Article Text

Abstract
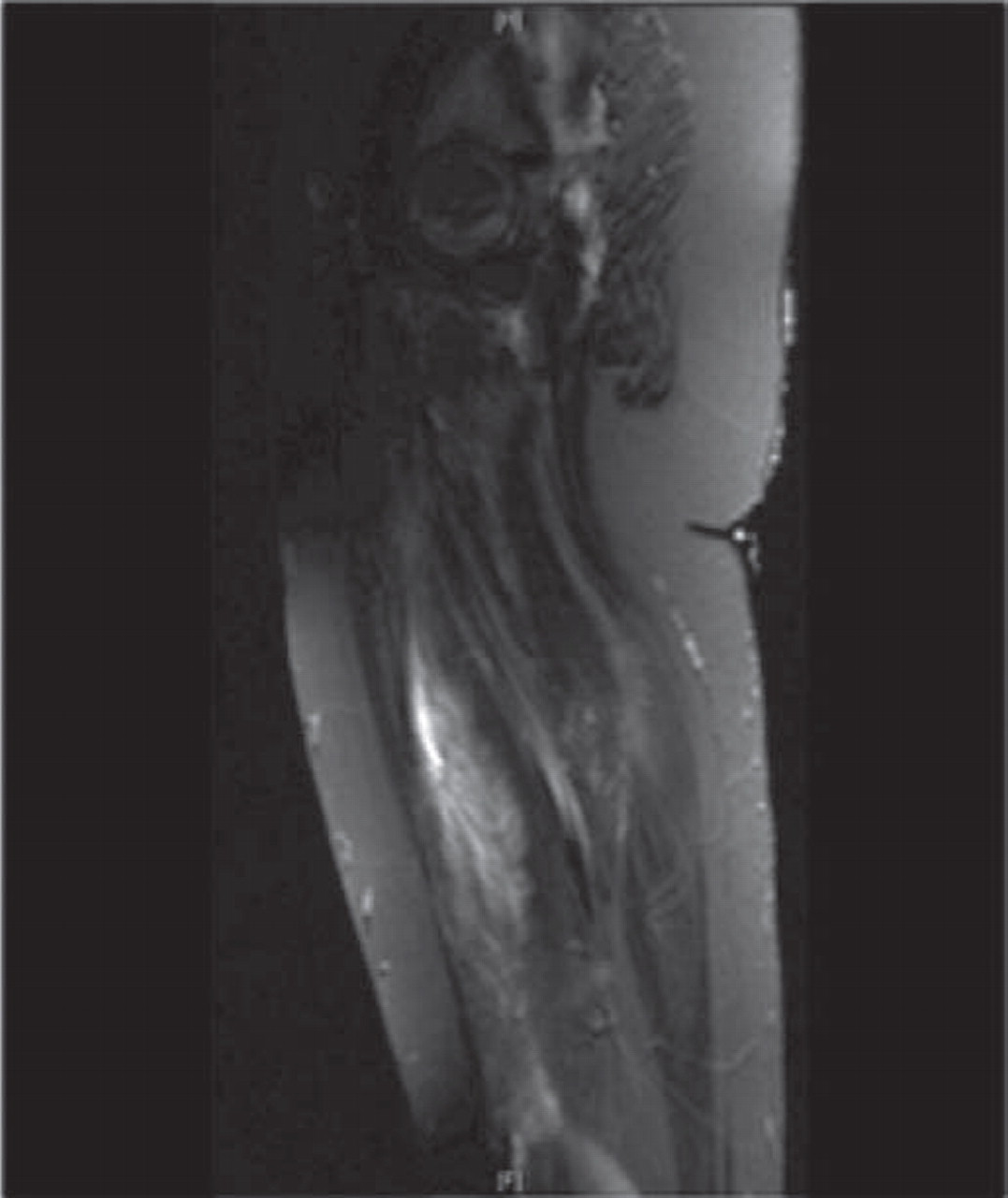
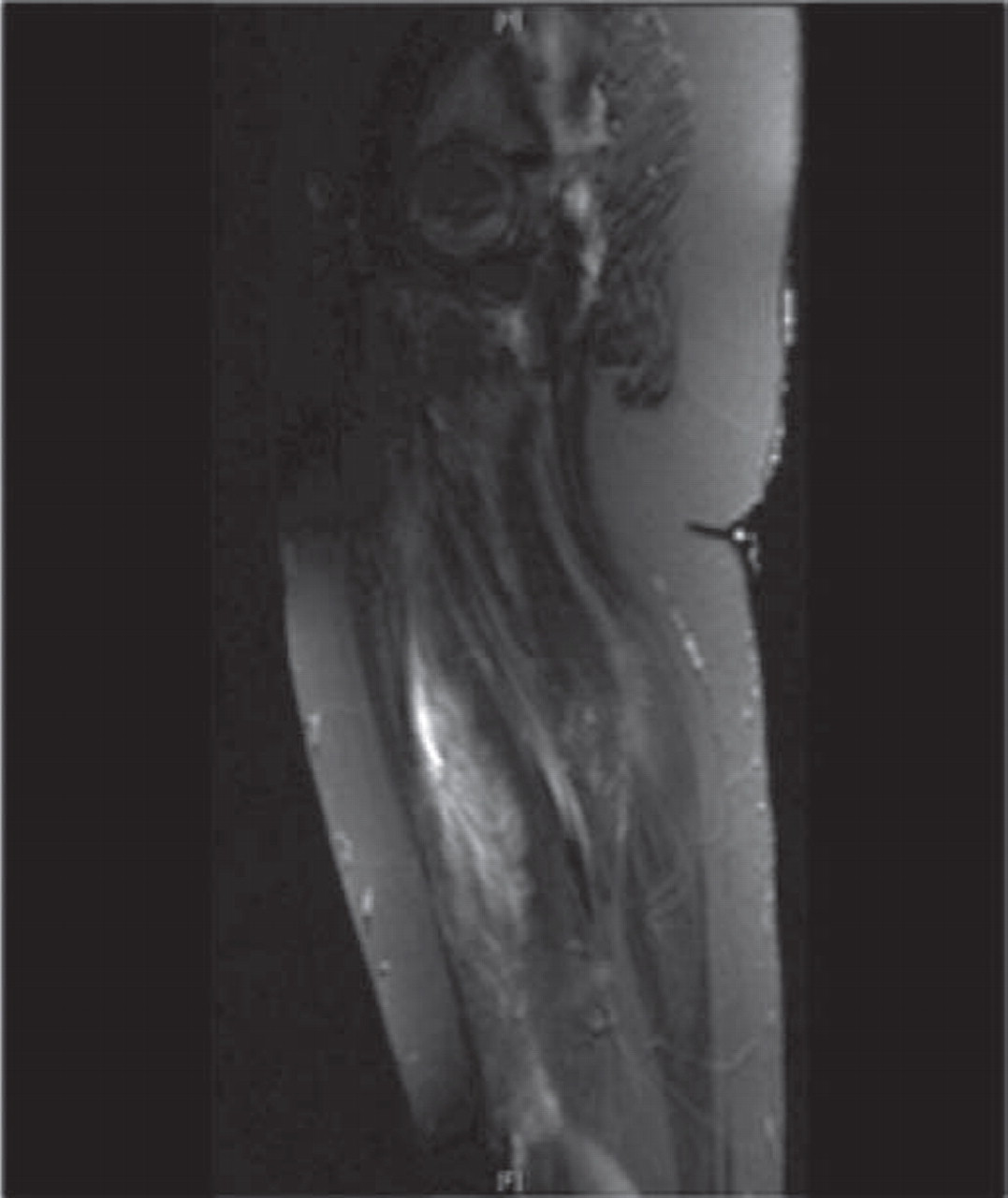
Case history A 13 year old boy of African origin was admitted with an acute onset of fever, cough and right leg swelling. He was born in Malawi and moved to UK at 3 years of age. Findings on examination included a temperature of 39°C, oral candidiasis, crepitations on the right side of chest. His right calf was swollen, erythematous and tender. There was evidence of proximal muscle weakness. He was started on IV Cefuroxime for possible LRTI. Tests included: C reactive protein (345 mg/dl), normal doppler scan of lower limbs, CD4 count (10 cells/mm3, CD4% of 1), HIV viral load (>1 million copies/ml), CK 453 U/l (30–175 U/l) and blood culture was positive for Streptococcus pneumoniae. MRI thighs showed inflammation of right quadriceps muscles. A presumptive diagnosis of acute bacterial myositis was made and IV Clindamycin was added. After 10 days, he was discharged home on oral antibiotics. He was readmitted 5 days later with Varicella and recurrence of right leg swelling. A repeat MRI showed inflammation of right calf muscles in addition to the thigh muscles (figures 1 and 2). HAART was started and the myositis improved with 3 weeks of intravenous antibiotics. Proximal myopathy gradually improved on HAART.

MRI left lower limb shows muscle edema
{kind=link}
{kind=link}
MRI left lower limb shows muscle edema
Discussion Muscle involvement in HIV infection can take the form of myopathy, infective or infiltrative lesions and rhabdomyolysis. Bacterial myositis can be pyomyositis or acute bacterial myositis. Pyomyositis is an acute bacterial infection of skeletal muscle with localised abscess formation. Staphylococcus aureus accounts for 75–90% of these infections. Acute bacterial myositis is an infection within the muscle, but inflammation extends diffusely through muscle groups without distinct abscesses. Group A streptococci account for majority of these infections. MRI is the optimum imaging modality and treatment is with intravenous antibiotics and surgical drainage if there is a pus collection.
Conclusion Acute bacterial myositis should be considered in a child presenting with fever, leg swelling and muscle weakness. This child appeared to have both an acute bacterial myositis which improved with antibiotics and a chronic proximal myopathy which improved more slowly on antiretrovirals.