Article Text

Abstract
Background Patients with morbid obesity may require both bariatric surgery and total knee/hip arthroplasty (TKA/THA). How to sequence these two procedures with better outcomes remains largely unstudied.
Methods This cohort study extracted claims data on patients with an obesity diagnosis that received both bariatric surgery and TKA/THA surgery within 5 years of each other (Premier Healthcare database 2006–2019). Overall, 1894 patients received bariatric surgery before TKA or THA, while 1000 patients underwent TKA or THA before bariatric surgery. Main outcomes and measures include major complications (acute renal failure, acute myocardial infarction, other cardiovascular complications, sepsis/septic shock, pulmonary complications, pulmonary embolism, pneumonia, and central nervous system-related adverse events), postoperative intensive care unit utilization, ventilator utilization, 30-day readmission, 90-day readmission, 180-day readmission and total hospital length of stay after the second surgery. Regression models measured the association between the complications and sequence of TKA/THA and bariatric surgery.
Results Undergoing TKA/THA before bariatric surgery (compared with the reverse) was associated with higher odds of major complications (7.0% vs 1.9%; adjusted OR 4.8, 95% CI 3.1, 7.6, p<0.001). Similar patterns were also observed for intensive care unit admission, ventilator use postoperatively, 30-day, and 90-day readmissions. Patients who received a second surgery within 6 months of their first surgery exhibited worse outcomes, especially among the TKA/THA first patient cohort. Major complication incidences occurred at 20.5%, 12.5%, 5.1%, 5.0%, 5.8% and 8.5% with time between TKA/THA and bariatric surgery at <6 months, 6 months–1 year, 1–2, 2–3, 3–4 and 4–5 years, respectively.
Conclusions Patients who require both bariatric surgery and TKA/THA should consider bariatric surgery before TKA/THA as it is associated with improved outcomes. Procedures should be staged beyond 6 months.
- outcomes
- outcome assessment
- health care
- treatment outcome
- postoperative complications
Data availability statement
Data may be obtained from a third party and are not publicly available. The data used in this study are commercially available from Premier Healthcare database (Premier Healthcare Solutions, Charlotte, North Carolina, USA).
Statistics from Altmetric.com
Introduction
Morbid obesity (body mass index >40 kg/m2) is increasingly common among surgical candidates for total knee/hip arthroplasty (TKA/THA).1 These patients carry a higher comorbidity burden and are at risk for worse surgical outcomes.2 Preoperative health optimization programs have been implemented to reduce overall postoperative complications which include preoperative weight loss with some patients with obesity referred to bariatric surgery (BS) before TKA/THA surgery.3 4 Coincidentally, this exact patient population—obesity requiring surgical intervention—is more likely to be indicated for joint arthroplasty to treat end-stage osteoarthritis. Unfortunately, the mobility associated with debilitating osteoarthritis may hinder the effectiveness of weight loss treatment programs, including BS.
Despite potential theoretical benefits, there are several studies indicating that BS before lower extremity joint arthroplasty might increase patients’ risk of perioperative complications5–7 although this finding is not universally seen across studies8 even those using the same dataset.9
Clinicians therefore continue to debate the rationale of which surgery to recommend first as it is unclear which hypothesized mechanism may lead to better outcomes. Indeed, TKA/THA before BS may result in less pain and more functional mobility for weight loss, while conversely, BS surgery related weight loss pre-TKA/THA might potentially decrease perioperative complications as well as improve functional outcomes of arthroplasty. Previous studies have primarily focused on outcomes after joint arthroplasty and lack important information on the final outcome as well as the overall healthcare burden for patients in need of both surgical interventions. In addition to the sequence of clinical practice, the best timing between these two surgical interventions remains unknown.
In this study, we aimed to answer the following questions: (1) Is performing BS before TKA/THA associated with better surgical outcomes than the opposite sequence, and (2) What is the optimal timing between the two surgical procedures?
Methods
This study followed Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines.
We conducted a retrospective cohort study from 2006 to 2019 using the Premier Healthcare database (Premier Healthcare Solutions, Charlotte, North Carolina, USA), a national claims database consisting of comprehensive hospitalization information. Patients who underwent both BS and primary TKA/THA surgery within 5 years, and who were diagnosed with obesity at the first surgery were selected. BS codes were identified based on International Classification of Diseases, 9th Revision (ICD-9) and 10th Revision (ICD-10) procedure codes, Current Procedural Terminology codes (online supplemental appendix 1).10 TKA was defined based on ICD-9 procedure code 81.54 or ICD-10 procedure codes 0SRC0XX, 0SRD0XX. THA was defined based on ICD-9 procedures codes 81.51 or ICD-10 procedure codes 0SR90xx, 0SRB0xx. Obesity was defined using ICD-9 diagnosis code 278.0x, V85.3, V85.4 or ICD-10 diagnosis code E66, Z68.3, Z68.4. There were 4783 patients who received both BS and TKA/THA surgery. Exclusion criteria were: no obesity diagnosis at first surgery (N=1446), outpatient TKA/THA surgery (n=6), non-elective surgery (n=139), missing race (n=5), duplicated cases (n=122), cancer as indication for BS (n=3), bilateral arthroplasty (n=158), or two arthroplasty procedures during the study period (n=10); see figure 1 for a study flow chart.
Supplemental material
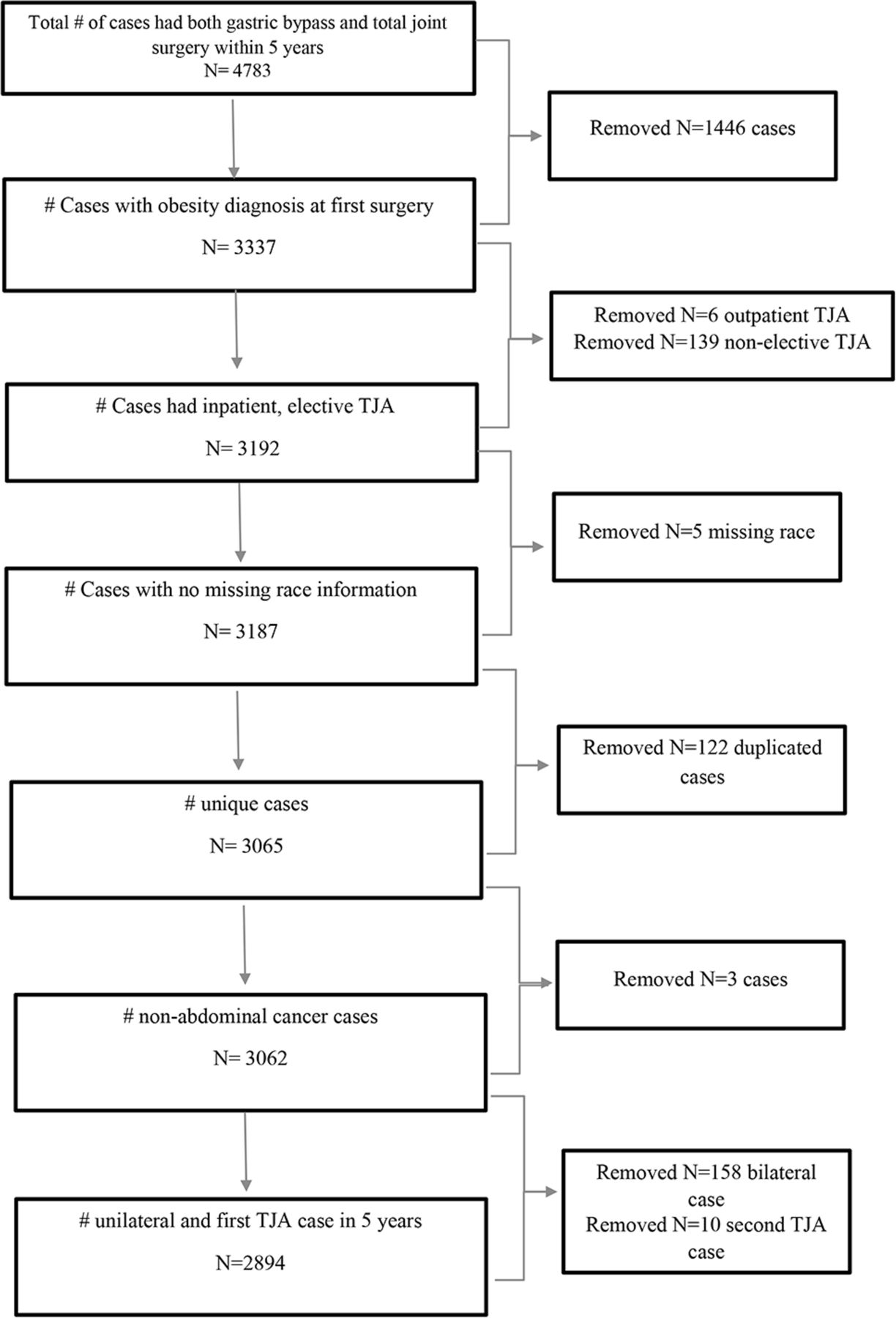
Strengthening the Reporting of Observational Studies in Epidemiology diagram of patient selection.
Study variables
The primary outcome measure was any major complication during the hospitalization after the second surgery, which could be either BS or TKA/THA. These included acute renal failure, acute myocardial infarction, other cardiovascular complications, sepsis/septic shock, pulmonary complications, pulmonary embolism, pneumonia, and central nervous system related adverse events. All complications were defined based on ICD-9 and ICD-10 diagnosis codes during the hospitalization (online supplemental appendix 2) as previously published.11 Secondary outcomes include any post-operative intensive care unit (ICU) utilization, any ventilator utilization, total hospital length of stay (LOS), any 30-day readmission, any 90-day readmission, and any 180-day readmission after the second surgery, either BS or TKA/THA.
Demographic variables included age, gender, race (black, white, or other), insurance provider (commercial, Medicaid, Medicare, uninsured, unknown), Charlson-Deyo comorbidity index12 at the first surgery (either BS or TKA/THA; categorized as 0, 1, 2, 3+), a diagnosis of obesity at the time of the second surgery, region (Midwest, Northeast, South, West), and time between 2 surgeries (categorized as <6 months, 6 months–1 year, 1–2, 2–3, 3–4, and 4–5 years).
Statistical analysis
All statistical analyses were performed using SAS V.9.4 (SAS Institute). TKA and THA were analyzed as one group. Descriptive analyses were stratified by the sequence of the surgeries (BS first or TKA/THA first). Categorical variables were reported as absolute numbers and frequencies, and analyzed using χ2 tests while continuous variables were reported as median and IQR, and analyzed using Wilcoxon-rank sum tests.
For the primary outcome, multivariable logistic regression models were run to determine if the order of BS and TKA/THA surgeries was a significant predictor of major complications after the second surgery on adjusting for all covariates. Covariates in our model were based on biological plausibility and included age, gender, Charlson-Deyo comorbidity index at first surgery, type of surgery (TKA/THA), year of the second surgery, and time between two surgeries. ORs and 95% CIs were reported. All p values reported were from two-tailed tests. A p value of <0.05 was determined significant. The same multivariable logistic regression models were applied for binary secondary outcomes (ICU admission, ventilator use, 30-day, 90-day, and 180-day readmission). For LOS, we utilized generalized linear models with a Poisson distribution and log-link controlling for the same covariates. Percent change and CIs were reported. Sensitivity analyses were performed using the same statistical models to evaluate composite any major complication after both BS and TKA/THA surgeries, not just after the second surgery only (as in the main analysis); see online supplemental table 1).
Results
Overall, 1894 patients received BS before TKA/THA, and 1000 patients underwent TKA/THA before BS. The majority of patients who received both BS and TKA/THA within 5 years were female (76.7% and 77.5%), white (75.7% and 76.9%), commercially insured (52.8% and 57.4%), and underwent surgery in a hospital located in the South (41.3% and 42.7%) (table 1). TKA/THA patients, who received BS first, presented with lower comorbidity burden at the second surgery compared with their comorbidity burden at the first surgery; interestingly, the comorbidity burden for those who underwent TKA/THA first increased over the time between the two surgeries (table 1).
Patient characteristics of the bariatric surgery (BS) and total knee/hip arthroplasty (TKA/THA) cohort
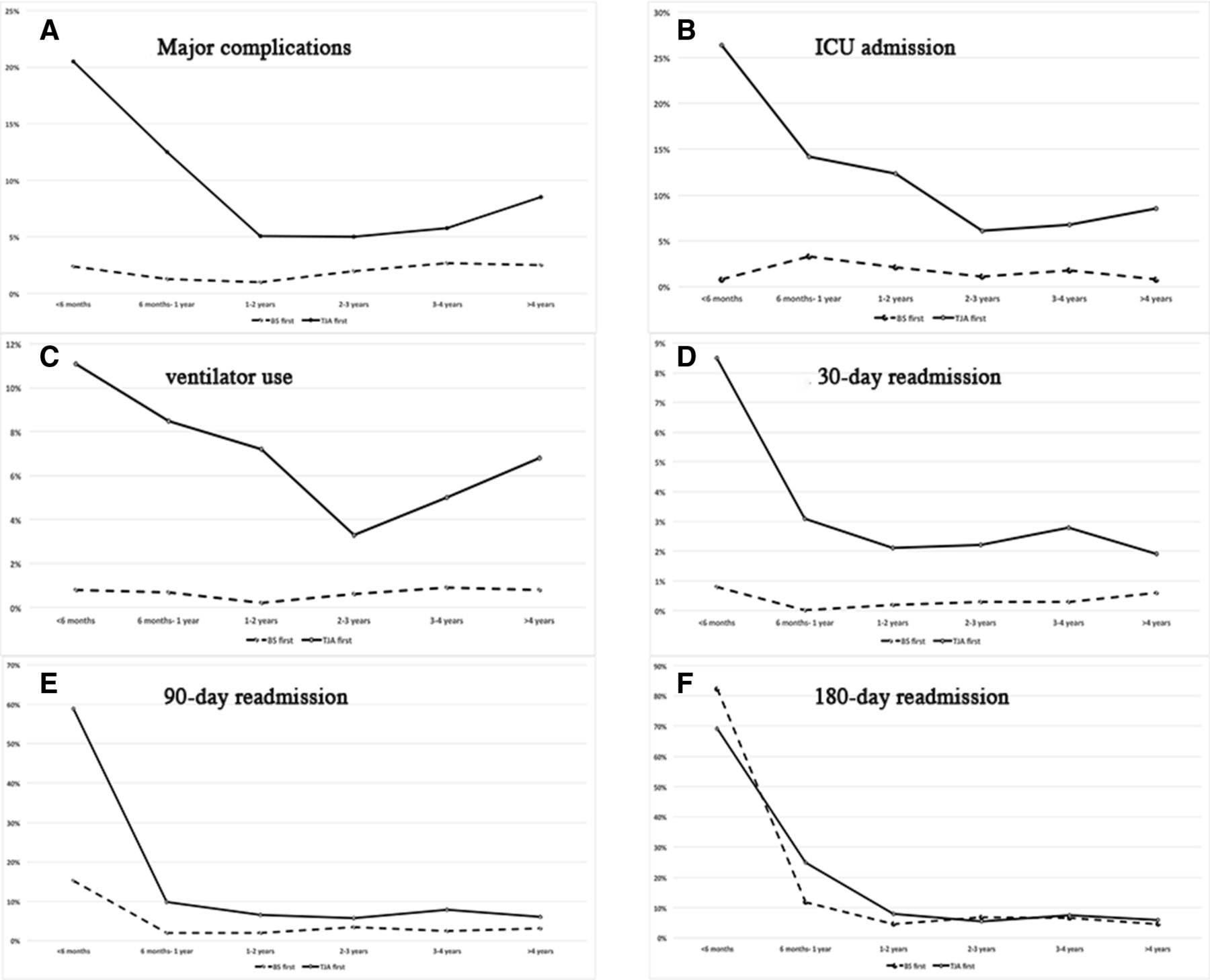
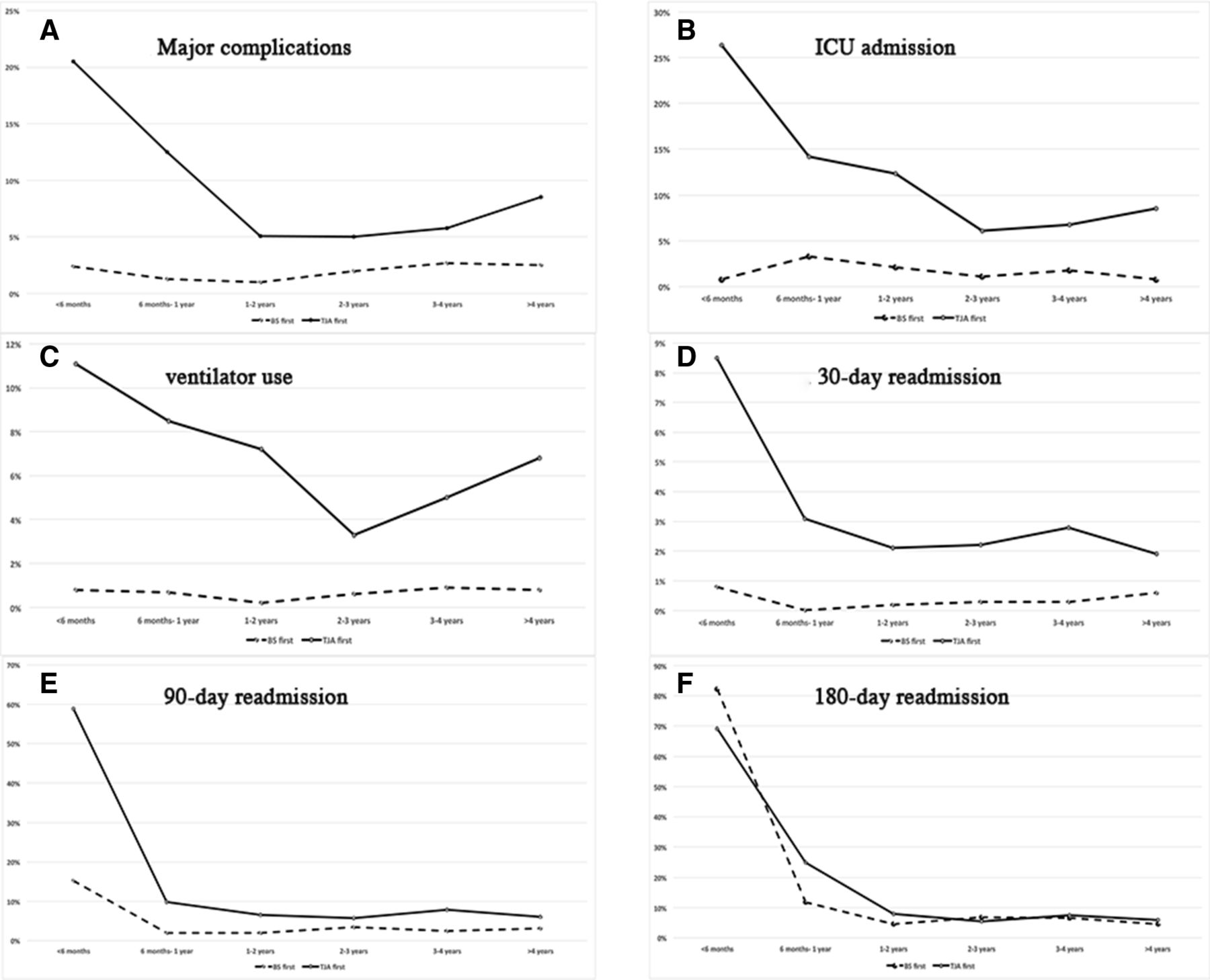
After adjustment for relevant covariates, those who underwent TKA/THA first (compared with those undergoing BS first) had higher odds of major complications (7.0% vs 1.9%; adjusted OR 4.8, 95% CI 3.1, 7.6, p<0.001) (table 2). Among those who underwent TKA/THA ahead of BS, we found the highest complication incidence when BS was performed within 6 months after TKA/THA (20.5%) (figure 2).
Summary of outcomes after the second surgery
{kind=link}
{kind=link}
Outcome measurements after second surgery of either bariatric surgery (BS) or total knee/hip arthroplasty (TKA/THA) by time between surgeries. (A) major complications; (B) ICU admissions; (C) ventilator use; (D) 30-day readmission; (E) 90-day readmission; (F) 180-day readmission.
As for secondary outcomes, the group undergoing TKA/THA first had higher odds of ICU admission (7.7% vs 1.7%; adjusted OR 6.8, 95% CI 4.3 to 10.7), ventilator use postoperatively (5.1% vs 0.6%; adjusted OR 13.1, 95% CI 6.7 to 25.6), 30-day readmission (2.1% vs 0.3%; adjusted OR 6.9, 95% CI 2.6 to 18.2), and 90-day readmission (5.5% vs 3.4%; adjusted OR 2.2, 95% CI 1.5 to 3.4). The outcomes of patients who had BS first were ubiquitously better than those that received TKA/THA first (figure 2). For patients who had TKA/THA first, the worst outcomes were usually seen when two surgeries were performed within 6 months of each other (including ICU admissions, ventilator use, 30-day, and 90-day readmission) (figure 2).
Our sensitivity analyses looking into composite major complications and other outcomes after both BS and TKA/THA surgeries (not just after the second surgery only, as in the main analysis), demonstrated the same pattern as our main analysis (online supplemental table 1): worse outcomes for patients undergoing TKA/THA first.
Discussion
We conducted a retrospective cohort study with the goal to address the question on how to manage and stage morbidly obese patients in need of both BS and TKA/THA. Our study indicated that the practice of BS before joint arthroplasty of either the knee or the hip was associated with better outcomes. Further, our results suggest that these procedures should be staged at least 6 months apart.
A number of studies have reported improved TKA/THA outcomes among those who first received BS, while several other studies have concluded that BS before TKA actually might be associated with increased risk of complications. However, most of these studies include small sample sizes, and the results should be interpreted cautiously. A meta-analysis conducted by Smith et al concluded that BS prior to THA or TKA does not significantly reduce most perioperative complications.13 Another meta-analysis by Li et al, synthesizing data from nine studies, concluded that BS before TKA/THA was associated with reduced LOS, operative time, and short-term periprosthetic infection risk, while no long-term benefit was found.14 A third meta-analysis by Gu et al, including 13 studies, could not reach consensus on the effect of BS before TKA/THA on both short-term and long-term complications.1 In addition, a recent Swedish registry data analysis of 441 patients showed a higher infection-related revision risk among those that first received BS (HR 2.2, 95% CI 1.1 to 4.7).15
As evidence indicates that BS before TKA/THA may not be effective in reducing perioperative complications, the question arises if patients in need of both BS and TKA/THA should undergo BS first. Kulkarni et al studied the National Health Service database of the UK between 2005 and 2009, with 53 patients receiving BS first and 90 patients undergoing arthroplasty first.16 The authors observed that complications after joint arthroplasty appear to be lower in the BS first cohort. Moreover, Nearing et al conducted a similar retrospective cohort study on 102 patients to evaluate the outcomes after TKA/THA, and concluded that both early complications and late reinterventions were similar, except in operative time and LOS.17
It is noteworthy that all these studies focused on complications after TKA/THA, and did not include the associated risks and outcomes of BS which can be substantial in this high-risk patient group. To better serve this morbidly obese patient population, it is best to understand the incidence of major complications from both BS and TKA/THA surgeries relevant to the sequential orders of and staging intervals associated with the surgeries, and more importantly the final outcomes after the second surgery, an evidence gap that is addressed by the current study.
Our study included 1894 patients who underwent BS before TKA/THA, and 1000 with the opposite approach. Those receiving TKA/THA before BS had higher odds of composite complications, ICU admission, and readmission across all time groups. Our analysis clearly indicated that receiving a second surgery within 6 months of the first surgery was associated with worse outcomes irrespective of the sequential orders of the surgeries, while more obvious and significant in the TKA/THA first cohort. Our retrospective study could not identify the etiology of this observation. However, the period of catabolic weight loss and malnutrition immediate after BS may inadvertently increase postoperative complication risk after another surgery. Future studies are indicated, especially prospective studies that are not burdened by potential confounders that may influence both decision-making on which surgery to perform first and the timing between surgeries.
Few studies have incorporated timing in their analysis. For example, Severson et al compared staging interval of <2 years to one of >2 years in a total of 125 patients. Their analysis did not show a difference in 90-day complication rates.18 In addition, Schwarzkopf et al studied the HCUP California state inpatient database and identified 330 BS-THA and 1017 BS-TKA cases.19 Their analysis indicated that THA surgery more than 6 months after BS was associated with less 90-day readmission, while no association on 90-day complications were observed. While studies on the optimal timing between BS and THA/TKA surgery are complicated by the small sample sizes available, continued monitoring is required in order to define more exact thresholds. Such information may greatly benefit not only surgeons and policymakers, but also patients.
Our study has limitations. First, this is a retrospective cohort study without prior knowledge of the decision-making process in regards to the exact practice pattern or type of BS chosen, that is, gastric bypass surgery versus gastric sleeve surgery. We were also unable to determine the aetiology of our observation. Third, the patient cohorts undergoing different surgical sequences of surgical treatment may differ. Patients may drop out during the process for various reasons and decisions for one or the other surgery may be unrelated. For example, some patients might receive BS with a plan for TKA/THA later. However, symptoms might improve after BS and therefore surgery for TKA/THA may become unnecessary. Similarly, some patients who receive TKA/THA first, after which they might be able to increase activity and achieve weight loss. This may negate the need for BS. Nonetheless, our study is the first to investigate the total risk burden for patients with morbid obesity who underwent both BS and TKA/THA. Our study has a clear and consistent message, which should be valuable for patients and clinicians when making educated decision for value-based practice.
Conclusion
Patients who require both BS and TKA/THA should consider BS before TKA/THA for better outcomes. Patients should be staged beyond 6 months for the second surgery.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data used in this study are commercially available from Premier Healthcare database (Premier Healthcare Solutions, Charlotte, North Carolina, USA).
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the institutional review board (Hospital for Special Surgery IRB #2012-050). The requirement for written informed consent was waived given the deidentified nature of the data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jbLiujb, @jashvant_p, @sgmemtsoudis
Contributors JL, JP, and SGM: conception, study design, analysis and interpretation of data, and drafting manuscript. HZ: data analysis and drafting manuscript. PKS and DHK: conception, interpretation of data, and drafting manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.