The NHS founding principles are still appropriate today and provide a strong foundation for the future
BMJ 2024; 384 doi: https://doi.org/10.1136/bmj-2023-078903 (Published 31 January 2024) Cite this as: BMJ 2024;384:e078903Read the full series: The BMJ Commission on the Future of the NHS

- Nigel Crisp, independent member of the House of Lords1,
- JS Bamrah, consultant psychiatrist2,
- Jessica Morley, postdoctoral researcher3,
- Charlotte Augst, executive director for policy, campaigns and improvement4,
- Kiran Patel, consultant cardiologist and chief medical officer56
- 1House of Lords, London, UK
- 2Greater Manchester Mental Health NHS Foundation Trust, Manchester, UK
- 3Yale Digital Ethics Center, Yale University, CT, USA
- 4Diabetes UK, London, UK
- 5University Hospitals Coventry and Warwickshire, Coventry, UK
- 6Medical School, University of Warwick
- Correspondence to N Crisp crisp{at}parliament.uk
The NHS is currently experiencing the gravest crisis in its history. While much excellent treatment and care is being delivered, too many people are not receiving the care they or their relatives need. Staff, patients, and the public are experiencing a loss of hope, confidence, and trust which must be reversed.1 Austerity, the covid-19 pandemic, and major financial and staffing problems, have left the NHS in a weakened state.23
Radical change is needed in the way services are designed to make better use of the technologies available and to provide more services in homes and communities. These changes should be led by the professionals and communities directly involved. They can build on the UK’s world class biomedical science and professional education,4 the skills and passion of NHS staff, and new contributions to improve health and wellbeing from all sectors. They can be modelled on best practice in the UK and other countries. These changes must be supported by an engaging vision for the future and by adequate levels of funding and staffing.
This article addresses the question of whether, given the problems and scale of change needed, the NHS founding principles are still appropriate now and for the future. The article is the first in a series of papers from the BMJ Commission; others will deal with equity, finance, workforce, wider health determinants, redesigning the health and care systems, and sustainability and the physical environment.
We begin with the founding principles, review how science and the wider environment have changed since 1948, and describe the current problems before returning to the principles. We identify three areas for development to help the NHS deliver—policies on wider health and wellbeing, the roles of patients and citizens, and use of technology and data—before presenting a final section on implementation and a recommendation.
A national health and care emergency
The NHS’s problems require urgent and speedy action. The NHS was founded through a major act of political will against opposition from the BMA and other powerful interests. The next government should be similarly bold and declare a national health and care emergency, calling on all parts of society to help improve health, care, and wellbeing. It should, in effect, relaunch the NHS with the active participation of all sectors.
Government needs to be honest about the scale of the problems, the financial, staffing, and other constraints, and the length of time and effort that will be required. It should establish an Office for NHS Policy and Budgetary Responsibility to provide an independent and expert assessment of NHS plans and policies, which would help protect the NHS from short term political pressures and policies that are poorly thought out.
Equally, the NHS should prioritise tackling inequalities in access and outcomes and give particular attention to the disadvantage and racism experienced by different ethnic groups both as patients and staff of the NHS.
These developments should be supported by embedding NHS policy within a cross-government and cross-sectoral health and wellbeing strategy, and by developing better ways to involve patients, the public, and community groups alongside other stakeholders in policy, planning, and improvement.
The founding principles
The 1946 NHS Act (fig 1) made the minister of health responsible for establishing “a comprehensive health service designed to secure improvement in the physical and mental health of the people of England and Wales and the prevention, diagnosis and treatment of illness […] and to provide or secure the effective provision of services. […] The services so provided shall be free of charge, except where any provision of the Act expressly provides for the making and recovery of charges.”5 Parallel legislation was enacted for Northern Ireland and Scotland.

{kind=link}
The Act explicitly refers to the NHS as being comprehensive, free of charge, and, by implication, available to everyone equally. Neither the legislation nor health minister Aneurin Bevan’s speeches mention founding principles, but review of extensive discussion at the time suggests it is reasonable to identify five founding principles: the NHS as a comprehensive service, universally available, based on clinical need, free at the point of need, and funded through collective contributions.
The principles have since been defined more clearly by the policies adopted to implement them. These policies have changed over the years in response to changes in the wider environment. Since the outset, tension has existed between national and local decision making, with practice changing from one administration to another.
Additions and modifications have also taken place. The most important for England are the seven principles in the 2013 NHS Constitution for England.6 The first two are rewritten versions of the founding principles, with the addition of a wider duty to promote equality. The other five relate to achieving the highest standards of excellence and professionalism, putting patients at the heart of everything, working across organisational boundaries in partnership, providing best value for taxpayers’ money, and accountability. These principles were reconfirmed in 2023.
No other UK country has published a constitution, but each has broadly similar statements of values or principles.
Our discussions produced other suggestions for principles, including recognising the importance of supporting staff and ensuring their welfare. This is the topic of another BMJ Commission article, and we will limit ourselves to discussing the five founding principles.
The changing environment
Enormous changes have occurred since the 1940s. Some of the most obvious affecting the NHS are: demography, where an aging and more diverse population requires a wider range of services; epidemiology, where the greatest burden of disease is now longer term conditions and disability; science and technology, where options for diagnosis and treatment have expanded enormously and personalised medicine is becoming reality; and in the economy, where cheap alcohol, processed food, high stress working conditions, and growing inequalities increase risks to health.
The aging population and changing disease patterns have resulted in more comorbidities, with patients needing support from several services. The increase in longer term conditions, together with a move to a more personalised service, mean that much healthcare needs to be long term and relational, not transactional and episodic. Despite this, the NHS (like other industrialised health systems) still uses service models based on hospitals and episodes of care, which were designed for the different needs of a younger population in the 1940s (more infectious disease, trauma, and acute illnesses). This is a major source of inefficiency in the NHS. In effect it is using a 20th century model to address 21st century problems.
In addition, we now know that most ill health can be linked to external causes (poverty, housing, education, nutrition, and others) and this requires a new focus by wider society and the NHS on preventing disease and creating health.
The current position
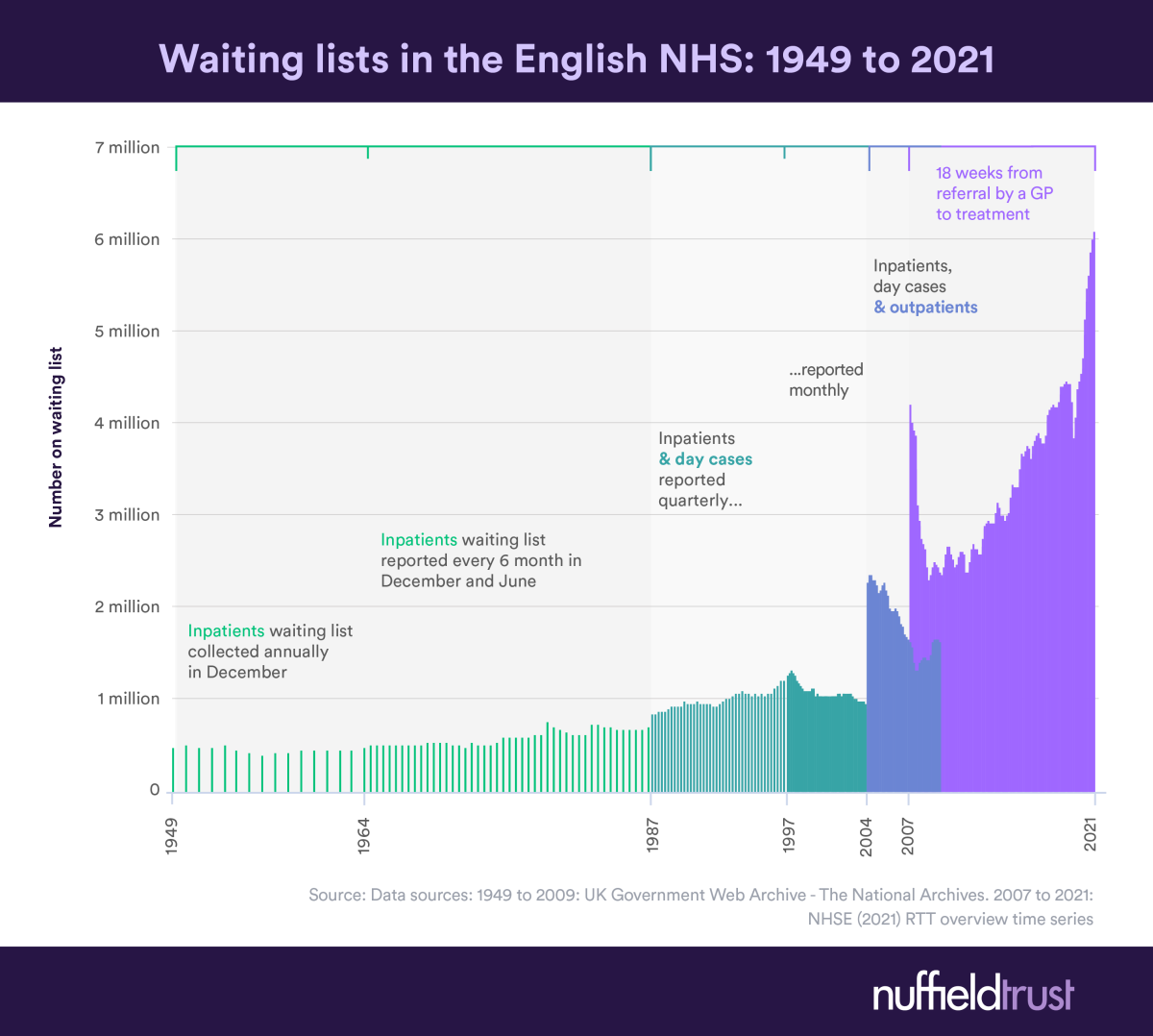
Box 1 describes the problems one clinician describes in delivering a comprehensive health service. We expect that most health workers will recognise these problems. In recent years, the decades-long improvements in life expectancy in England have slowed dramatically,7 waiting lists are at their highest levels ever,8 and confidence in the NHS has fallen. Austerity and covid-19 have played major roles in this. As a result, more people in England who can afford it are using the private sector.9 As the UK champions policy for universal health coverage globally—so that everyone everywhere has access to healthcare—the UK’s own system is in crisis, as are others in western Europe.10
A clinician’s view of the barriers to providing a comprehensive healthcare system
Funding and resource allocation
Funding constraints affect the range of services, the availability and quality of care, and the consistency with which services can be offered. Personalised medicine and advances in healthcare make it increasingly costly to offer and make available all healthcare opportunities. The effective and efficient allocation of resources is variable across the NHS, resulting in health outcomes that range from excellent to inadequate.
Fragmented care
Integration and coordination of care across primary, secondary, and specialised care services is often lacking, leading to a disjointed patient experience.
Health inequalities
Health inequalities arising from socioeconomic, ethnic, cultural, and environmental factors are significant causative factors for poor life expectancy, morbidity, disease prevention, access to services, and measures of life quality.
Technological advances
Providing a comprehensive service requires that technology can be exploited safely and effectively across the whole range of services, particularly in electronic care records, digital consultations, health applications, and other digital solutions, enhanced with the closely governed use of artificial intelligence. This requires significant investment, training, and infrastructure support.
Workforce shortages
The NHS, like other health systems globally, faces severe shortages of doctors, nurses, and other allied healthcare professionals. Adequate staffing levels are crucial for providing comprehensive care, addressing the needs of the population, tackling health inequalities, and meeting demand.
Appropriateness of the founding principles
The key test for whether the founding principles are still appropriate is whether they can (in the words of the 1946 Act) “secure improvement in the physical and mental health of the people of England and Wales and the prevention, diagnosis and treatment of illness.”
The five founding principles are connected, and work together to provide an overarching framework for the system, although they can sometimes be in conflict (as seen below). Bevan said that a comprehensive service would “ensure that every man and woman and child can rely on getting all the advice and treatment and care which they may need in matters of personal health.”11 What constitutes a comprehensive service is not simple, however. Services can be provided in a variety of ways: in the community or hospital, for example, or through prevention rather than treatment. Opinions differ on what constitutes effective and necessary treatment and care, and different parts of the community have different needs.
Moreover, the financial implications are significant. In the first year of its existence, the NHS spent £32m on optometry against a budget of £1m, prompting the government to introduce charges for dentistry, prescription, and optometry.
Successive governments have introduced policies to manage the tensions between providing a comprehensive service and it being free at the point of need. These include:
Exemptions from dentistry, optometry, and prescription charges for children, people drawing a pension, those with disabilities or long term sickness, pregnant women, new mothers, and those in receipt of certain benefits. Only the English NHS still charges for prescriptions. The Scottish NHS provides eye tests and dental examinations free of charge.
National and local arrangements for priority setting, which are sometimes in conflict, and permitting the development of waiting lists to ration and delay access.
Managing resources through evidence based practice and protocols, and introducing new technologies largely through professional education and the National Institute for Health and Care Excellence (NICE) and its equivalents in the four countries.
These provide a policy framework. However, the NHS and its clinicians and managers need constantly to adapt to the situation on the ground, make judgments, and manage politics and their patients’ expectations.
Alternatives to a comprehensive service
The alternative to a comprehensive service is to limit the services either to a particular range available to everyone and/or to limit them to a part of the population. This would be typical, for example, of an insurance policy which had a defined set of benefits provided only to its policy holders. People would then have to pay for any additional services either directly or through an insurance system if they could afford to, or go without them.
Defined benefits
A defined benefits system has several drawbacks. The benefits package may be eroded over time to become a minimum safety net of services. Cash strapped governments might exert pressure to reduce benefits (austerity is a recent example) and commercial interests are likely to promote more expensive options as alternatives to the basic package. A safety net service is likely to lead to stagnation and poor services as innovation, development, and investment move into other areas with higher profitability. Inequality is likely to increase because poorer people can’t pay for additional services, and service quality and health outcomes may suffer if only some needs are met.
A comprehensive system, in contrast, promotes innovation in the services available to everyone. We argue that a comprehensive service should remain as a vital aspiration that will constantly force planners and commissioners to consider how best to achieve it. It is a spur to progress, but it will only work when there is transparency and trust.
Today’s NHS can best be described as a comprehensive service with some limited exceptions where resources are managed through waiting lists and other practical means such as NICE guidance and protocols. This needs to be publicly acknowledged together with a public commitment to making it as comprehensive as possible, adding new services as evidence of their effectiveness and value is demonstrated and resources permit. Priority setting will remain essential and must be conducted through public, visible, and accountable processes with everyone—patients, staff, and the public—having good information about what can or cannot be provided at any given time.
Trust and transparency are essential. Health workers, who have to make decisions about treatment, as well as patients, will benefit from greater transparency in decision making.
Defining benefits might be perceived as bringing certainty, but this is not entirely true. Difficult and disputed decisions will still need to be made. Defined benefits need to change as practice advances and, for example, insurance based systems that take a defined benefits approach spend a great deal of time and money on disputes about contracts and coverage.
The greatest anomaly in the English system is that social care, on which a lot of healthcare depends, is the responsibility of local authorities, is mostly means tested, and varies enormously between areas. Shared health and care management, as occurs in Scotland, Northern Ireland, and Manchester, offers a partial solution, but this approach is not widespread. The problem is beyond the scope of this paper.
On the subject of clinical need, practice has become more sophisticated with, for example, patients and their advocates increasingly involved in clinical decisions through co-creation and informed choice. What matters to patients can be as important as what is the matter clinically. Similarly, assessing the health needs of populations and communities has become more comprehensive and needs to involve patients and citizens who can identify issues not recognised by professionals.
Charging patients at the point of care
Another alternative would be to provide a comprehensive service by charging patients for using some or all services through co-payments. This takes us to discussion of the NHS being free at the point of need. Aneurin Bevan, in his book In Place of Fear, argued that “no society can legitimately call itself civilised if a sick person is denied medical aid because of lack of means,” and describes the difficulties people had without a free health service.12 The establishment of the NHS eliminated the catastrophic economic impacts that illness often had on an individual and their family. In contrast, two thirds of bankruptcies in the US (where services are largely insurance based) result from medical costs, and medical debt affects enormous numbers of people.13
Charging for care might be expected to reduce unnecessary health service usage, affecting poorer people more acutely. The RAND Health Insurance Experiment, a randomised controlled trial conducted in the US between 1974 and 1982, was designed to assess the impact of cost sharing between the insurer and the patient, or co-payments, on people’s use of health services.14 It showed that cost sharing reduced “appropriate or needed” medical care as well as “inappropriate or unnecessary” medical care. This had minimal impact on health status, except in people who were poor and sick, where the reduction was on average harmful: “The projected effect (from having no charges) was about a 10% reduction in mortality for those with hypertension.”14
A recent report that considered these issues concludes that user charges are not an effective way of directing people to use health services more efficiently. It finds that people do not value interventions more highly when they have to pay for them out of pocket, and that even relatively small user charges can deter people from using needed healthcare. Such charges can reduce adherence to essential medicines and other forms of treatment, increase the use of other health services, lead to financial hardship, increase the use of social assistance, and adversely affect health, particularly in people with low incomes or chronic conditions.15
One option would be to give exemptions to charging, as currently happens with prescribing, optometry, and dentistry. About 40% of the English population has exemptions, but almost 90% of items prescribed are exempt.16 This is unsurprising given that older, younger, sicker, and poorer people, who are largely exempt, are more likely to need prescriptions and services. If the same exemptions were agreed, charges would be paid only by a small part of the population and would need to be high to make a material difference to the NHS budget.17
With the UK’s current approach, financial risks are shared across a large population, and general taxation is the cheapest way to raise funding without the large overheads of insurance or patient payment systems. Proponents of alternative ways of funding will need to demonstrate how the benefits of change will outweigh the increase in overheads and the costs of changing to a system of insurance, private payments, or co-payments.
The principle of collective contribution is about solidarity and sharing risks. It is a natural accompaniment to a system free at the point of need and is a unifying factor at a time when society is becoming less cohesive.
Financial issues are discussed in more depth in a later article from the BMJ Commission.
Universality, equality, and equity
The NHS Constitution states: “[the NHS] is available to all irrespective of gender, race, disability, age, sexual orientation, religion, belief, gender reassignment, pregnancy, and maternity or marital or civil partnership status.” However, major inequalities in access and in health outcomes exist between different groups of service users. In 2022, the difference in healthy life expectancy between the highest and lowest local authority areas in the UK was 19.8 years for women and 17.8 for men.18
The NHS also needs to consider equity. This means recognising that people do not all start from the same place, and acknowledging and adjusting for imbalances. Allocation of resources and opportunities should therefore be based on what is needed by different groups to access appropriate services equally and to achieve equal outcomes. Against this background, it is important to make equity more explicit in operational policy and to stress the importance of measuring and achieving equality of outcomes.
People from black and Asian backgrounds, as well as recent migrants, make up a higher proportion of NHS staff than their representation in the wider population. They also suffer worse access to services and poorer health outcomes, from maternal services to surgery and mental health. Given their numbers, tackling the disadvantage and inequalities affecting these groups will make a major contribution to reducing inequalities overall.19
Some asylum seekers, undocumented migrants, and many recent migrants do not always have full access to services, and many have to pay a fee for them (even those who work for the NHS). These issues must be addressed, but are beyond the scope of this paper.
The NHS performs well on equity in international comparisons of health systems, such as the Commonwealth Fund, but this is not the whole story. The NHS was designed to meet the needs of everyone, including the poorest. Today, however, inequity in access to services and health, and the ability of people with higher incomes to express needs, claim rights (often described as the inverse care law), and to opt for private care, leaves the poorest at greatest disadvantage. Covid-19 starkly revealed these inequalities.
Were Bevan redesigning the NHS today he would surely ask why the service was failing those most in need.
These issues are also discussed more fully in a later article from the BMJ Commission.
Summary
We have argued that the NHS is a comprehensive service with some limited exceptions, where resources are managed through waiting lists and other practical means, and that the aspiration to being comprehensive needs to be retained as a spur to innovation and development.
We have also argued that being (very largely) free at the point of need promotes equity and is a practical and appropriate approach to improving the health of the population. Any movement away from it is likely to be expensive and without certainty of improvement.
The other founding principles of universality, decisions based on clinical need, and collective contributions follow from the first two, and are relatively uncontentious.
In summary, we believe that the NHS founding principles are still appropriate today and provide a strong foundation for the future. We recommend that the government in place after the next election re-commits to these principles as part of a wider set of actions. These include giving immediate priority to tackling inequalities in access and outcomes and paying particular attention to the disadvantage and racism suffered by different ethnic groups both as patients and staff of the NHS.
Much can be learned from other health systems in both high and low income countries.2021 The NHS is not unique; most western European systems are based on comprehensiveness and universality and have different ways of managing the issues raised here. All have some exceptions and/or charges. Private and insurance based systems, as in the US, ration by the ability to pay and often do not cover vital areas such as mental health. Other systems combine public and private health approaches and have many exclusions and co-payments. Meanwhile, the lowest income countries have predominantly out-of-pocket payment systems.
The NHS has a serious financial problem to resolve, but the central issue is a health problem, which can only be dealt with through changing the approach to health and healthcare. Financial solutions need to follow health ones.
The next section briefly discusses three areas for development which will help the NHS perform its role. These are wider policies on health and wellbeing, the roles of patients and the public, and technology and data. We conclude with recommendations.
Future developments
Policies on health and wellbeing
It is well understood that social, economic, commercial, and environmental determinants shape a large proportion of an individual’s health status.22 The NHS can only directly affect these as an employer and anchor institution in local communities. We therefore recommend the creation of a cross-government and cross-sectoral health and wellbeing policy where wellbeing is, as described by the World Health Organization, “a state of mind” encompassing “quality of life and the ability of people and societies to contribute to the world with a sense of meaning and purpose.”23
We argue for the development of such a policy and the introduction of a UK version of the “health for all policies” approach pioneered in other countries, and placing new emphasis on the importance of communities, social structures, wellbeing and health creation.24 This would be characterised by:
Strengthening the roles of all parts of society—government, families, businesses, communities, schools, and more—in promoting health and wellbeing, protecting the public, and preventing disease. An example would be the recent Healthy Homes Bill, which, if passed, would have laid a duty on the secretary of state to ensure that all new housing promoted health, safety, and wellbeing.25
Understanding that the health of an individual is intimately linked to the health of their family, community, the health of wider society, and the health of the planet, and introducing measures to promote health and wellbeing at all these levels.
Recognising the importance of promoting and creating health and wellbeing, as well as tackling the causes of disease and preventing disease and injury. Health is not simply the absence of disease.26 Factors that promote health include having a social network, meaning and purpose in life, an increased degree of autonomy, and access to nature and green spaces, as well as the more familiar factors such as exercise, good diet, and good conditions of employment and living.
Treating improved health and wellbeing as a positive contributor to the country’s economy and not, as too often happens, a cost. This involves a recognition that human development and “human capital” are central to the wellbeing and prosperity of the country.
Patients and the public
The 2002 Wanless report, commissioned by the Treasury to look at the long term sustainability of the NHS, recommended that this could only be achieved through the full engagement of patients in their own health and healthcare.27 Relatively little progress has been made since, with a focus on immediate service provision rather than upstream on human behaviours, illness and injury prevention, and health creation. This needs to be reversed, with patients and the public (as voters and future patients) engaged not only in maintaining and improving their own health but also in maintaining and improving the system.
Patients and the public can play a greater role in the design and evaluation of NHS services. Patients are experts in what it is like to experience NHS care, to live with specific conditions, or to care for loved ones experiencing ill health. They often know better than researchers and analysts the most important research questions, the most vital services needed, the right outcomes to measure, and the best ways to ensure that the NHS delivers on its ultimate goal of patient and public benefit.
Patients and the public also have important roles in improving and creating health, and make an important contribution to the future success of the NHS. Organisations within local communities and in every sector are already dealing with some of the most difficult health issues and creating health for themselves and others, with or without the assistance of the health system and health professionals.28 We therefore recommend that the government develops better ways to connect patients, the public, and community groups with the NHS, particularly at local level.
We propose that the NHS needs to embrace these roles by:
Placing community assets and efforts at the centre of health creation and long term conditions management.
Recognising that measures that strengthen community connection, voluntary sector activity, citizen voice, and health democracy strengthen the NHS’s ability to do its job properly and create the conditions for people to be healthy.
Learning from community health improvement in environments where resources are more constrained: focusing on the essentials, looking upstream, majoring on inclusion, and advocating for rights.
This approach will help rebuild confidence and trust in the NHS. We are not proposing structural changes or going back to structures such as regional health authorities, but looking for behavioural change and new approaches such as citizens’ assemblies, where patients and the public can better engage in governance and decision making, alongside other stakeholders.29 Local services and planners need to think about how patients, the public, and community groups can be connected at the most local level and feel part of the efforts to care for themselves, their fellow citizens, and communities.
Some of the loss of trust in the NHS appears to be about the role of politics in its management. This is why we recommend a method for independent scrutiny of plans and policies.
Technology and data
The importance of advances in technology can be exaggerated, but it is clear that increasingly “Science, technology, and data will determine much of the framing and the language of health, shaping how health workers think about health problems and possible solutions, and how they act.”30
Technology and data are themes running through all the BMJ Commission’s articles and have so much to contribute to improving health, healthcare, and wellbeing in the future. NHS data on tens of millions of patients over many years, for example, are extraordinarily valuable for research and development.
However, artificial intelligence could also be used for private gain or disruptive purposes, and this relates directly to issues of trust and confidence in the NHS. Poor performance of the English 111 service has already led to criticism of diagnosis by algorithm, and suspicion of motives will make this worse where private companies are involved, as in the Post Office scandal.
Mitigating these risks requires the NHS to adopt a principle of values based innovation and to put in place robust governance arrangements to protect the core principles and values from trade-offs and dilution. One of the authors (JM) has published recommendations for how to secure appropriate governance. These cover use of NHS data for training AI algorithms, accountability, technical validation, prevention of vendor lock-in, economic evaluation, and the potential for AI screening of the population.31 This would support development of the NHS as a Learning Health system driven significantly by data, as well as digital and predictive AI.32
Recommendations
We have argued that the NHS founding principles are, with the qualifications noted, still appropriate now and provide a strong foundation for the future. But we need to make major changes to how these principles are put into practice. These include updating service models to make them fit for the 21st century, greater use of technology and data, developing an approach that encompasses all of society in creating health and preventing disease, and a focus on people—trust, engagement of patients, citizens, and staff, the development of human and social capital—and changes to professional education.
Implementing change at this scale is difficult and it is useful to look back at the major reforms introduced in 2000, which the King’s Fund reported as leading to the most significant sustained improvements in the history of the NHS.33 Lessons can be learnt about what worked and what didn’t.34
Three key actions enabled those reforms. They involved people from across the NHS and its partners in developing a 10 year plan.35 This was supported by a major programme of “investment for reform” and by the Wanless report, which produced a long term financial plan and brought in the Treasury.27 These actions created buy-in and momentum which carried the NHS through the next few years when controversial policies were introduced about use of the private sector and patient choice. This momentum was maintained by success in achieving targets from 2002 onwards—with waiting lists and waiting times down significantly,36 substantial improvements in cardiac and cancer care, and public satisfaction doubling over a 10 year period. The private sector, which had gained patients from the NHS in the 1990s began to lose business from 2003 onwards as people came back to the NHS.
Despite this, problems arose because of over-focus on numbers and targets rather than quality. Too many reorganisations took place, and there was political infighting over the direction of policy, too great a political involvement in operational issues and, ultimately, a failure to pivot towards health and away from a focus only on health services.
This discussion illustrates how important politics are to the NHS. Political will drove its foundation and the NHS Plan, but political engagement in operational policy and planning can be influenced by short term political objectives, and therefore should be subject to independent public scrutiny. The NHS needs long term thinking and stable, consistent policies. We therefore recommend the establishment of an Office for NHS Policy and Budgetary Responsibility for England. This would be based on the role of the Office for Budget Responsibility.37 It would review national NHS plans and policies and publish its conclusions, thereby helping to ensure that they are well based on evidence and properly costed. It should not, however, duplicate the roles of any existing bodies. The BMJ Commission group on finance will develop this idea further.
Given the extreme seriousness of the situation and the lessons learnt, we recommend that the government in post after the election should declare a national health and care emergency calling on all parts of society to help improve health, care, and wellbeing. The government should, in effect, relaunch the NHS with the active participation of communities, employers, businesses, housing providers, local authorities, food producers, schools and the public, as well as patients, health and care workers, carers, and others in preventing disease, providing care, and creating health.
This would involve:
Making a clear statement of commitment to the NHS and its founding principles, and engaging all parts of society in a renewed vision and plan for health, care, and wellbeing that will generate the buy-in and momentum to implement the necessary reform.
Creating a cross-government and cross-sector health, care, and wellbeing strategy, of which NHS strategy would be an integral part, to show how the whole population and all sectors can contribute, and supporting this with legislation as necessary.
Developing better ways to connect patients, the public, and community groups with activities and planning for the NHS, particularly at local level.
Giving immediate priority to tackling inequalities in access and outcomes and paying particular attention to the disadvantage and racism suffered by different ethnic groups both as patients and staff of the NHS.
Establishing an Office for NHS Policy and Budgetary Responsibility to provide an independent and expert assessment of NHS plans and policies, which would help protect the NHS from short term political pressures and policies that have not been sufficiently thought out.
Providing some additional funding to support early improvements and commissioning a review of future sustainability similar to the 2021 Wanless review.
This recommendation is summarised in box 2.
Recommendations
The government in post after the election should declare a national health and care emergency, calling on all parts of society to help improve health, care, and wellbeing and, in effect, relaunch the NHS with the active participation of the whole of society. This would involve:
A commitment to the NHS and its founding principles and engaging all parts of society in a renewed vision and plan for health, care, and wellbeing
Creating a cross-government and cross-sector strategy for health, care, and wellbeing
Developing better ways to connect patients, the public, and community groups with the NHS, particularly at local level
Giving immediate priority to tackling inequalities in access and outcomes, with particular attention on the disadvantage and racism suffered by ethnic groups both as patients and staff of the NHS
Establishing an Office for NHS Policy and Budgetary Responsibility to provide an independent and expert assessment of NHS plans and policies
Providing some additional funding to support early improvements and commissioning a review of future sustainability
Footnotes
This article is part of The BMJ Commission on the Future of the NHS. The purpose of our NHS Commission is to identify key areas for analysis, lay out a vision for a future NHS, and make recommendations as to how we get there
Competing interests: We have read and understood The BMJ policy on declaration of interests and declare that we have no competing interests.
Contributors and guarantor: All authors contributed to the research, writing, review, and editing of this manuscript. NC is the guarantor. All authors were members of the BMJ commission.
Provenance and peer review: commissioned; externally peer reviewed.
The BMA, which owns The BMJ, grants editorial freedom to the editor in chief of The BMJ. The views expressed in the papers of the BMJ Commission on the Future of the NHS, are those of the authors and may not necessarily comply with BMA policy. The BMJ convened this commission, which was chaired independently by Victor Adebowale, Parveen Kumar, and Liam Smeeth. The BMJ was responsible for the peer review, editing, and publication of the papers of the commission.
All of the articles in this commission are available at https://www.bmj.com/nhs-commission.
{kind=link}