Article Text

Statistics from Altmetric.com
Description
A 62-year-old woman was referred by her general practitioner to the rapid access transient ischaemic attack (TIA) clinic. She had persistent atrial fibrillation (AF) with one previously failed DC cardioversion and two previously failed AF ablations. She was anticoagulated with warfarin. The patient's medical history included hiatus hernia, bilateral shoulder arthritis and migraines. She underwent redo catheter ablation for AF, which was complicated by right common femoral artery pseudo aneurysm and haematoma and hence warfarin was withheld. Two weeks later she developed painless visual loss in her right eye, appearing as a crescent-shaped black spot. Her visual acuity was excellent measuring 6/5 in the right and 6/4 in the left at presentation, with no visual field defects. She had completely clear media, but her fundal examinations showed three cotton wool spots in her right eye (figure 1) and also two in her left eye (figure 2). A fluorescein angiogram (figures 3 and 4) showed capillary changes, secondary to small areas of retinal infarctions. Her CHADS2-VASc score was 3. She was restarted on warfarin.
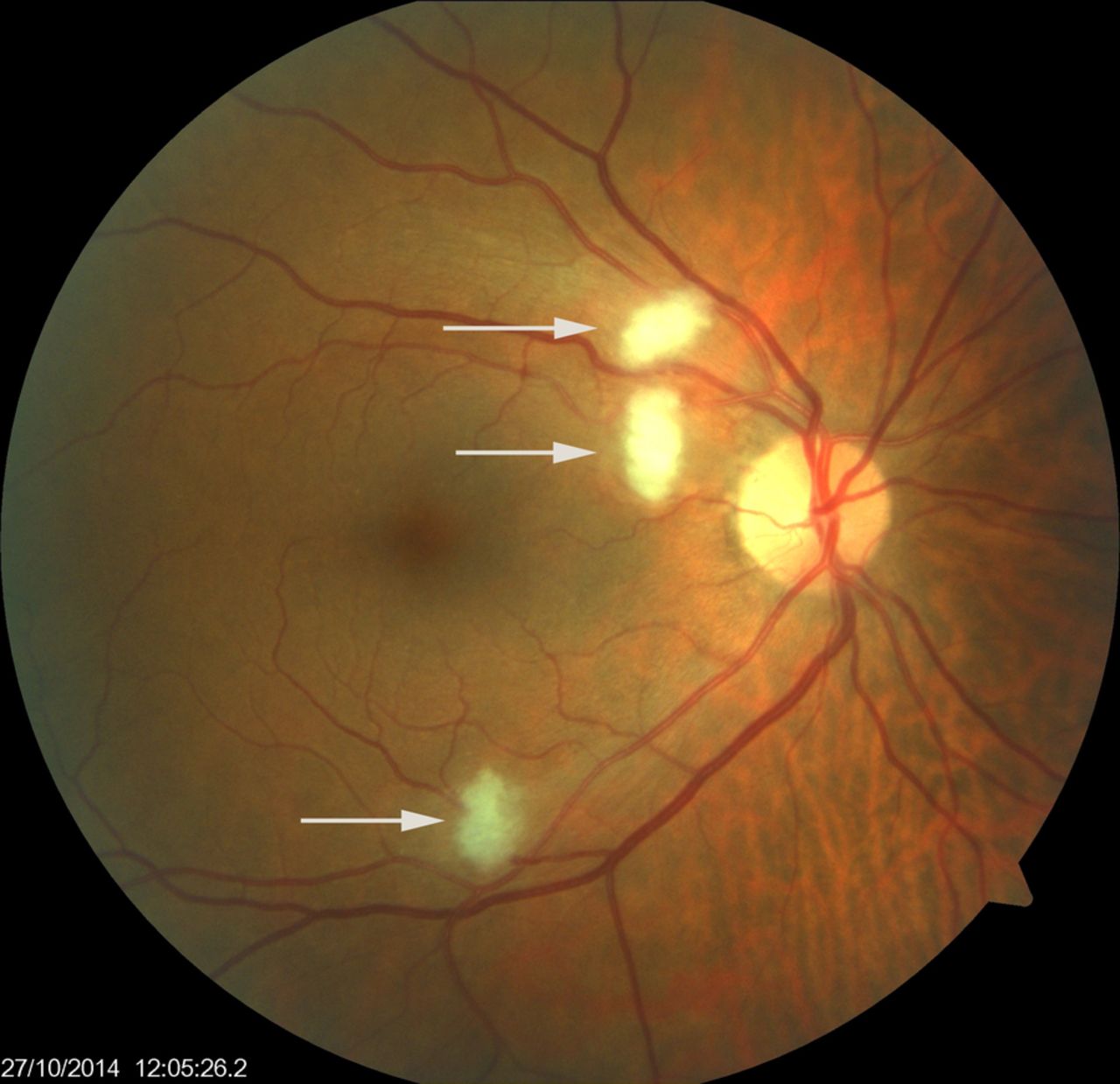
Ophthalmoscopic view of the retina showing three cotton wool spots in her right eye.

Ophthalmoscopic view of the retina showing two cotton wool spots in her left eye.

Fluorescein angiogram of the right eye showing capillary changes, secondary to small areas of retinal infarctions.

Fluorescein angiogram of the left eye showing capillary changes, secondary to small areas of retinal infarctions.
It appeared that she had suffered multiple microemboli to both retinae following AF ablation. AF ablation is extremely thrombogenic per se. Catheter ablation is associated with a transient increase in thrombotic risk, particularly in the periprocedural period.1 Well-acknowledged risks associated with AF catheter ablation include pulmonary vein stenosis, TIA and stroke.2 Cotton wool spots in this patient were an unforeseen complication following such a procedure, as opposed to larger arterial occlusion. Patients with amaurosis fugax may not seek medical attention because of its self-limiting nature. AF ablation procedures may therefore cause more cotton wool spots than we are aware of, in contrast to central retinal artery occlusion. The incidence of cotton wool spots post-AF ablation could only truly be measured if all patients had a fundus examination after the procedure. Our literature search did not reveal any previous reports of retinal microemboli following AF ablation. At the 6-month follow-up visit she had experienced no further episodes of visual loss and fundal examination showed complete spontaneous resolution of cotton wool spots (figures 5 and 6).

Ophthalmoscopic view of the retina showing complete spontaneous resolution of cotton wool spots in the right retina.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ophthalmoscopic view of the retina showing complete spontaneous resolution of cotton wool spots in the left retina.
Learning points
Bilateral cotton wool spots post atrial fibrillation (AF) ablation are self-limiting.
The presence of cotton wool spots should trigger thorough investigation to identify the underlying aetiology.
The incidence of cotton wool spots post-AF ablation could only truly be measured if all patients have a fundus examination after the procedure.
Footnotes
Contributors LRGS was involved in the case report and identifying references for learning points. RN was involved in case discussion; MJHR in formulating the idea for the case report, discussion and amalgamating learning points.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.