the two groups was not completely randomised. However, the baseline characteristics were well balanced and multivariable analysis reinforced the primary outcome of this study. The number of BP measurement in the present study was relatively low, although previous studies demonstrated the feasibility of BP measurements≥3 times for investigating BP variability.21 22 Despite the multivariable adjustment, whether the potential BP variability lowering effect of febuxostat in this study was independent of absolute BP levels is uncertain, because mean systolic BP was reduced in the febuxostat group than in the control group. Additionally, the present study population was highly selected, with the SUA level>7.0 mg/dL and maximum carotid IMT≥1.1 mm at screening, and approximately 90% of participants were hypertensive patients. Thus, external generalisability may be considered.
Conclusion
The present subanalysis of the randomised PRIZE Study showed that febuxostat, an XO inhibitor, was associated with reduced visit-to-visit BP variability as well as reduced PR variability.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was conducted in compliance with the Declaration of Helsinki. The study protocol was approved by review boards and ethic committee at all participating sites (2013-10-02 and 2020-05-R01). Participants gave informed consent to participate in the study before taking part. Written informed consent for the PRIZE Study was obtained from all participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the study conception, design and operation. Funding acquisition for the study was carried out by KN, who was the principal investigator of the PRIZE trial. The data analyses and interpretation were performed by all authors. HY was responsible for the statistical analyses. The first draft of the manuscript was written by YS and all authors reviewed subsequent drafts of the manuscript. All authors read and approved the final manuscript. AT and KN accept full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The PRIZE Study was supported by Teijin Pharma Limited, Japan.
Competing interests AT has received honoraria from Boehringer Ingelheim and research funding from GlaxoSmithKline and Takeda. DU has received honoraria from Novo Nordisk Pharma, Eli Lilly Japan, Sanofi, Mitsubishi Tanabe Pharma, Sumitomo Pharma and Kissei Pharmaceutical. KN has received honoraria from Astellas, AstraZeneca, Bayer Yakuhin, Boehringer Ingelheim Japan, Daiichi Sankyo, Eli Lilly Japan, Kowa, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, MSD, Novartis Pharma, Novo Nordisk Pharma, Ono Pharmaceutical, Otsuka and Teijin Pharma; research grant from Asahi Kasei, Astellas, Mitsubishi Tanabe Pharma, Teijin Pharma, Boehringer Ingelheim Japan, Eli Lilly and Company, Novartis Pharma, Fuji Yakuhin and Mochida Pharmaceutical; and scholarship from Daiichi Sankyo Healthcare, Mitsubishi Tanabe Pharma, Teijin Pharma, Medtronic and Bayer Yakuhin.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.