Article Text

Abstract
Objectives To highlight the need for standardisation in the communication of head impact telemetry from instrumented mouthguards (iMG). The purpose of this study is to examine how the frame of reference for reporting head acceleration events (HAE) may affect the interpretation of head impacts recorded from iMGs in community rugby players.
Methods An analytical investigation of 825 video verified HAEs recorded from male community players during 5 rugby match exposures. HAEs were captured with an iMG, known to be reliable and valid for this purpose. The linear and angular head acceleration at the centre of mass (head_CG) was calculated from filtered iMG accelerometer and gyroscope data, and the location of impact was estimated. The iMG and head_CG data were examined for systematic bias, geometric differences and the degree of concordance. Finally, mixed model analyses were fitted to assess the differences in peak resultant acceleration (PLA) by impact locations and directions of head motion while controlling for intra-athlete correlations.
Results The degree of concordance between the iMG versus head_CG measures varied by impact location. The mixed model confirmed differences in the PLA by location (F(8,819) = 16.55, p<0.001) and by direction of head motion (F(5,417) = 7.78, p<0.001).
Conclusion The head acceleration reported at the iMG is not proportional to measurements that have been transformed to the head_CG. Depending on the impact location and direction of head motion, the acceleration measured at the iMG may overestimate, underestimate or miss entirely the PLA with respect to the head_CG. We recommend standardising the reporting of iMG data within the head_CG frame of reference.
- Biomechanics
- Contact sports
- Head
- Measurement
- Accelerometer
Data availability statement
Data are available on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
There is some scepticism within the public and medical sector regarding the clinical value of field measurements of head acceleration events from telemetered instrumentation.
There is significant disparity among the rugby head acceleration event data reported in the literature.
Signal processing algorithms differ between instrumented mouthguard (iMG) products, which may lead to differences in reporting of head acceleration events captured in contact sports.
WHAT THIS STUDY ADDS
This study elucidates a significant source of bias that may exist within the current literature where telemetered head kinematic data has been reported.
The findings emphasise the importance of an agreed standard for reporting of head acceleration events collected with iMG devices.
Offers a simple explanation and methodological approach for a non-engineer audience.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Provides researchers, practitioners and journal reviewers with scientific background for evaluating studies that report head kinematics from iMGs.
Standardising the reporting of head impact data will allow greater generalisability of findings across study populations and allow data to be pooled across studies increasing the power for statistical analyses.
Being able to pool data is important for determining critical thresholds for head acceleration events associated with negative clinical outcomes such as concussion.
Introduction
The risk of concussion in rugby union is an ongoing concern as it is for many collision sports.1 The growing concern around concussions in rugby is evident in the published research. According to PubMed, in 2021, there was a 1200% increase in the number of publications about concussions in rugby compared with 2010.2 With such growing concern, there is currently a considerable appetite for on-field instrumentation that may monitor significant head acceleration events (HAEs) in real time.3–7 Most collision sports require athletes to wear mouthguards for participation, therefore making it easier to get athlete buy-in for wearing an instrumented version. Coupling of the mouthguard instrumentation to the dentition of the athlete has significantly improved the accuracy of telemetered head kinematics during contact events when compared with skin or helmet-mounted devices.8 Therefore, instrumented mouthguards (iMGs) show substantial promise for improving accuracy in real-time measurement of HAE in field sports.9–12 The data collected can be used to improve player welfare by informing decisions regarding training loads.6 13 For clinicians and sports scientists, the hope is that real-time on-field evaluation of head impacts will lead to earlier detection of potential injurious events, support earlier medical intervention and removal from play for at-risk players.14
Currently, there are many iMG products on the market, but no accepted gold standard for collecting, postprocessing or rendering this data. Variations in data handling may lead to inconsistencies among the reported data in the literature.15 The inconsistencies in the reported data create difficulties for scientists, clinicians or sport’s governing bodies to use the existing data to make determinations regarding safety thresholds for HAEs.16 Having trust in existing data is important particularly when making or changing policy guidelines regarding contact training for a collision sport (eg, The Football Association, 2021). One such inconsistency in the existing literature is in the variation of frame of reference used for reporting head kinematic data. The centre of gravity is the most common frame of reference used when following standardised reporting of impact kinematics in laboratory-based studies.9 17 Yet, in relation to in-field head kinematics, some publications report data from the iMG frame of reference,18 19 others from the centre of gravity of the head,5 while some give no specific mention to the frame of reference used.14 Agreeing to a standardised frame of reference when reporting kinematic data aids in the generalisability and comparability of the data person to person and study to study.20 The purpose of this study is to examine how the frame of reference for reporting HAEs may affect the interpretation of head impacts recorded from iMGs in a sample of community rugby players.
Methods
Participants
This prospective observation study examined HAEs using iMGs in a convenience sample of four premier senior men’s teams (highest level of amateur rugby in NZ) over five regular season games during the 2021 community rugby season.
Study protocol
Preseason, participants completed a paper-based questionnaire capturing key demographic variables such as age, weight, height, playing position, years rugby experience, history of previous concussions. Each athlete was fitted with a boil-n-bite iMG (Prevent Biometrics, Minnesota, USA) by a qualified dentist to maximise coupling of the iMG to the player’s unique dentition.
All game events were video recorded with high-definition cameras from three field angles, including a GoPro (Hero8, GoPro, USA) attached to the head of the match referee. The video content from the three cameras was synced and imported into Hudl Sportscode (V.11, Agile sports Technologies, NE, USA) video analysis software along with an xml file containing the iMG event data for all players in each match. Each iMG was then time synchronised to the Sportscode timeline using a real-world time flash recorded in the video. The unique serial number from the iMG was matched to the corresponding player jersey number. All HAEs for each player were video verified as either direct head contact or indirect HAE by a trained analyst and confirmed by a second reviewer. A direct head contact event occurs when the iMG is triggered by a direct impact on the head. In contrast, an indirect acceleration event occurs where no direct contact is made with the head, but contact is made with the body resulting in a whiplash-like inertial acceleration of the head triggering the iMG.
Study equipment
Each iMG included a 3.2 kHz triaxial accelerometer and gyroscope to capture linear acceleration and rotational velocity and has been validated both in the laboratory and in-field.9 11 12 Two independent studies Liu et al9 and Kieffer et al12 found Prevent boil-and-bite mouthguards to have a concordance correlation agreement with laboratory reference measures of 0.95 for peak linear acceleration (PLA) and 0.95 for peak angular acceleration (PAA). The precision of the mouthguard to detect true on-field impact events was found to be 82% (95% CI 75% to 88%). For this study, the trigger threshold was set at 5 g on a single axis, with a 50 ms sampling window.15
Data reduction and processing
Transforming iMG HAE to head_CG
All postprocessing and data reduction were performed with purpose-written Matlab routines (R2021b, Mathworks, California, USA). The raw linear acceleration and angular velocity data from the iMG accelerometer and gyroscope were imported into Matlab and filtered with a 200 Hz low-pass, fourth-order Butterworth filter. The location and coordinate system for the head_CG was defined as that of the 50th centile male based on the Hybrid III crash test anatomical model.3 21 The iMG frame of reference at the mouth (m) and the head_CG (h) are shown in figure 1. The PLA variables, PLAiMG calculated as the raw filtered data measured at the iMG reference and PLACG, which is filtered and transformed to the head_CG reference.

The accelerometer iMG reference frame (m) and the head_CG reference frame (h). CG, center of gravity; iMG, instrumented mouthguards.
To calculate the acceleration of the head_CG (ah), it is assumed that the head is a rigid object and the iMG maintains a fixed orientation and distance (rm) from the head_CG. Therefore, the iMG and the head_CG have the same angular velocity (ω) and angular acceleration (α). The difference in acceleration between the two frame of references can be described by the relative acceleration (equation 1). The relative acceleration has two components, the tangential acceleration (at), which acts on a tangent of a circle on a plane perpendicular to the angular acceleration vector (figure 2) and the radial acceleration (ar), which acts radially towards the centre of a circle perpendicular to the angular velocity vector (equation 2). As shown in figure 2, the tangential acceleration increases proportionately with distance from the iMG.
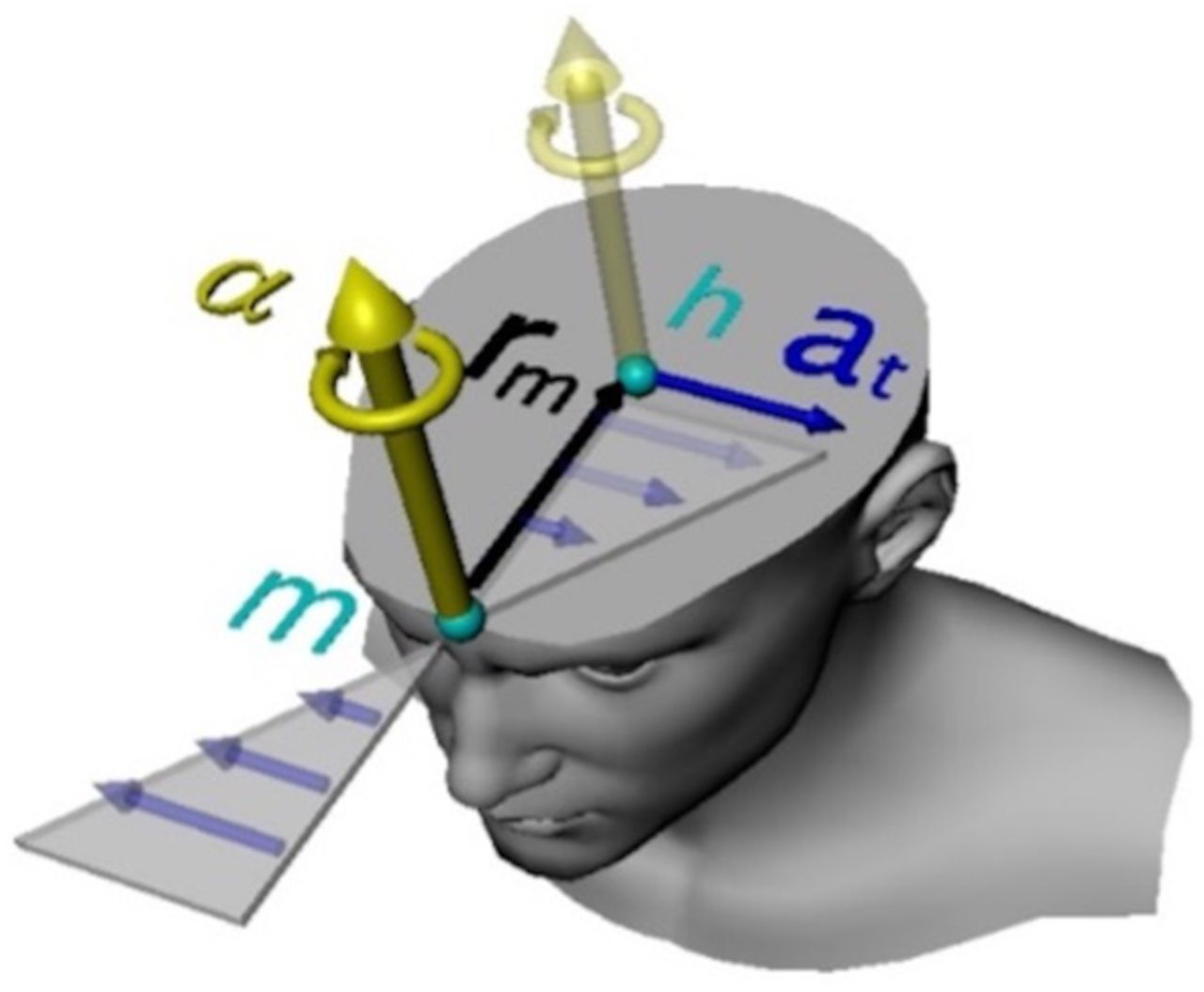
Illustration of how the tangential acceleration vector (at) at the head_CG (h) relative to the iMG (m) is generated by the head angular acceleration vector (α) and the radial distance (rm). For clarification, all three-dimensional vectors and locations in figures in this paper are simplified to their components on a single plane and the angular acceleration vector is shown with the left-hand rule direction rather than the traditional right-hand rule. CG, center of gravity; iMG, instrumented mouthguards.


The relation between the iMG and head_CG linear acceleration in equation 1 is fully expressed in (equation 3), showing the role of the angular velocity (ω) and angular acceleration (α). The angular acceleration was calculated as a derivative of the filtered angular velocity using the MATLAB gradient function. The angular acceleration is filtered, the radial (ar) and tangential (at) accelerations are calculated and added to filtered linear acceleration from the iMG (am).

Determining location of impact and direction of head rotation
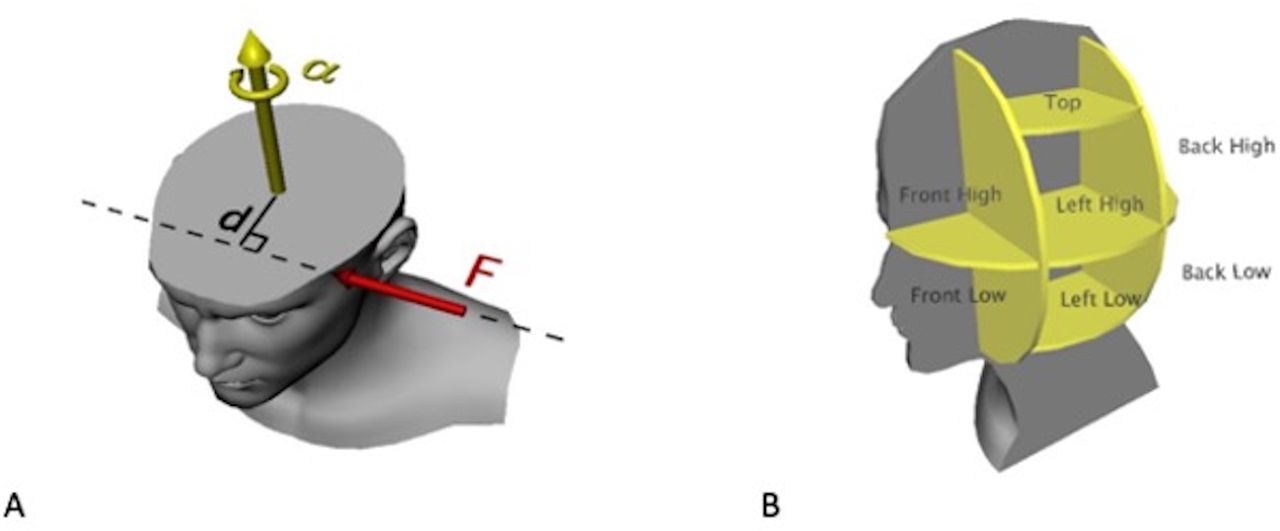
Assuming that the accelerations during HAEs are created by a single impulsive force and that the head is approximated by a rigid sphere, the force magnitude, direction and location of impact can be estimated. The magnitude and direction of the impulsive force is calculated using the head acceleration multiplied by the estimated head mass (F=ma) (figure 3A). An iteration method was used to calculate the location of impact on the head required to generate the impact angular acceleration (figure 3B). The location of impact was designated (back high, back low, front high, front low, left high, left low, right high, right low, top) in accordance to point of force application (figure 3A). Front and back and top and bottom was designated as being greater than 4 cm from the head_CG along each respective axis. The motion of the head was categorised (head backward, head forward, tilt left, tilt right, turn left, turn right) from the dominant direction of the angular acceleration. Tilt represents rotation of the head about the anterior–posterior axis (ear to shoulder) and turn represents rotation of the head about the vertical axis.
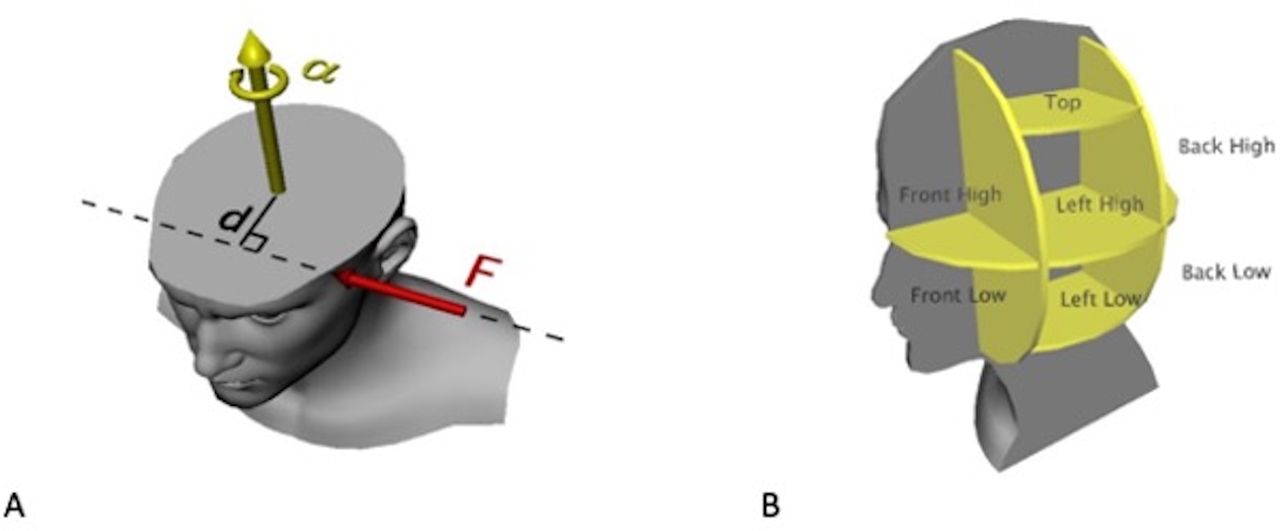
(A) Illustration of how impulse force (F) generates angular acceleration (α). The magnitude of the angular acceleration also depends on the distance (d) of the force line of action to the head_CG; (B) Illustration of how the impact location was described with respect to regions in the head reference.
Statistical analysis
Demographic details age, height, weight, years of rugby experience and the number of head impacts sustained over the study period are reported using mean, SD and range. Ethnicity and history of previously diagnosed concussions were recorded using frequency and presented as percentages. The statistical analysis was carried out with SPSS (V.26, IBM) and R (V.4.0.3; R_Core_Team 2015) with alpha at p≤0.05. Inter-rater agreement was evaluated for the verification of HAE events as either yes/no and event type direct/indirect, with the Cohen’s kappa. Verified head impact data were used to quantify the HAE in terms of median and IQR resultant peak head acceleration (PLACG & PLAiMG) and PAA from the two frames of reference. The PLACG versus PLAiMG were examined for the presence of systematic or proportional bias using a Bland-Altman analysis with linear regression.22 23 The level of agreement between the two measures was examined using Lin’s concordance correlation coefficients (LCCC) and associated 95% confidence limits.24 Strength of agreement criteria for LCCC was >0.8 very strong, 0.6–0.8 strong, 0.3–0.5 fair and <0.3 poor.25 The geometric differences between the iMG and head_CG resultant waveforms were measured using the root mean square deviation (RMSD, equation 4). The RMSD was normalised (NRMSD) to the PLAiMG to give the percentage difference between the two measurements.26 Finally, mixed model analyses were fitted to assess the differences in PLA measures (PLACG vs PLAiMG) by impact locations (frame of reference × impact location) and directions of head motion (frame of reference × head motion) while controlling for intra-athlete correlations. Post hoc tests compared frame of reference PLA for each impact location or head motion, using Sidak adjustments to control for type I error. For inference testing, log-transformations were applied due to the right skew distribution of the PLA data.

Results
Demographic details
A total of 1406 HAEs were captured over five games from 56 individual players. Demographic details, rugby player experience and concussion history, are presented in table 1. All HAEs were video verified by an experienced rugby performance analyst and confirmed by a second reviewer. Inter-rater agreement for verification of HAEs was κ=0.873 (95% CI 0.824 to 0.923), and for determination as Direct or Indirect κ=0.826 (95% CI 0.781 to 0.870). After the verification process, 85% (n=1199) of events were confirmed as true direct or indirect HAE. The indirect HAEs were removed, leaving 825 direct-head-impact HAEs included in the final analysis.
Participant demographic variables
Agreement between measurements
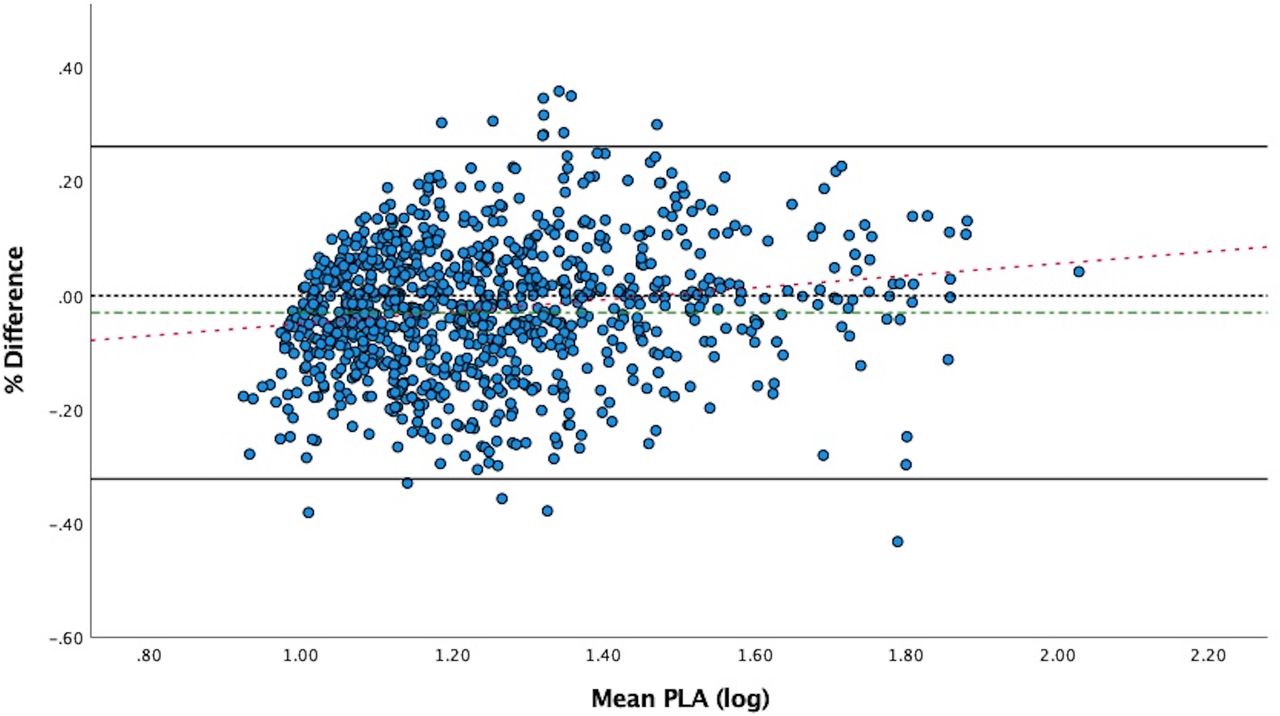
The Bland-Altman analysis performed on the log-transformed data (figure 4) confirms a significant proportional bias (ß=0.172, t=−6.104, p<0.001) between the PLA measures from the two frames of reference. Medians and IQRs of PAA, PLAiMG and PLACG are presented in table 2 by impact location. The level of agreement between the two measures ranged from poor to fair (eg, LCCC=0.51 (0.27, 0.67)) to strong to very strong25 (eg, LCCC=0.88 (0.84, 0.91)) dependent on location of impact (table 2). The median geometric differences (RMSD) for the iMG and head_CG resultant waveforms are similar across all impact locations, 1.87–2.5 g. However, the range for the RMSD median values indicate a particularly wide spread of differences for some impact events such as the right_high (range=37.7 g) or front_low (range=28.33 g).

Bland-Altman plot visualising the agreement between the iMG and head_CG measurements. The x-axis shows the average of the paired log transformed iMG and head_CG measurements. The y-axis is normalised to per cent difference (iMG - head_CG) to minimise heteroskedasticity. Black lines represent the bound of the 95% limits of agreement (LOA= −32.25% to 26.11%) defined as the range of difference for of the measurements. The green dashed line represents the mean bias (−3.07%), while the red dashed line represents the proportional bias (slope 0.172, SE 0.025). CG, center of gravity; iMG, instrumented mouthguards; PLA, peak linear acceleration.
Comparison of head acceleration events between iMG and CG frames of reference for each direction of head motion
Mixed model analysis comparing measures across PLA impact location and head motion
Mean differences between PLAiMG and PLACG measures by impact location are presented in figure 5. The results of the mixed model showed a significant effect for frame of reference × impact location (F(8,819) = 16.55, p<0.001). Post hoc comparisons showed significant differences in PLA between iMG and head_CG for back_high (t=3.89, p<0.001), back_low (t=2.52, p=0.01), front_low (t=−7.40, p<0.001), left_high (t=2.06, p=0.04), right_high (t=4.64, p<0.001), right_low (t=−2.23, p=0.03), top (t=6.45, p<0.001).

95% CI of the mean differences in PLA magnitudes between the two frames-of-reference. Black bars on figure represent locations of impact that were significantly different between the iMG and had_CG reference frames in the Mixed Model (p<0.05). Percentages show what percentage of the data set is represented within that impact location. Positive values indicate significant iMG underestimation of the HAE at the CG and negative values indicate significant iMG overestimation of the HAE at the CG. CG, center of gravity; HAE, head acceleration event; iMG, instrumented mouthguards; PLA, peak linear acceleration.
The comparison of iMG and head_CG measurements for each direction of head motion is presented in table 3. The mixed model analysis also showed a significant effect for frame of reference × head motion (F(5,417) = 7.78, p<0.001). Post hoc comparisons showed significant differences in PLA between iMG and head_CG for head backward (t=3.37, p=0.001), tilt left (t=3.46, p=0.001), tilt right (t=4.42, p<0.001), turn right (t=−2.94, p=0.003).
Comparison of head acceleration events (HAE), in the iMG and CG frame of references for each direction of head motion
Discussion
This study examined the differences in head acceleration when measured from the iMG frame of reference compared with data that is transformed to the anatomically relevant frame of reference located at the centre of gravity of the head (head_CG). The findings show that measurements from these two systems are not equivalent, with statistically significant differences being identified depending on the impact location as well as the direction of head motion. The RMS deviations between the iMG and the head_CG (center of gravity) range from 1 to 37 g, but more critically, the differences appear to increase with magnitude of impact event. The NRMS deviations normalised to the peak acceleration was 40% for the highest acceleration values. This magnitude of error in the PLA due to the reference system could mean that a 60 g event may be wrongly reported as either 95 g or 35 g, depending on the impact kinematics and location. The rationale for the observed differences between measures is described below with basic biomechanics principles and highlights specific real-life scenarios we identified in our current rugby data set.
Basic rigid body mechanics can help explain why the iMG acceleration does not accurately describe the acceleration of the head mass. Due to the anatomical constraints on the head mass, nearly all impact forces applied to the head will cause some translation of the head combined with rotation. When the rigid body rotates about its centre, the points on the surface of the body will travel further in the same time frame compared with points near the centre of mass, thus, the points on the surface experience greater tangential velocity and acceleration. It may help to think of a merry-go-round and how difficult it feels to hang-on when near the outside compared with being near the centre. Because of the tangential acceleration effect, the linear acceleration at the iMG is not the same as the acceleration at the centre of the head.
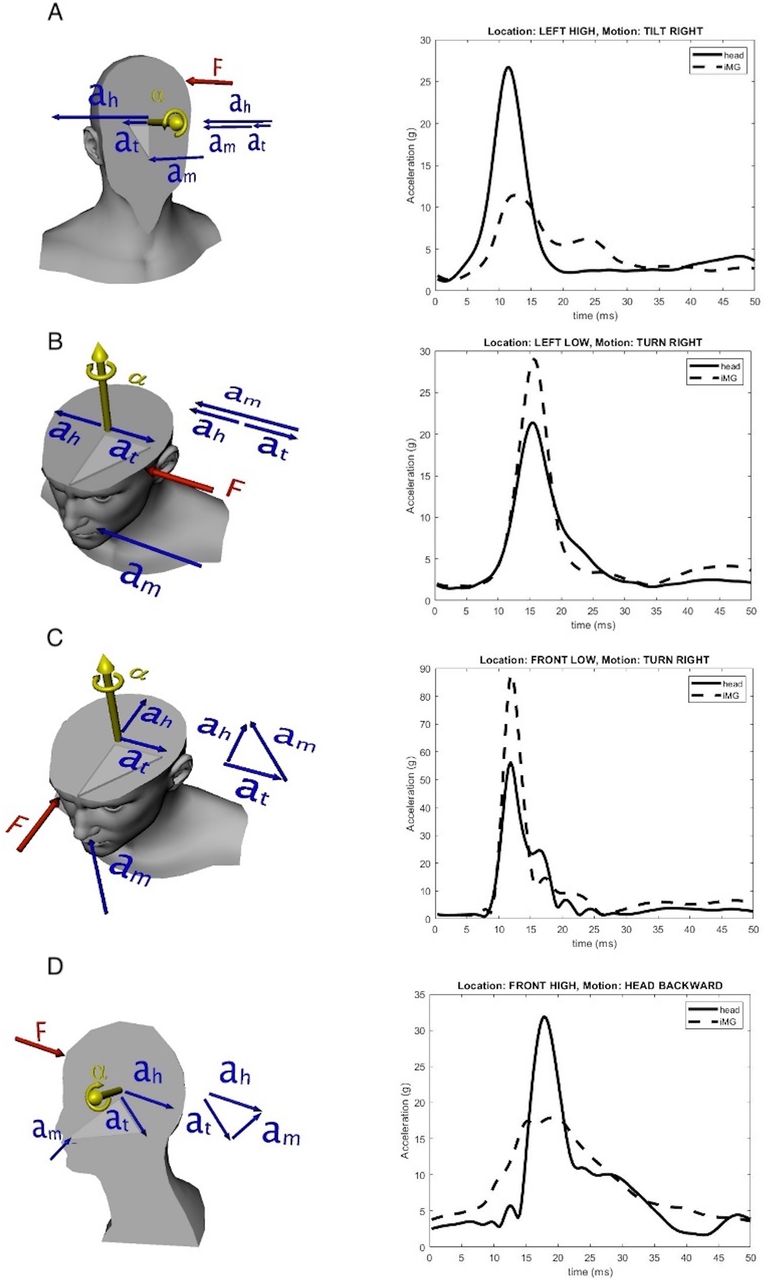
The significance of the tangential component can be seen in figure 6A–D. If for example, a medially (left high) directed impulse is coupled with frontal axis rotational acceleration impulse causing the head to tilt to the right, the tangential acceleration acts in the same direction as the mouth acceleration (figure 6A). In this circumstance, the head acceleration is larger than the acceleration of the mouth and the iMG underestimates the head_CG, the PLA_iMG will be lower than the true PLA_CG. Conversely, when the tangential acceleration acts in the opposite direction of the mouth acceleration, with LEFT directed impulse coupled with an axial acceleration impulse that rotates the head to the right, the head acceleration is smaller than the mouth and thereby the iMG overestimates the head acceleration (figure 6B). In this instance the PLA_iMG will be larger than the PLA_CG. As shown in figure 6C,D, the tangential acceleration can also act at right angles to impact forces resulting in, not only, an increase or decrease in acceleration, but also a change in direction that is not realised in the PLA. In all instances, the iMG measure would not accurately describe the head_CG for the impulsive event. Moreover, if these impacts were averaged together, the differences could cancel out and be missed. As we see from the total median values in table 2, median PLA=15.7 g at the iMG vs 17.1 g at the head_CG.
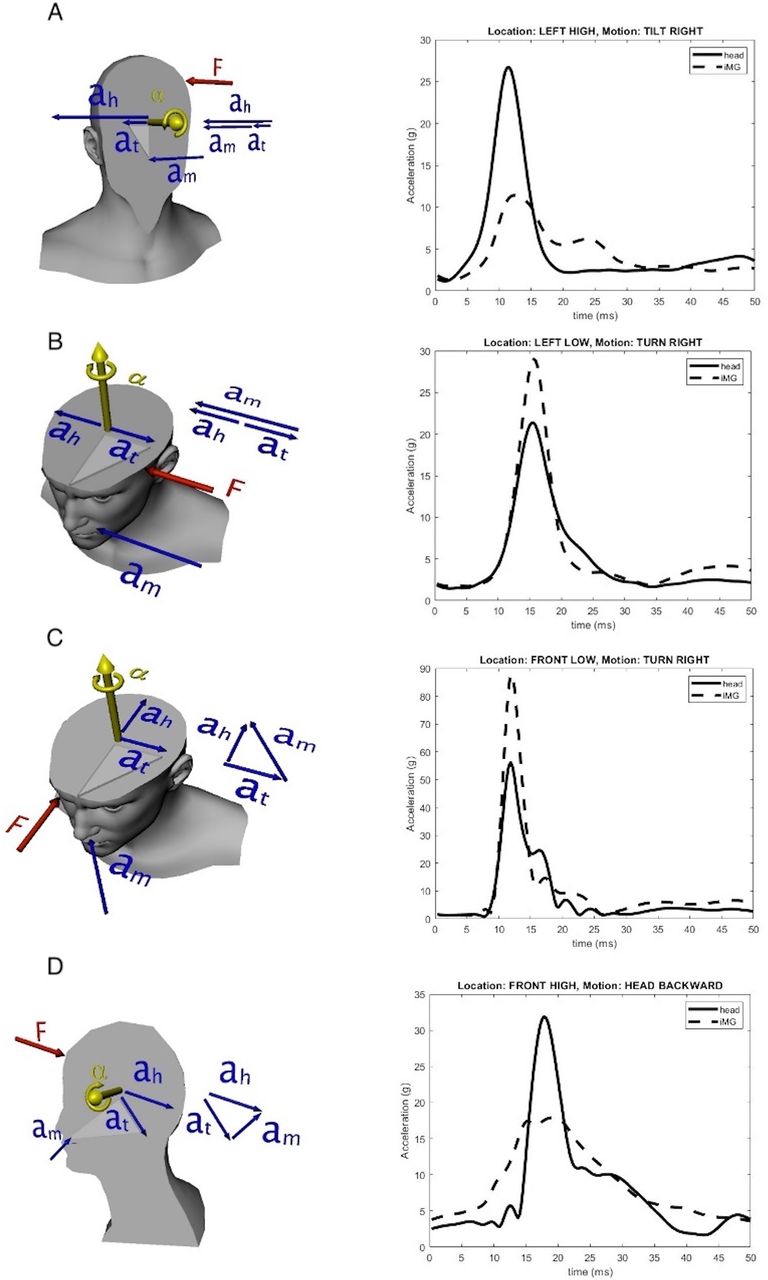
These cross-sections illustrate how linear acceleration measured at iMG (am) may be significantly different than at the head_CG (ah) due to the impact location (F) and resulting head motion (α). Most of the difference can be attributed to the tangential acceleration (at) shown by the vector summation diagrams (ah=am+at). (A) Left High, Tilt Right ah>am, (B) Left Low, Turn Right: am>Ah, (C) Front Low, Turn Right: am>Ah, (D) Front High, Head Backward: ah>am. CG, center of gravity; iMG, instrumented mouthguard.
Another significant issue that may arise, whereby the iMG will miss the peak acceleration entirely. As one may imagine there is a point in space about which the tangential acceleration acts equal and opposite to the direction of the head acceleration, effectively cancelling out the overall acceleration of the head—this point is called the pivot point. If the pivot point is near the mouth, the guard may only identify a small portion of the head acceleration. Such a situation may arise in a back low impact (figure 7A) where the head effectively pivots around the mouth and the iMG may miss the peak acceleration entirely (figure 7A). A similar finding was highlighted by Wang et al, as a potential cause for missing impact events if the trigger threshold is set too high.15 If the trigger threshold was set for 10 or 15 g, a significant impact event such as the one highlighted in figure 7B, could be missed. On the other hand, if the pivot point is far away, the guard is accelerated greater than the head (figure 7B). For example, in a front low impact, the pivot point is on the other side of the head from the guard, and the iMG is accelerated greater than the head centre (figure 7B). In this circumstance, the iMG will overestimate the PLA of the event.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of the pivot point and direction of linear acceleration impulse may affect the PLA (A) Miss completely the impact peak or (B) Overestimate. iMG, instrumented mouthguard; PLA, peak linear acceleration.
Limitations
The data used in the study were delimited to male adult rugby players and may not represent impact events in other sports. Most of our discussion has focused on the tangential acceleration effect although as outlined in equation 3, there is also a radial component that contributes to the difference between head and iMG accelerations. It was our finding within the Rugby data sample that the tangential acceleration effect was more dominant in most HAEs accounting for more than 90% of the difference in most cases. This may be different in other sporting contexts. Further, we assume that a single impulsive force is wholly responsible for the resulting angular acceleration.
Implications
There is poor agreement between filtered PLAiMG and the same HAE described with respect to an anatomically relevant frame-of-reference located in the centre of gravity of the head PLACG. In our current data set, in 73% of the impacts the iMG either overestimated, underestimated or missed entirely the PLA of the head_CG (figure 4). Such significant misalignment means that data from these two reference frames cannot be compared directly. Agreement in the industry about how HAE events are described and processed is important particularly for those attempting to use this data to inform policy and player welfare guidelines. As technology improves, iMGs are being used more frequently as a side-line tool for identifying in real-time, high-risk impact events.27 Yet not all iMG providers supply data standardised data to the end user.3 19 28 The less informed user may not fully understand how to interpret data presented in the arbitrary frame of reference of the iMG, which may lead to incorrect player welfare decisions being made. Our goal for this study was to provide sport science practitioners with the knowledge and understanding of the underlying mechanical principles of head kinematics which must be considered when choosing iMG devices and interpreting their data.
Aside from disagreement between reference frames, missed peaks may be more likely with a frame of reference that sits on the perimeter of the head. Impacts that cause the head to rotate about an axis aligned with the axis of the iMG, such as our back low impact example. These types of impacts are commonly associated with the head-to-ground mechanism in Rugby.29 Our data sample had only a small proportion of head-to-ground (back low) events, yet in some sports this mechanism may be more likely. For instance, in freestyle skiing the most common mechanism of head impact is from backward pitching falls.30 Such a mechanism would, putatively, lead to a higher proportion of back low acceleration impulses and if not standardising to head_CG a significant number of potentially dangerous impact events could be missed.
Conclusions
The main takeaway from this study is that acceleration events reported from the iMG frame of reference do not accurately reflect the acceleration of the head. Frames of reference imbedded in measurement devices are typically arbitrary in terms of the human system, they can only represent movement of the device. Transformation of the iMG acceleration measurements to the head_CG should be viewed as a form of normalisation of the data, which ensures generalisability and comparability of the HAE data person to person and study to study. This is something we should strive for across the industry.
Data availability statement
Data are available on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics name: University of Otago Human Ethics CommitteeID:H21_056UOHEC (Health) ID H21_056. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the sports analysts JJT, WW and JP, along with other research assistants who aided in the data collection and video coding of the impact data used in this study.
References
Footnotes
Contributors MDB wrote the statistical analysis plan, cleaned and analysed the data, and drafted and revised the paper. She is the guarantor. PD analysed the data and drafted and revised the paper. DS initiated the collaborative project, monitored data collection for the whole trial, and revised the draft paper. JR monitored data collection for the whole trial and revised the draft paper. DT and GS revised the draft paper.
Funding The data used in this paper were collected for a larger project, the ORCHID study, which is funded by World Rugby 2021–2022.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.