Article Text

Abstract
Starting in a new hospital can be an overwhelming experience for any grade of doctor. There is a vast amount of information that needs to be learnt immediately to function in the new environment. There is an annual changeover of doctors between hospitals in August nationwide and most junior doctors rotate specialties every 4–6 months. Evidence shows that doctors feel this transition has a negative impact on patient care and indicates that inpatient mortality rises during the August changeover. In our hospital, we noted problems with access to guidelines, referral information and investigations by junior doctors, especially at changeover. In an initial questionnaire, 100% of doctors had experienced difficulties with referring to a specialty and 96% felt time was wasted doing so. Furthermore, 87.5% of doctors had difficulties with ordering laboratory investigations and 100% of survey participates expressed difficulty accessing guidelines.
To tackle this issue, we created guidelines on how to refer to different specialties, order investigations and general running of the hospital. We then used a free app platform called induction and uploaded the guidelines as well as formal hospital guidelines to the app. After use of the app, we assessed these problems via further questionnaires. Doctors reporting problems with finding how to refer to specialties reduced from 100% to 0% in the final survey. Problems finding how to request investigations fell from 100% to 14.3% after 1 month to 7.7% after 3 months. Finally, problems finding guidelines fell from 100% to 15.4%. Further, 100% of doctors felt the app saved time.
Use of the induction app to access guidelines saves time and reduces problems accessing information needed to carry out tasks. This an easily replicated project with low running costs which proved to help with the universal problems around induction to a new hospital environment.
- Information technology
- Mobile Applications
- Healthcare quality improvement
- Clinical practice guidelines
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
In the month of August, hospital wards throughout the UK welcome the arrival of new doctors, some of whom are new graduates. These doctors are expected to familiarise themselves with the hospital, their colleagues and the job itself almost immediately. There is often little continuity with the medical staff at this time of year as junior doctors change over on the same day. For new graduates especially, these tasks can be daunting in the first few months as there is a shift in responsibility from the role of a student to doctor. New graduates in the UK start in foundation year 1 (FY1) progressing after a year to foundation year 2 (FY2). They rotate through various hospital specialties every 4–6 months. They mostly work on the wards, dealing with ward-related tasks, for example, ordering investigations, making referrals to other specialities, prescribing and seeing unwell patients. Following FY2, they can choose to go into higher specialty training.
Starting in new hospital can be an overwhelming experience. The vast volume of hospital-specific information to be learnt is challenging and difficult to retain. There is a mandatory week of induction training prior to starting FY1. In our hospital, University Hospital Wishaw (UHW), this involves, getting a general overview of the hospital and how it runs, induction with information technology (IT) and training on specific programmes, as well as an introduction to your base ward. The current junior doctors typically give informal tips and advice to new doctors; this advice can be variable. Doctors more senior to FY1 have one short day of induction at the start of the year.
From working in our hospital as junior doctors, we, along with our colleagues, struggled with routine ward tasks due to a lack of knowledge on the systems within the hospital. These tasks included finding contact details and information on referring to other specialties and requesting investigations. UHW is a small district general hospital with 626 inpatient beds, and as a result, many specialties and radiological investigations are not on site. Some scans require a formal request and written confirmation in a book with ‘slots’, some are carried out in Glasgow hospitals and require a special request form which are only available from one or two secretaries in the hospital and some need specific preinvestigation preparation and workup. Finding out what services are available, where and how to access them took time. With regard to laboratory investigations, these are all written requests on paper forms. This creates problem, particularly with new junior doctors who are not familiar with blood requests, components of common blood screens and the various colours of blood bottles. A further issue was difficulty of access to clinical guidelines which were not easily located on the intranet. All these problems were worse at the start of the year and when doctors rotated specialties.
The aim of this project was to ease the transition of junior doctors into the hospital and rotating between specialties, to save time and improve access to local guidelines, referral and investigation information at UHW. We aimed to reduce the reported problems found by doctors and improve access to local guidelines, referral and investigation information by 50%. We aim for it to be used as an adjunct to the formal induction programme to facilitate an effective handover of information and improve patient care.
Background
The transition from a medical student to an FY1 is challenging. To ease the transition, in 2013 the Department of Health introduced a mandatory 4-hour shadowing period to all new FY1 doctors immediately prior to changeover. There is no set curriculum for the content of this induction and anecdotal evidence suggests there is variability in programmes across the UK.
Unfortunately, due to the nature of foundation training, rotating through various hospitals and specialties on a 4–6 monthly basis, the knowledge gained by the doctors over the course of their clinical rotation is lost at changeover. An electronic survey of doctors in the UK reported negative impact of the August transition, highlighting patient care and safety issues.1 The information given at induction can be overwhelming and difficult to retain. The learning and re-learning of often hospital-specific administrative-related tasks creates a significant challenge to working effectively and efficiently in a new and already stressful job. There is evidence to suggest that inpatient mortality increases during this changeover period.2
Ideas to improve this transition period and accessibility to guidance and information to doctors have made a positive impact. Junior doctors themselves are best placed to lead efforts to tackle this as they face these issues daily. Two projects that highlight this are a project with a junior doctor–led induction programme and a junior doctor–written induction booklet.3 4 Both these projects addressed issues with familiarity of the working environment. The induction programme project was criticised for being too long and we had concerns about the information overload in this approach from our anecdotal experience of induction programmes. Further projects have tackled specifically access to clinical guidance, with positive results.5–7 These projects showed there are universal problems with junior doctors accessing guidance throughout different healthboards. It also highlighted that junior doctors depend on guidelines and simple reorganisation onto one platform saves time to locating these. One of these projects was an app created by a junior doctor.7 While this is impressive, this is less replicable as not all doctors have skills to make an app. A project, one of our lead authors worked on, focused on referral information onto a frequently accessed intranet page.8 With this project, we aimed to tackle multiple problems on one platform. A project with similar aims was an electronic handbook for junior doctors located on an intranet webpage.9 This project achieved the goal of locating a large volume of information in one place but was hindered as the information was not portable. Similarly, the doctor toolbox compiles information into an app reported to save junior doctors 39 min a day. The subscription fee paid by the healthboard for this app is a major barrier which can be overcome by using free software such as the induction app.10
Measurement
Baseline data were collected through an online questionnaire which was sent out to all 48 junior doctors working within medicine. The questionnaire asked about difficulties experienced by junior doctors with regard to completing basic ward tasks such as referring to various specialties, requesting investigations and accessing local guidelines.
The results revealed that all 24 doctors who completed the survey experienced difficulties with referring to either a medical or surgical specialty and 96% felt time was wasted while making referrals. Meanwhile, 87.5% of doctors completing the survey had difficulties with laboratory investigations and 54% report difficulties with requesting investigations in general. Further, 100% of survey participants expressed difficulty accessing guidelines and 92% felt time was wasted doing so. Doctors reported that patient care was compromised due to wasted time. All doctors fed back that they felt a handbook containing key information for their new role in UHW would be useful resource. A free text box asked the participants what kind of information they would like to share in the document and some suggestions are given below:
An app-based version as books go missing easily.
A comprehensive list of all referrals.
Easier access to guidelines.
What to put in a liver/renal/myeloma screen and what tubes to go in/how many.
Contact numbers for seniors when on call.
Most participants highlighted the importance of the information being readily available and many suggested an app format. All survey responders had access to a smart phone but expressed difficulties with poor signal related to hospital Wi-Fi use.
Following the baseline questionnaire, it was clear that that there were three distinct problems which became our three outcome measures:
Difficulty finding out how to refer to a specialty.
Difficulty finding out how to order an investigation.
Difficulty finding hospital guidelines.
We aimed to see reported difficulties in these areas fall by 50%. We would reassess this in further questionnaires at 1 and 3 months.
Design
To address the issues, we identified with the online survey we used a platform called ‘Induction’ to share information and resources we acquired during our time as junior doctors in UHW. Induction is a free app online and to download on all smartphones with offline capabilities. The app was created by a UK company called ‘Induction Healthcare’ and is used by thousands of doctors and healthcare professionals worldwide. The app allows healthcare workers to create their own hospital version on the app. The existing version of the app for ‘Wishaw hospital’ contained only a directory which was not maintained and was infrequently used. There was no hospital document uploaded to the app; therefore, the app was underutilised in our hospital.
Our team involved an FY1 doctor, a core medical trainee doctor and a consultant overseeing the project. To gain access to uploading documents to the app, we had to liase with the induction team first. This is to ensure they could make the documents secure by changing the hospital version of the app to invite only. After liaising with the team at ‘Induction’, we were able to set up a UHW version of the app to upload and store hospital-specific information. We wrote guidance on ‘how to refer to a specialty,’ order investigations, laboratory tests and general running of the hospital. The ‘how to refer to a specialty’ document outlined the ways in which each medical and surgical specialty preferred to be contacted (both for inpatient and outpatient reviews), where to send the referral and typically how long you will wait on a reply. A clear and concise document highlighting the important aspects of requesting investigations and laboratory tests was created and uploaded onto the app. In addition to these self-made documents, local guidelines sourced from the UHW staffnet page were uploaded to a separate folder within the app and included the antibiotic protocol and hyperkalaemia guidelines for example. For online security, the app was invite only and first-time users would request access from us, as administrators of the app. After liaising with switchboard operators, we also gained access to hospital phone numbers and created a directory on the app. You can call the extension direct from your mobile app—again saving time and effort to find a telephone during time away from the ward. A screenshot of the app layout and orientation can be found in figure 1.

(A) Screenshot of induction app in action in the default home page. Documents can be accessed by clicking the icon in the top left corner in figure 1A. Figure 1B shows the documents page. Documents can also be accessed by clicking the book icon on the bottom of the screen. ACS, acute coronary syndrome; NBM, nil by mouth; TIA, transient ischaemic attack.
This is a sustainable project with limited associated costs which can be used throughout hospitals across the UK. To keep the information up to date, it was decided that the chief resident of UHW would take over the project at each changeover and become an administrator of the UHW version of the app. The information, documents and local guidelines are easily updateable by the administrator through use of the website. This ease of access makes this ‘handbook’ easy to maintain and thus a reliable source of information. The induction staff are very helpful and easy to contact.
Strategy
Four Plan-Do-Study-Act(PDSA) cycles were conducted over the period of 1 year.
PDSA cycle 1
Baseline data identified three problem areas: referring to specialties, requesting investigations and accessing guidelines. All survey participants agreed a ‘junior doctor style handbook’ would be useful. To tackle and reduce these problems, documents with guidance were created and uploaded onto a ‘locked’ UHW version of the ‘Induction’ app alongside some local guidelines. A directory that included contact numbers of various wards and doctors within the hospital was also updated.
PDSA cycle 2
This new UHW version of the app was trialled for 1 day among a small cohort of colleagues and received positive verbal feedback. The UHW version of the app was then launched at a medical postgraduate meeting. Invitations to use the app were sent out to all junior doctors working in the medicine department.
PDSA cycle 3
A follow-up anonymous survey was sent out via email to the junior doctors, 1 month after the launch. The survey comprised of 14 questions; 8 yes or no, 2 ‘chose from option of three’ and 4 free text-style question and answers. The content included grade of doctor, whether they had they heard about the app, whether they use it/how often they use it, what they use the app for and information on user satisfaction. It also asked, after use of the app, did they experience any problems with referrals to specialties, investigations or finding hospital guidance. There was a free text box for suggestions/comments. The results were positive with feedback highlighting the usefulness of the information and easy accessibility. It was highlighted that some phone numbers were incorrect and some guidelines were missing. Changes were therefore made as per the recommendations and the app was updated. The app was now being integrated as part of the medical induction.
PDSA cycle 4
A further follow-up survey was sent out 3 months after the launch of the ‘UHW version’ of the app. The survey was initially distributed via email link to medical doctors; however, to gain more responses, the questions were printed and distributed by hand to the medical wards and handed out at a teaching session. The results were collected over the next few days and remained anonymous. The survey contained the same questions as the previous survey. Alongside the survey, data from the induction website were analysed. The app was presented at the hospital ‘Quality Improvement Showcase.’ After feedback from the surgical department, the surgery induction booklet was added to the app and this is now presented as part of the induction to surgery. The hospital presentation increased awareness of the app and usage statistics showed steady increase.
Users can submit requests of information to be added to the administrators to ensure ongoing feedback and development. Statistics on the app usage can be readily assessed on the administration login page on the induction website, and this is viewed periodically by the current administer.
Results
After 1 month of the induction app going live, a second anonymous survey was sent as part of PDSA cycle 3, there was seven responses by doctors using the app. After 3 months, a third survey was sent out, there were 15 responses. The surveys were circulated on media and email as well as filled out at teaching. Both questionnaires were only completed by those who had used the app. Although the number of doctors signing up to the app was known, it could not be determined whether they used it or not. This likely limited the uptake of the questionnaire.
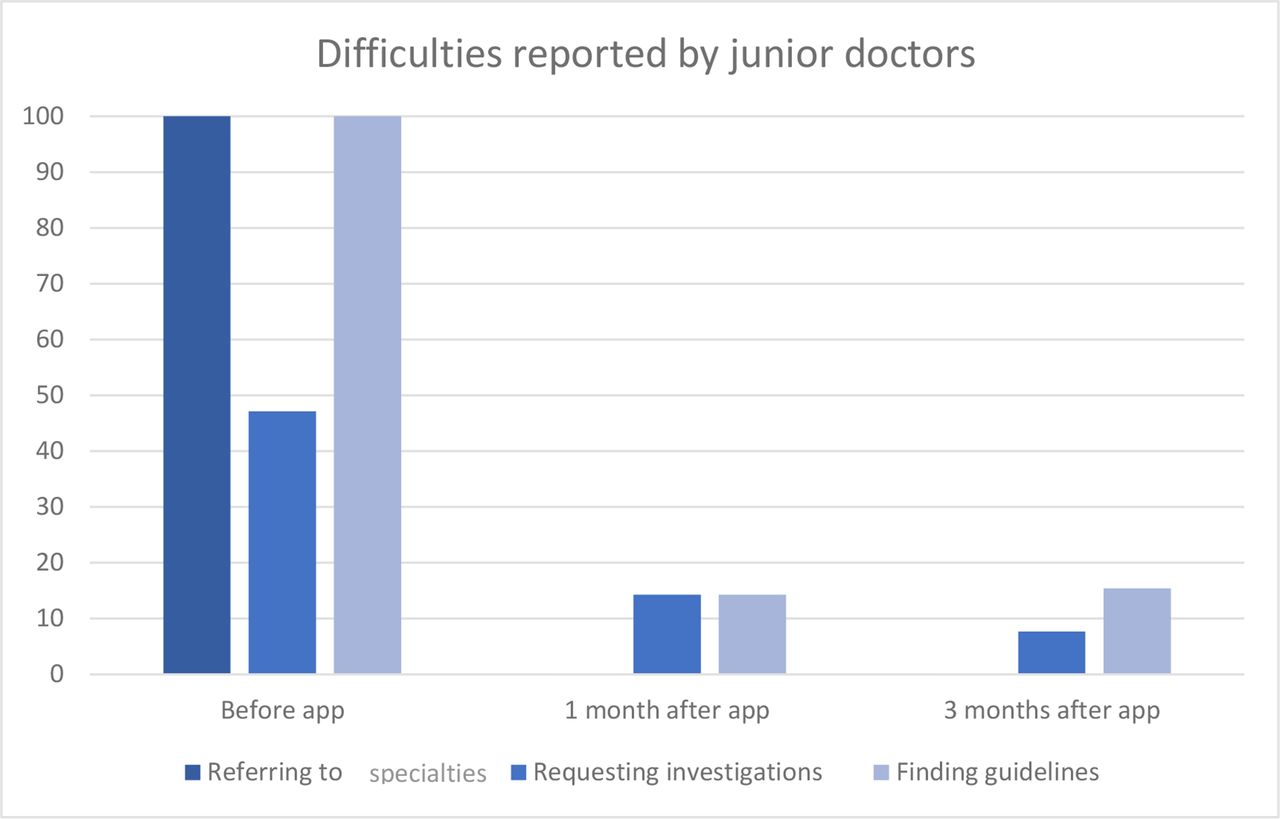
Figure 2 shows the decline in doctors reporting problems in three main problem areas after using the app. Doctors reporting problems with finding how to refer to specialties reduced from 100% in the first survey to 0% after 1 month and this was sustained at 3 months. Problems finding how to request investigations fell from 100% to 14.3% after 1 month and to 7.7% after 3 months. However, as only seven doctors completed the second survey, we cannot compare data directly to the 24 doctors who completed the first survey. On the other hand, we can see in the final survey of 15 doctors, there is a downward trend, supporting an improvement. Finally, reported problems finding guidelines fell from 100% to 15.4%.

{kind=link}
{kind=link}
Bar chart illustrating problems with referring, requesting investigations and finding guidelines as reported by junior doctors before using the app, 1 month after using and 3 months after using the app.
Doctors reporting the app as useful went from 87.5% at the first survey to 100% in the second survey; 100% of doctors felt the app saved time in the third survey. The vast majority using the app and completing the surveys are FY1 doctors. In the third survey, 69.2% of doctors use the app at least once a month, the remainder using it every month.
Data on the app usage were recorded via the induction website over the past year, as shown in table 1.
An overview and breakdown of app usage from Febuary 2019 to January 2020
Comparing the last 6 months to the first 6 months, there is increasing views on the app, especially of documents uploaded; 908 compared with just 493 initially. There is a key spike in app usage in August reflecting changeover time when the app was hypothesised to be most useful. The referral guidance is the most popular document viewed, this takes up 39% of all documents viewed and the investigations guidance is the second most popular.
Below are some of the free text comments from the third survey.
“Good information, easy to access.”
“Easy to use platform.”
“Very useful, please keep it going and keep updating it.”
“Great initiative and find the help with referrals and investigations so useful. Will be a great help with new starts in August – Fy1s in particular!!!”
“Great development, really helpful and can even call directly from phone to departments with ease.”
“Really useful to have all the information for referring to specialities in one place.”
Lessons and limitations
The project’s results from the surveys are limited by the lack of responses. Although still indicative of opinion, this makes data drawn from these less reliable. Doctors are inundated with survey requests and have limited time to fill them out. Teaching sessions allowed us to give out the survey; however, not all doctors were present. In future projects, taking opportunities like teaching sessions to ask for feedback to be filled proved most profitable. Fortunately, we could collect data on the use of the app by the app itself which showed that it as being used by many doctors reflecting its worth.
We had issues with raising awareness of the project initially, we tried via email, word of mouth and placing posters. The largest advantage was when the app was made part of the medicine induction which happens each 4-month rotation. Another issue was that it was not possible to delete the original ‘Wishaw Hospital’ app version which contained only a directory, which created confusion among users trying to sign up as there was two versions available.
The strength of this project is that it is applicable to every healthcare system, it is easy to replicate and it is free to use. There are universal issues with access to information needed by junior doctors as demonstrated in the Background section of this article. The app interface is easy to use, and documents are easy to upload. The induction staff are happy to help and, in our experience, very easily to contact via email and happy to share data with us. The app is secure and as an administrator you have control over who can view the app.
The app needs to continuously be updated with the latest guidelines. Our hospital medical director was keen to see the continuity of the app, so he entrusted the administration of the app to the role of the chief resident, every year. Our concern is whether the interest in maintenance of the app page may vary from chief resident to chief resident.
Conclusion
Overall, the results show that junior doctors feel the app has saved time and allows them quicker access to guidelines. We reduced problems finding referral information and ordering investigations and problems with access to guidelines. Satisfaction with the app was high. The ongoing usage of the app and the documents uploaded to it highlight how helpful it is and the sustainability of the project through time.
There are universal problems noted by junior doctors in the literature on the availability of information that is needed to perform tasks as a junior doctor. Due to the large scale of the problem encountered, there are several projects that have attempted to fix these issues. Our project is easily replicable and free to set up and use. You can use the app offline, on the go, and it negates the need to log into a computer. It can be accessed repeatedly so vast volumes of information do not need to be retained.
The project started in the medicine department but has spread to other departments. We now have incorporated the surgical induction booklet into the documents. We hope to soon include some other specific departments like obstetrics and gynaecology and paediatrics. Latterly, we hope to role this out to other hospitals in National Health Service (NHS) Lanarkshire.
Acknowledgments
Beth Keohane, Induction Healthcare, was extremely helpful with pulling data off the induction app for us to use. Thanks is due to Mr Hakim Ben Younes, Chief of medical services, University Hospital Wishaw, for showing support to our project and for helping to make it sustainable.
Footnotes
Contributors KC and JC contributed equally to writing of this paper and involvement of the project, we would like to be joint first authors. KC created documents of referral and investigations information for the app and created the surveys. JC approached the induction app team and set up the app for the hospital, uploaded guidelines and help create the surveys and obtained user data. MP was the supervisor of the project, contributed advice and gained hospital management support, and helped edit the final paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to this study are included in the article.