Article Text

Statistics from Altmetric.com
Description
A 28-year-old healthy woman, with two previous pregnancies with no intercurrences and healthy children, was send to our prenatal diagnosis centre due to a suspicion of congenital heart disease (CHD) at the third trimester. Actual pregnancy uneventful but with late beginning of fetal-maternal surveillance, at the second trimester. At the fetal ultrasound, she presented: thymus size above the 90th percentile; discrete chambers disproportion, with a smaller left side; an atrial septal aneurysm (ASA) (figure 1; video 1); a complete aortic arch, apparently without narrowing but with retrograde flow in 3VT (figure 1; video 1) and sagittal views and a conditioned left atrioventricular (AV) flow (figure 1; video 1), seemingly due to the aneurysmatic bulging into the left atrium. Ultrasound surveillance was made every 2 weeks, with no significant changes till delivery, which was vacuum-assisted at 39 weeks. The newborn was 3395 g, had an Apgar index of 9/10. He stayed at the neonatal intensive care unit because of the suspicion of CHD and for foramen ovale closure surveillance. CHD was not confirmed, with the only altered echocardiographic finding being patent foramen ovale. He was dismissed at the sixth day of life. At the third month of cardiology appointment, he was asymptomatic, with normal growing curves. Ecocardiographic evaluation showed proportional cardiac chambers, a restrictive ostium secundum atrial septal defect, with no other abnormalities and the eletrocardiographic evaluation was normal. A follow-up appointment was scheduled for the second year of life.

{kind=link}
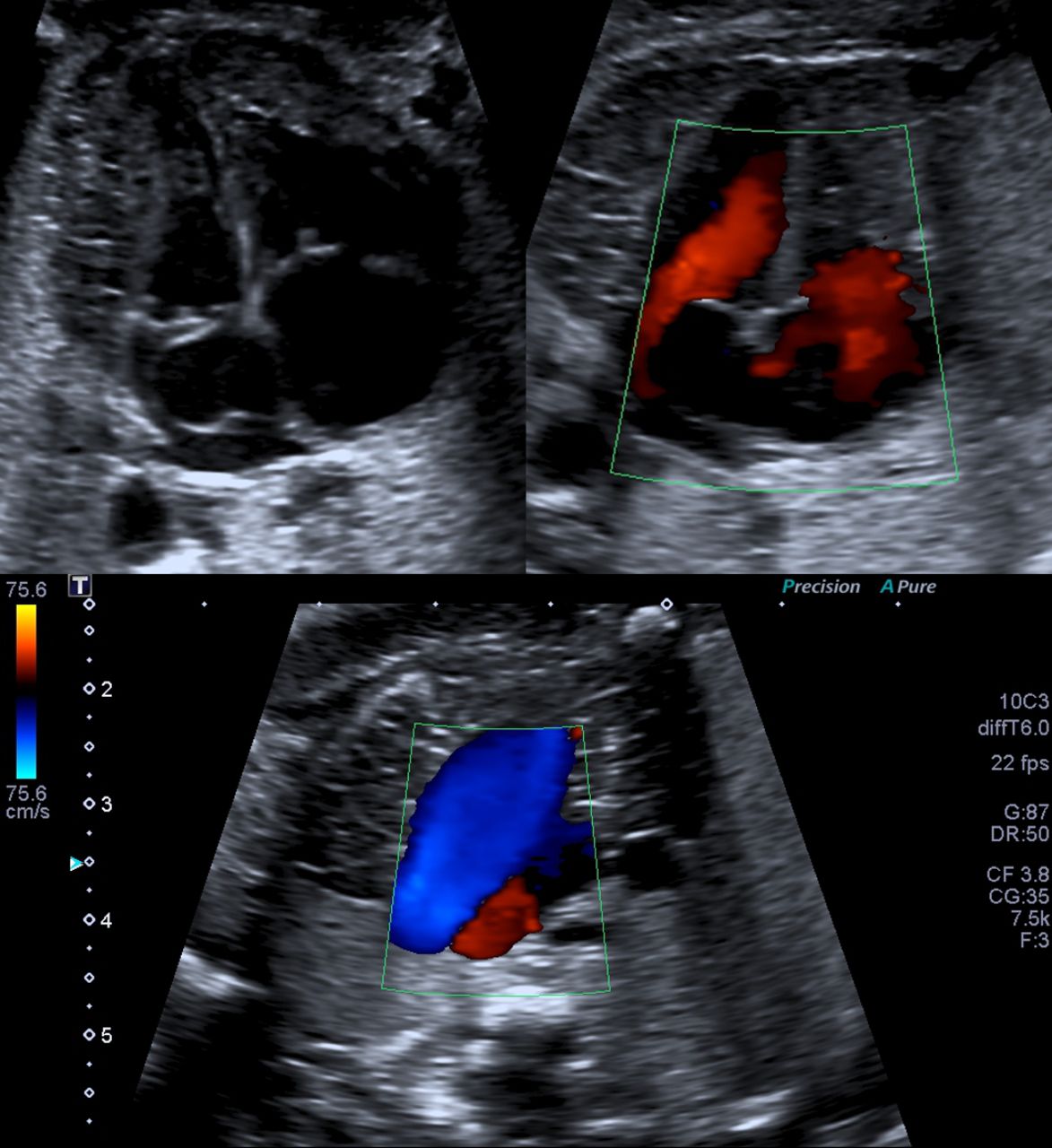
Top left: 4 chamber view (4CV) - the atrial septal aneurysm; discrete chambers disproportion, with predominant right chambers. Top right: colour Doppler in 4CV - limited flow through the mitral valve. Bottom: 3 vessel trachea (3VT) view - retrograde flow in the aortic arch.
In this report, we present fetal ultrasound images of retrograde flow in the aortic arch and cardiac chambers disproportion, with predominant right chambers (figure 1; video 1). Considering these findings, especially the first, differential diagnosis includes, mainly, causes of severe left side structural heart disease, such as hypoplastic left heart, aortic stenosis/atresia or aortic coarctation, with this last hypothesis being of difficult prenatal exclusion.1 2 In this case, the only cardiac finding, besides the previously mentioned, was an ASA with no other structural abnormality.
ASA is an abnormal large structure at the level of the foramen ovale that corresponds to a redundant septum primum which has an excessive excursion into the left atrium. The information regarding this finding in the fetus is scarce. Frequently it is described as an uncommon condition, although in one large study a prevalence of 7.6% was reported.3 An association between ASA and arrhythmias have been reported in several studies, with some reports identifying an unexpected high incidence (up to 70%) of ASA in fetuses referred for evaluation of arrhythmias.4 5 However, ASA usually is not a pathological condition, being self-limited, with some authors defending that it should be considered benign and transient.3 Nevertheless, in cases where there is a severe bulging of the redundant septum primum into the left atrium, it can cause a compromise to the flow through the mitral valve, creating the appearance of ventricular disproportion, with a small left ventricle. This flow compromise can be significant to the point of causing a retrograde flow in the aortic arch, raising the suspicion of an important left side cardiac structural disease. After delivery, in most of the cases, because of the physiological vascular modifications, there is a normalisation of the ventricular size and a repositioning of the atrial septum.6
Learning points
Aortic arch retrograde flow is a predictor of a left side structural heart disease, usually associated with a reserved prognosis.
It is important to keep in mind the possibility for other diagnosis with different prognosis, such as the atrial septal aneurysm, an usually benign cardiac finding.
ASA is an hypothesis that should be considered and excluded due to its implications in prenatal diagnosis counselling, as it can mimic a left side structural heart disease.
Footnotes
Contributors All authors have read and approved the manuscript. All authors contributed to the work according to ICMJE requirements for authorship. All authors declare that the manuscript is an original work that has not been submitted to another journal or conference. ACS was responsible for planning, conception, bibliographic research, reporting, design and interpretation of data. MB was responsible for planning, conduct, conception, acquisition of data and interpretation of data. PM was responsible for planning, conception, conduct and interpretation of data
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.