Article Text

Abstract
Introduction Family physicians or general practitioners play central roles in many countries’ primary care systems, but family medicine (FM) remains relatively unestablished in Japan. Previous studies in Japan have examined the general population’s understanding of FM as a medical specialty, but none have explored this topic using actual FM clinic patients. Here, we describe a protocol to explore the perceptions of FM among long-term patients of one of Japan’s oldest FM clinics.
Methods and analysis The study will be conducted at the Motowanishi Family Clinic in Hokkaido, Japan, using patients who have attended the clinic for over 10 years. The analysis will adopt a two-phase explanatory sequential mixed methods design. During phase I, quantitative data from participants’ medical records will be collected and reviewed, and patients’ perceptions of FM will be assessed through a questionnaire. The correlations between participants’ knowledge that the clinic specialises in FM and various characteristics will be examined. In phase II, qualitative data will be collected through semi-structured interviews of approximately 10 participants selected using maximum variation sampling based on phase I results. A thematic analysis will be conducted in phase II to identify patients’ perceptions and changes in perceptions. Finally, each theme identified in phase II will be transformed into a quantitative variable to analyse the relationships between the phases. A joint display will be used to integrate the phases’ findings and examine how phase II results explain phase I results.
Ethics and dissemination The institutional review board of the Japan Primary Care Association has approved this research (2019-003). The results will be presented at the association’s annual academic meeting and submitted for publication in relevant journals. The findings will also be provided to the patients via the clinic’s internal newsletter.
- primary care
- protocols & guidelines
- qualitative research
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The participants represent a unique population with no preconceptions of family medicine (FM) at their first visit, and subsequently formulate their perceptions over 10 years or more.
Quantitative results from phase I will be used to guide maximum variation sampling for the qualitative analysis in phase II.
The integration of quantitative and qualitative data will show how patients’ perspectives have been shaped by their experiences from a pragmatic perspective.
Changes in patients’ perceptions of FM can be investigated qualitatively during interviews in phase II, but there is a risk of recall bias.
The results may have generalisability issues as this is a single-centre study with long-term patients who are likely to have more positive perceptions of FM.
Introduction
The roles of primary care physicians in improving community-based health outcomes and alleviating the economic burden of healthcare services are well established.1 2 A major function of primary care physicians, such as general practitioners in the UK, is to act as gatekeepers who determine initial treatment and subsequent referrals for patients during first contact for a wide variety of health issues.3 4 In Japan, family physicians ostensibly fulfil the same role as the UK’s general practitioners. However, under Japan’s universal healthcare system, patients are free to seek care from any healthcare institution ranging from primary care clinics to university hospitals. Although some individuals may select a family physician as their first contact, many others choose to go directly to a specialist. As a result, the specialty of family medicine (FM) has not been widely adopted in Japan’s healthcare system.5
As Japan’s population continues to age at an unprecedented rate, it faces an urgent need to stem the rise in medical expenditures and ensure the efficient provision of high-quality care.6 To this end, family physicians may play a key role in primary care to promote the use of community-based care and reduce the strain on hospitals. Although the Japanese Academy of Family Medicine first certified FM specialists in 2006, the national government did not initially recognise these accreditations. Finally, in 2018, the Japanese Medical Specialty Board recognised family physicians as general practitioners with the following six competencies: patient-centred care, a comprehensive approach, interprofessional management, a community-oriented approach, ethics and management in a multiclinical setting.7 The World Organization of Family Doctors8 and the Japanese Medical Specialty Board9 define the roles and responsibilities of this specialty from the physicians’ perspective in the position of care provider. In addition, the performance of FM in primary care can be assessed through the functions of first contact, longitudinality, coordination and comprehensiveness.10 In order to facilitate the dissemination of FM in Japan, there is a need for Japanese people to understand this specialty and how it can contribute to their health and lives.
Studies have previously described the perceptions of family physicians among the general population and patients in Hong Kong.11 12 In Japan, a qualitative study addressed the increasing need for physicians in primary care,13 and a quantitative online survey explored the impressions and expectations of family physicians.14 However, these studies were performed on individuals sampled from the general population without regard to their experiences with FM. To the best of our knowledge, no studies have focused on long-term FM clinic patients in order to explore their perceptions as actual users of primary care within a country (such as Japan) where FM remains underdeveloped.
Therefore, we are undertaking a study to examine the perceptions of FM as a medical specialty among patients attending one of Japan’s oldest FM clinics. The study participants comprise patients who are currently consulting a family physician, and have attended the FM clinic for over 10 years. When these patients first visited the clinic, they would be representative of the general Japanese population in which many are unfamiliar with FM. This specialty emphasises the establishment of longitudinality, or a mutual relationship between patients and physicians, over many years. We hypothesise that these patients’ perceptions may gradually change over time as they continue to attend the clinic, and will explore these changes and their underlying causes. We believe that this study’s findings can contribute to the further development and dissemination of FM in Japan.
Objectives
The aims of this study are:
To ascertain the perceptions of FM among patients who have attended one of Japan’s oldest FM clinics for over 10 years.
To explore the temporal changes, if any, in these perceptions and their underlying reasons.
Methods and analysis
Study setting
Motowanishi Family Clinic (MFC) was founded in 1996 in Muroran city, Hokkaido, Japan, by Dr Ryuki Kassai, who was certified as an FM specialist by the College of Family Physicians of Canada long before family physicians were introduced in Japan.15 Since its inception, one of the clinic’s most important roles is that of education through Japan’s first residency training programme aimed exclusively at FM. The clinic’s signboard states ‘Internal Medicine and Paediatrics’, with ‘Family Medicine’ in parentheses. Four family physicians are on staff to provide outpatient and home-visit care in a group practice. There is always a trainee in a 1 year programme preparing to become a specialist, as well as a trainee in a 2-year programme preparing to become a supervisory family physician. This means that one or two physicians, who have 3–8 years of experience after graduating medical school, change every year. Around the clinic, there are two solo practice internal medicine clinics within 800 m, two solo practice paediatric clinics within 4400 m and a 347-bed hospital with emergency facilities 2800 m away. The population of Muroran city is over 88 000, and approximately 9445 individuals (41.7% are aged ≥65 years) reside in the vicinity of MFC.16
Participants
The study population comprises patients who have attended MFC for over 10 years. Having introduced electronic medical records in 2008, we are able to review all patients who have attended this clinic from April 2009 until April 2019. During the study period, all outpatients who have attended the clinic for over 10 years (n=209) were identified as candidate participants. Based on our previous experience, we anticipate a potential response rate of 80%.17 Patients who are unable to answer the questionnaire or undergo interviews by themselves will be excluded.
Patient and public involvement
Patients were not involved in the design of the study. MFC physicians will recruit each candidate participant at the end of a medical consultation and obtain their consent. The study’s findings will be disseminated to the patients via the clinic’s internal newsletter.
Research methods
Research design
The study will adopt an explanatory sequential mixed methods design (figure 1).18 This is one of the three core mixed methods designs (the other two being convergent design and exploratory sequential design), and the study will be conducted in two phases.19 In phase I, quantitative data on the patients’ characteristics and perceptions of FM will first be collected through medical record reviews and a questionnaire. In phase II, qualitative data on any changes in the patients’ perceptions and the reasons for these changes will be collected through semistructured interviews. Finally, the results of phase I and phase II will be interpreted to provide insight into the formation and changes in patients’ perceptions of FM over time.

Explanatory sequential mixed methods design of the study.
Phase I
During phase I, we will investigate the following four categories of variables: patient characteristics, past clinical experiences, present clinical experiences and perceptions of FM. The questionnaire (online supplemental appendix 1) includes items on the perceptions of FM based on those used in a previous study that sampled the general population in Japan.14 This enables a comparison between the perceptions of our participants and those of the general population.
Supplemental material
Patient conditions will be classified using the International Classification of Primary Care, which is composed of 17 chapters based on body systems with additional chapters for psychological and social problems.20 The Japan version of the Primary Care Assessment Tool (JPCAT) (online supplemental appendix 2) will be used to assess the patients’ experiences of the quality of primary care.21 This tool covers six primary care domains: first contact, longitudinality, coordination, comprehensiveness (services available), comprehensiveness (services provided) and community orientation. Information on various patient characteristics and previous health conditions will be obtained through a review of medical records (online supplemental appendix 3). Patients’ perceptions of FM include their knowledge that the clinic specialises in FM and their impressions of FM (table 1).
Data sources and assessment categories in phase I and phase II
Quantitative data will be analysed using descriptive statistics. We will also analyse the univariate correlations between the nominal variable of knowing (vs not knowing) that MFC specialises in FM and each item identified in the exploratory process (eg, patient characteristics and JPCAT score). Moreover, we will examine the correlations between the distribution of patients’ perceptions of FM and the distribution of these items.
Phase II
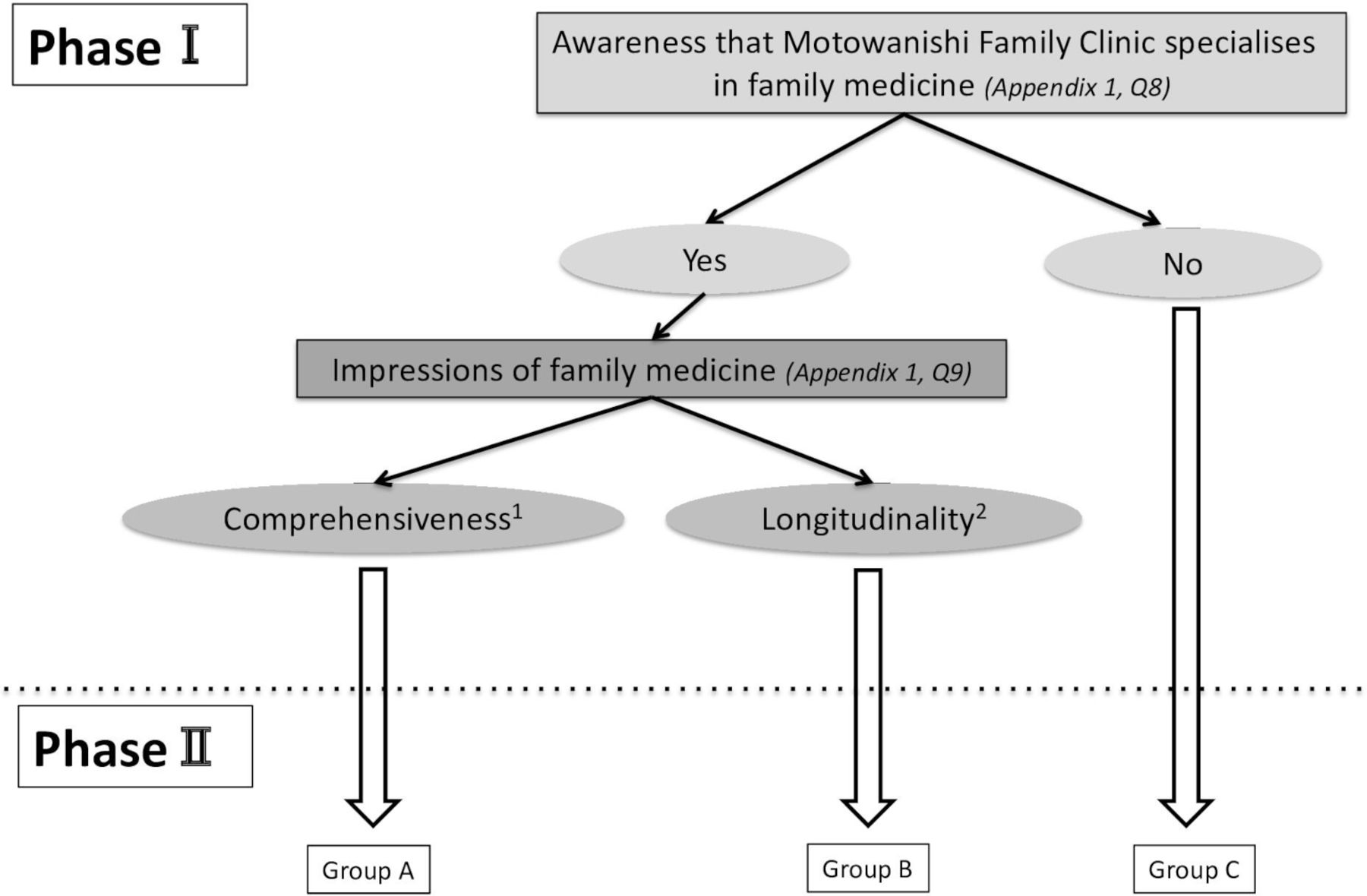
To identify participants for phase II, we will use maximum variation sampling19 based on the results from phase I (figure 2). The participants will first be classified into three groups according to their perceptions of FM, and several participants will be selected from each group to undergo semistructured interviews conducted by physicians. Qualitative data will be collected through these interviews. If the participants selected for phase II show a high level of homogeneity with regard to their knowledge that the clinic specialises in FM and their responses to question 10 (online supplemental appendix 1), we may choose to conduct a focus group interview instead of individual interviews.22 All interviews will be conducted using an interview guide (online supplemental appendix 4).

{kind=link}
{kind=link}
Flowchart of group categorization for phase II based on the results from phase I. Several participants will be selected from each group to take part in the semistructured interviews in phase II. 1Participants who selected options 1–7 for question 10 in the patient questionnaire (online supplemental appendix 1). 2Participants who selected options 8–9 for question 10 in the patient questionnaire (online supplemental appendix 1).
It may be difficult to obtain negative perceptions from the participants because patients who have regularly attended the clinic for over 10 years are likely to be satisfied with their experiences. We plan to overcome this issue in the semistructured interviews by directly asking about the inadequacies of FM and expectations for the future. There is also the risk of recall bias when conducting interviews about past experiences and perceptions. We intend to ask participants about these points using shorter recall periods, and use reference materials to aid recall; these materials will include medical records, photographs of family physicians who have treated the patients in the past and patient diaries. The interviews will be audio recorded and transcribed verbatim.
The data will be analysed independently by two researchers using a thematic analysis23 24 to explain the patients’ perceptions and any changes in these perceptions. This analysis will identify recurrent patterns present in the data and explore the meanings and processes associated with the observed categories of patients’ perceptions of FM.
Interpretation
A portion of the qualitative results from phase II will be presented as nominal variables, thereby transforming them into quantitative data. Using these data, the correlations between the results in phase I and phase II will be analysed. In addition, we will interpret the results on patients’ perceptions of FM from phase I based on the results from phase II using joint displays.25
Ethics and dissemination
The institutional review board of the Japan Primary Care Association has approved this research (2019-003). Participation in this study is voluntary, and we will assure patients that participation or non-participation would not affect their medical care. Participants will be fully informed about the study aim, data collection and use of collected data. In each phase, returning the survey sheet or participating in an interview will be interpreted as consent.
The study’s findings will be presented at the Japan Primary Care Association’s annual academic meeting and submitted for publication in relevant peer-reviewed journals. The findings will also be reported to the patients via the clinic’s internal newsletter.
References
Footnotes
Contributors KS and TK conceptualised the study. KS wrote the first draft of the protocol, and all authors participated in further drafting. RM revised the qualitative methods and interview guide. All authors read and approved the final manuscript.
Funding This work was supported by a research grant from the Japan Primary Care Association.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.