Article Text

Abstract
The current electronic laboratory order set at Epsom and St Helier University Hospitals NHS Trust for suspected pre-eclampsia includes a full blood count, urea and electrolytes, liver function, gamma-glutamyltransferase and uric acid. Local and national guidelines do not recommend the use of gamma-glutamyltransferase or uric acid for the investigation or monitoring of pre-eclampsia, as they are poor predictors of maternal and neonatal outcomes. We aimed to remove the automatic inclusion of gamma-glutamyltransferase and uric acid from the electronic laboratory order set for suspected pre-eclampsia. Stakeholders were approached to gain an understanding of whether gamma-glutamyltransferase and uric acid were being used in the clinical assessment of suspected pre-eclampsia. Obstetric consultants and maternity staff confirmed that they do not use uric acid in their clinical assessment, despite the laboratory phoning with abnormal results. In addition, an isolated gamma-glutamyltransferase rise is of no particular significance and is not part of the National Institute for Health and Care Excellence (NICE) diagnostic criteria for pre-eclampsia. The baseline number of gamma-glutamyltransferase and uric acid requests from the maternity department was identified over 2 months. The hospital information technology service was then asked to remove gamma-glutamyltransferase and uric acid from the electronic laboratory order set. The number of gamma-glutamyltransferase and uric acid requests from the maternity department following the intervention was identified over 2 months. A significant reduction in both gamma-glutamyltransferase and uric acid requests were noted. In addition, the midwives within the maternity assessment unit noted a significant reduction in phone calls from the laboratory to escalate abnormal blood results. This has saved the trust money and reduced staff time answering phone calls regarding abnormal blood results. A repeat assessment at 8 months following the removal of gamma-glutamyltransferase and uric acid demonstrated sustainability of the project.
- electronic health records
- obstetrics and gynaecology
- healthcare quality improvement
- information technology
- cost-effectiveness
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- electronic health records
- obstetrics and gynaecology
- healthcare quality improvement
- information technology
- cost-effectiveness
Problem
Epsom and St Helier University Hospitals NHS Trust consists of two busy general hospitals: Epsom hospital and St. Helier hospital, serving the South West London and North East Surrey population. The maternity service delivers roughly 5000 babies each year.
Both hospitals have a midwife-led MaternityAssessmentUnit (MAU) for monitoring a variety of conditions in pregnancy such as high blood pressure (and suspected pre-eclampsia), suspected rupture of membranes, reduced fetal movements and itching. The MAU at St. Helier hospital is a walk-in service for women who are at least 20 weeks pregnant and have either been referred by a health professional or have a concern themselves regarding their pregnancy. It is open from Monday to Friday from 8:30 to 16:30. The MAU at Epsom hospital is by appointment only and is open from Monday to Friday from 8:00 to 18:00. Out of hours, patients are reviewed in the triage area on the labour wards of Epsom and St. Helier hospitals.
Women attending with high blood pressure and/or symptoms of pre-eclampsia should have a focused history and clinical examination, a full set of observations taken and blood tests to rule out any organ dysfunction. The current electronic laboratory order set at Epsom and St Helier University Hospitals NHS Trust for suspected pre-eclampsia includes a full blood count, urea and electrolytes, liver function, gamma-glutamyltransferase and uric acid. The National Institute for Health and Care Excellence (NICE) guidelines for the diagnosis and management of hypertension in pregnancy1 do not recommend the use of gamma-glutamyltransferase or uric acid for the investigation or monitoring of pre-eclampsia, as they are poor predictors of maternal and neonatal outcomes. Gamma-glutamyltransferase and uric acid are also not included in the local trust guideline.2 A quality improvement project was developed to rationalise the blood tests requested in suspected pre-eclampsia by removing the automatic inclusion of gamma-glutamyltransferase and uric acid from the electronic laboratory order set.
Background
Hypertensive disorders of pregnancy complicate around 10% of pregnancies. Pre-eclampsia is defined by new onset of hypertension (>140 mm Hg systolic or >90 mm Hg diastolic) after 20 weeks of pregnancy and the presence of new-onset proteinuria (urine protein:creatine ratio (uPCR) of >30 mg/mmol).1 Symptoms include: severe headache, visual disturbances, severe pain below the ribs, vomiting and sudden oedema of the face, hands and feet. Blood pressure measurement and urinalysis for protein should be carried out at each antenatal appointment to screen for pre-eclampsia.3 When pre-eclampsia is suspected, patients should be assessed in secondary care by a healthcare professional trained in the management of hypertensive disorders of pregnancy. Blood tests including full blood count, urea and electrolytes and liver function, as well as quantification of proteinuria using uPCR should be performed.
National1 and local2 guidelines do not recommend the measurement of gamma-glutamyltransferase or uric acid, but they are part of the hospital’s electronic laboratory order set for suspected pre-eclampsia. This electronic laboratory order set is used by the healthcare staff within the MAUs and labour wards, instead of searching for the blood tests individually. The order set can be accessed by typing ‘PET’ into the search bar of the hospital electronic patient information system. A survey of healthcare staff at St. Helier hospital demonstrated that out of 35 midwives and 12 doctors questioned, 100% use the electronic laboratory order set in suspected pre-eclampsia.
South West London Pathology, the integrated pathology service provider for the region, confirmed the price for the measurement of serum gamma-glutamyltransferase and serum uric acid was £1.67 and £1.68, respectively.
Measurement
The number of requests for gamma-glutamyltransferase and uric acid within the maternity department were used as a measure within the quality improvement project. The maternity departments consisted of both MAU and labour wards at Epsom and St. Helier hospitals. The patients were all pregnant or postpartum women.
The hospital electronic patient information system (iSoft Clinical Management; iCM) was used to identify requests for gamma-glutamyltransferase and uric acid from the maternity department. This was accessed by the clinical nurse analyst.
Baseline measurements identified 155 gamma-glutamyltransferase requests within the maternity departments in November 2020 and 228 in December 2020. There were also 115 uric acid requests in November 2020 and 149 in December 2020.
It was predicted that following the removal of gamma-glutamyltransferase and uric acid from the electronic laboratory order set, there would be a significant reduction in these requests. The high level of requests for these two blood tests is likely due to their automatic inclusion within the electronic laboratory order set for suspected pre-eclampsia and not because a healthcare professional deemed them necessary. No effect on clinical care or the rate of diagnosis of pre-eclampsia was expected.
Design
The project team was made up of an obstetric registrar, obstetric consultant, MAU midwife and clinical nurse analyst.
Stakeholders were approached to gain an understanding of whether gamma-glutamyltransferase and uric acid were being used in the clinical assessment of suspected pre-eclampsia. The proposal to remove gamma-glutamyltransferase and uric acid from the electronic laboratory order set was approved in the monthly consultant meeting and the women’s health quality meeting. The quality improvement project was also registered and approved by the Epsom and St. Helier quality division, clinical audit and effectiveness manager and the directorate quality lead.
It was expected that the number of uric acid requests from the maternity department would significantly reduce, as there are no other conditions where uric acid would be routinely measured. A moderate reduction in the number of gamma-glutamyltransferase requests was expected due to it being used in the investigation of other obstetric and non-obstetric conditions.
Strategy
Once the baseline number of gamma-glutamyltransferase and uric acid requests from the maternity department was identified, the intervention was implemented. The Epsom and St. Helier Hospitals information technology service were asked to remove gamma-glutamyltransferase and uric acid from the electronic laboratory order set for suspected pre-eclampsia.
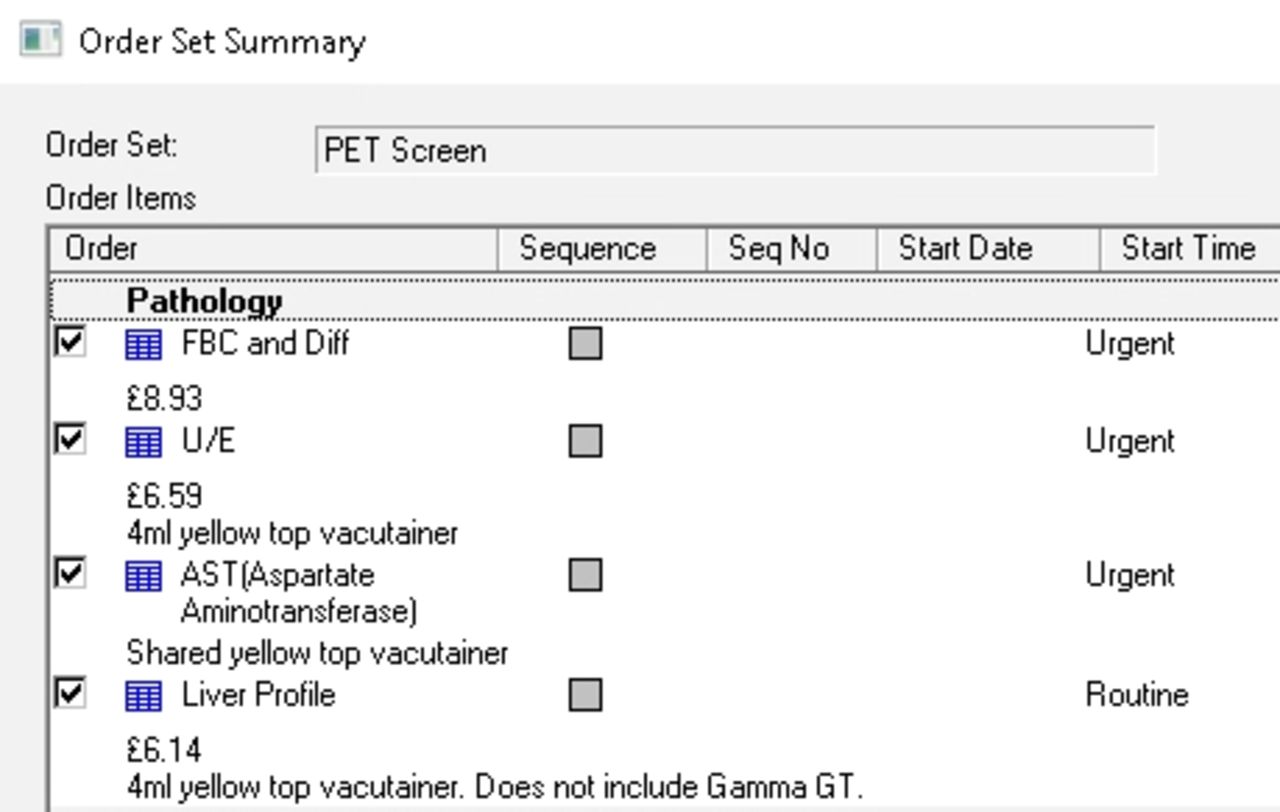
The electronic laboratory order set was amended in January 2021 (figure 1) by the clinical nurse analyst. An email was sent to the maternity department informing all staff of the change to the electronic laboratory order set.
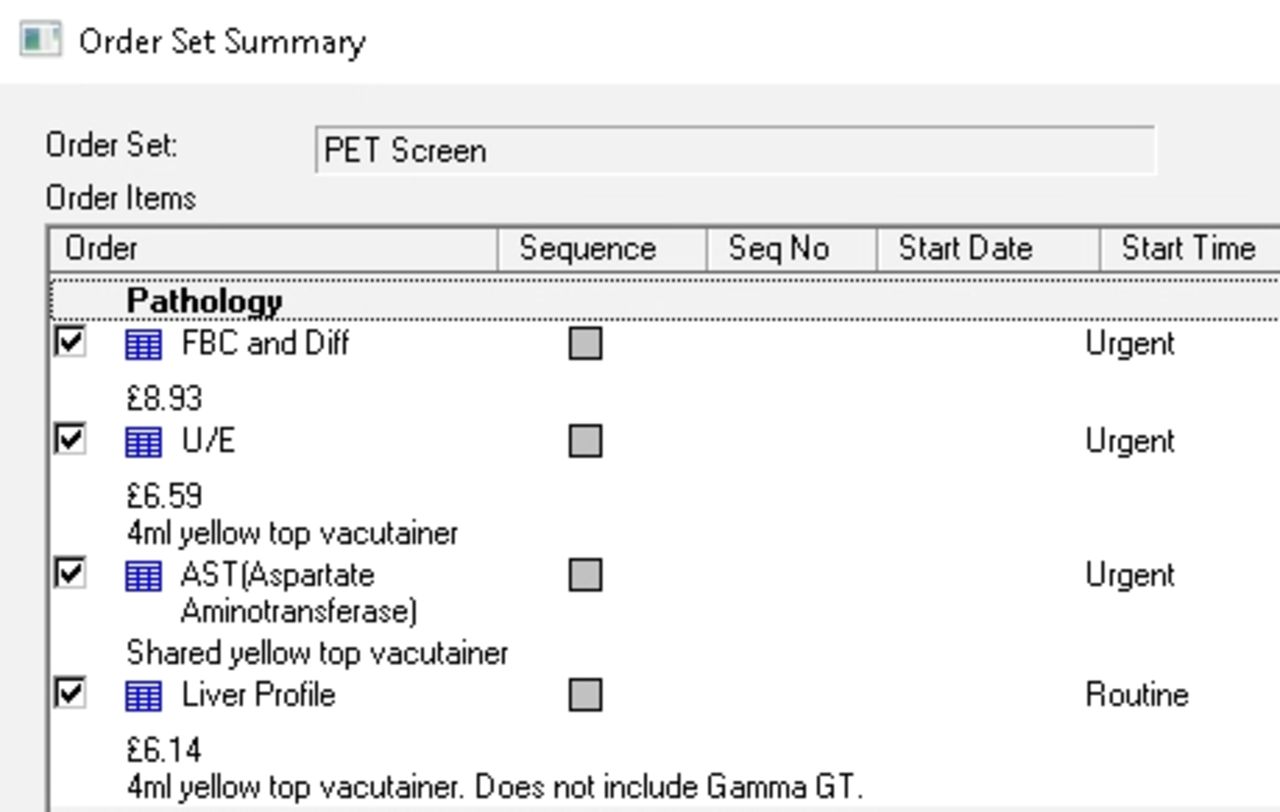
The amended electronic laboratory order set.
The number of gamma-glutamyltransferase and uric acid requests from the maternity department in February and March 2021 (following the intervention) were identified.
A third data collection occurred 8 months following the intervention to assess for sustainability of the project.
Results
Obstetric consultants and MAU staff confirmed that they do not use uric acid in their clinical assessment, despite the laboratory phoning the MAU with abnormal results. An isolated rise in serum gamma-glutamyltransferase, without other liver function derangements, was noted to be of limited value and not part of the diagnostic criteria for pre-eclampsia.
The number of gamma-glutamyltransferase and uric acid requests at baseline and following the removal of their inclusion in the electronic laboratory order set can be seen in table 1 and figure 2.

{kind=link}
{kind=link}
Run chart showing gamma-glutamyltransferase and uric acid requests over time.
Number and laboratory costs of gamma-glutamyltransferase and uric acid requests before and after the intervention
There were 155 gamma-glutamyltransferase requests within maternity in November 2020 and 228 in December 2020. Following the amendment of the electronic laboratory order set, there were 69 gamma-glutamyltransferase requests in February 2021 and 85 requests in March 2021. Gamma-glutamyltransferase is used in the investigation and monitoring of other obstetric and non-obstetric conditions, and therefore it was not expected that this level will reduce much further.
There were 115 uric acid requests within maternity department in November 2020 and 149 in December 2020. Following the amendment of the electronic laboratory order set, there were six uric acid requests in February 2021 and three requests in March 2021. Four of these requests were made by the same junior doctor. The other uric acid requests were made by a small number of midwives at Epsom hospital. It is expected that the number of uric acid requests will remain low as there are no other conditions in pregnancy where uric acid is routinely measured.
In addition, the midwives within the MAU noted a significant reduction in phone calls from the laboratory to escalate abnormal blood results.
The quality improvement project and results were presented at the Epsom and St. Helier’s Women’s Health Quality Meeting and at the Royal College of Obstetrics and Gynaecology World Congress 2021 as an iPoster.4
A third data collection was performed in August 2021, 8 months after the intervention, to assess sustainability of the project. There were 62 gamma-glutamyltransferase and 6 uric acid requests. All uric acid requests were by three midwives at Epsom hospital. The midwifery matron at Epsom has been informed to improve compliance.
The cost of gamma-glutamyltransferase and uric acid measurements in November and December 2020 was £452.05 and £631.08, respectively. After the amendment of the electronic laboratory order set, the cost of gamma-glutamyltransferase and uric acid measurements in February and March 2021 was £125.31 and £146.99, respectively. The cost at the third measurement in August 2021 was £113.62. Table 1 details the number and cost of each request.
Conclusion
Gamma-glutamyltransferase and uric acid are not part of the national or local guidelines for the investigation and monitoring of pre-eclampsia. Gamma-glutamyltransferase and uric acid have been successfully removed from the electronic laboratory order set for suspected pre-eclampsia. This has resulted in a cost saving for the trust and reduced the time staff spend answering phone calls regarding abnormal blood results.
The majority of healthcare professionals sampled in the study frequently used the electronic laboratory order set to request investigations. We believe the intervention is sustainable due to changes made within the coding of the electronic laboratory order set. Only administrators that manage the electronic laboratory order sets are able to reverse this intervention, which prevents accidental inclusion of inappropriate blood tests. This has been evidenced by finding a sustained improvement 8 months following the intervention.
We encourage other hospitals to review their electronic laboratory order set for suspected pre-eclampsia and consider rationalising the blood tests included. By doing so, it not only reduces waste within the National Health Service (NHS) but also can lead to cost savings.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Footnotes
Contributors ADJ proposed the project, analysed the data and wrote the report. MC collated survey data from midwifery staff and supported data analysis. SD amended the electronic order set and extracted the blood test request data. AJ supervised and approved the project, and is the guarantor for the overall content. All authors read and approved the final report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.