Article Text

Statistics from Altmetric.com
Description
A 2-year-old developmentally normal girl presented to us with a history of deviation of angle of mouth to right only during crying, persisting from neonatal period. She was born at term by normal vaginal delivery to a primigravida mother with a birth weight of 2.2 kg and smooth perinatal transition. Parents noticed asymmetry of face from neonatal period visible only during crying, which disappeared when she was consoled, without any drooling, regurgitation of feeds or poor sucking. There is no history suggestive of any other neurological or systemic abnormality in index case or in family.
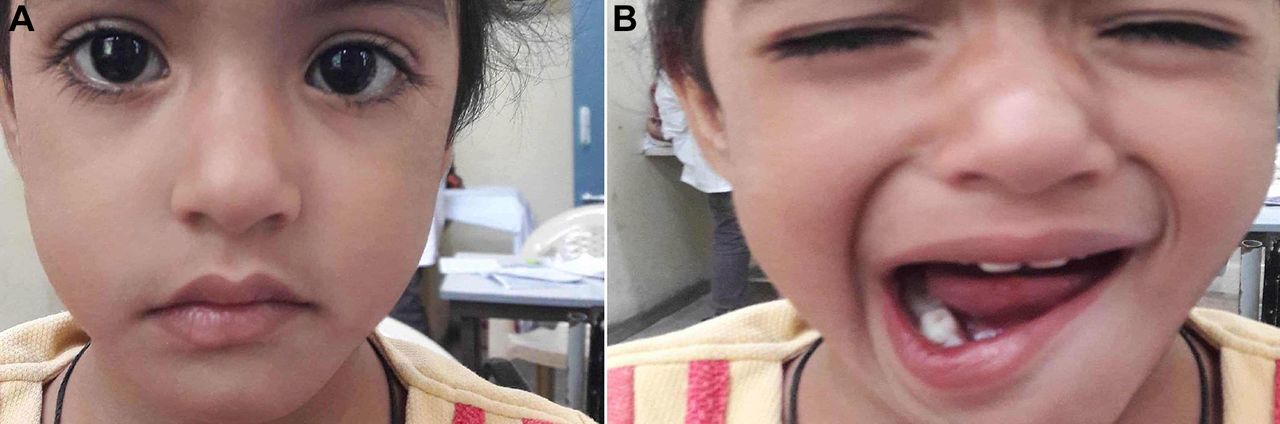
Local examination revealed thinning of lower lip near left angle of mouth on palpation. There was no facial asymmetry while the child was calm (figure 1A), however, on crying there was deviation of the angle of mouth downwards and towards right side (figure 1B). There was no evidence of hypoplasia or weakness of any other facial or extraocular muscle. There was no dysmorphism, facial or ocular deformity and any overt evidence of systemic disease. Neurological examination of this alert, conscious and cooperative child revealed normal power, tone and deep tendon reflexes. There was no evidence of any cranial nerve palsy, cerebellar signs or synkinesis. Rest of systemic examination was unremarkable.

{kind=link}
(A) Normal bilateral facial symmetry when child is calm. (B) Deviation of angle of mouth downwards and towards right while crying.
A diagnosis of congenital hypoplasia of depressor anguli oris muscle (CHDAOM) of left side was made and parents were counselled about the benign nature of the condition. CHDAOM is a rare entity affecting 3–6/1000 live births and often mimics facial nerve palsy.1 The depressor anguli oris muscle fibres originate from oblique line of mandible and are attached to the lower lip. It is innervated by buccal and mandibular branches of ipsilateral facial nerve and its function is to depress the ipsilateral corner of mouth and to evert the lower lip. In CHDAOM, the angle of mouth and mandible are pulled down on normal side due to unopposed action of DAOM, while no movement on hypoplasia side. The affected lower lip may look thinner because of the lack of eversion and muscle agenesis. The exact cause of CHDAOM is unknown. The patient usually presents in the neonatal period with asymmetric crying facies but with symmetrical forehead wrinkling, eyelid closure and nasolabial furrowing in contrast to facial nerve palsy. Diagnosis is predominantly clinical; electrophysiological studies may demonstrate normal nerve conduction time to mentalis and orbicularis oculi muscles.2 CHDAOM may be associated with other anomalies like congenital heart disease (40%–50%), head and neck anomalies (45%–50%), skeletal defects (22%) and genitourinary anomalies; as well as along with syndromes like CATCH22, Cayler cardiofacial syndrome, vertebral defects, anal atresia, cardiac defects, tracheo-esophageal fistula, renal anomalies, and limb abnormalities (VACTERL) association and DiGeorge syndrome.3 Investigations for the same are indicated only if clinical examination is abnormal. Differential diagnoses include birth trauma to face, facial nerve palsy and congenital absence of facial nerve nucleus. Cosmetic issues may be present, but usually becomes unnoticeable by adulthood, nor does it interfere with either speech or feeding. This correct clinical identification of CHDAOM prevents the child from being subjected to unnecessary investigations, but associated anomalies must always be kept in mind and excluded, if indicated on clinical examination. Parental counselling is of paramount importance.
Learning points
Congenital absence of depressor anguli oris is a rare cause of facial deviation in infancy and childhood.
History and clinical examination are crucial for diagnosis and avoid unnecessary investigations.
It usually becomes unnoticeable by adulthood and parental counselling is of paramount importance.
Footnotes
Contributors DB: patient management, literature review and preparation of the initial draft of the manuscript. SKA: clinician-in-charge, critical review of the manuscript for important intellectual content and final approval of the version to be published. RS: patient management, literature review and preparation of the initial draft of the manuscript. BB: critical review of the manuscript for important intellectual content and final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.