Article Text

Abstract
Introduction Physical inactivity and excessive sedentary behaviours are major preventable causes in both the development and the treatment of obesity and type 2 diabetes mellitus (T2DM). Nevertheless, current programmes struggle to engage and sustain physical activity (PA) of patients over long periods of time. To overcome these limitations, the Digital Intervention Promoting Physical Activity among Obese people randomised controlled trial (RCT) aims to evaluate the effectiveness of a group-based digital intervention grounded on gamification strategies, enhanced by social features and informed by the tenets of the self-determination theory and the social identity approach.
Methods and analysis This trial is a two-arm parallel RCT testing the effectiveness of the Kiplin digital intervention on obese and patients with T2DM in comparison to the usual supervised PA programme of the University Hospital of Clermont-Ferrand, France. A total of 50 patients will be randomised to one of the two interventions and will follow a 3-month programme with a 6-month follow-up postintervention. The primary outcome of the study is the daily step count change between the baseline assessment and the end of the intervention. Accelerometer data, self-reported PA, body composition and physical capacities will also be evaluated. To advance our understanding of complex interventions like gamified and group-based ones, we will explore several psychological mediators relative to motivation, enjoyment, in-group identification or perceived weight stigma. Finally, to assess a potential superior economic efficiency compared with the current treatment, we will conduct a cost–utility analysis between the two conditions. A mixed-model approach will be used to analyse the change in outcomes over time.
Ethics and dissemination The research protocol has been reviewed and approved by the Local Human Protection Committee (CPP Ile de France XI, No 21 004-65219). Results will inform the Kiplin app development, be published in scientific journals and disseminated in international conferences.
Trial registration number NCT04887077.
- behavior change
- cost-utility
- e-health
- gamification
- intervention
- mhealth
- mobile app
- obesity
- physical activity
- RCT
- T2DM
- weight stigma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- behavior change
- cost-utility
- e-health
- gamification
- intervention
- mhealth
- mobile app
- obesity
- physical activity
- RCT
- T2DM
- weight stigma
Strengths and limitations of this study
Randomised controlled trial comparing a digital gamified intervention targeting physical activity to another existing non-drug treatment.
Between-person and within-person level analyses of daily steps will provide insight on group differences and individual trajectories of behaviour change.
A 6-month follow-up will inform on the sustainability of the intervention effect.
The intervention involving multiple components, it will be difficult to affirm which component is involved in the efficacy of the intervention.
We will attempt to address this limitation by conducting in-depth mediation analyses, to identify the salient ingredients behind the effect.
Introduction
Overweight and obesity, which concern one in two adults in western countries,1 are among the most important health risk factors, and is associated with comorbidities such as type 2 diabetes mellitus (T2DM), which affects 5% of the French population under 65 years of age, and 15% of people over 65 years old. If the roots of obesity and T2DM are complex and multifactorial, physical inactivity and sedentary behaviours (SB) are both major factors in the development of these diseases.2–7
Positive effects of physical activity (PA) for these patients are recognised both at the scientific and institutional levels. Indeed, they can benefit from supervised PA programmes suited to their disease (ie, adapted PA, APA), which allow to improve functional capacity and muscle strength without having detrimental effects or complications on disease progression.8 However, these programmes can be difficult to access for patients, due to lack of availability on the scheduled sessions, lack of economic means or geographical distance.9 As a result, a limited adherence to PA at the end of these programmes is generally observed.10
Given that PA of obese and patients with T2DM remains very low,11–13 promoting their long-term PA participation is a major challenge for researchers, practitioners and the global healthcare economic system.14 A promising solution is to overcome the limitations of current face-to-face programmes, by developing digital interventions. In this vein, this study will evaluate the efficacy of a digital intervention in subjects with chronic diseases, by comparing it to the gold standard (supervised face-to-face PA).
e-health and gamification
Digital tools may provide effective, cost-effective, safe and scalable interventions to improve health and healthcare.15 These devices introduce a new care approach where patients participate in their treatment in a dynamic and interactive way, contributing to their empowerment. These interventions offer a wider and more individualised scope than face-to-face interventions, with potentially lower long-term costs.16 Nevertheless, no rigorous trial has yet demonstrated the superiority of digital PA interventions over existing ones. Although e-health interventions are gaining popularity for the treatment of obesity, appearing advantageous compared with current programmes, no evidence of cost-effectiveness has been demonstrated.17 In addition, concerns remain regarding the adherence rate and engagement in the long term.18 Therefore, the use of gamification appears as an interesting way to address these limits.
Defined as the use of game design elements in non-game contexts,19 gamification is the art of improving a routine activity in an engaging and motivating way, by the integration of specific ingredients that make games enjoyable. By gamifying PA, participants are encouraged to move and walk to play, and this tends to make their activity more playful and motivating.20 A recent meta-analysis21 revealed that gamified interventions improved PA with an increase of more than 1600 daily steps. Importantly, additional analyses indicated that (1) gamified interventions appear more effective than equivalent non-gamified interventions and (2) PA improvement persists in the long-term.21 This suggests that gamification is more than a novelty effect, and that is a promising healthcare approach, as it can be easily implemented in daily life without adding demands to people’s schedules. In sum, gamified interventions seem to be a critical strategy to engage participants in digital interventions. However, more rigorous trials are needed to confirm these promising results, to better understand the mechanisms explaining gamification effects, and to test the healthcare potential of gamified interventions.21
Barriers to PA and determinants of behaviour change in obese people
Another key driver to enhance the effectiveness of e-health interventions is the use of behaviour change theories and techniques (BCTs), as they allow to target the active ingredients of behaviour change.22 In the early days of digital interventions, mobile apps, internet platforms and connected objects designed to promote PA were rarely based on scientific knowledge, or at least the characteristics of the programmes were not detailed enough to allow the mapping with evidence-based theories and techniques.23 24 For example, Conroy et al25 evidenced that commercial apps released before 2014 do not contain a large amount of BCTs. Since then, recommendations provided by the Consolidated Standards of Reporting Trials (CONSORT) statement26 or the WHO27 have emphasised the need to systematically use a theory-based approach in the development of digital interventions. More especially, eHealth and mHealth devices constitute an excellent opportunity to both develop and test behaviour change theories (eg, theory of planned behaviour,28 transtheoretical model,29 self-determination theory (SDT)30) and BCTs.31
In addition, recent research has emphasised the importance of precision medicine which focuses on individual variability and social and societal factors of behaviour change in the development and evaluation of therapies.32 In this vein, the social psychology approach can be promising as it highlights the importance of collective-level factors. Notably, it suggests that weight stigma is an important driver of the obesity increase.33 Overweight and obese persons may face specific barriers related to weight stigma when they try to implement exercise in their daily life. They may indeed face or fear to face discrimination from a prejudiced person, or they may have internalised negative stereotypes into their self-perceptions, leading them to avoid activities in which they feel being stigmatised, such as PA.34 For example, the more obese people perceive themselves negatively or feel discriminated because of their weight, the more they avoid PA.35 Considering the impact of weight stigma in the development of obese-targeted interventions is therefore vital to optimise their effectiveness.
Theoretical framework
To address these challenges, the present intervention was built based on the tenets of the SDT36 and the social identity approach (SIA).37
SDT: The SDT is an empirically validated framework which focuses on factors that promote sustained motivation and well-being.38 At its core, this model proposes that motivation is regulated along a continuum from lack of motivation to a completely autonomous motivation, in which the behaviour comes from the individual’s will. Research has revealed that an autonomous motivation has positive emotional, cognitive and behavioural consequences, and is strongly associated with PA over time.39 The most autonomous forms of motivation are the intrinsic ones, which occur when people perform an activity for its own satisfaction, its inherent interest and enjoyment. Especially, practicing PA for the direct pleasure and the inherent satisfaction it provides is an important predictor of the long-term maintenance of physical practice.39 This suggests that a game-based intervention that provides fun and playful experiences would feed the autonomous motivation of participants and would be more correlated with long-term adherence of PA.
In parallel, SDT postulates that autonomous motivation increases when three basic psychological needs are satisfied30: the need for autonomy (ie, need to feel responsible of one’s own actions), for competence (ie, need to feel effective in one’s interactions with the environment), and for relatedness (ie, need to feel connected to other people). Again, gamifying interventions seems particularly promising with this regard, as it can provide basic need satisfaction,20 40 leading to a significant intrinsic motivation improvement.41 First, gamification strategies such as points scores, badges, levels and competitions, sustain the need for competence by providing feedbacks on the user’s behaviour. Second, customisable environments of the games or user choices may support autonomy. Finally, leaderboards, teams, groups or communication functions may support the need for relatedness.20
SIA: It is now well established that exercising in group-based settings may be effective to engage participants in PA and sustain their practice over time,42 43 regardless of the population characteristics.44 However, results from group-based interventions are mixed,45 suggesting that bringing people together does not systematically make interventions successful.46 The SIA offers a relevant paradigm to explain these mixed results. It argues that social groups can affect health behaviours and outcomes only when individuals perceive they share the same identity with another individual or group.46 SIA is the combination of two related theories—the social identity theory47 and the self-categorisation theory.48 As social identity theory introduces the capacity for groups to be internalised into our sense of self (ie, speaking and living situations in the name of ‘we’ and ‘us’ rather than just ‘I’ and ‘me’), the self-categorisation theory explains how people develop their social identity within groups. More especially, it proposes that the salience of a particular social identity results from a context-sensitive categorisation process. Individuals categorise themselves according to a set of core attributes that are salient and observable such as age, gender, ethnicity or weight status. The knowledge of these determinants is precious when designing group-based interventions in order to catalyse the effects of groups with shared social identities.
A recent body of work investigates the links between self-categorisation theory and long-term adherence of PA programmes. Beauchamp et al49–51 have shed light on important attributes that determine engagement in PA. These researchers found that age and gender are particularly relevant markers of shared social identity through PA. Importantly, moderator analyses revealed that adults who were overweight reported a particularly strong preference for exercising within same-gender groups relative to mixed-gender groups, in comparison to normal weight adults.50 The consideration of these attributes that determine engagement in a PA programme can inform and guide intervention choices. Moreover, based on the rejection-identification model,52 Jetten et al53 proposed that social identities derived from group membership can act as psychological resources when individuals are confronted with stigmatisation. Thus, the shared identities forged during a group-based intervention regrouping individuals with the same stigma (eg, weight status) could be the keystone for the emergence of a social identity and social support able to counteract the negative effects of group-based discrimination.
The study aims
The main objective of the Digital Intervention Promoting Physical Activity Among Obese (DIPPAO) randomised controlled trial (RCT) is to evaluate the effectiveness of the Kiplin intervention—a group-based digital programme centred on gamification strategies and informed by the tenets of SDT and SIA—to promote PA among patients with obesity and/or T2DM. The Kiplin intervention is composed of four components embedded within a smartphone app: (1) a gamification of PA through multiple games, (2) a remote APA programme with videoconferencing sessions, (3) an interface for exchange and conversation and, (4) an activity monitoring tool. This study will investigate the short and long-term effects of the intervention over 3 and 9 months in comparison with the usual care provided at the University Hospital of Clermont-Ferrand, France (ie, 3 months face-to-face supervised APA programme). Additional objectives of this RCT will be to better understand the mechanisms underlying this digital intervention and to test its cost–utility compared with the usual care. More specific hypotheses on the expected effects of the intervention are proposed in online supplemental material 1.
Supplemental material
Methods and analysis
Study design
This study will be a two-arm parallel RCT comparing the effectiveness of the Kiplin digital intervention to the usual supervised PA programme of the University Hospital of Clermont-Ferrand, on patients with obesity and/or T2DM. Both arms will benefit from a 3-month programme and assessments will be carried at baseline, 3 and 9 months. The conduct and reporting of the trial will follow the CONSORT guidelines.26 54 For an overview of the study design, see figure 1.
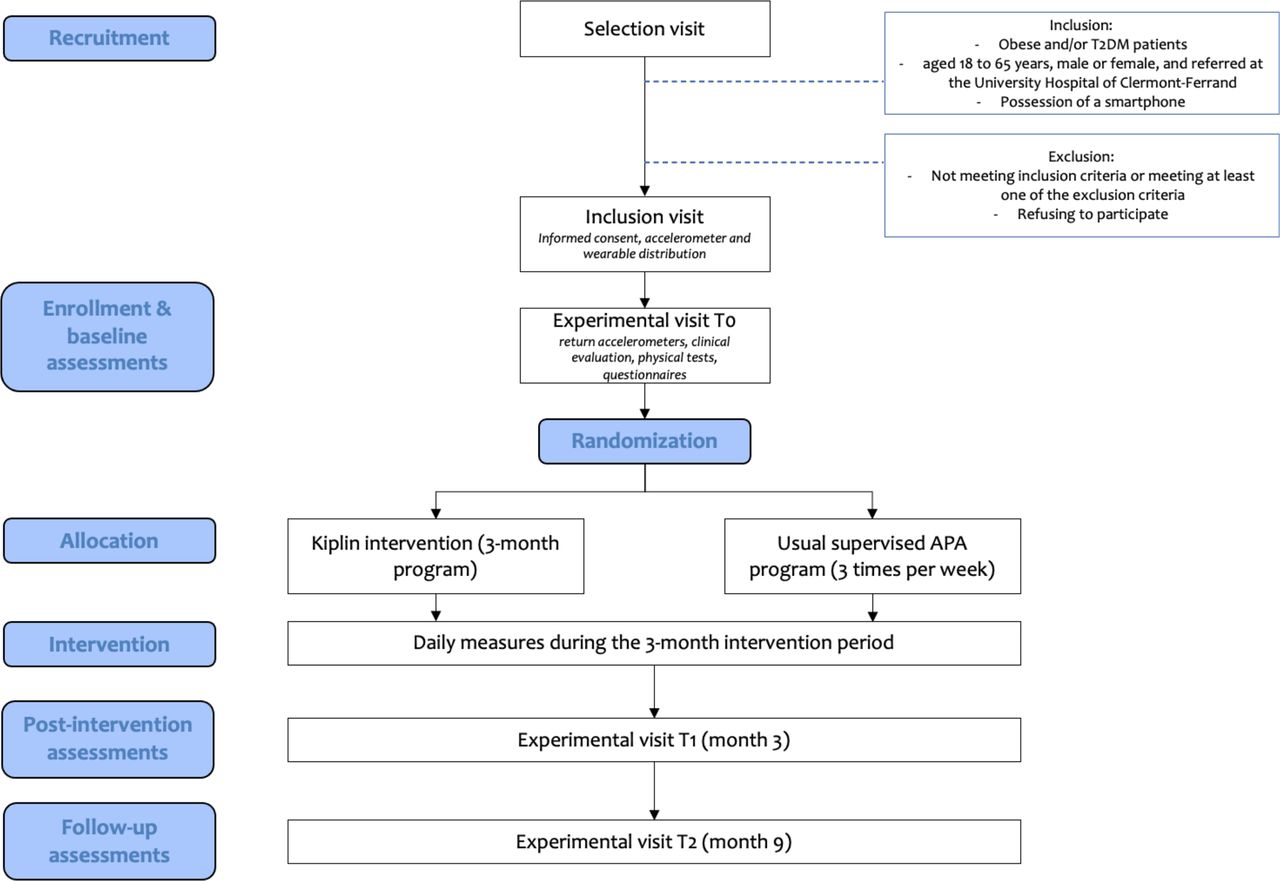
Study flow chart. APA, adapted physical activity; T2DM, type 2 diabetes mellitus.
Participants
Eligibility criteria
Participants will be voluntary patients affected by obesity (BMI ≥30 kg/m² and <45 kg/m²) and/or overweight/obesity and T2DM, aged 18–65 years, male or female, and referred to the department of sports medicine of the University Hospital of Clermont-Ferrand by their physician to benefit from supervised PA. The participants must have a smartphone with a compatible operating system (at least iOS12 or Android 6.0) to be eligible. They must also be covered by health social security and be naive to any APA intervention. In order to ensure the understanding of the different questionnaires used in the study, sufficient proficiency of French will be required. The presence of one of the exclusion criteria listed in online supplemental material 2 will lead to the exclusion of the participant.
Supplemental material
Recruitment
A total of 50 patients (25 per group) will be recruited at the University Hospital of Clermont-Ferrand (department of sports’ medicine). At their inclusion, patients meeting inclusion criteria will be invited to participate to the study and the inclusion will be done during a medical consultation. They will sign a written consent form before being included in the study (see online supplemental material 3 for the patient consent form). Participants will not receive monetary compensation. However, the wearable device (Garmin Vivofit 3) distributed to all participants at the beginning of the study will be offered to them at its end. Recruitment began on June 2021 and the expected end date of recruitment is July 2022, for a start in spring 2022 depending on the sanitary situation. A total of 30 patients were recruited on February 2022.
Supplemental material
Protocol
Procedure
There will be five visits for all participants: the selection visit, the inclusion visit and three experimental visits (T0, T1, T2, see figure 1). Visits will occur in the department of sports medicine (University Hospital) of Clermont-Ferrand. During the selection visit, one of the investigating physicians will check the patients’ ability to complete the full protocol based on eligibility criteria. Only after signing the informed consent form, patients will move to the inclusion visit and will be given a wearable device (Garmin Vivofit 3) and an accelerometer (Actigraph GT3x) for the baseline assessment of PA for 7 days. At least 1 week after this visit, the T0 experimental visit will occur to complete baseline assessments before the start of the intervention. At the end of the 3-month programme, the T1 experimental visit will be carried, and the T2 experimental visit will be placed 6 months after the end of the programme in order to evaluate the follow-up of the intervention. Apart from a few questionnaires, the three experimental sessions will be identical. To ensure equal conditions for all participants, physical condition assessments will be conducted by the same APA coach, within the same day, at the same moment and in the same order.
Randomisation, allocation and blinding
Following the first experimental visit, patients will be randomised in one of the two conditions with a 1:1 allocation. The associate biostatistician will carry out a permuted block randomisation in advance by computer with randomly varying block sizes. The randomisation list will be transmitted using sequentially numbered, opaque, sealed envelopes to the data collectors. Research assistants collecting data will be blinded to the treatment allocation. Double blinding is nevertheless not possible in such interventions because allocation concealment is impossible for participants. Moreover, the APA coaches will not be aware of group allocation at baseline but blinding will be impossible afterward, as the coaches will have seen patients during the sessions.
Data management
All data will be entered electronically into Research Electronic Data Capture, a secure, web-based software platform specifically designed to support data capture for research studies. Data will be reported as it is obtained. All principal investigators will be given access to the cleaned data sets. Investigators with direct access to the data will take all necessary precautions to ensure the confidentiality of information relating to the medical products, the trials, the participants involved and more particularly their identity and the obtained outcomes. A fully anonymised data set, statistical code and all study materials will be made publicly available on the Open Science Framework.
Intervention
Preliminary testing
Feasibility of the gamified part of the Kiplin app has been previously assessed via a qualitative study among breast cancer survivors.55 This study showed that the intervention was associated with positive feelings and was seen as a ‘motivational catalyser promoting good habits’ by the participants. Afterward, the full intervention including telecoaching APA sessions in a 12-week programme has been pilot tested on different patient pathways (unpublished data), including obese and patients with T2DM. Patients’ feedbacks were all positive and enthusiastic and no organisational issues have been identified, suggesting that the intervention was ready to be tested in an RCT.
Intervention overview
To promote behaviour change, we implemented within the Kiplin app 16 BCTs. Previous meta-analyses have shown these techniques to be effective in increasing walking behaviour,56 to encourage behaviour change of overweight and obese populations,57–59 and which were particularly suited for digital interventions.60 Table 1 displays how BCTs have been implemented within the app. Patients will be offered a free download of the app as part of their treatment The Kiplin intervention is composed of four main features:
APA sessions. Participants of the Kiplin group will benefit from an APA programme. Videoconferencing is an interesting perspective to reduce the organisational limitations of face-to-face programmes. With this telemedicine approach, professionals can offer tailored interventions from a distance and propose a remote home-based APA programme to patients in addition of providing monitoring, social support and therapeutic education.61 Thus, this programme will be mainly remote and the number of sessions per week will decrease over 3 months. Patients will benefit of 3 sessions per week the first 2 weeks (1 face-to-face and 2 telecoaching sessions), 2 telecoaching sessions per week the next 6 weeks and 1 telecoaching session per week the third month, for a total of 22 sessions. Sessions conducted in face to face during the 2 weeks have the objective to ensure that the correct movements are adopted by the patients. The telecoaching sessions will be group-based live remote APA classes of 60 min taught by a professional APA coach with a small group (between 5 and 7 patients). Each week, several sessions will be offered to patients who can register according to their preferences and availability (figure 2A). Patients will see in advance the theme of the session. After registering on the app, they will receive a Livestorm link by email allowing them to join the session on their smartphone, tablet or computer. Some sessions will be playful with the integration of quizzes, riddles or tips on PA in addition to physical exercises (ie, endurances exercises, muscle strengthening and stretching). Thus, the sessions will integrate therapeutic education to inform participants on the benefits of PA, the deleterious consequences of SB, and some general knowledge like injury prevention.
Gamification of PA. In addition to the APA sessions, patients of the Kiplin group will benefit from three PA games. Patients will be able to participate in one game per month for a duration of 14 days each. These settings seemed to be the most appropriate considering previous findings and recommendations21 highlighting that gamified interventions of 12 weeks or more would be less efficient than shorter ones. These results suggest that multiple gamification doses would be better than only one long game. The three different games (ie, the adventure (figure 2B), the mission (figure 2C) and the board game (figure 2D); more details about the games in online supplemental material 4) are structured in the same way: the daily step count performed by each participant is converted into points within the game and permits to progress by teams. Thus, the objective is to increase patients’ daily activities through game mechanics and social interactions. Participants will not be given specific instructions on how often they should log in to the app.
Chat and messenger. The messaging functions aimed to encourage social interactions are composed by an internal messaging space to communicate with the team and a general messaging system with all the patients of the programme (figure 2E). During the games, this messenger will be animated every day by ‘Pilot Kiplin’ (ie, a real Kiplin team member animating the app and who takes the form of a funny mascot) who launch challenges, announce results and carry internal messages to motivate participants. In addition, regular notifications (which can be turned off) will be sent by the app to mobilise and inform participants about the games or to remind them to participate to the telecoaching session they are registered.
Activity monitoring tool. Patients will be able to view their activity at any time of the day with their Garmin pedometer. The intervention focuses on daily step count rather than MVPA for several reasons. First, walking appears more adapted for obese people,62 and is statistically associated with declines in all-cause mortality63 64 and improvement in body composition,65 regardless of its volume or intensity.63 66 Along with the pedometer, a visual and numerical interface within the mobile app displays the daily activity (daily step count), the week average and the graphical evolution of the number of daily steps (figure 2F). This tool aims to give feedback on behaviour and promote self-monitoring of PA. Self-monitoring and goal setting strategies have been pointed as major predictors of PA at short term and long term in overweight and obese adults.58 59 For this reason, another major element of the Kiplin app is the goal setting of PA. Recent research on goal setting revealed that interventions that set weekly or daily goals produced greater effects on PA than goals set over a longer time frame.67 Moreover, it appears better to consider the achievement of the goals in ‘percentage of objective achieved’ rather than in a binary way (success/fail) in order to inform that the objective is reached or close to being reached.68 Following these recommendations, the initial step goal at the beginning of the programme will be based on the daily step count of the evaluation week. By the end of the intervention participants will aim to achieve 2000 more daily steps than baseline. To support this objective, daily goals during the games will be fixed on this objective. During time periods without games, participants’ goal step will be increased progressively by 500 steps in order to reach the final step objective at the end of the 3-month programme. The performances will be displayed each day as a percentage of the goal achieved in the form of a gauge that fills up. Each week, a new daily step goal will be settled based on the performance of the previous week. Participants will have the opportunity to personalise their goal increase tier.
Supplemental material

{kind=link}
{kind=link}
Screenshots of the Kiplin app. (A) The telecoaching sessions reservation. (B) The adventure. (C) The investigation. (D) The boardgame. (E) The chat. (F) The activity monitoring tool.
Implementation of BCTs within the app following Michie et al’s taxonomy 75
Finally, in addition to the collaborative teams, leaderboards and the chat aimed to enhance social interactions, several elements have been adjusted in order to facilitate the development of a social identity among Kiplin users. The team’s allocation will be done in such a way that favours homogeneous groups in terms of gender and age. In addition, participants will complete a short and fun personality questionnaire on entering their programme. The answers will be additional elements allowing us to associate in teams people resembling each other. Other strategies will be implemented to facilitate social identification among the teams as the option to choose a team name, the option to see who is registered for APA sessions so patients can join their peers, and incentives by Pilot Kiplin to push participants to meet and walk together in real life.
All these features are part of the standard Kiplin app, which will ensure the generalisability of the results outside the scope of this trial.
Control condition
Participants allocated to the control condition will benefit from the usual PA care of the University Hospital of Clermont-Ferrand, which is a 3-month programme of face-to-face APA, 3 sessions a week on non-consecutive days, for a total of 36 sessions. These individual sessions will be composed of a warm-up, followed by 50 min of endurance exercises, muscle strengthening exercises and stretching, all supervised by an APA coach in a dedicated room. Aerobic and resistance exercises will be performed in a circuit organised as a row of six exercise stations (three aerobic and three resistance exercises). Aerobic exercises will be performed at 50% of VO2max the first week and the intensity will be gradually increased by 10% every 2 weeks to target at least 80% of VO2max over the last 9 weeks. For resistance exercises, patients will perform a single set of 8–12 repetitions of unloaded exercises the first week and the number of sets will be gradually increased to 3. These exercises will be performed at 50% of 1RM during the first week and the load will be gradually increased by 10% every 2 weeks and remain at 80% of 1RM over the last 5 weeks.
The content of both groups is summarised in table 2.
Summary of the groups content
Outcome measures
Primary outcome
The primary outcome will be the daily PA change measured as the daily step count assessed via the Garmin Vivofit 3 (Garmin International, Olathe, Kansas, USA), a wearable activity tracker featuring an accelerometer that has been shown to accurately detect the number of steps under a variety of walking conditions.69 The temporal zone of evaluation will extend from 7 days before the start of the intervention (ie, baseline assessment), through the 3 months of intervention (ie, evolution during the interventional phase), to 7 days after the end of the intervention (ie, post-intervention assessment). Non-wear days will be defined as days with fewer than 1000 steps (as previous research suggested that daily step values less than 1000 may not represent full data capture70 71) and will be removed from the analysis. As using pedometers positively influence daily PA,72 the Garmin wearable will only display on its screen the time and date during the evaluation time. During the intervention period, as self-monitoring of PA is an integrated part of the digital intervention, participants of the Kiplin group will see their object unblocked (ie, display of the daily number of steps, calories burned, distance travelled and minutes of activity performed) following the randomisation. The wearables of the usual supervised PA programme group will stay unchanged during the intervention period.
Secondary outcomes
The secondary outcomes will be the changes in (1) anthropometric measurements and body composition, (2) PA level and SB, (3) physical capacities and (4) quality of life. Psychological mediators and programme adherence will also be examined. Finally, this study will include an evaluation of the cost-utility of the Kiplin intervention in comparison to the usual care. Table 3 provides an overview of all the outcomes measures and table 4 provides the schedule of assessment (following the Standard Protocol Items: Recommendations for Interventional Trials schedule template73).
Outcomes measures of the DIPPAO RCT
Schedule of enrolment, interventions and assessments
Statistical analyses
Sample size and power analysis
Sample size estimations are based on the primary outcome measure of steps per day measured using the Garmin Vivofit 3. We conducted an a priori sample size estimation based on a previous meta-analysis74 that have reported an effect size of d=0.51, (95% CI 0.12 to 0.91, I²=90%) for PA interventions comprising wearables and smartphone apps compared with control groups. However, considerable statistical heterogeneity has been observed in the results of this meta-analysis. The authors therefore excluded studies with a high risk of bias in sensitivity analyses. The meta-analysis revealed a larger effect size of d=0.67 (95% CI 0.48 to 0.86, I²=0%). To conciliate these two results, we decided to base our sample size estimation on an intermediate effect size of d=0.60.
In order to demonstrate a difference equivalent of an effect size of 0.6 on our primary outcome, we will require a sample size of 44 for 80% power and a two-sided type I error at 0.05. More precisely, if we consider that the statistical individual is an individual-day and an intraclass correlation coefficient of 0.5 (in order to take into account the interindividual and intraindividual variability), 2002 individual-days are necessary per group (ie, 22 participants per group). We propose to include 25 participants per group in order to foresee potential dropouts, inherent to such trial.
General points in data analyses
The statistical analyses will follow intention to treat and per protocol principles. Characteristics of participants will be described and compared between groups at inclusion according to the following variables: compliance with eligibility criteria, epidemiological characteristics, clinical characteristics and possible treatments. A description of protocol deviations and causes of dropout will also be provided. Initial comparability of the two arms will be assessed on main participant characteristics and potential factors associated with the primary outcome. Statistical analyses will be performed using R (R Foundation for Statistical Computing, Vienna, Austria) and Stata (V.15; StataCorp).
Analyses of primary outcome
Longitudinal data will be assessed using linear mixed models in order to account for intraindividual differences. Differences in step count changes in function of the condition (group allocation) will be evaluated using models that include the following fixed effects: group, time and group × time interaction. We will consider random intercepts for participants and random linear slopes for repeated measures at the participant level. The normality of residuals will be checked. When appropriate, a logarithmic transformation of the dependent variable will be performed. A Sidak’s type I error correction will be applied to take into account multiple comparisons. The results will be expressed using effect sizes and 95% CIs.
Analyses of secondary outcomes
In a second phase, the primary analysis could be completed by a multivariate approach to take into account the possible confounding factors retained with regard to the results of the univariate analysis and to their clinical relevance (eg, gender, age, BMI and engagement). Particular attention, primarily descriptive, will be paid to participants’ adherence to different intervention programmes. Moreover, an in-depth analysis of drop-outs occurrence will be proposed by considering the dropout as censored data (estimation by Kaplan-Meier method). As the primary analysis will be conducted following intention-to-treat principles, sensitivity analyses will be performed to evaluate the statistical nature of missing data, and to propose, if necessary, the most appropriate data imputation method.
Finally, modelling analyses of longitudinal trajectory profiles could also be carried out, if possible, as well as multiple mediation modelling to examine the hypotheses according to which psychological mechanisms may partially or totally mediate the relationships between the intervention and the number of steps, the PA level and SB. Considering our lack of knowledge about intervention effect sizes on variables such as consequences of weight stigmatisations or in-group identification, Bayesian inferences could be applied in an exploratory perspective.
Continuous secondary outcomes will be analysed as described above for the primary outcome. For non-repeated data, the following comparison tests will be used: Student’s t-test or Mann-Whitney test for quantitative data, and χ2 test or Fisher’s exact test for categorical variables. Because of the potential for type 1 error due to multiple comparisons, findings from analyses of secondary outcomes will be interpreted as exploratory.
Patient and public involvement
The Kiplin intervention has been developed following an iterative process and a user-centred design philosophy. Interviews with patients and healthcare professionals along with usability tests informed us about the different user profiles, their needs and their usage. These data then guided the development of the app. Patients were not involved in the development of the research question, the design, or the recruitment of the trial. Results will be reported individually through a personal report and a summary of the overall research findings on request to the principal investigator.
Ethics and dissemination
The DIPPAO RCT adheres to the principles of the Helsinki declaration. The research protocol has been reviewed and approved by the Local Human Protection Committee (CPP Ile de France XI, No 21 004-65219). All participants will receive information sheets and consent forms to sign before the potential inclusion. Any modification of the research protocol must be subjected to an authorisation agreement from the Ethics Committee.
The results of this study will be disseminated through international conference presentations and in relevant scientific journals. The three complementary but distinct objectives of the trial will be addressed in different publications at the end of the study.
Discussion
The Kiplin intervention is a group-based gamified digital programme aim to promote behaviour change and long-term PA among patients with obesity and/or T2DM. Backed by scientific knowledge, this intervention may change patient’s behaviour by improving their self-determined motivation towards PA, reducing weight stigma that usually act as PA barriers, and ultimately participating to improve programme adherence. More globally, this intervention is the opportunity to address a wider audience though one unique programme by responding to the limits and constraints of face-to-face programmes. Findings will be of interest to researchers, practionners and policy-makers in future discussions on the relevance of digital interventions in the treatment of chronic diseases.
Ethics statements
Patient consent for publication
Acknowledgments
The authors wanted to thank the challenge 3 I-SITE Clermont Auvergne Project 20-25 for their grant and all members of the Kiplin team involved in the development of the mobile application.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AlexMazeas
Contributors AM, AC, MB and MD conceptualised the project and obtained the funding. All authors provided input into the study design. AM and BP designed the data analysis plan. The first draft of the manuscript was written by AM and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding This project is funded by a grant of the challenge 3 I-SITE Clermont Auvergne Project 20-25. The work of AM is supported by an ANRT grant (Cifre PhD Thesis) and by the company Kiplin. Trial sponsor: University Hospital CHU G. Montpied, Clermont-Ferrand.
Disclaimer The funders had no input in the design of the trial and will have no influence on the collection, interpretation or publication of the study results.
Competing interests AC, BP and MD declare that they have no competing interests. AM’s PhD grant is funded by the French National Association for Research and Technology (ANRT) and Kiplin. MB is employed by Kiplin.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.