Article Text

Abstract
Background In high-income and low-income countries, including Ethiopia, hypertension (HTN) is a serious public health concern. As a consequence, a massive self-care practice (SCP) is necessary, and the domains of SCP, including adherence to medication, physical activity, weight management, low-salt diet, non-smoking, moderate alcohol usage, and dietary management, are required. However, there is no nationwide study on HTN SCPs in Ethiopia. This meta-analysis, therefore, aimed to estimate the pooled level of HCP among individuals living with HTN in Ethiopia.
Methods The Preferred Reporting Items for Systematic Reviews and Meta-Analysis guideline was used to report this systematic review and meta-analysis. We systematically searched the databases PubMed/MEDLINE, Embase, Google Scholar and Science Direct for studies conducted in Ethiopia. All observational studies published until July 2020 were included. Data were analysed using R V.3.5.3 software, and the pooled prevalence with 95% CIs was presented using tables and forest plots. The presence of statistical heterogeneity (I2) within the included studies was evaluated. We used a funnel plot to identify evidence of publication bias. The random-effects meta-analysis model was employed to estimate the pooled proportion of good HTN SCPs.
This was submitted for registration with the International Prospective Register of Systematic Reviews in March 2020 and accepted with the registration number CRD42020175743 (https://www.crd.york.ac.uk/PROSPERO).
Results Our search databases produced 356 papers. Twelve of these papers fulfilled the inclusion and were found suitable for the review. The total population in this study was 3938. Off these hypertensive populations, 44% (95% CI 34 to 53) had good SCP. The subgroup analysis for each component of SCP was done. The subgroup analysis of good adherence to low-salt diet, alcohol abstinence, medication adherence, non-smoking, physical exercise and weight management was 52% (95% CI 39% to 66%), 77% (95% CI 69% to 88%), 65% (95% CI 45% to 85%), 92% (95% CI 88% to 95%), 43% (95% CI 30% to 56%) and 51% (95% CI 32% to 69%), respectively. In conclusion, nearly half of patients with HTN had good SCPs.
- hypertension
- hypertensive heart disease
- antihypertensive drugs
Data availability statement
Data are available upon reasonable request. NA.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
To the best of our knowledge, this is the first and only systematic review and meta-analysis that has focused on self-care practice (SCP) among hypertensive patients in Ethiopia, which is important for Ethiopian policymakers.
What does this study add?
Nearly half of the patients with hypertension (HTN) had good SCPs.
Strong and reliable methodological and statistical procedures were used in this review and meta-analysis.
How might this impact on clinical practice?
Our findings from the meta-analysis have implications in clinical practice as these can contribute to giving attention to the prevention and care of patients with HTN.
Background
Hypertension (HTN) is a growing problem that affects about a billion people worldwide, including two-thirds from low-income countries.1 Alarmingly, 1.56 billion adults are estimated to have HTN in 2025.1 2 HTN is the leading cardiovascular disease (CVD) risk factor for stroke, myocardial infarction, congested heart failure, impairment and death.1 3 4 HTN is one of the main risk factors for CVDs causing 45% of global cardiovascular morbidity and mortality.1 This condition remains asymptomatic in most cases until it is followed by stroke, myocardial infarction, renal dysfunction, visual problems and others.1 5
According to the WHO fact sheet, in 2015, one in four men and one in five women had HTN. Of those, less than one in five people with HTN have the problem under control.1 One of the global targets for non-communicable disease is to reduce the prevalence of HTN by 25% by 2025.1 The prevalence of HTN varies across the WHO regions and country income groups. The WHO African region has the highest prevalence of HTN (27%), while the WHO region of the Americas has the lowest prevalence of HTN (18%).1 A review of current trends shows that the number of adults with HTN increased from 594 million in 1975 to 1.13 billion in 2015, with the increase seen largely in low-income and middle-income countries.1 This increase is due mainly to a rise in HTN risk factors in those populations.1 Uncontrolled hypertension (UHTN) is the most common risk for cardiovascular morbidity and mortality, as well as target organ damage.6 7 UHTN is a major public health problem among patients with HTN both in high-income and in low-income countries.8 9 According to different studies, UHTN is a common health public problem in Ethiopia.9–13 To control high blood pressure and to improve high blood pressure status, it is important to apply self-care practices (SCPs).14 The main domains of SCP are adherence to medication, physical activity, weight management, low-salt diet, non-smoking, moderate alcohol usage, and dietary management. Excessive alcohol intake, cigarette smoking, increasing weight are the significant components of SCP that increase high blood pressure, whereas exercise, diets rich in fruits and vegetables, adherence to medication and reduced saturated fat can lower both the risk of high blood pressure and assist with blood pressure control.15–21 This study gives highlights on the crucial and urgent need to focus on the SCP in Ethiopia to better understand the condition and to address specific action plans which will surely result in mitigating the morbidity and mortality due to HTN and its related complications throughout the country.
The results of this study also will assist the ministry of health and clinical, facility managers, and governmental and non-governmental organisations in being aware of SCP and will have its contribution in taking action based on the research results. Besides, this study could be used as a baseline for future researchers and other concerned bodies. Therefore, this study tries to assess the pooled estimation of SCP among patients with HTN in Ethiopia.
Methods
Search strategy and information sources
Data source and search strategies in published and unpublished research articles that were conducted to assess a minimum variety of hypertensive self-care (overall hypertensive self-care, medication adherence, physical activity, weight management, low-salt diet, non-smoking, moderate alcohol usage and adherence to dietary management) in Ethiopia were included during this study.21 An extensive search was done from PubMed/MEDLINE and Embase online databases to access articles done on hypertensive SCPs. Moreover, Google Scholar and ScienceDirect were used to retrieve articles. Besides, reference lists of screened studies were checked. The two authors (DBT and HG) administered the search independently. The term ‘hypertension’ was searched with all of the subsequent terms as a mix of free text and thesaurus terms in numerous variations: hypertensive self-care, medication adherence, physical activity, weight management, low-salt diet, non-smoking, moderate alcohol usage and adherence to dietary management and Ethiopia.21 Moreover, the subsequent keywords were used to retrieve studies from the PubMed database: (Hypertensive self-care) OR hypertensive dietary care) OR physical activity) OR adherence to dietary management) AND Ethiopia. Studies that were relevant by title and abstract were assessed by full text to see those that provided adequate data to be included in our meta-analysis.
Data extraction, selection and process
Data were extracted using a preconceived and standardised data collection format and the data extraction was performed by two blind and independent reviewers. The two reviewers (DBT and HG) screened the titles, abstracts and the full-text search results to identify potentially eligible studies. Where necessary, authors were contacted for additional information to confirm eligibility of studies. Disagreements were resolved by discussion. Where there is missing information, the corresponding author of the study was contacted to request the missing information. A maximum of three emails were sent to the corresponding author of the retrieved studies to request for additional information before excluding the study. For studies appearing in more than one published article, we considered the most recent, comprehensive and with the largest sample size (SS). For surveys appearing in one article with multiple surveys conducted at different time points, we treated each survey as a separate study.
The data extraction format was composed of information about the year of publication, country, objective and design of the study, measuring criteria of SCP.
Eligibility criteria
Inclusion criteria
Study setting: studies were done in Ethiopia.
Study participants: studies were conducted among all hypertensive patients.
Publication status: all published and unpublished articles were included.
Language: all studies were included without language restriction.
Types of studies: studies that employed observational study design were included.
Publication date: the authors included articles published until July 2020.
Exclusion criteria
Despite the aforementioned preset eligibility criteria, articles in which we were unable to access the full texts after two email contacts of the principal investigator of the particular study were excluded from the final analysis. Studies that lack relevant data needed to compute the prevalence of SCP were excluded
Quality assessment of included studies
The methodological quality of the included studies was evaluated using the Newcastle-Ottawa Scale (NOS). The NOS is designed to assess the quality of non-randomised studies in meta-analyses. This scale is primarily formulated by a star allocation system, assigning a maximum of 10 stars for the risk of bias in three areas: a selection of study groups (4 or 5 stars), comparability of groups (2 stars) and ascertainment of the outcome of interest or the exposure (3 stars). No validation study provides a cut-off score for rating low-quality studies. We arbitrarily established 0–3, 4–6 and 7–10 stars be considered at high, moderate and low risk of bias, respectively.22
Outcome measures
The primary outcome is a SCP among hypertensive patients in Ethiopia. SCP was assessed using Hypertension Self-Care Activity Level Effects (H-SCALE), which includes medication adherence, dietary management, smoking status, physical activity, weight management and alcohol intake. H-SCALE has provided a detailed description of the scoring method of each component.23
Good SCP
This included adherence to all the components of the H-SCALE.
Poor SCP
This included non-adherence to at least one component of the H-SCALE.
Medication adherence
Three items assessed the number of days in the last week that an individual takes medication, at the recommended dosage, and at the same time. Responses were summed (range 0–21). Score=21 was considered adherent.
Low-salt diet: six items assessed practices related to eating a healthy diet. A mean score is calculated. Scores of 6 or better were considered adherent.
Exercise-related adherence
This included respondents who reported having exercised for 30 min/day, at least three times per week.
Weight management
Seven items, strongly disagree (1) to strongly agree (5), assessed weight management. Responses were summed, creating a range of scores from 7 to 35. Scores of ≥28 were considered adherent to weight management practices.
Smoking-related adherence
This included respondents who reported having never smoked or stopped smoking.
Alcohol consumption-related adherence
Respondents who reported having never consumed alcohol.
Data analysis and presentation of results
Data were analysed using the R V.3.5.3 and Rstudio V.1.2.5003 software. Forest plots were drawn to visualise the combined SCP and the extent of statistical heterogeneity between studies. Statistical heterogeneity was assessed using a standard χ2 test (Cochran Q test) and was quantified by calculating the I2 statistic (with values of 25%, 50% and 75% assumed to be representative of the low, medium and high heterogeneities, respectively). There was clinical heterogeneity between the included studies in this study. Consequently, we used a random-effects meta-analysis to estimate the overall pooled SCP. To visualise possible publication bias, a funnel plot was used.
Data management
Based on the inclusion and exclusion criteria, a tool has been developed to guide the screening and selection process. The tool was piloted and revised before data extraction began. The search results were first uploaded to EndNote software to remove duplicates.
Data items
Data on general information, authors, year, country, and region, type of publication, study characteristics (study design, setting, SS, response rate, mean or median age, or age range), data on measuring of SCP and information on the use of anti-hypertensive medication/therapy were extracted. When relevant information for estimating SCP is not available, we contacted the corresponding author of the study to provide us the missed information.
Risk of bias in individual studies
Methodological quality and risk of bias assessments were performed by two reviewers (DBT and HG) blindly and independently. The blinding was maintained by using the Covidence software that allows/obligates each reviewer to work without knowing of the other reviewer’s choice. This diminishes errors and the risk of bias in the selection of the studies. Disagreements were solved by discussion and where necessary by arbitration involving a third author. For each included study, we estimated the precision (C) or margin of error, considering the SS and the observed prevalence (p) of SCP using the formula
SS=  ,
,
where Z was the z value fixed at 1.96 across studies (corresponding to 95% CI). The desirable margin of error is 5% (0.05) or lower.
Data synthesis
A meta-analysis was performed to estimate the pooled prevalence of SCP. Results were presented using forest plots. A subgroup analysis was summarised by geographical regions where the studies were conducted. Random-effects meta-analysis was performed24 to determine the pooled estimate of the prevalence of SCP in Ethiopia. Heterogeneity was explored using Cochrane’s Q and quantified by I2 statistics.25 Results were reported as proportions with corresponding 95% CIs. This review is registered in the International Prospective Register of Systematic Reviews (CRD42020175743, https://www.crd.york.ac.uk/PROSPERO), and the results of this review were reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.26
Results
Screening flow
Figure 1 is a flow diagram outlining the process of identification and selection of included studies. We identified 356 records through a comprehensive search among which 178 duplicates were identified and removed. Subsequently, we screened 119 titles and abstracts and excluded 18 irrelevant papers. Only 12 studies met the inclusion criteria and were thus retained for qualitative and quantitative analyses (figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram which shows the study selection of the meta-analysis on levels of hypertension self-care practice in Ethiopia, 2020.
Study characteristic
All included studies were observationally conducted from 2000 to 2020 in different regions, but we found published articles from 2016 to 2020. Twelve studies were included with a total of the sample of 3938. Three articles from Adiss Ababa administrative city, three articles from Oromia region, two articles from Amhara region, two articles from Tigray region, one article from Harar region and one article from South Nation Nationalities and Peoples region had a total SS of 1158, 885, 693, 596, 401 and 205, respectively (table 1).
Study characteristics of included articles for the final systematic review and meta-analysis on hypertension self-care among hypertensive patients in Ethiopia
All included studies were from referral and general hospitals. Based on the NOS quality assessment method, the included studies were greater than seven. The potential risk factors from each study were being female, being a rural resident, educational level, social support, disease duration, blood pressure status, knowledge, comorbidity, age, khat chewing, monthly income, widowed marital status, distance from health institution, having no regular follow-up visit and being employee (table 2).
Study characteristics of included articles for the final systematic review and meta-analysis on HTN self-care among hypertensive patients in Ethiopia
Adherence to SCP among hypertensive patients
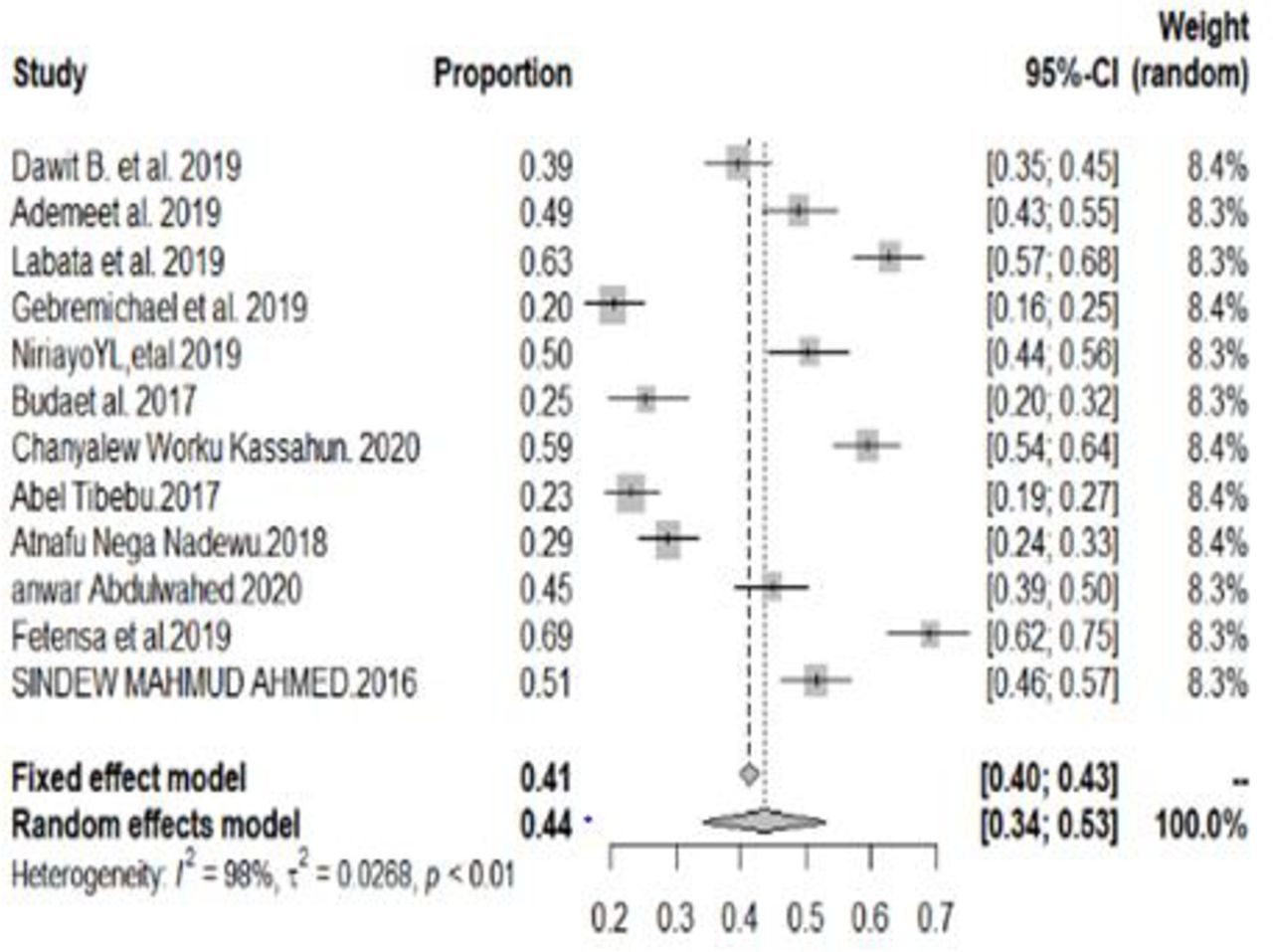
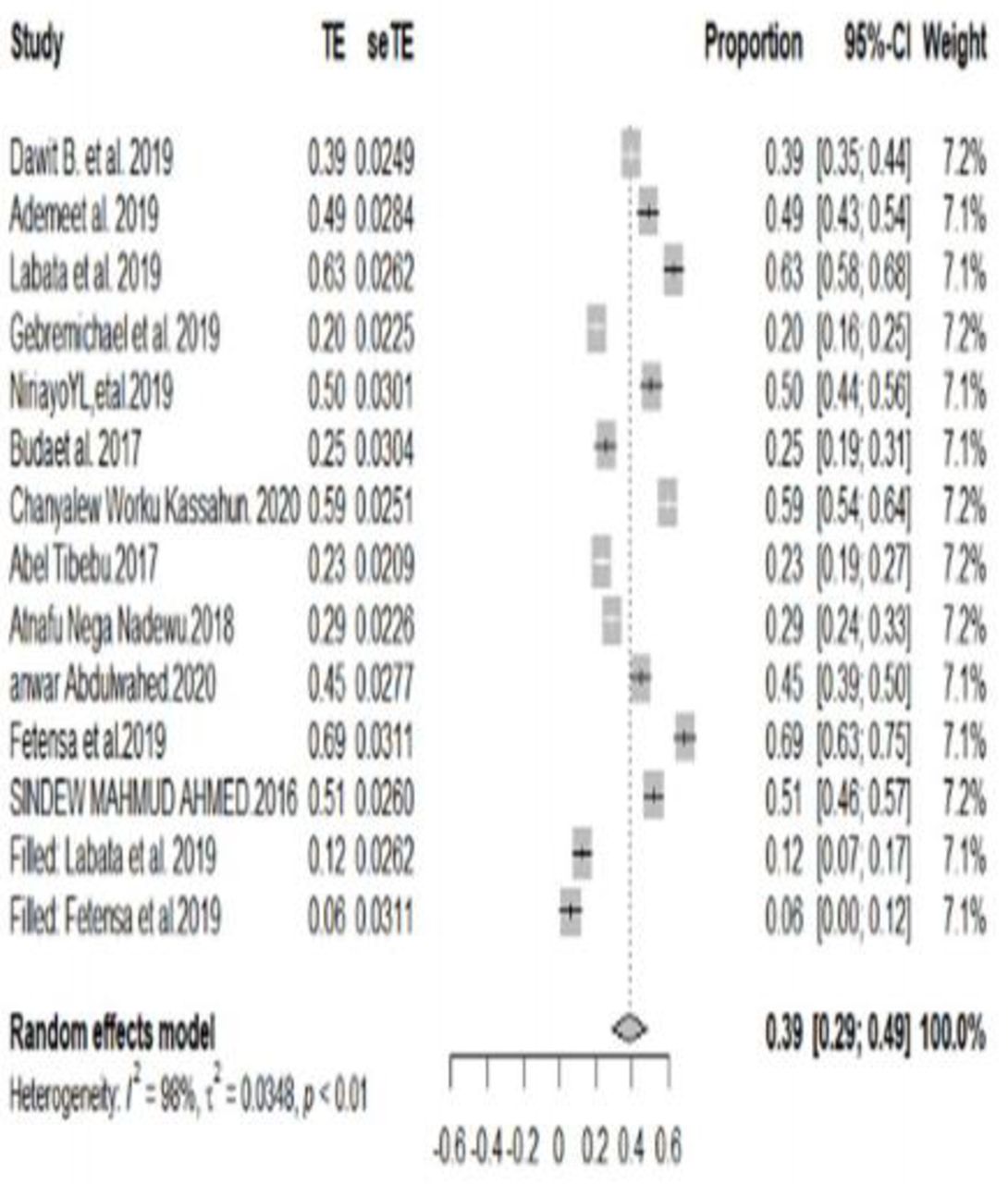
The overall good adherence to SCP among patients with HTN in Ethiopia was 44% (95% CI 34% to 53%). The heterogeneity test showed I2 was 98%, indicating that there was heterogeneity. The prevalence of good adherence to SCP varied widely in each study (figure 2).

Meta-analysis (forest plot) of the pooled prevalence of overall good self-care practice among hypertensive patients in Ethiopia, 2020.
A funnel test was used to test for publication bias, and it showed the presence of publication bias. Therefore, there are unpublished data that can modify the prevalence of good adherence to SCP (figure 3).

Funnel plot showing evidence of publication bias across studies.
Sensitivity analysis
In sensitivity analyses using the forest plot by precision (trim-and-fill) approach, none of the studies had a significant effect on the pooled prevalence estimates and measures of heterogeneity within primary studies. Therefore, sensitivity analyses using the random-effects model revealed that no single study influenced the overall prevalence of SCP among hypertensive patients (figure 4).
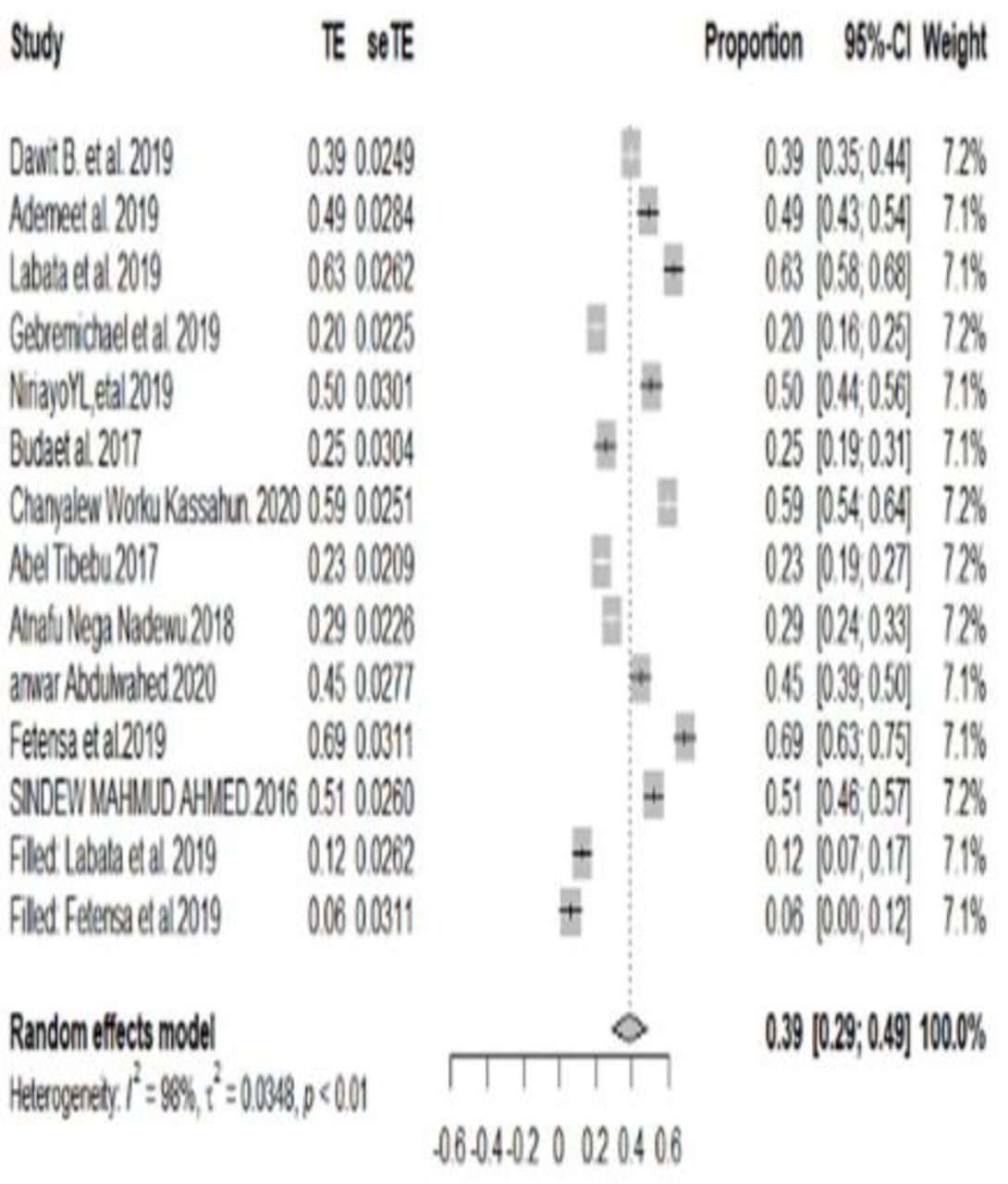
Result of sensitivity analysis of the studies.
Subgroup analysis of SCP by the components of SCP
Medication adherence
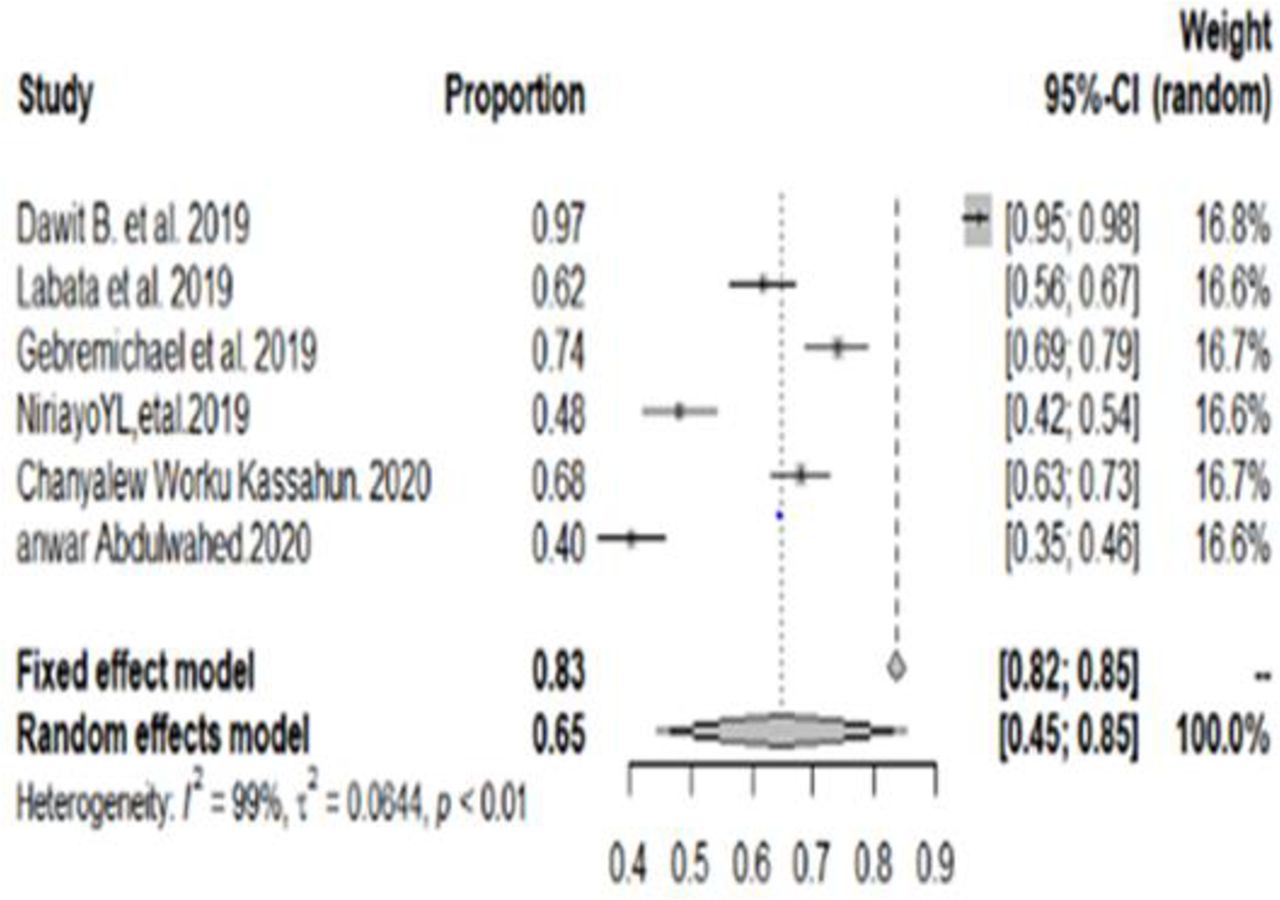
Based on the subgroup analysis, good medication adherence among patients with HTN was 65% (with 95% CI 45% to 85%) (figure 5).

Forest plot for subgroup analysis of medication adherence among hypertensive patients in Ethiopia, 2020.
Adherence to weight management
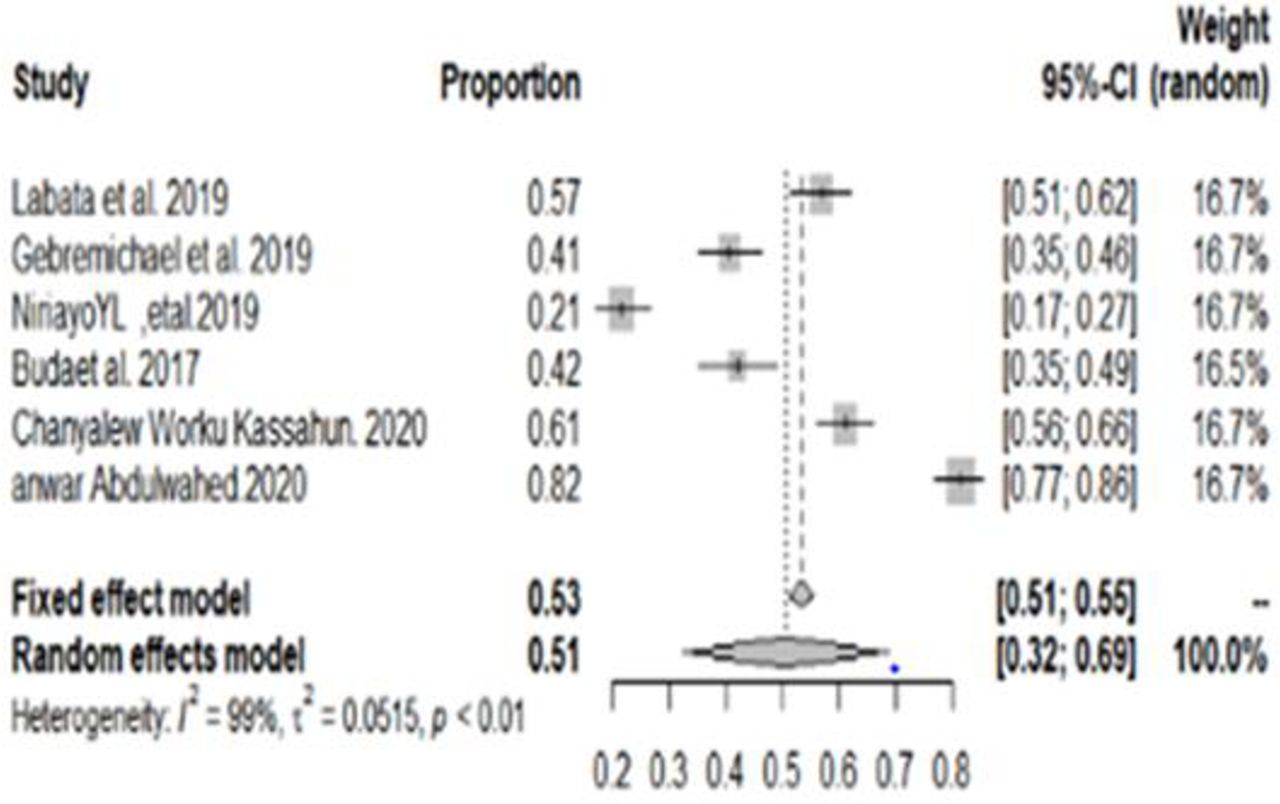
The subgroup analysis of good adherence to weight management was 51% (with 95% CI 32% to 69%) (figure 6).
Forest plot for subgroup analysis of adherence to weight management among hypertensive patients in Ethiopia, 2020.
Adherence to physical exercise
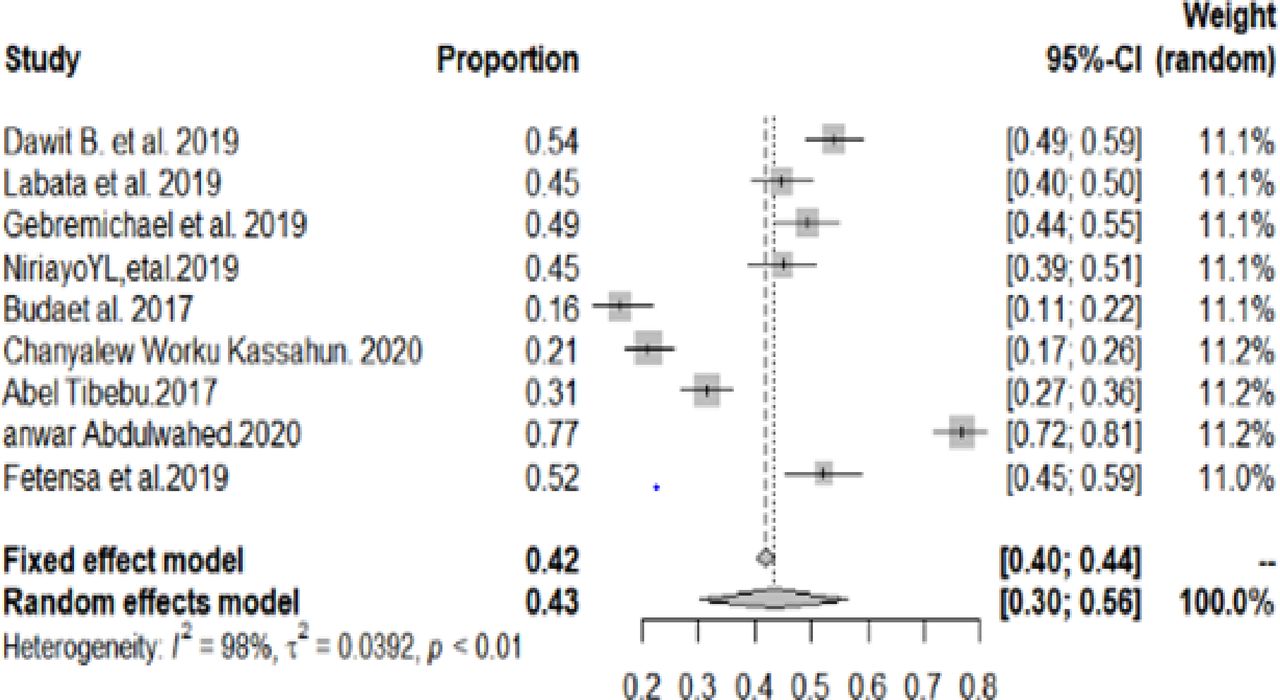
The pooled good adherence to physical exercise was 43% (with 95% CI 30% to 56%) (figure 7).

Forest plot for subgroup analysis of adherence to physical exercise among hypertensive patients in Ethiopia, 2020.
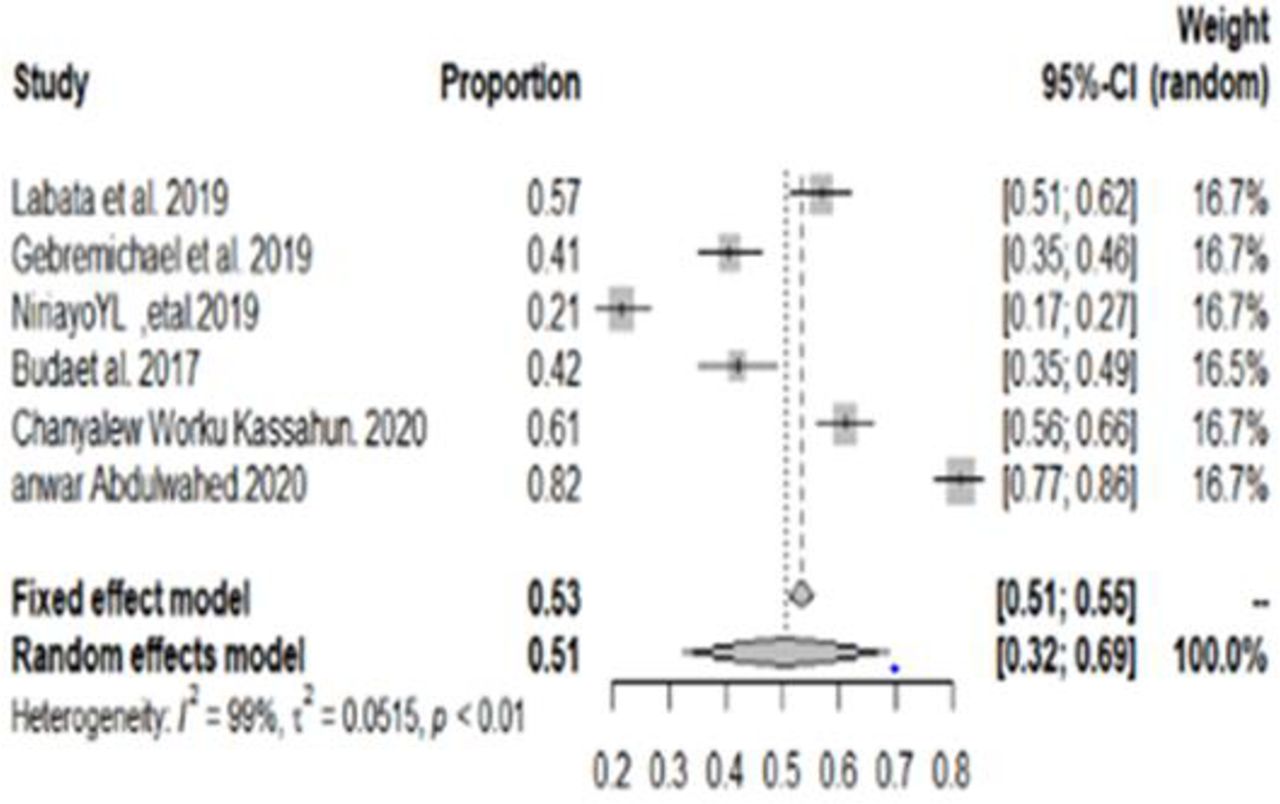
Adherence to a low-salt diet
In this meta-analysis, 52 %(with 95% CI; 39 to 66) of patients with HTN were engaged in the recommended low-salt diet (figure 8).

Forest plot for subgroup analysis of adherence to a low-salt diet among hypertensive patients in Ethiopia, 2020.
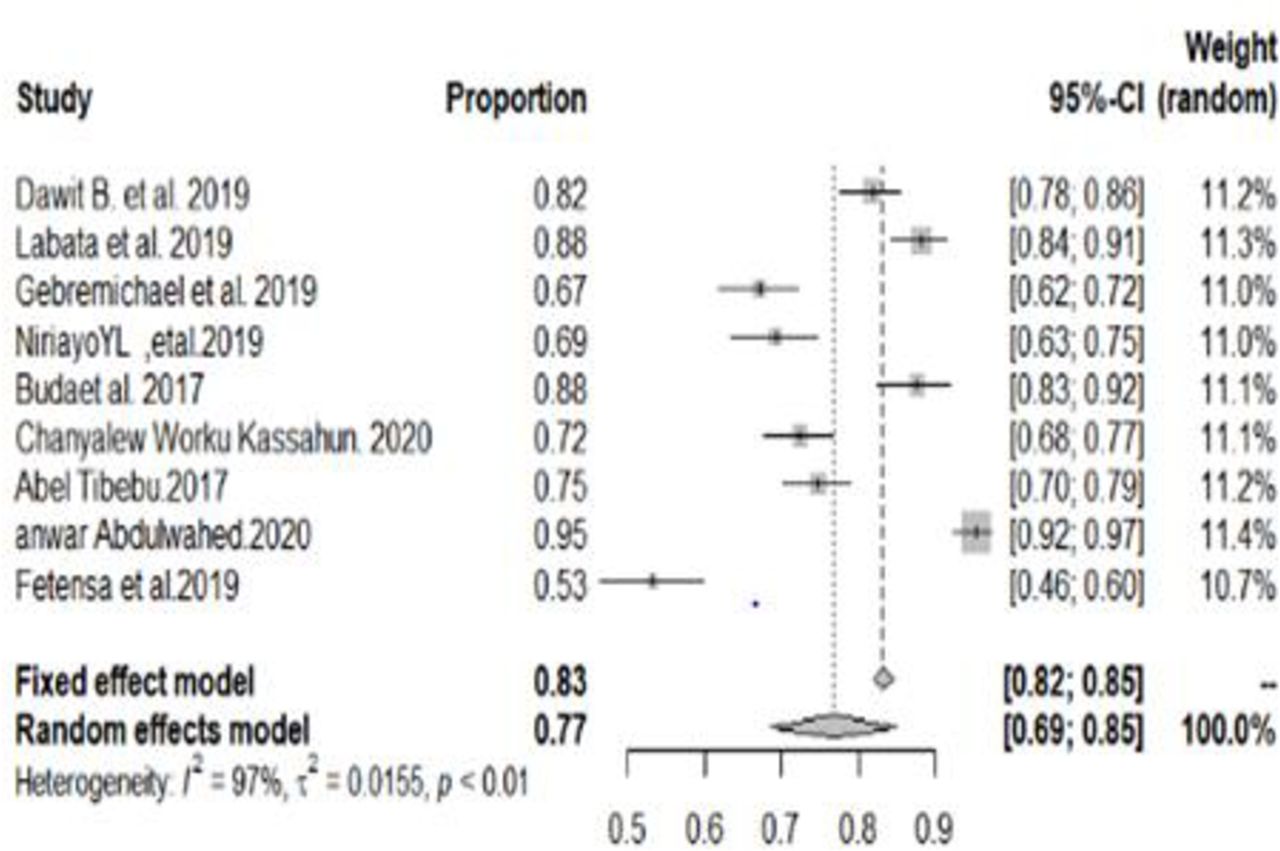
Adherence to alcohol abstinence
In this subgroup analysis, three-fourth of the hypertensive patients followed the recommended practice to abstain from alcohol consumption (figure 9).
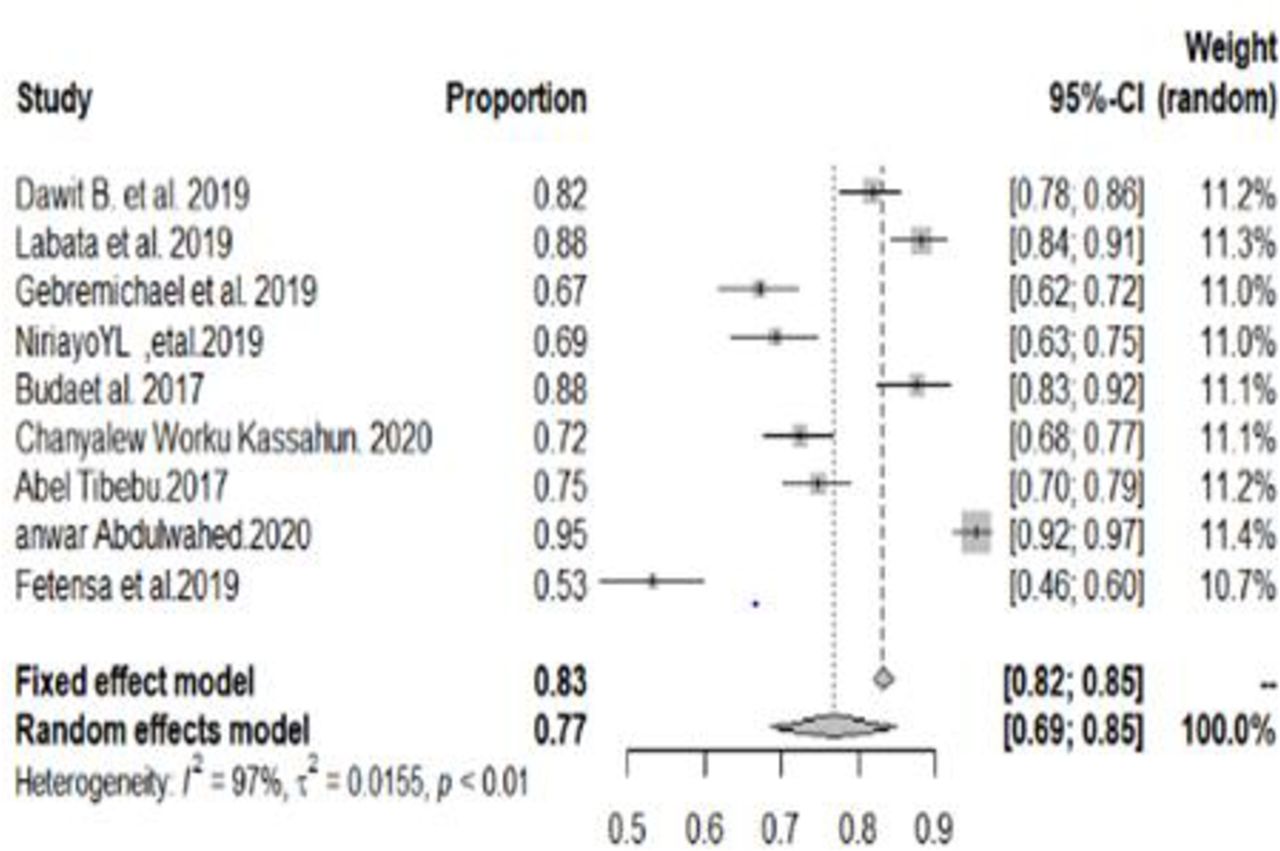
Forest plot for subgroup analysis of adherence to alcohol abstinence among hypertensive patients in Ethiopia, 2020.
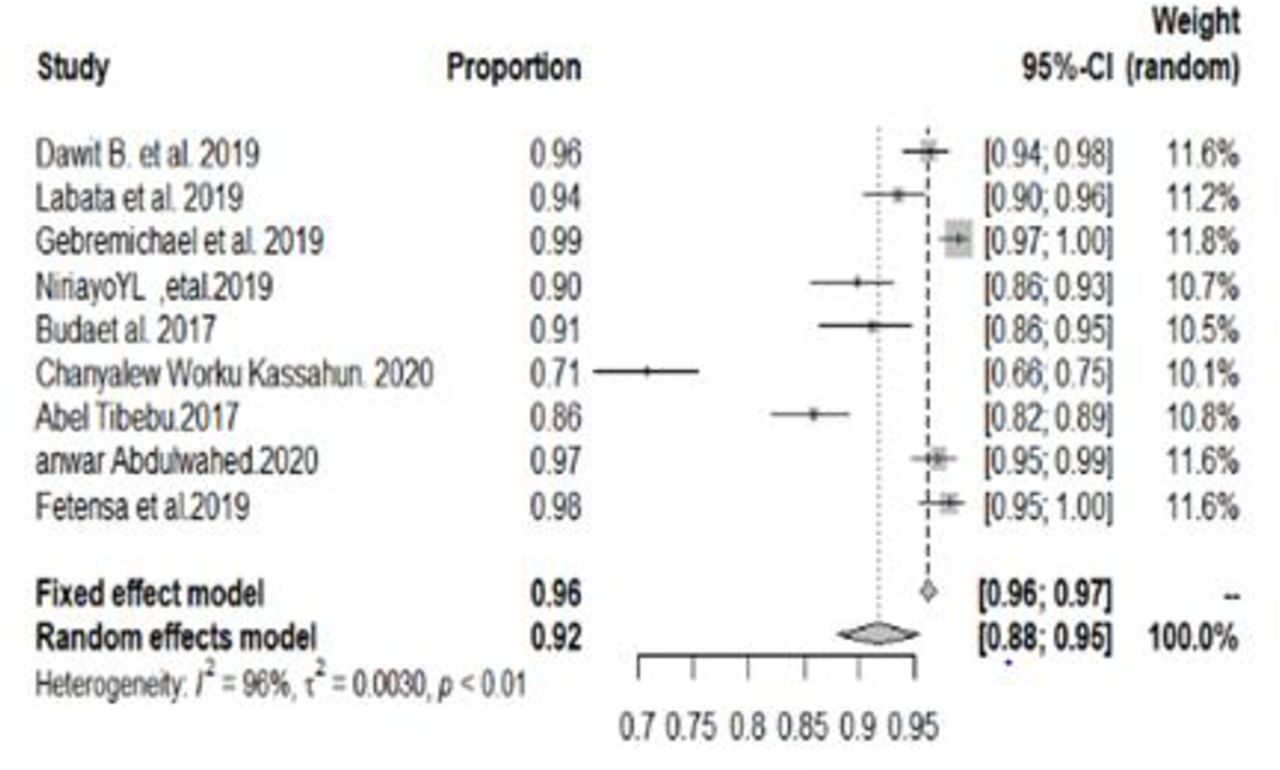
Adherence to non-smoking
The subgroup analysis towards the recommended adherence to non-smoking among hypertensive patients was 92% (with 95% CI 88% to 96%) (figure 10).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for subgroup analysis of adherence to non-smoking among hypertensive patients in Ethiopia, 2020.
Discussion
This systematic review and meta-analysis was performed to produce a pooled estimation of SCP among patients with HTN in Ethiopia. Individually, there was a variety in the prevalence of good SCP in the studies included in our review, which ranged from 20% as reported by Gebremichael et al27 to 70% as reported by Fetensa et al.28
This meta-analysis showed that the pooled estimate of good SCP in Ethiopia stands at 44% (95% CI 34% to 53%). The pooled estimate of good SCP in this study (44%) was lower than that in the study conducted in Saudi Arabia (74.4%)29 and Ghana (72%)30 but higher than that in the study conducted in Kenya 13%).31
To obtain the heterogeneity of the studies included in this review, we conducted a subgroup analysis by the domains of SCP and found that good adherence to medication was 65% (with 95% CI 45% to 85%), and this in line with the study conducted in South Africa (63%),32 Turkey (78%),33 Bangladesh (52%)34 and Saudi Arabia (46.7% and 79.3%).29 Our finding was also similar to that of the WHO report that rates the adherence to pharmacological treatment by patients with HTN varying between 20% and 80%35 and the systematic review conducted in Portugal (55.3%).36 However, the finding of the current study is higher than the figure reported in Saudi Arabia (33.3%)37 and Iran (36%).38 On the contrary, this finding is lower than that of the study conducted in Nepal (92%)39 and Netherlands (84%).40 This discrepancy could be due to differences in healthcare settings, such as tertiary and primary healthcare, that may cause a difference in screening tools and assessment practice. Moreover, it may also be because there is no uniform assessment measurement criterion in clinical practice in all healthcare settings or the use by different clinicians of their unique clinical expertise in the examination and individualisation of their patients.
The subgroup analysis of adherence to weight management was 51% (with 95% CI 32% to 69%). This finding was consistent with the result conducted in Iran (39%).41 42 On the other side, this finding was lower than that of a report in Kenya (90.5%).31 39
In this meta-analysis, 43% (with 95% CI 30% to 56%) of participants have good adherence to the recommended exercise. This finding was higher than that of a study conducted in Turkey (20.6%)41 43 and Iran.41 42 The finding was lower than that of a study conducted in Kenya (67%).31 39 The discrepancy might be explained due to sociocultural differences, the difference in the, as well as the level of education, provided for hypertensive patients.
In this meta-analysis, 52% (with 95% CI 39% to 66%) of patients with HTN were engaged in the recommended low-salt diet. This finding was similar to that of the study conducted in Kenya (63%).31 39 Our findings were lower than that of the study conducted in Nepal (74%).39 44 On the contrary, findings in this study were higher than those in the study conducted in Iran (12.3%).41 42
In this subgroup analysis, more than three-fourth (77%, 95% CI 69% to 85%) of the hypertensive patients were following the recommended alcohol consumption. This finding is similar to that of the study conducted in Nepal (84%)44 and Iran (86.7%),41 42 but higher than that of a study conducted in Kenya (49.5%).31 39
The subgroup analysis towards adherence to non-smoking among hypertensive patients was 92% (with 95% CI 88% to 96%). This finding was comparable with that of the study in Kenya (90.5%).31 39 The findings in this study are higher than those of the study conducted in Turkey (49.0%).41 43 Our finding was lower than that of the study conducted in Nepal (80%).44 In the opposite side, our finding was lower than that of the study conducted in Iran (100%).41 42
Our findings from the meta-analysis have implications in clinical practice as it can contribute to giving attention to the prevention and care of patients with HTN. This pooled point of estimates for SCP in patients with HTN provides updated evidence to advance prevention strategy, serves as key indicator of patient safety, and reflects the quality of healthcare service and appropriate intervention strategy for those patients with poor SCP. Use of adherence interventions, such as patient education and counselling on how to self-monitor blood pressure, and lifestyle modification interventions, such as exercise, weight reduction and healthy diet. Therefore, the blood pressure control strategy should keep in mind that, in addition to prescribing appropriate anti-HTN medicines and hypertensive SCP, they need to include resources that help patients overcome individual challenges to reduce the development of such HTN complications using SCP. The implication of this study, particularly the pronounced variation between studies (20%–70%), reflects that patients with HTN require development of standards for management and implementation of endorsed guidelines for SCP.
Conclusion
The pooled estimation of good SCP is low at the national level. The ministry of health, health policymakers, clinicians and other healthcare providers should strengthen the quality of healthcare service for patients with HTN that can help to increase SCP.
Strengths and limitations of this study
To the best of our knowledge, this is the first and only systematic review and meta-analysis that has focused on self-care in Ethiopia. Strong and reliable methodological and statistical procedures were used in this review. Different studies use different variables; this results in variation in the significant variables.
Data availability statement
Data are available upon reasonable request. NA.
References
Footnotes
Contributors Both authors, DBT and HG, conceived and designed the study, conducted the literature search, and extracted and analysed the data; drafted the manuscript; critically revised the manuscript; and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.