Article Text

Abstract
Background Following the first COVID-19 peak in 2020, came the seasonal childbirth peak at Hôpital Universitaire de Mirebalais (HUM). This peak is associated with overcrowding on the labour and delivery (L&D) ward. Lack of sufficient bed-space for sick neonates in the neonatal ICU at HUM, has led to overcrowding and lengthy stays of sick newborns on L&D. These conditions contribute to the subsequent lack of bed-space for newly postpartum mothers and potentially decreases quality of care for both new mothers and neonates.
Methods A Maternity Task Force was created by hospital leadership to address these urgent needs. The team’s objective was to eliminate mothers and newborns laying on the floor in L&D. The Six-Sigma/DMAIC quality improvement methodology was used as the problem was urgent, demanded rapid results and centred around the process of patient flow in the institution. Process flow chart and Ishikawa diagrams were used to identify the root causes of the issues.
Results An average of 22% of postpartum women did not have a bed preintervention and 0% of postpartum women were laying on the floor post intervention. An average of 33% of newborns received paediatric care on the maternity ward pre-intervention compared with an average of 17% postintervention. The team did not achieve its objective for this second indicator, which was to have less than 10% of sick newborns on the maternity ward receiving paediatric care.
Conclusion HUM hospital leadership took the vital decision to form the Maternity Task Force to make changes, which consequently led to a sustainable positive and lasting impact on the lives of new mothers and their babies at the institution. The objective of 0 postpartum mothers and newborns on the ground was achieved and fewer newborns receive intensive paediatric care on the maternity ward as a result of our interventions.
- Maternal Health Services
- Paediatrics
- Six Sigma
- Quality improvement
- Leadership
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Little is known in terms of resolving maternity services overcrowding using a QI approach in the existing literature. This project is important because this has not been addressed in low-resourced settings especially given the leadership and financial support that is requisite for success.
WHAT THIS STUDY ADDS
This Quality Improvement project used DMAIC as QI methodology in this international context, which allowed for the hospital leadership to take rapid decisions therefore inducing prompt results to address the root causes of overcrowding.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The Maternity Task Force required cross-sector teamwork and good planning of staff, stuff, space and systems to support the quality issues confronted and to address these appropriately.
Introduction
Problem description
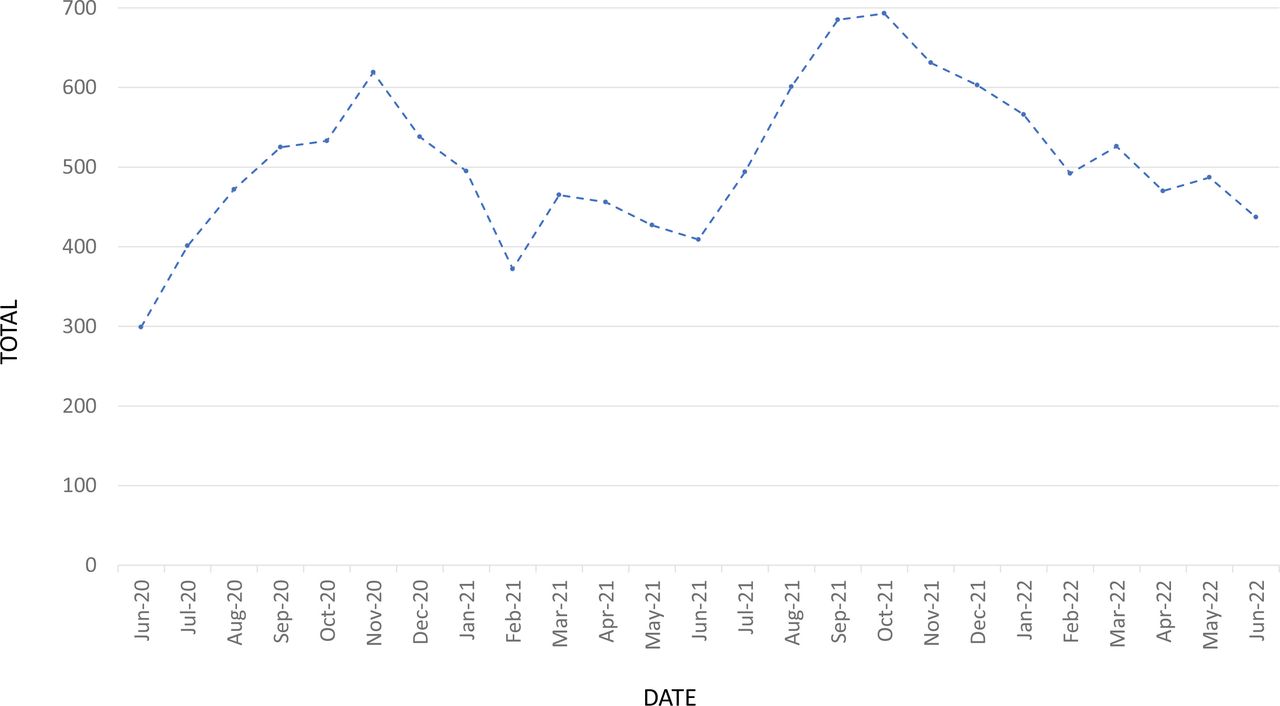
The data trends at Hôpital Universitaire de Mirebalais (HUM) for childbirth showed a seasonal peak that generally starts in August and lasts through November of each year (see figure 1).1 This peak is associated with not only overcrowding on the labour and delivery (L&D) ward, but also can affect the delay in paediatric care which can decrease the quality of care for both new mothers and newborns.
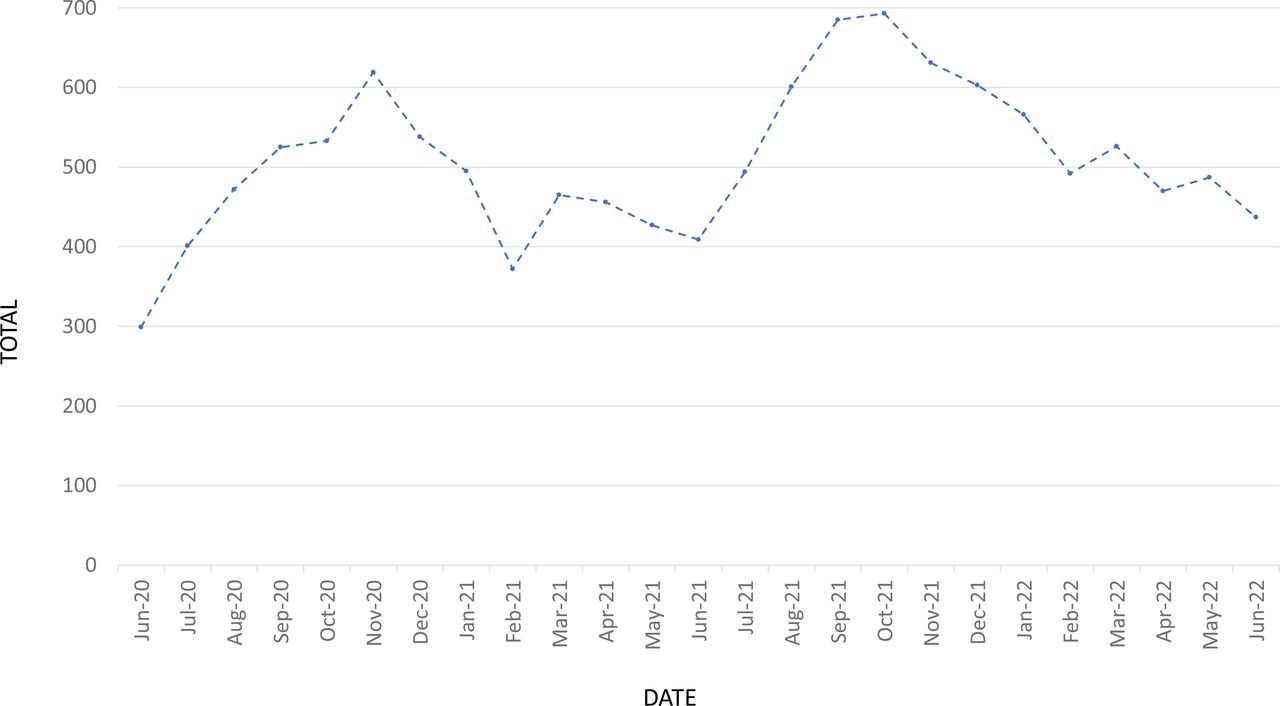
Deliveries per month HUM 2020–2022. HUM, Hôpital Universitaire de Mirebalais.
Available knowledge
Few studies were found during the literature search on the impact of overcrowding on quality of care in maternity services in international settings. Overcrowding in hospitals has been found to decrease quality of care received and increase morbidity and mortality.2 3 Outcomes in overcrowded emergency departments include long delays to receiving care, patients at risk for poor outcomes, prolonged pain and suffering, increased frustration and patient dissatisfaction with care.4 These same outcomes can be applied to maternity wards where overcrowding can have mortal consequences for mothers and fetus/neonates. Another study that looked at the frequency and outcomes of infection related maternal deaths in low-income and middle-income countries (LMICs) found that these accounted for more than half of the intrahospital maternal deaths.5 The added complexity of COVID-19 can also contribute to neonatal morbidity and mortality especially in overcrowded and resource-limited settings6 where nosocomial transmission of COVID-19 can spread rapidly.7 Previous studies have found that pandemics, such as Ebola in West Africa, can impact the provision of maternal health services.8 A modelling study from 2020 estimated an 8%–38% increase in maternal deaths per month due to reduced coverage of essential maternal and child health interventions due to supply chain interruptions across over 100 LMICs during the COVID-19 pandemic.9 According to the authors, the reduced coverage of four key interventions that included parenteral administration of uterotonics, antibiotics and anticonvulsants, and clean birth environments would account for approximately 60% additional maternal deaths.9
Rationale
Infection acquired in hospital leads to increased morbidity and mortality, which has added significantly to the economic burden on institutions; especially those in lower-resourced countries.10 This could also potentially contribute to an increased risk for acquisition of nosocomial SARS COV-2 infection transmission as found by Nakstad et al, in a small study this past year.6 The lack of space for sick neonates to be transferred to the 16-bed neonatal ICU (NICU) at HUM, has led to premature and sick neonates spending weeks on L&D with their mothers. These conditions can contribute to an increase in morbidity and mortality among well neonates on the maternity ward due to a lack of beds for newly postpartum mothers who end up on the ground in the ward.
Specific aim
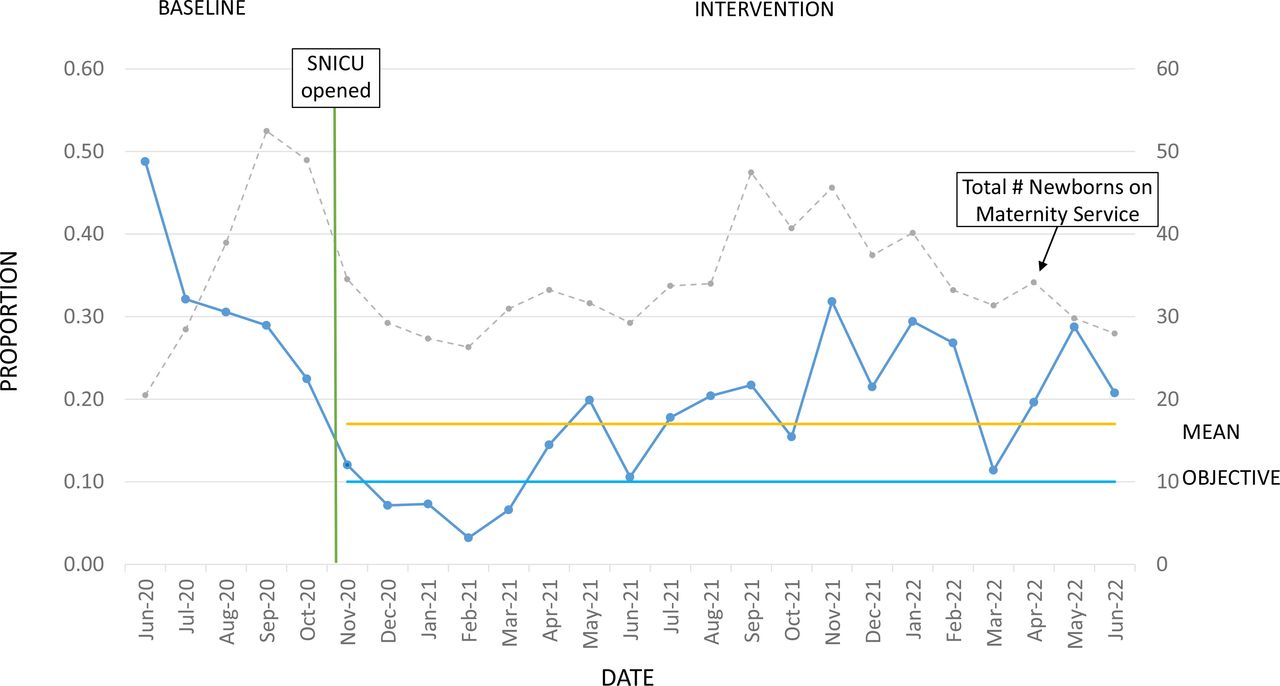
The aim of the Maternity Task force was to reduce overcrowding and improve the overall quality of care on the maternity ward by (1) having zero mothers and newborns on the ground in the ward (figure 2) and (2) to reduce the numbers of sick neonates receiving paediatric care on the maternity ward (figure 3).

Run chart of postpartum women on the floor in labour and delivery service 2020–2022; green line indicating the opening of the physiological postpartum unit.
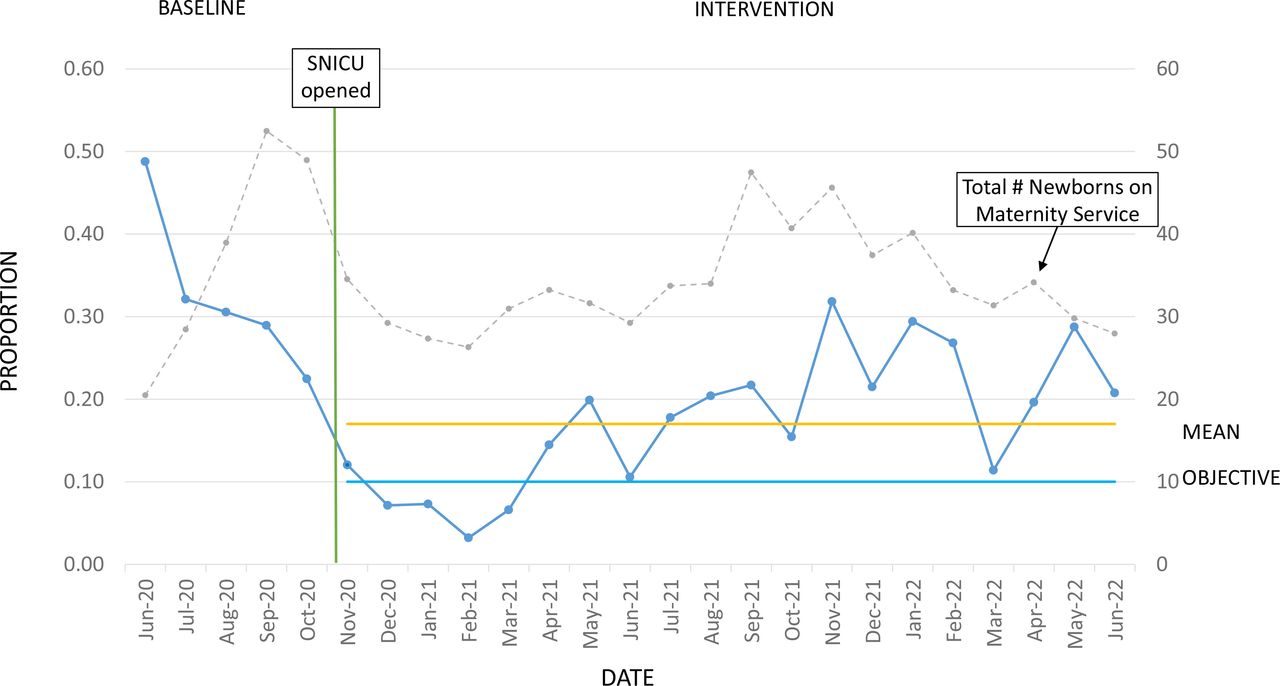
Run chart of neonates on maternity services receiving paediatric care 2020–2022; green line indicating opening of the SNICU; grey line indicating total number of newborns on the maternity service. SNICU, step-down neonatal ICU.
Methods
Context
HUM is a 300-bed partners in health -supported tertiary care facility. It has a large maternity service that encompasses one-third of the campus, including outpatient OB and GYN services, ~60 inpatient beds with surge capacity on antenatal, gynaecological and postpartum wards, a woman’s health emergency ward and ~30 beds on L&D. Over 500 deliveries occur every month, many of which are high-risk referrals made to the institution. The 16-bed NICU is located within the maternity block, facilitating easy referrals for premature and sick newborns.11 Haïti recorded its first COVID-19 cases in March 2020.12 Following urgent action to mobilise and provide isolation and treatment for the population affection, HUM, located in the Central Plateau Department of Haiti, was one of the first institutions selected in partnership with the Ministry of Health13 as having the capacity to provide the level of care necessary in a country that has a total of 124 Intensive Care Unit (ICU) bed nationally.14
Intervention
The Six-Sigma/ DMAIC quality improvement methodology (Define, Measure, Analyse, Improve and Control)15 was used in this project as the problem was urgent and centred around the process of patient flow in the institution. It also demanded rapid results given the urgency of the situation. As Six-Sigma DMAIC is defined by the Institute for Healthcare Improvement ‘speed and results are key ingredients to building Six Sigma momentum inside an organisation, and projects should be sized to assure team success and project closure inside reasonable time limits’,15 this approach was used to build on the motivation of the task force team while documenting and gathering data throughout.
The Maternity Task Force team was created by hospital leadership to address the urgent needs on the L&D unit regarding overcrowding and lack of NICU space. The team was composed of nurses and medical doctors from the maternity and paediatrics wards, in addition to non-medical personnel such as data collectors, and HUM quality improvement committee representatives.
Two urgent problems were identified by the Task Force; the indicators were clearly defined with fixed objectives set.
Postpartum women were laying on the floor in the labor and delivery unit.
Sick neonates were receiving paediatric care on maternity services.
The first of the teams’ quality improvement goals was to eliminate the number of postpartum women on L&D ward who did not have a bed and were laying directly on the floor with their newborns. An average of 14% of postpartum women who had given birth vaginally were boarding on the floor with their newborns before the intervention. The objective of this quality improvement Task Force was to reduce from 14% to 0%, the numbers of postpartum women on the floor between August and October 2020 (figure 2). It is an ethical and moral obligation to respect the dignity and the rights to provide good quality of care for these women and their newborns.
The second problem identified was the lack of space in the 16-bed NICU to ensure the management of all sick newborns needing care. An average of 33% of the total number of newborns on the services before the intervention, were sick and should have been cared for in the NICU. The second objective of the Task Force was to reduce the numbers of sick newborns receiving medical care on maternity services from 33% to less than 10% between August and October 2020 (figure 3). These newborns, including premature infants, stayed in the service with their mothers on post partum, L&D or sometimes the Antenatal ward, due to lack of bed space in NICU or paediatric wards where they would have received more appropriate care and less risk of exposure to nosocomial infections or SARS COVID-19 impacting neonatal mortality.6 10
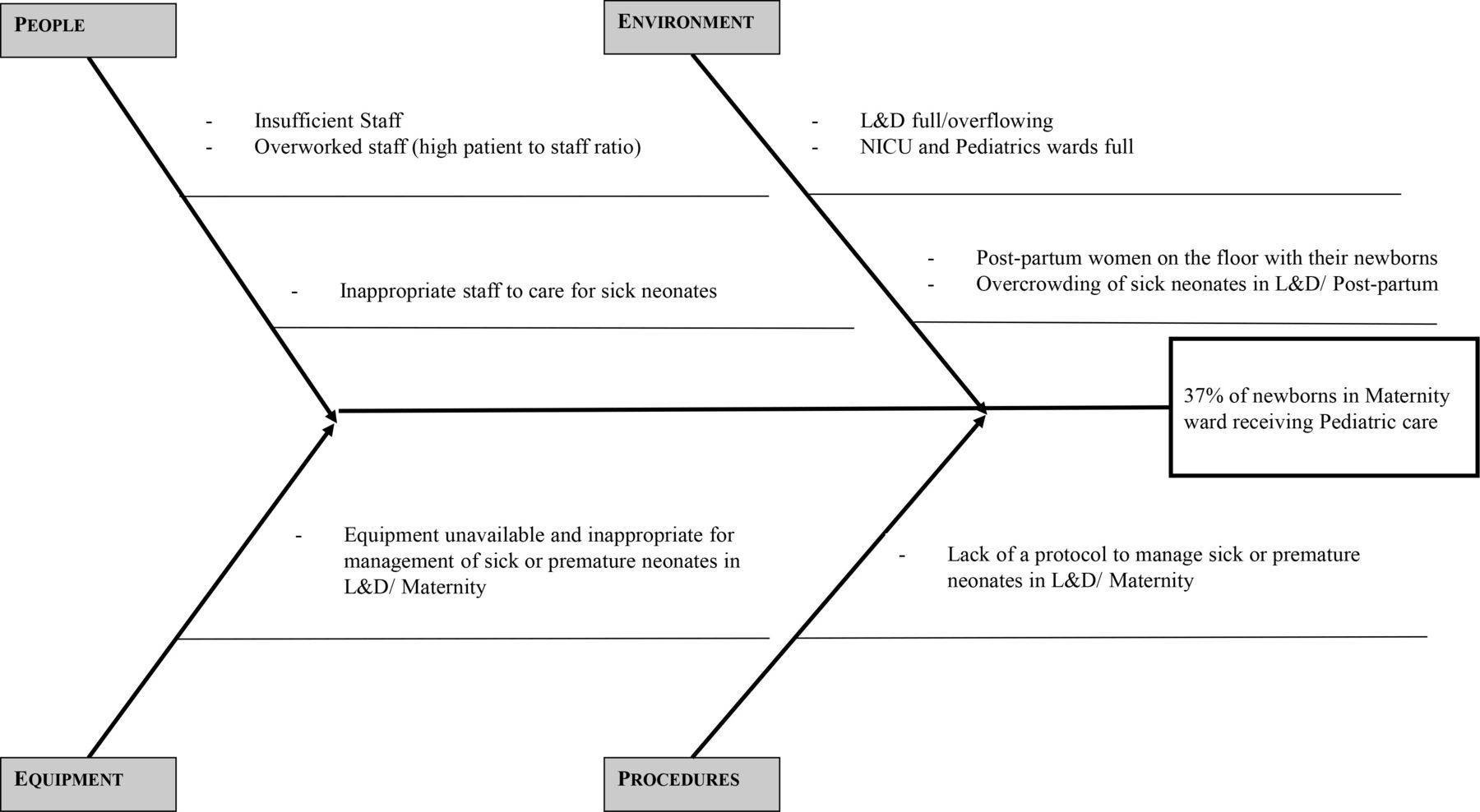
Reflective of our baseline data, the Maternity Task Force team identified and isolated the primary causes of the two indicator using a qualitative approach. Process flow charts (figures 4 and 5) as well as Ishikawa diagrams (figures 6 and 7) were used to analyse the causes contributing to the problems identified. These tools allowed the team to better identify and target significant causes in order to focus on the most important causes that contributed to the resulting improvement.

Flow chart diagram 1 mothers on the floor in L&D. L&D, labour and delivery.

Flow chart diagram 2 neonates receiving paediatric care on maternity services.

Ishikawa diagram 1 mothers on the floor in L&D. L&D, labour and delivery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ishikawa diagram 2 neonates receiving paediatric care on maternity services.
The Ishikawa, or cause and effect diagram, was used to help identify and analyse the root causes that contributed to the problems. Using the Ishikawa diagram for the first indicator, postpartum women lacking a bed, it was found that two of the primary contributory causes were environmental issues: lack of space on L&D, and a lack of bed turnover on this unit. Root causes identified under ‘people’, included a lack of nursing staff.
The process flow charts can be seen in figures 4 and 5. The flow chart in figure 4 for postpartum women prior to the start of the project ‘preintervention’ highlights the lack of bed space available on L&D for a newly postpartum woman. If no empty bed was available, she and her newborn stayed on the floor.
The flow chart in figure 5 for paediatric patients on maternity highlights the lack of bed space available in the NICU and paediatric wards in the ‘preintervention’ diagram. In this case, the premature and sick newborns stayed with their mothers and occupied beds for weeks at a time on the L&D service that necessitates a rapid bed turnover following normal uncomplicated deliveries.
The medical treatment for many of the premature and sick neonates lasts weeks to months, during which time they complete intravenous antibiotic and other medical treatment courses. This also increases the bed occupancy rate in the maternity service. After the mothers are discharged from hospitalised postpartum care, they continue to stay on the maternity unit with their sick neonates, which contributes to a backup of patients. Newly postpartum women consequently have to sleep on the floor therefore increasing the risk for nosocomial infections, overwhelming staff and thus compromising the quality of patient care and potentially clinical outcomes. It is important to note that the staff on L&D and postpartum are not trained in intensive neonatal care and are frequently overwhelmed with deliveries, postoperative mothers or mothers with severe pre-eclampsia/ eclampsia or other pathologies that merit intensive intrapartum and postpartum nursing care. Overcrowding in hospitals can severely impact inpatient mortality and clinical outcomes as mentioned previously.2 3
Measurements
For the first indicator, the number of postpartum women who did not have a bed (the numerator) was compared with the total number of postpartum women who delivered vaginally, in the maternity service (the denominator). The baseline for this first indicator (figure 2) was measured from June through August 2020 and showed an average of 14% of postpartum women admitted to the L&D ward following a vaginal delivery, did not have a bed. The objective of this first indicator was to have zero women sleeping on the floor in the HUM maternity service, between August and October 2020.
For the second indicator, sick newborns receiving paediatric care on maternity services, the numbers of sick newborns receiving paediatric treatment who stayed on the Maternity ward (the numerator), was compared with the total number of newborns in all of the maternity wards (denominator). The baseline for the second indicator (figure 3) was measured from June to August 2020 and revealed an average of 33% of newborns on the maternity ward were receiving paediatric care. The objective for this second indicator was to have less than 10% of the newborns admitted to the maternity ward, receiving paediatric treatment between August and October of 2020
Data collection methodology was carried out through the direct entry of data into an excel spreadsheet gathered from daily ‘What’sApp’ messages shared from nurse managers from L&D, postpartum and paediatrics wards, every work-day, not including holidays or weekends. This amounted to a total of 489 days over 2 years from 29 June 2020 to 30 June 2022. The data were verified and found after analysis that 94.5% of the data was complete for the time period evaluated. The data are gathered directly from nurse managers on the wards who pass through the services and personally verify several other indicators also shared on a daily basis including staffing ratios and critical patients, which is all shared electronically with hospital leadership every morning.
As part of the intervention to remove postpartum women and their newborns from the floor of L&D, a new ward of 17 beds with optimal resources was opened in mid-September 2020 ‘physiological post partum’ (PPP), which meant that the postpartum nurse manager began reporting data on this new service.
As part of the intervention to reduce the numbers of sick neonates on Labour & L&D and postpartum wards, a new ward of 16 beds with optimal resources was opened in mid-October 2020, step-down neonatal ICU (SNICU) and the paediatric nurse manager began reporting data on this new service.
Additionally, the numbers of deliveries per month was gathered from the monthly HUM ‘Reproductive Health’ report16–18 and can be seen in figure 1 to give perspective regarding the annual peak delivery periods.
Analysis
The tool used to analyse the data was in the form of a run chart (figures 2 and 3). The run chart helps us to visualise the shifts or trends in the data over time.
This was not a research study, so other statistical tests to understand the variations in the data were not applied. The run charts are simply describing the variations in the results but the team did not measure whether the results were statistically significant.
Results
The run chart of the postpartum mothers in figure 2 shows all data remained stable at zero (0) following the intervention, which was the objective of this indicator. On the other hand, the run chart of the data on the sick neonates in figure 3 did not show any particular trend aside from two runs, the first, below the mean at the opening of the SNICU and the second above the mean, during the peak delivery period in 2021. We hypothesise that the peak in sick neonates in May 2022 can possibly be attributed to a peak in nosocomial infections in April and May 2022 in the NICU (data not included in this manuscript) leading to the deep cleaning of this unit, as one potential cause for the increase in sick newborns on the maternity services.
The objective of this second indicator (figure 3) was to have less than 10% of sick neonates receiving paediatric care on the maternity service. The run chart shows the mean at 0.17, slightly higher than the 0.10 objective as outlined on the diagram. The total number of newborns on the maternity services as plotted in light-grey dashes on a secondary axis in figure 3, and total deliveries in figure 1, both indicating the annual peak delivery periods from September to November. The variations observed as increases in sick neonates receiving treatment on maternity services is generally proportional to the total number of newborns on the units.
The Maternity Task force focused on finding solutions to the root causes identified. For the first intervention, hospital leadership took the decision to open the new ward PPP, on the 15 September 2020 with 17 beds. The results showed zero postpartum women laying on the floor in L&D, with their newborns (figure 2). An average of 14% of postpartum women admitted to the L&D ward, did not have a bed during the baseline evaluation and 0% of postpartum women were on the ground postintervention. The objective of this first indicator was to have zero women sleeping on the floor in the HUM maternity service.
For the second intervention, hospital leadership opened the ‘SNICU’ ward, on the 19 October 2020 with 12 incubators or bassinettes, the results showed an average of 17% of newborns on the maternity services were receiving paediatric care (figure 3). There was an observed reduction from an average of 33% baseline, to 17% of newborns on the maternity ward under paediatric care, postintervention, the team did not achieve its objective for this second indicator. The goal was to have less than 10% of newborns admitted to the Maternity ward, receiving paediatric treatment.
The improved flow chart for postpartum women in figure 4. ‘Postintervention’ includes the resolution addressing the lack of beds: the opening of PPP Ward, specifically for women who had vaginal deliveries. The improved flow chart for paediatric patients in figure 5. ‘Postintervention’ includes the opening of the SNICU for sick newborns who did not need as intensive care as the NICU but who merited hospitalisation for continued medical care and treatment.
The ‘control’ phase of DMAIC reinforced the changes made during the improvement phase and ensured that the changes are sustainable. Data were gathered and analysed over a total of 24 months: June 2020–June 2022. As described in both the improved flow charts and run charts for both of the indicators identified, the opening of new hospital wards partially or completely resolved the problems identified. With these new wards and staff identified to work on the units, postpartum women are no longer laying on the ground on L&D at HUM over 24 months postintervention and more sick newborns are receiving an appropriate level of care in the SNICU services with equipment, staff and medications suitable for meeting these high-risk patients’ needs. The data demonstrate the sustainability of the changes postintervention for the first indicator. Although the objective of the second indicator was not met, an improvement was observed.
Discussion
Prior to the start of this project, many ineffective interventions had been attempted including: trying to send patients home earlier, transfer of stable patients to another facility, and strict bed management. However, with so many patients on the floor, these interventions were not effective and were determined to be potentially dangerous. It was critical to find an efficient way to address this issue. The opening of new hospital wards is generally not an option when an institution in under-resourced settings is faced with overcrowding and high bed-occupancy rates with little turnover. Better bed management and patient flow would have been more ideal; however, lengthy hospitalisations for sick or premature neonates admitted onto the NICU can last for weeks or months depending on level of prematurity and complexity of the pathology which impacts admission rates from other services and consequently low bed turnover rates as explained above.
Summary
Statement of principal findings
An average of 14% of postpartum women at HUM did not have a bed preintervention; 0% of postpartum women were on the ground post intervention, this objective of this indicator was met. An average of 33% of newborns on the maternity ward were sick preintervention compared with 17% postintervention. The team did not achieve its objective for the second indicator, which was to have less than 10% of newborns on the maternity ward receiving paediatric treatment.
Interpretation within the context of the wider literature
Studies have shown that the frequency and outcomes of infection-related maternal deaths in LMICs accounted for more than half of the intrahospital maternal deaths.5 Additionally, long waiting times and overcrowding increases dissatisfaction with maternity care.19 And increasing staffing workload increased the likelihood of negative patient outcomes including near-miss events.20 Similarly, WHO and UNICEF both noted that understaffing and overwhelming workload may lead to providers compromising both health workers and patient safety.21–23 Removing postpartum women from the floor of an overcrowded tertiary referral L&D ward, in addition to housing sick and fragile neonates in appropriate wards will hopefully have the cascading effect in our setting of reducing workload for staff in very busy services providing care to high-risk labouring, delivering and postpartum women and their newborns. This can contribute to the reduction in negative outcomes and to an increase in satisfaction in the care received by patients.
Implications for policy, practice and research
This project has shown that demands on hospitals in poorly resourced settings to deliver high quality and equitable access to care as is crucial, especially where the health system is weak, resulting in overcrowded wards. Planning for expansion and growth is important to satisfy the needs in under-resourced settings. Budget availability, equipment and human resources are challenges but essential to addressing these problems, and therefore, to avoid morbidity, mortality including exposure to nosocomial infections. Further research is needed to examine the correlation between maternal and neonatal mortality resulting from overcrowding and nosocomial infections.24
Strengths and limitations
To our knowledge, this is the first reported quality improvement project on this issue in Haiti. The commitment and engagement of the hospital leadership proved critical to the success of this project. One of the strengths of the project was the financial support for the opening of the two new wards that was addressed by the executive team to allocate the necessary support. Across the pillars of staff, stuff, space and systems that have been shown to strengthen health services delivery24; staff, stuff and space were the primary budgetary constraints. The additional space and staff were identified from other wards and materials were allocated for the opening of the 17 bed and 12 bed units for which funds were reallocated from another project to prioritise mothers and newborns.
Limitations
HUM is a tertiary referral hospital; a long-term objective is to decentralise patients to peripheral sites consequently reducing overcrowding overall including on other wards in the hospital, however, the sociopolitical situation in the country persists and the influx of patients to the hospital cannot be controlled.
Neonatal length of stay and nosocomial infections among neonates were not tracked as part of this project, however, this merits further investigation and another study since hypothetically nosocomial infections among neonates at HUM seems to be contributing to sick newborns remaining on maternity wards. As mentioned in the results, we hypothesise that a peak in nosocomial infections in April and May 2022 in the NICU, potentially caused more sick newborns to stay on the maternity ward as seen in figure 3.
The objective of this quality improvement project was to target and resolve the causes of overcrowding on the maternity ward. This intersected with the provision of services for ill and vulnerable neonates who should be in more appropriate wards, and the potential reduction in infections that comes with the opening of a controlled ward (SNICU) for these newborns. Other future studies could examine factors impacting neonatal length of stay, overflow of the NICU and the cascade of factors including risk of nosocomial infections among vulnerable neonates not on the correct ward exposed to multiple people in a non-controlled ward.25 In addition to incorrect wards, the point of origin of the neonate who was later admitted into the NICU (from postpartum, L&D or the operating room) can also hypothetically impact the risk of infections.
Lastly, the team recognises the need to further examine whether more women are coming from outside the catchment area to deliver at the hospital as a consequence of the sociopolitical climate in the region. This project cannot be generalised to other services and systems because the data on insecurity and where patients were coming from was not available. It was additionally discovered that an extreme gas crisis coincided with two peak periods that also reflected in increases in sick neonates on the maternity services (figure 3) in October/November 2021 and May 2022 and resulted in patients not able to leave the hospital due to lack of transport from this gas shortage.
Conclusion
To answer the overcrowding problem in the maternity ward, after several ineffective interventions from the OBGYN staff, the hospital leadership took the vital decision to form a multidisciplinary team ‘Maternity Task Force’ composed of motivated and dedicated personnel. The team analysed the causes of the problem and implemented changes, which consequently led to a sustainable and positive impact on the lives of our patients: mothers and newborns. We have learnt that planning for infrastructure, human resources, biomedical equipment, protocols and procedures, and social support are all essential to address the issues; and the implication of the institution leadership in the quality improvement of care is critical.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This was a Quality Improvement project carried out by hospital leadership, which was approved by the institution’s Quality Improvement Committee. There was no conflict of interest on the part of the Maternity Task Force team.
Acknowledgments
The authors would like to recognise the other members of the Maternity Task force, who significantly contributed to the success of this project: Dr. Jean Louis Romain, Miss Abdonie Laguerre, Miss Rose Myriam Beauvil and Miss Junie Severin.
Footnotes
Twitter @Jimdameus
Contributors MR proposed and supervised the project, MCJ-B analysed the data and wrote the main content in the report and is guarantor for the finished work. CM, OS and MJ provided main content and edits. KJRD facilitated the project and provided edits to main content. TMJ and JGF provided edits to content. All authors read and approved the final report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.