Article Text

Statistics from Altmetric.com
Description
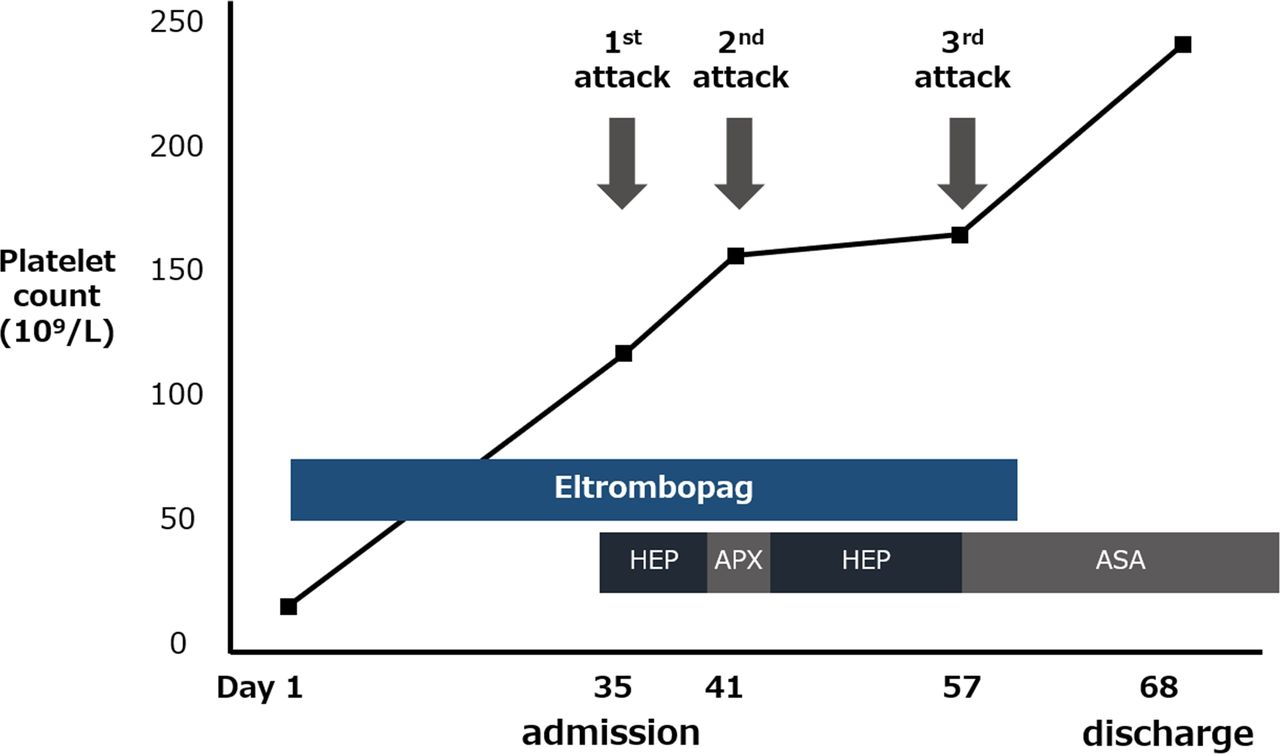
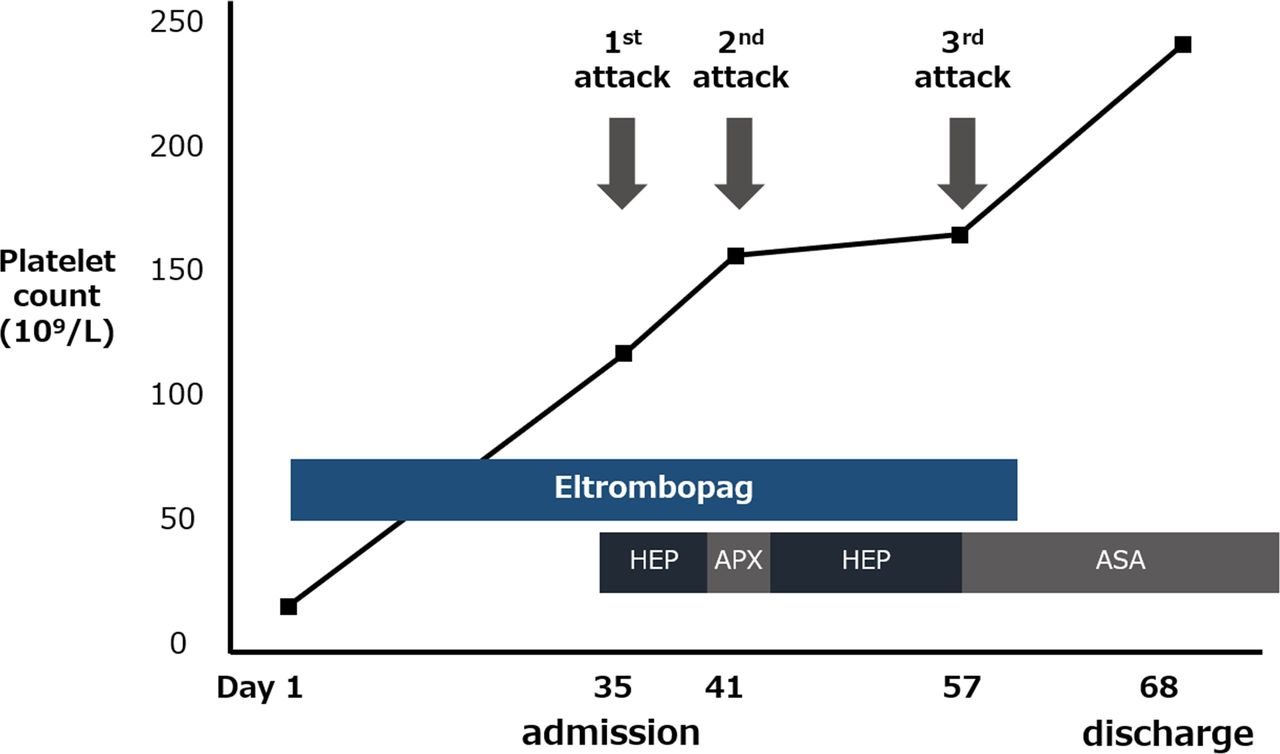
A 75-year-old woman was diagnosed with primary idiopathic thrombocytopenic purpura (ITP). The patient had no history of thrombotic events. We could not administer the standard dose of glucocorticoid because of her old age, and her platelet count did not increase with glucocorticoid monotherapy. According to the international guidelines,1 intravenous immunoglobulin (IVIg) therapy is recommended in this situation. However, we could not choose IVIg therapy because of the insurance system in our country; therefore, eltrombopag (12.5 mg/day) was administered. The patient did not undergo splenectomy. Left hemiplegia developed 1 month after the initiation of eltrombopag. The patient’s platelet count was 116×109/L on admission. In addition, brain MRI showed multifocal cerebral infarctions in the right hemisphere (figure 1A,B). We suspected cardiogenic thrombosis from her imaging findings. Therefore, we started intravenous heparin, followed by apixaban; however, a follow-up MRI showed recurrent cerebral infarction (figure 1C,D). After a second ischaemic attack, intravenous heparin therapy was administered again, but another ischaemic attack occurred (figure 2). No antiphospholipid antibodies or concomitant inherited risks for thrombosis were detected. Eltrombopag was suspected to be responsible for the stroke. No subsequent recurrence of stroke existed after eltrombopag was stopped. Eventually, acetylsalicylic acid was administered to prevent stroke.

(A, B) Diffusion-weighted MRI (DW-MRI) on admission (day 35) shows multiple high-intensity spot lesions in the right frontal lobe. (C, D) DW-MRI on day 41 shows other infarct lesions on both hemispheres of the brain (arrow).
{kind=link}
{kind=link}
Clinical course of the patient. The patient developed cerebral infarction three times during the use of eltrombopag. After eltrombopag was discontinued, the patient did not experience any recurrent stroke. APX, apixaban; ASA, acetylsalicylic acid; HEP, heparin.
Studies have shown that ITP could cause stroke. The increased level of platelet microparticles in patients with ITP could be associated with the development of thrombosis.2 However, some studies have suggested that eltrombopag causes thrombosis, including cerebral infarction.3 The risk of eltrombopag-induced adverse effects should be considered in patients with ITP, who develop cerebral infarction.
Learning points
In patients with idiopathic thrombocytopenic purpura (ITP), the risk of stroke should be considered.
In addition, stroke could be caused after ITP treatment.
Eltrombopag could be a cause of thrombosis, including cerebral infarction, even when the platelet count is normal.
Ethics statements
Patient consent for publication
Footnotes
Contributors YM was a major contributor in writing the manuscript. DY and YT also treated the patient, and interpreted the patient data. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.