Article Text

Abstract
Objectives The objective of this study was to examine the structural validity and internal consistency of the original English version of the Patient Centred Assessment Method (PCAM) in a primary care setting in a Japanese island area.
Design Cross-sectional study.
Setting A clinic on a remote island in Okinawa, Japan, that provides general outpatient and 24-hour emergency services.
Participants This study included 355 patients who visited Tarama Clinic from 1 April 2018 to 30 June 2018, were aged ≥20 years, lived in Tarama Village and had decision-making capacity.
Main outcome measures Patient complexity scored by the PCAM.
Results The mean (SD) PCAM score was 21.4 (5.7). The distribution was skewed to the right and there were no ceiling and floor effects. Confirmatory factor analysis found that the previously reported two-factor and three-factor structures did not show a good fit (root mean square error of approximation 0.18 and 0.16, comparative fit index 0.83 and 0.89 and standardised root mean square residual 0.14 and 0.11, respectively). Exploratory factor analysis revealed a new two-factor structure: ‘Biomedical complexity’ and ‘Psychosocial complexity’. The Cronbach’s alpha values for the total PCAM score, the ‘Biomedical complexity’ factor, and the ‘Psychosocial complexity’ factor were 0.81, 0.82 and 0.74, respectively.
Conclusions In this study, confirmatory factor analysis found that the data did not fit sufficiently using the previously reported two-factor and three-factor structures. Instead, exploratory factor analysis revealed a new two-factor structure, for which the Cronbach’s alpha values exceeded the threshold level. Therefore, the structural validity and internal consistency of the English version of the PCAM were verified in a primary care setting in a Japanese island area.
- epidemiology
- general medicine (see internal medicine)
- primary care
- social medicine
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Most patients on Tarama Island are expected to choose Tarama Clinic because of geographical restrictions; therefore, this study collected data regarding almost all patients who needed to visit a medical institution for any reason during the inclusion period.
The generalisability of these findings may be limited because this study was conducted at a single medical institution in an island area of Okinawa Prefecture, Japan.
Although most patients on Tarama Island are expected to choose Tarama Clinic because of geographical restrictions, some might have visited a medical institution located off the island, which could have led to overestimation or underestimation of Patient Centred Assessment Method (PCAM) scores.
Patients with presumably high patient complexity, who were highly dependent on medical and nursing care or who required advanced medical care, would have been forced to move off the island because of the lack of medical and nursing care resources there, which could have led to underestimation of PCAM scores.
Some eligible participants were excluded, and exclusion of possible participants with high or low patient complexity might have resulted in underestimation or overestimation of PCAM scores.
Introduction
Increased attention has been paid to both biological and psychosocial aspects of patients. In the latter half of the 1970s, Engel proposed a biopsychosocial model as a holistic alternative to the biological model that was predominant in the mid-20th century, but was considered to have substantial limitations caused by understanding and responding to patients’ suffering from a biological perspective.1 As its name indicates, the biopsychosocial model adopts biological, psychological and social perspectives and seeks to understand and respond to patients’ suffering holistically.1 From a biopsychosocial perspective, patients’ characteristics are incorporated into a concept called ‘patient complexity’.2 This is defined as ‘person-specific factors that interfere with the delivery of usual care and decision-making for whatever conditions the patient has’.2
Various tools have been developed to assess patient complexity. INTERMED is one such tool, for which the validity and reliability have been evaluated in secondary care settings.3 4 The Minnesota Complexity Assessment Method (MCAM) was developed for use in primary care settings based on INTERMED.2 Both INTERMED and MCAM, which are not patient self-assessment type questionnaires, were designed to be completed by healthcare workers who conduct patient interviews.2–4 The Patient Centred Assessment Method (PCAM) is an advanced version of the MCAM and assesses patient complexity using 12 items across four domains: ‘Health and Well-being,’ ‘Social Environment,’ ‘Health Literacy and Communication’ and ‘Service Coordination’.5 The PCAM is also designed to be completed by healthcare workers.5 The PCAM enables healthcare professionals to identify and assess patients’ problems from a biopsychosocial perspective and deal with these problems in order of priority based on severity and level of urgency.5 Therefore, the PCAM supports healthcare professionals to make referrals to a wide range of services to better meet patients’ needs.5
Several studies regarding patient complexity and the PCAM have been published. Pratt et al developed and established the face validity of the original English version of the PCAM.5 Yoshida et al confirmed the structural/criterion validity and internal consistency of the original English version of the PCAM in a Japanese secondary care setting.6 Mutai et al developed a Japanese version of the PCAM and confirmed its structural validity and internal consistency in a primary care setting in a Japanese urban area.7 Previous research using the PCAM showed that PCAM scores were associated with various health outcomes, such as length of hospital stay,6 burden for physicians and nurses8 and alcohol consumption/alcohol use disorders.9
However, no research has clarified the structural validity and internal consistency of the original English version of the PCAM in a primary care setting in a Japanese island area. Verification of the validity and reliability of the PCAM will promote more research on the association between the PCAM and other health outcomes, which will lead to better assessment and understanding of patient complexity and provide healthcare professionals with guidance regarding optimal medical care. The objective of this study was to examine the structural validity and internal consistency of the original English version of the PCAM in a primary care setting in a Japanese island area.
Methods
This study was conducted in conjunction with another study that examined the association between alcohol consumption/alcohol use disorders and patient complexity.9
Design
This study used a cross-sectional design and was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.10
Setting
We conducted this study at Tarama Clinic, Okinawa Miyako Hospital, which is located on Tarama Island, Okinawa Prefecture, Japan.11 Tarama Island is situated approximately 67 km west of Miyako Island (125 min by ferry12 or 25 min by aeroplane13),14 which is approximately 300 km southwest of the main island of Okinawa Prefecture (55 min by aeroplane13).15 Tarama Island is the main part of Tarama Village,14 which had a population of 1194 people (555 women and 639 men) in 2015.16 The percentage of population ageing (the percentage of the population aged 65 years or older) for that year was 26.4%,17 which was almost same as the national average (26.6%).17 In Tarama Village, 41.6% of the population work in primary industries (agriculture, forestry and fishery) and almost all of these workers (41.2% of 41.6%) are engaged in agriculture.18 19 This proportion is considerably higher than the national average (3.8%).20 Overall, 92.0% of the land on Tarama Island is devoted to raising beef cattle and growing sugar cane, vegetables and tobacco.14 21 The average annual income is 1 765 000 yen,22 which is substantially lower than the national average (3 203 000 yen) in 2015.23
Tarama Clinic, which has four staff (a physician, a nurse, a nurse assistant and a clerk), is the only medical institution on the island (other than a dental clinic) and provides general outpatient and 24-hour emergency services.24 Japan has a ‘free access’ healthcare system where patients are free to choose any medical institution.25 However, most patients on Tarama Island are expected to choose Tarama Clinic because of geographical restrictions. Therefore, this study collected data regarding almost all patients who needed to visit a medical institution for any reason during the inclusion period.
Participants
We consecutively included patients who visited Tarama Clinic from 1 April 2018 to 30 June 2018. We included patients only once, even if they visited more than once during the inclusion period. Of these patients, those who were aged ≥20 years, lived in Tarama Village and had decision-making capacity were judged to be eligible for this study. Patients who refused to participate in this study were excluded. Patients whose participation was judged to have an unfavourable influence on the patient–physician relationship were also excluded. Some questions regarding personal issues, such as financial insecurity, which needed to be asked to complete the PCAM,26 27 might be psychologically invasive for some patients and could potentially damage the patient–physician relationship. In the medical context of Tarama Island, patients had no choice of medical institutions other than Tarama Clinic.24 Thus, if the patient–physician relationship was impaired, the patient would not be able to visit another medical institution, which could cause them to drop out from any treatment they were receiving. For this reason, careful attention was paid to the patient–physician relationship. Finally, patients were excluded if the primary investigator was out of office and unable to obtain informed consent from a patient, or when many patients were in the waiting room and obtaining informed consent from a patient interfered with usual medical practice.
Data collection
We collected data for this study from 1 April 2018 to 31 March 2019. When patients visited Tarama Clinic, the sole physician (primary investigator) scored the PCAM during and after the visit in accordance with the ‘PCAM User Guide for Conducting the Assessment’.28 Japanese is widely and commonly used in Japan, and all interviews for scoring the PCAM were conducted in Japanese. However, a Japanese version of the PCAM,7 which was published in 2020, was not available when the study was conducted. Therefore, using and translating the original English version of the PCAM26 27 and the user guide containing its sample questions28 during the interview, the scorer asked appropriate questions in Japanese to score the items of the PCAM.
Outcome measures
PCAM
The PCAM is a tool for assessing patient complexity from a biopsychosocial perspective5 and has four domains: ‘Health and Well-being,’ ‘Social Environment,’ ‘Health Literacy and Communication’ and ‘Service Coordination’.26 27 Each domain has two or four items: ‘Health and Well-being’ has four items (#1 ‘Physical health needs,’ #2 ‘Physical health impacting on mental well-being,’ #3 ‘Lifestyle impacting on physical or mental well-being’ and #4 ‘Other mental well-being concerns’); ‘Social Environment’ has four items (#1 ‘Home environment,’ #2 ‘Daily activities,’ #3 ‘Social networks’ and #4 ‘Financial resources’); ‘Health Literacy and Communication’ has two items (#1 ‘Health literacy’ and #2 ‘Engagement in discussion’); and ‘Service Coordination’ has two items (#1 ‘Other services’ and #2 ‘Service coordination’).26 27 Each item has four levels of increasing complexity (‘Routine Care,’ ‘Active Monitoring,’ ‘Plan Action’ and ‘Act Now’) and is scored from 1 to 4 as complexity increases.26 27 This gives a total PCAM score from 12 (minimum) to 48 (maximum).27 The PCAM was developed for a range of primary care providers, such as general practitioners and nurses, and also for teams of providers assisting with communication in team-based care approaches.5 The PCAM, in accordance with the user guide, enables people in these professions to ask appropriate questions, to score items of the PCAM and to assess patient complexity.26–28
Participants’ characteristics
We collected the following variables to describe the characteristics of study participants. We obtained patients’ age and sex from their medical records and calculated their annual medical expenses during the prior year using medical expense receipts. A medical expense receipt is an invoice issued by a medical institution to a public medical insurer for medical expenses. This receipt contains information about examinations, medication, surgery, as well as the total medical expenses of both a patient and an insurer.29 We used a self-administered questionnaire to obtain information about educational background (‘below a high school diploma’ or ‘equivalent to a high school diploma or above’), employment status (‘in work’ or ‘out of work’), physical activity status (‘exercising’ or ‘not exercising’), smoking status (‘current smoker,’ ‘ex-smoker’ or ‘never smoker’) and the number of family members living with the patient. A nurse assisted patients to respond to the questionnaire as necessary. ‘In work’ was defined as full-time or part-time workers and housewives/househusbands, and ‘out of work’ as those without an occupation. ‘Exercising’ was defined as engaging in physical activity for more than half an hour twice a week for 1 year or more.
Sample size
Various methods of sample size calculation have been proposed for factor analysis, which are expressed as either the sample size or the ratio of sample size to the number of variables. A sample size of 300 is reported to be good.30 A large ratio of sample size to the number of variables (eg, 20:1) is also considered to be good,31 which gave a sample size of 240 for the 12 PCAM items. Based on these two methods, a sample size of 300 patients was used in this study.
Statistical analysis
We performed descriptive analysis on the characteristics of study participants and PCAM scores. Descriptive data were expressed as mean (SD) for continuous variables and count (%) for categorical variables.
We performed confirmatory factor analysis with weighted least square mean and variance adjusted (WLSMV) estimation, using the scores for each PCAM item as categorical variables. First, in accordance with previous study findings for the structural validity of the original English version of the PCAM in a secondary care setting, a two-factor structure (‘Patient-oriented complexity’ and ‘Medicine-oriented complexity’) was hypothesised.6 ‘Patient-oriented complexity’ included three ‘Health and Well-being’ items (#2, #3 and #4); two ‘Social Environment’ items (#2 and #3); and two ‘Health Literacy and Communication’ items (#1 and #2). ‘Medicine-oriented complexity’ included one ‘Health and Well-being’ item (#1); two ‘Social Environment’ items (#1 and #4); and two ‘Service Coordination’ items (#1 and #2).6 Second, in accordance with previous study findings for the structural validity of the Japanese version of the PCAM in a primary care setting, a three-factor structure (‘Personal well-being,’ ‘Social interaction’ and ‘Needs for care/service’) was also hypothesised.7 ‘Personal well-being’ included three ‘Health and Well-being’ items (#1, #2 and #4), and one ‘Social Environment’ item (#2). ‘Social interaction’ included one ‘Social Environment’ item (#3) and two ‘Health Literacy and Communication’ items (#1 and #2). ‘Needs for care/service’ included one ‘Social Environment’ item (#1) and two ‘Service Coordination’ items (#1 and #2).7 The fit indices were judged to be good if root mean squared error of approximation (RMSEA) was ≤0.08, comparative fit index (CFI) was ≥0.90 and standardised root mean square residual (SRMR) was ≤0.08.32
Where statistical testing found the model fit to be poor, exploratory factor analysis with WLSMV estimation and promax rotation was used to examine the structural validity of the PCAM. A scree plot and a cut-off value for factor loading of 0.4 were adopted to determine how many factors there were, and which items should be included on each factor.
In this study, we performed factor analysis using the scores for each PCAM item as categorical variables, although these were regarded as continuous variables in previous studies.6 7 These variables were scored 1, 2, 3 or 4 as complexity increased.27 When categorical variables, which are discrete in nature, are treated as continuous variables, bias caused by the approximation procedure cannot be excluded.33 Estimation methods designed for categorical variables are recommended in cases in which the variables are measured in relatively few (eg, two to four) categories.33 Therefore, the estimation method for categorical data were considered to be more appropriate and extracted the factor structure more accurately in this study.
Additionally, Cronbach’s alpha, which is considered satisfactory if the value is ≥0.7,34 was calculated to examine the internal consistency of the PCAM.
We performed descriptive analysis and calculated Cronbach’s alpha values using Stata/MP V.15.1.35 Confirmatory and exploratory factor analyses were performed using Mplus V.8.4.36
Patient and public involvement
We conducted this study without patient and public involvement.
Results
During the inclusion period, 521 patients visited Tarama Clinic. Of these, 57 patients were younger than 20 years, 13 patients did not live in Tarama Village and 25 patients did not have decision-making capacity, which left 426 eligible patients. We excluded 28 patients who refused to participate in this study and 9 patients whose participation was judged to have an unfavourable influence on the patient–physician relationship. The primary investigator was unable to obtain informed consent from 2 patients because he was out of office, and from a further 32 patients because many patients were in the waiting room at that time. As a result, 355 patients were included in this study (figure 1, reproduced from Sugiyama et al9). There were no missing values for outcome measures or participant characteristics among the study participants.
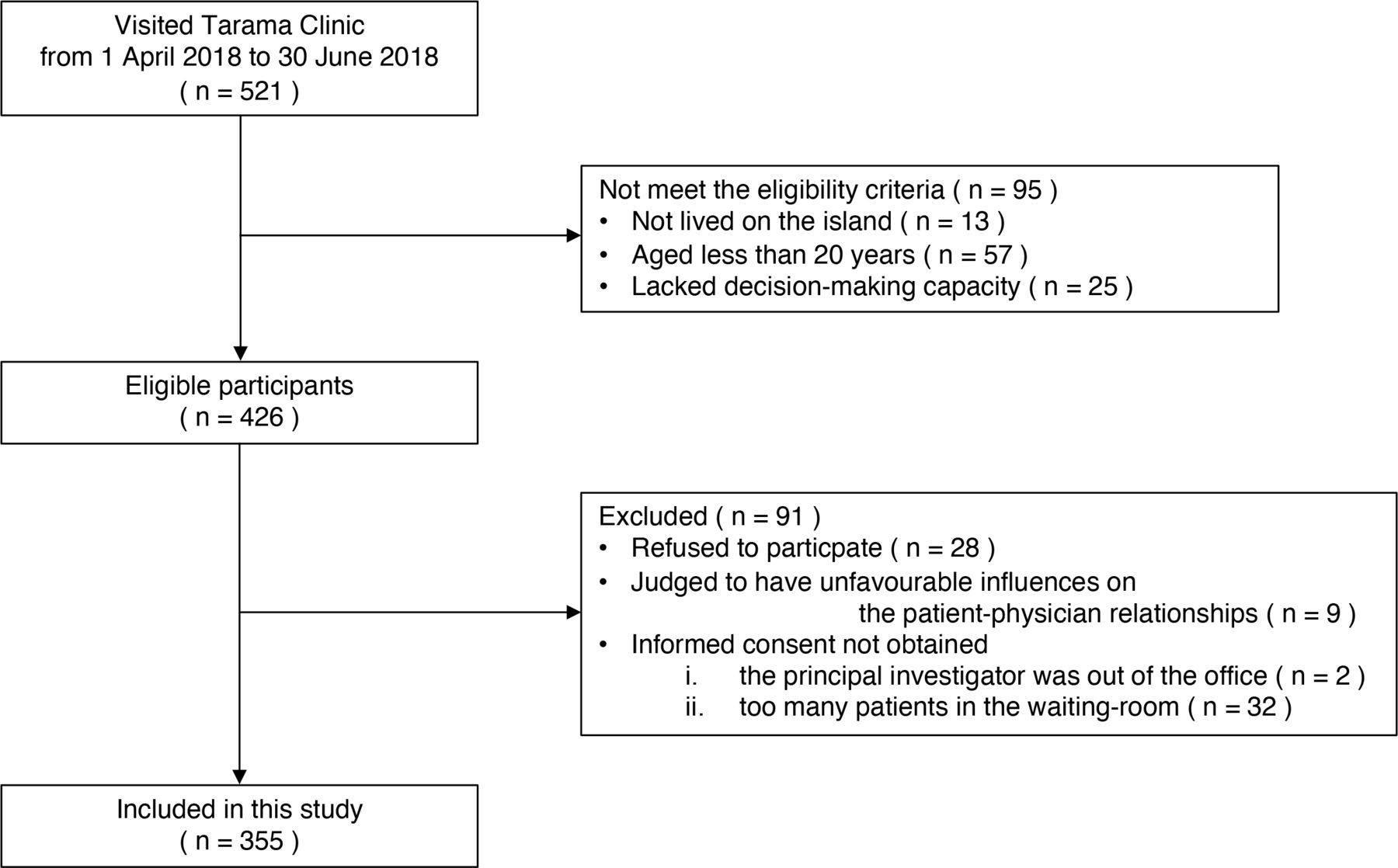
A flow chart detailing the process of inclusion and exclusion of study participants.
The characteristics of study participants are shown in table 1 reproduced from Sugiyama et al.9 The mean (SD) PCAM score was 21.4 (5.7). The distribution was skewed to the right and there were no ceiling and floor effects (figure 2, modified from Sugiyama et al9).
Characteristics of study participants

{kind=link}
{kind=link}
Distribution of PCAM scores. PCAM, the Patient Centred Assessment Method.
Confirmatory factor analysis found that using the previously reported two-factor structure,6 the fit indices were: RMSEA=0.18, CFI=0.83 and SRMR=0.14. Confirmatory factor analysis also found that using the three-factor structure,7 the fit indices were: RMSEA=0.16, CFI=0.89 and SRMR=0.11. Because the data did not fit sufficiently, we performed exploratory factor analysis to evaluate the factor structure.
This exploratory factor analysis revealed a new two-factor structure (table 2), which differed from previous studies.6 7 The first factor extracted comprised four items: two ‘Health and Well-being’ items (#1 and #3) and two ‘Health Literacy and Communication’ items (#1 and #2). The second factor extracted comprised eight items: two ‘Health and Well-being’ items (#2 and #4); four ‘Social Environment’ items (#1, #2, #3 and #4); and two ‘Service Coordination’ items (#1 and #2).
Exploratory factor analysis of Patient Centred Assessment Method scores
The Cronbach’s alpha values for the total PCAM score, the first factor and the second factor were 0.81, 0.82 and 0.74, respectively.
Discussion
In this study, confirmatory factor analysis found that the data did not fit sufficiently using the previously reported two-factor and three-factor structures. Instead, exploratory factor analysis revealed a new two-factor structure, for which the Cronbach’s alpha values exceeded the threshold level. Therefore, the structural validity and internal consistency of the English version of the PCAM were verified in a primary care setting in a Japanese island area.
While the distribution of PCAM scores was skewed to the right, or inclined to be low, Yoshida et al showed a widespread distribution of scores and a higher mean (SD) PCAM score at 25.0 (7.3) compared with our study.6 This discrepancy may be attributable to differences in clinical settings between the studies. Yoshida et al conducted their study in a secondary care setting and the participants were inpatients who were presumed to be biomedically and psychosocially more complex than outpatients in a primary care setting. Furthermore, the mean age (66.4 years) in this study was lower than that reported by Yoshida et al (77.4 years). Older people are expected to be more complex, and have more diverse and complicated backgrounds, such as multimorbidity, dementia and social isolation.37–39 Similarly, confirmatory factor analysis using the previously reported two-factor structure (‘Patient-oriented complexity’ and ‘Medicine-oriented complexity’)6 revealed that the poor fit may be attributable to differences in clinical settings and disparities between the island area in this study and the urban area in Yoshida et al. It is important to note that interlinking mechanisms cascade from social–structural conditions down to biomedical and psychological problems.40 Therefore, healthcare professionals should recognise that differences in care settings need to be considered when assessing patient complexity.
Conversely, Mutai et al showed a distribution with a floor effect similar to that in this study, but a lower mean (SD) PCAM score than our study at 16.5 (5.1).7 Both our study and Mutai et al were conducted in primary care settings. Mutai et al used the Japanese version of the PCAM, which was developed using forward translation, back translation and cognitive debriefing for cultural adaptation, whereas this study used the original English version of the PCAM. The modification of the tool might have contributed to the discrepancies. However, this was minimised because the contents of the Japanese and original English versions were almost the same. Instead, as described above, disparities between the island area in this study and the urban area in Mutai et al should be considered. For example, 52.7% of the participants in this study and 29.0% in Mutai et al had an education level below a high school diploma. Educational background is associated with various aspects of patient complexity, such as health risks and protective behaviours, wages and income and resources for health.41 In addition, the items ‘Daily activities (including employment status)’ and ‘Financial resources’ were directly associated with the proportion of participants who were out of work26 27 (13.5% and 56.7% in this study and Mutai et al, respectively). Although the mean age in this study (66.4 years) was lower than that in Mutai et al. (72.4 years), educational background might have had a greater influence on patient complexity given the higher PCAM score in this study than in Mutai et al. These differences may explain the poor fit as shown by confirmatory factor analysis of the previously reported three-factor structure (‘Personal well-being,’ ‘Social interaction’ and ‘Needs for care/service’).7 Compared with urban areas, healthcare professionals in areas with lower accessibility to medical services (such as island areas) may have to provide services to patients with higher complexity caused by underlying factors, including lower educational background. Therefore, they may need training to appropriately assess patients’ biopsychosocial needs.
In this study, the structural validity and internal consistency of the English version of the PCAM were verified in a primary care setting in a Japanese island area. Exploratory factor analysis identified a new two-factor structure. The first factor was labelled ‘Biomedical complexity’ because it concerned biomedical issues such as physical health needs, lifestyle behaviours and understanding of/engagement in mainly physical health needs. The second factor was labelled ‘Psychosocial complexity’ because it concerned psychosocial issues such as mental well-being, home environment, daily activities, social networks, financial resources and service coordination. This provided strong support for the structural validity of the PCAM, especially as the PCAM was developed to assess patient complexity from both biomedical and psychosocial perspectives.5 As described above, various factors contributed to our finding of a new two-factor structure. For example, ‘Health literacy’/’Engagement in discussion’ and ‘Social networks’ loaded on a common factor in Japanese urban areas.6 7 Mutai et al discussed why these items loaded on a common factor and explained that ‘Health literacy’ and ‘Engagement in discussion’ were associated with health literacy, including communicative/interactive literacy, which was also necessary for active participation in ‘Social networks’.7 However, ‘Health literacy’ and ‘Engagement in discussion’ loaded on a different factor from ‘Social networks’ in this study. Communicative/interactive literacy associated with ‘Health literacy’ and ‘Engagement in discussion’ may not always be necessary to participate in ‘Social networks’ in a small community in a Japanese island area, where participation is presumably ‘forced’ through stronger peer pressure than in urban areas.42 Additionally, the Cronbach’s alpha values in this study exceeded the threshold level, and confirmed the internal consistency of the PCAM. However, other types of validity, such as content validity and criterion validity, and other types of reliability, such as test–retest reliability or inter-rater reliability, were not evaluated in this study. Further studies are warranted to examine the validity and reliability of the PCAM. Thus, the current findings provided partial evidence that the PCAM is a valid and reliable tool for assessing patient complexity in a primary care setting in a Japanese island area.
There are important points to consider relating to this study. The accuracy of estimating factor structures might have resulted in discrepancies between the studies. In this study, we performed factor analysis using the scores for each PCAM item as categorical variables, although these were regarded as continuous variables in the previous studies.6 7 The estimation method for categorical data were considered more appropriate and extracted the factor structure more accurately.43 Additionally, difficulty in evaluating the PCAM might also have influenced the discrepancy between studies. The PCAM has 12 items across four domains, and each item includes a variety of topics.26 27 For example, the item ‘Social network’ covers social networks with friends as well as with family members and work colleagues.26 27 It may therefore take more time, which could be spent with patients, to collect all related information. Furthermore, some items are personal questions. For example, the item ‘Financial resources’ asks about financial insecurity, such as ability to make medical payments.26 27 Some patients might perceive it as inappropriate to discuss such financial topics with healthcare professionals;44 therefore, these items might have been answered incorrectly, as noted in previous research.7 Evaluating the PCAM correctly in a short consultation is difficult, which further complicates the issues of the variety of topics covered and collection of personal information. It is reported to take approximately 20 min to assess all items of the PCAM,44 although outpatient consultation time is less than 10 min for approximately 70% of patients visiting medical institutions in Japan.45 We needed to suspend the interviews and carry them over to the next consultation in some patients because of the limited consultation time. However, in this study, the primary investigator was the only physician in Tarama Village and lived together with the other residents (including study participants) in a small community,24 which created close patient–physician relationships. This might have enabled the primary investigator to understand a variety of topics and personal information,46 and thereby evaluate the PCAM more accurately than previous studies during a short consultation.6 7 These differences in evaluation may also explain the discrepancies between studies.
The PCAM might be able to improve long-term care services in communities in island areas. Japan is experiencing unprecedented ageing of the population, a phenomenon that has been termed the ‘super-aged’ society.47 Moreover, island areas were reported to have a substantially higher percentage of population ageing on average (34.2%48) compared with the national average (26.6%)17 in 2015. To address the challenge of population ageing, Japan has established the ‘community-based integrated care Ssystem,’ which comprehensively ensures the provision of healthcare, nursing care, preventive long-term care, housing and livelihood support.49 However, in areas isolated from their surroundings, such as remote islands, these services are not usually well developed.50 The PCAM can be helpful for identifying and highlighting the services that are necessary but lacking in communities. Based on these assessments, small communities may be able to address problems and improve services in a quick and flexible manner, with closer relationships among organisations including medical institutions, local governments and the private sector, related to the community-based integrated care system.50
There were several limitations in this study. First, we conducted this study at a single medical institution in an island area of Okinawa Prefecture, Japan, which may limit the generalisability of the findings. To ensure some degree of generalisability, further multicentre studies are warranted. Second, although most patients on Tarama Island are expected to choose Tarama Clinic because of geographical restrictions, some might have visited a medical institution located off the island, which could have led to overestimation or underestimation of PCAM scores. Additionally, patients who were highly dependent on medical and nursing care, such as patients with terminal cancer, or those who required advanced medical care, such as dialysis patients, would have been forced to move off the island because of the lack of medical and nursing care resources there. These patients were presumed to have high patient complexity, which could have led to underestimation of PCAM scores. Third, although we included study participants consecutively, 16.7% of eligible participants were excluded. Nine patients were excluded because their participation was judged to have an unfavourable influence on the patient–physician relationships. The main reason was that they had confirmed or suspected mental or personality disorders, which is likely to cause high psychological complexity. Exclusion of these possible participants might have resulted in underestimation of PCAM scores. Additionally, the primary investigator was unable to obtain informed consent from 2 patients because he was out of office, and from a further 32 patients because many patients were in the waiting room at that time. These patients visited the clinic only once during the inclusion period and therefore could not be enrolled in this study during a subsequent visit. These patients usually had mild acute diseases, such as upper respiratory tract inflammation or gastroenteritis, and were otherwise healthy, which meant their patient complexity was likely to be low. Exclusion of these possible participants might have resulted in overestimation of PCAM scores.
Conclusion
In this study, confirmatory factor analysis found that the data did not fit sufficiently using the previously reported two-factor and three-factor structures. Instead, exploratory factor analysis revealed a new two-factor structure, for which the Cronbach’s alpha values exceeded the threshold level. Therefore, the structural validity and internal consistency of the English version of the PCAM were verified in a primary care setting in a Japanese island area.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Ethics Committee of Okinawa Miyako Hospital (approval date: 8 February 2018) and the Ethics Committee of The Jikei University School of Medicine (acceptance number: 30-412 (9433)). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors express their appreciation to Ms C Higa (Tarama Clinic, Okinawa Miyako Hospital) for supporting data collection. We thank Audrey Holmes, MA, from Edanz Group (https://en-author-services.edanz.com/ac) for editing a draft of this manuscript.
References
Footnotes
Contributors YS designed this study, collected, analysed and interpreted the data, and prepared and reviewed the manuscript. RM, HY, RH and SY contributed to the design of the study and reviewed the manuscript. MM contributed to the design of the study, analysed and interpreted the data and reviewed the manuscript. All authors approved the final manuscript. YS is responsible for the overall content as guarantor.
Funding This study was supported by The Jikei University Research Fund for Graduate Students (grant number: N/A).
Competing interests YS, HY and SY are former trainees of the Jikei Clinical Research Programme for Primary-care. MM received lecture fees and lecture travel fees from the Centre for Family Medicine Development of the Japanese Health and Welfare Co-operative Federation. MM is an adviser for the Centre for Family Medicine Development Practice-Based Research Network and a programme director of the Jikei Clinical Research Programme for Primary-care. MM’s son-in-law worked at IQVIA Services Japan K.K., which is a contract research organisation and a contract sales organisation. MM’s son-in-law works at Syneos Health Clinical K.K., which is a contract research organisation and a contract sales organisation.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.