Article Text

Abstract
Objectives People living with dementia (PLWD) have a high prevalence of comorbidty. The aim of this study was to explore the impact of dementia on access to non-dementia services and identify ways of improving service delivery for this population.
Design Qualitative study involving interviews and focus groups. Thematic content analysis was informed by theories of continuity of care and access to care.
Setting Primary and secondary care in the South and North East of England.
Participants PLWD who had 1 of the following comorbidities—diabetes, stroke, vision impairment, their family carers and healthcare professionals (HCPs) in the 3 conditions.
Results We recruited 28 community-dwelling PLWD, 33 family carers and 56 HCPs. Analysis resulted in 3 overarching themes: (1) family carers facilitate access to care and continuity of care, (2) the impact of the severity and presentation of dementia on management of comorbid conditions, (3) communication and collaboration across specialities and services is not dementia aware. We found examples of good practice, but these tended to be about the behaviour of individual practitioners rather than system-based approaches; current systems may unintentionally block access to care for PLWD.
Conclusions This study suggests that, in order to improve access and continuity for PLWD and comorbidity, a significant change in the organisation of care is required which involves: coproduction of care where professionals, PLWD and family carers work in partnership; recognition of the way a patient's diagnosis of dementia affects the management of other long-term conditions; flexibility in services to ensure they are sensitive to the changing needs of PLWD and their family carers over time; and improved collaboration across specialities and organisations. Research is needed to develop interventions that support partnership working and tailoring of care for PLWD and comorbidity.
- QUALITATIVE RESEARCH
- DIABETES & ENDOCRINOLOGY
- comorbidity
- vision impairment
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Observational studies suggest that the prevalence of comorbidities in people living with dementia is high, despite this there is little research that focuses on the organisation and delivery of services for people living with dementia (PLWD) or the patient experience.
There is evidence that in many health systems, people with dementia do not have the same access to treatment and monitoring for conditions such as vision impairment and diabetes as those with similar comorbidities but without dementia.
This study suggests that services are not currently designed to provide appropriate integrated care for PLWD and comorbidity.
There are immediate and simple changes that can be made to improve care for this vulnerable group such as ensuring that: the impact of a diagnosis of dementia on pre-existing conditions is incorporated into care planning, information sharing with family carers is the default option while the PLWD still has the capacity to decide, PLWD are routinely given longer appointments and dementia-specific advice is included in guidelines for conditions such as diabetes and stroke.
Background
Dementia is primarily a condition of old age; consequently, many people living with dementia (PLWD) will have other long-term health conditions.1 ,2 A UK study found that, on average, PLWD had 4.6 chronic illnesses in addition to their dementia.3 As the population ages, and the proportion of people with dementia and comorbidity increases, the delivery of healthcare becomes increasingly complex and challenging.4
Certain comorbid medical conditions may exacerbate the progression of dementia. For example, there is evidence that cognitive decline may be accelerated in older people with conditions such as type 2 diabetes or cardiovascular disease.5–7 Moreover, the presence of dementia may undermine a patient's abilities to access routine care, self-manage chronic conditions and engage in health maintenance activities.8 Despite this, healthcare systems often treat dementia as an isolated condition with little understanding of how the presence of other complex health needs might impact on processes of care, health outcomes or how this population prioritise the uptake of health services.3 ,9
Navigating the different systems of care is particularly difficult for people with dementia and comorbidity, not least because they receive advice and support from different sectors of health and social care and increasingly third sector providers.10 ,11 While there are policy and practice initiatives to improve healthcare for PLWD,12 there is little evidence of how comorbidity is experienced by PLWD and its management over time by primary and secondary healthcare services. There is, therefore, a need to consider what kind of system-based support can enable different health professionals, patients and their carers to access and manage the multiple systems of care that they need. The overall aims of this study were to explore the impact of comorbidities, for a PLWD, on access to non-dementia services and continuity of care and to identify ways of improving integration of services for this population.
Methods
In the light of the lack of previous research in this area,8 we took an exploratory qualitative approach involving in-depth semistructured interviews and focus groups. The purpose was the identification and development of appropriate theory to support the development of interventions for PLWD and comorbidity and their family carers.13
We recruited purposive samples of PLWD and at least one of the following three conditions: diabetes, stroke or vision impairment (VI). These conditions were chosen as they are common in older people, require external monitoring and collaboration between primary and secondary care, may exacerbate the progression of dementia and their management is likely to be complicated by the presence of dementia.14 We also recruited family carers and healthcare professionals (HCPs) who organise and deliver care for people with stroke, diabetes and VI in primary and secondary care. Recruitment took place between December 2013 and July 2014.
PLWD were recruited via dementia registries, GP practices, memory clinics and voluntary organisations in the South and North East of England. They were asked whether they received any significant help from a family/unpaid carer, and if so, the patient's permission was sought to invite the carer for interview. HCPs were identified and recruited via specialty-specific clinical networks. The methods are reported in greater detail elsewhere.2
Procedures
Interview schedules/focus group prompts were designed to explore experiences of healthcare and the barriers and facilitators to effective service provision for PLWD and a comorbid condition. They were informed by a scoping review8 and consultation with service user representatives, and were tailored to the type of participant and the comorbidity involved. The majority of interviews with patients involved patient–carer dyads and took place in the participants' own home, with one interview taking place in a participating memory clinic. Patient and carer interviews were conducted by one researcher (either A-MB or MP). Participants were given a copy of the study information sheet which provided contact details of the research team and a consent form, which they were asked to read and sign. They were informed that they could have a break from the interview or withdraw at any time. Five focus groups with HCPs were conducted in the clinical setting, each lasting about an hour and were facilitated by two female researchers (FB, A-MB). One interview was conducted face to face and the rest by telephone; interviews and focus groups were audio recorded and transcribed.
Analysis
We undertook thematic content analysis15 which was informed by the different characteristics of continuity of care16 and access to care.17 ,18 Data were coded independently by two researchers with emerging themes discussed with service user representatives, the project research team and advisory group. Further analysis was carried out using NVivo10 software. This paper builds on analysis of data presented elsewhere.2
Results
We interviewed 28 PLWD and 33 family carers (characteristics are summarised in table 1). The 56 HCPs included 10 GPs; 18 nurses (specialist and general); 13 consultants/senior clinicians specialising in stroke, diabetes and VI; 9 therapists and 2 managers. Individual interviews were conducted with 27 participants, and the rest participated in focus groups (see table 2). There are three main themes: (1) family carers facilitate access and continuity, (2) impact of severity and presentation of dementia and (3) poor communication and collaboration across disciplines and services may block access to care for PLWD. These themes and the way they link to our key recommendations can be seen in figure 1. Selected quotes supporting each theme are identified in the text and given in full in table 3.
Characteristics of people with dementia (total n=28)
Details of focus groups by region
Selected quotes illustrating the themes
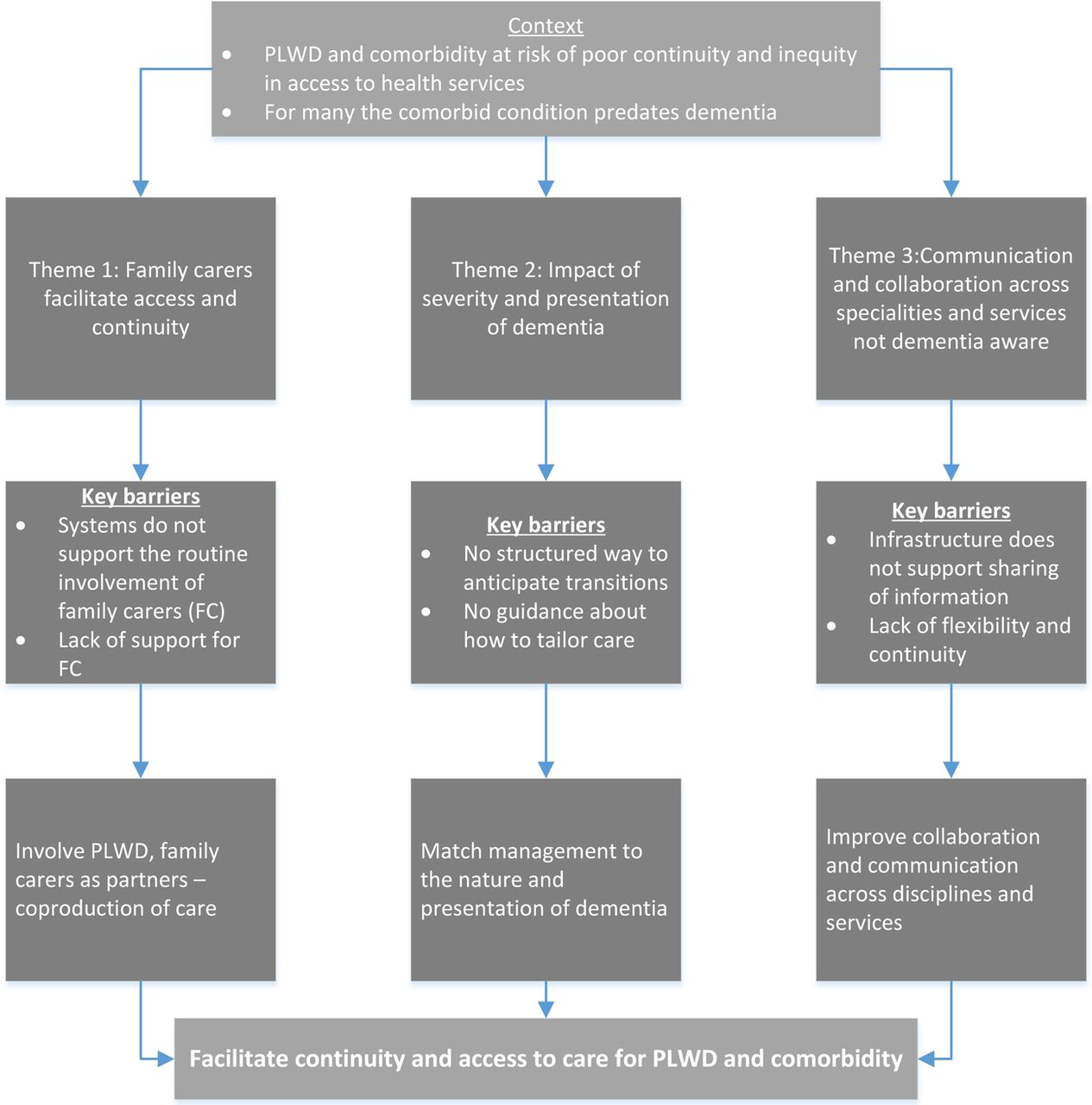
Summary of main themes showing how they link to key recommendations.
Theme 1: family carers facilitate access and continuity
Family members were often proactive in facilitating continuity and negotiating access to services for their relatives with dementia. This included acting as an advocate for their family member with dementia, noticing when something was wrong and seeking help (Q1, Q2), and helping clinicians make treatment decisions, such as whether to thrombolyse a PLWD after a stroke. Family carers also had a significant role in coordinating their relative's care, navigating healthcare systems and facilitating continuity of care; for example, managing appointments, organising transport, keeping records of test results and medication (Q3) and actively transferring information between HCPs and different services (Q4). The availability of a family carer to act as a proxy, and provide consent, information and postdischarge support impacted on a PLWD's access to care. HCPs recognised that PLWD who lived alone, or did not have support from a family carer or advocate, were particularly vulnerable and may have poorer access to care (Q5).
Although HCPs in our study valued the role family carers played, there was little formal recognition of the carers' role, and no systems for negotiating how or when carers' views could be incorporated into care planning. This was reflected in the many examples provided by our interviews where carers felt undervalued or excluded from decision-making about their relative's care (Q6). HCPs' concerns about confidentiality meant that carers sometimes had trouble accessing the information they needed to manage their relative's care. For example, being refused copies of letters or details of hospital appointments. Although a number of carers and PLWD mentioned lasting power of attorney, this was seen as facilitating management of financial affairs rather than healthcare.
There were many challenges for family carers. These included difficulty in understanding how health systems worked and who to contact, their own health problems, emotional and practical challenges of changing roles (Q7) and living at a distance and/or with work and family commitments that made taking on responsibilities for day-to-day care difficult. Caring at a distance may be particularly problematic for carers of PLWD as it is difficult for them to offer support or to monitor adherence to medication over the phone (Q8). Support from social networks, such as extended family, friends and religious groups, and from third sector providers (Q9) were clearly important to PLWD and their carers, but formal support from health and social care was often seen as inadequate (Q10).
PLWD and family carers valued continuity, in terms of relationships with practitioners but also in terms of encounters that factored in the impact of dementia, that built on earlier conversations and appointments and that included people with dementia and their carers in decision-making. Many PLWD and carers reported positive relationships with their GPs and recognised the role that GPs played in coordinating care (Q11). HCPs cited the use of practices for mitigating the impact of living with dementia such as reminding patients of upcoming appointments, giving them longer appointments (Q12) or making sure that it was always the same HCP that saw patient and carer. However, these practices were at the discretion of individual HCPs and not formal processes of care.
Theme 2: impact of severity and presentation of dementia on management
How PLWD managed their care, for example, either independently, in tandem with a family carer or with external health and social care support, was linked to where they were on the dementia trajectory. Some people with early-stage dementia were still able to self-manage their care. As the dementia got worse, the PLWD's ability to self-manage declined and responsibility moved, either partly or totally, from the PLWD to a carer. These transitions often happened when strategies to facilitate self-management, for example, memory aids, diaries and dosette boxes, ceased to be effective (Q13). An example of such a transition, which resulted in a hypoglycaemic attack and hospitalisation, can be seen in figure 2. Data showed that HCPs did not have a structured way of anticipating changing needs and these were times when PLWD could drop out of the system (such as failure to keep appointments), be at risk of exacerbation (eg, taking too much or too little medication) (Q14) or family breakdown in care arrangements that had previously worked well.

{kind=link}
{kind=link}
Illustration of one person's transition from self-management to dependence.
The data show how the severity of dementia, and the ability of the PLWD to cooperate with treatment, impact on clinical decision-making. Access to care was also affected by clinician's previous experiences and their attitudes towards risk. For example, there were contrasting attitudes towards the benefits of performing cataract surgery for PLWD and different opinions about the safety of taking someone off insulin (Q15, Q16). There was also considerable variation in access to care such as screening and monitoring for diabetes.
HCPs in all specialities spoke about the importance of personalising care for PWLD. For example, personalising target values for blood glucose for people with diabetes, simplifying medication regimes for people with VI and adapting stroke rehabilitation programmes. However, there was little evidence of knowledge about personalising care for PLWD being widely translated into practice and many HCPs appeared to lack the skills and confidence to tailor investigations and care to the needs of PLWD, for example, the creation of cognitive impairment friendly eye tests (Q17). This was reflected in the many examples provided by PLWD and their family carers where they felt HCPs had not recognised their need for a different approach. For example, giving patients complicated medication regimes they were unable to manage (Q6).
Theme 3: communication and collaboration across specialities and services is not dementia aware and may block access to care
Most of our participants with dementia and comorbidity had input from a variety of services and specialties. While HCPs gave some examples of successful integrated working (Q18), such as community matrons, or a community multidisciplinary team, a number also outlined how current infrastructure did not support the sharing of information across different specialities (Q19), particularly across mental and physical health services (Q20). HCPs were often unaware that someone had a diagnosis of dementia which impacted on their ability to carry out assessments. For example, VI specialists, who relied on patients being able to provide feedback from vision tests, reported that they were frequently not made aware a patient had dementia before they saw them in clinic.
For many of our participants, their comorbid health condition predated the diagnosis of dementia. Despite this, there appeared to be inadequate consideration by some services of the implications of a diagnosis of dementia on the management of existing conditions (Q21). HCPs from all specialities suggested ways of helping patients navigate multiple encounters with different professionals. This included key workers, case managers or hand-held patient records. However, while this indicated a recognition of the need to bridge the gap between different services, there were few examples of such interventions in practice.
A lack of flexibility in health and social care was also a problem. For example, HCPs reported that in some instances, insulin regimens had to be altered to fit with the schedules of district nurses who were only available at certain times of the day (Q22). The split between social care and healthcare was also identified as a particular problem. Supporting PLWD to live independently at home is invariably seen as social care. This broke down when social services carers were not able to test blood sugars or oversee medication for people with diabetes, making it difficult to coordinate meals and medication and putting PLWD at risk of hypoglycaemia (Q23).
Discussion
We conducted interviews with 28 people with dementia and 33 family carers, and focus groups or interviews with 56 HCPs. What emerged from our analysis is that in order to facilitate access to care and improve continuity for PLWD and comorbid conditions, there is a need for: coproduction of care in which HCPs, PLWD and family carers work in partnership, the matching of management to the needs of the individual (including ways of anticipating changes in needs and tailoring care appropriately), and improved collaboration across specialities and organisations. We found examples of good practice, but these tended to be about the behaviour of individual practitioners rather than system-based approaches; current systems may unintentionally block access to care for PLWD. Our study further highlights not only how family carers are often responsible for negotiating continuity and access for family members with dementia but also how care systems often hinder rather than support their efforts.
While qualitative research does not generally set out to be representative, it is appropriate to consider the transferability of findings. Our study was conducted in two, primarily urban, geographical areas in England, and participants in other areas or countries may face different barriers to accessing services. However, previous reviews have found many similarities in the experiences of people with dementia and their family carers regardless of culture, context or country.8 ,19 Our findings, therefore, should have resonance for the wider international community of older people with dementia and comorbidity. HCPs in our study were a self-selecting sample willing to have their practice examined. As such, it is possible that they may have had more awareness of the needs of PLWD and more interest in their care needs than their colleagues. However, the accounts of HCPs were validated against the accounts of PLWD and their family carers. Like much qualitative research with people with dementia,19 the majority (78%) of our participants with dementia lived with a family carer and we are able to say less about the experiences of those who live alone.
Like previous research, we found that fragmented care, clinical guidelines that focus on single conditions and poor communication and collaboration between different specialities were barriers to continuity and access to care for PLWD.3 ,20 Models of care designed to improve interprofessional working include components such as case management, specialist nursing support, comprehensive geriatric assessment and colocation of different specialities to promote integration and holistic care.21 Randomised controlled trials have provided conflicting information about the clinical or economic benefits of many of these interventions for PLWD,22–25 although non-randomised studies have found positive impacts, particularly on patient and caregiver satisfaction.26 ,27 Our study suggests that relatively minor changes to healthcare systems, such as ensuring that PLWD are identified in advance of visits to outpatient services and primary care, or for providers to make information sharing with family carers the default option while the person still has capacity to decide, could lead to improvements in care.
PLWD are often reliant on others, typically family members, to act as their advocate or help with care management. There is a need for approaches to care that recognise that families are often crucial allies for quality and safety and should, subject to patient agreement, be routinely involved in decision-making for PLWD and comorbidity.28 Such approaches, however, need to incorporate consideration of the capacity of patients and their family carers to attend to current and future healthcare demands, and the support needs of the family carer.29 Participants in our study ranged from those who were able to self-manage their condition and navigate health and social care systems with minimal support to those who required extensive support, often provided by family carers. Consideration should be given to the recognition and management of times of transition, such as when worsening symptoms of dementia, or a medical emergency, impact on a PLWD ability to undertake appropriate self-management. PLWD and their family carers need for support may be particularly acute at such times. People with dementia who live alone or do not have family support may need additional help to navigate systems and access care.
Our study supports calls for health and social care services to take a collaborative approach that recognises PLWD and family carers as partners in their care.30 However, such approaches may be difficult to embed in care for PLWD where decision-making is complicated by concerns about polypharmacy, consent, concordance and the appropriateness of treatment in people with advanced dementia. Further research is needed to develop interventions that support partnership working and that incorporate the consideration of the risk–benefit balance of different treatment options. The call for healthcare for PLWD to be individualised is not new. Despite this, our study suggests that more research is needed to identify how assessment, treatment and ongoing support for conditions such as diabetes can be tailored to meet the needs of PLWD and that is responsive to the way in which changes in the severity and symptoms of dementia might impact on the support required. For example, the development of appropriate methods of assessment for vision in PLWD.
Conclusions
Significant numbers of PLWD have comorbid conditions such as stroke, diabetes and VI; and many of them have multimorbidity. The presence of dementia complicates the delivery of healthcare, and magnifies the known difficulties people with long-term conditions experience when navigating health and social care. Current approaches to improve dementia awareness in the workforce are unlikely to address the challenges described in the study. There is a need for changes in the way PLWD are integrated into systems of care. The delivery of high-quality care to PLWD demands a particularly high standard of care across multiple domains, including communication, multidisciplinary care and clinical decision-making.31 Key elements include: the PLWD and family carer at the centre,32 ,33 flexibility around processes, good communication between services, ensuring that all services are aware when someone has a diagnosis of dementia, taking into account the impact of the nature and presentation of dementia on pre-existing conditions, and incorporating this into guidelines and care planning.
Acknowledgments
The authors would like to thank Dr Simon Conroy, Dr Catherine Dennison, Professor Murna Downs, Ms Heather Maggs, Dr James Pickett and Dr Jill Rasmussen who were members of the Project Advisory Group and Dr Vina Mayor, Ms Marion Cowe, Ms Heather Maggs, Dr Paul Millac, Mrs Diane Munday, members of the Patient Involvement in Research Group at the University of Hertfordshire who acted as the User Reference Group for the study.
References
Footnotes
Twitter Follow Frances Bunn @bunn_f
Contributors FB, CG, CB, GR, LR, JS and SN wrote the protocol. A-MB, FB and MP collected and analysed the data. JS recruited patients. FB wrote the first draft of the manuscript. All authors contributed to the writing of the manuscript and approved its content. FB (the manuscript's guarantor) affirms that the manuscript is a honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding This article presents independent research commissioned by the National Institute for Health Research (NIHR) under HS&DR (grant reference number 11/1017/07).
Disclaimer The views expressed in this paper are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests FB reports grants from the UK National Institute of Health Research during the conduct of the study. CG reports personal fees from the National Institute for Health Research (NIHR) during the conduct of the study.
Ethics approval Ethical approval was obtained from NRES Committee East of England. REC reference 13/EE/0091.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.