



At the onset of the coronavirus disease pandemic (COVID-19), university students who were quarantined on campus and in communal housing were at elevated risk of infection compared with those who could isolate non-communally. 1 Thus, at many universities, including the setting of the present study, the only students permitted to remain in campus housing early in the pandemic were those who were housing insecure Reference Cox, Henwood and Rodnyansky2 —that is, those who were at risk of losing housing or who did not have stable, safe, adequate, and affordable housing. Housing insecure individuals are frequently underrepresented in disaster research, due to measurement by household Reference Malmin3 or with general university samples. Reference Tkachuck, Schulenberg and Lair4 In the United States (US), both international and US national students who lacked stable housing continued living in on-campus communal housing (eg, dormitories). During COVID-19 or any disasters that necessitate both evacuation and international travel bans, international students are at high risk of housing insecurity. Asian international students were at further risk of pandemic-related harm due to increased discrimination against Asians/Asian Americans during COVID-19, ranging from shunning them to verbal harassment to physical attacks—for example, spitting or coughing on them. Reference Gover, Harper and Langton5,Reference Jeung6 Given the intersectional pandemic vulnerabilities for individuals in communal housing who are housing insecure and/or international students and/or Asian (American), equitable and effective pandemic preparedness and response hinge upon a better understanding of preparedness amongst these populations.
Individual disaster preparedness refers to specific behaviors, such as emergency planning and obtaining necessary supplies for a disaster. Reference Malmin3,Reference Weber, Schulenberg and Lair7 Even within disaster-prone regions, preparedness varies widely, and underpreparedness is common. Reference Malmin3 Pandemic preparedness rates for the aforementioned intersectionally vulnerable populations are understudied; pre-COVID-19 research found that international students in the United States were less prepared for natural hazards than US national students, Reference Tkachuck, Schulenberg and Lair4 although this may be due to unfamiliarity with local hazards—a circumstance less applicable to pandemics.
Predictors of Preparedness
Empirical findings about the effects of self-efficacy and risk perception on preparedness are mixed. Reference Wachinger, Renn, Begg and Kuhlicke8,Reference Lechowska9 Disaster self-efficacy (ie, perceived preparedness, confidence in responding, response efficacy) is one’s perceived ability to respond effectively to a specific hazard when it occurs. Both inverse and positive relationships have been found between disaster self-efficacy and disaster preparedness. Reference Wachinger, Renn, Begg and Kuhlicke8 Risk perception is an assessment of likelihood that a specific hazard will occur (ie, perceived likelihood) and perception of how severe a hazard would be, if it were to occur (ie, perceived severity). Reference Witte10 While fear and risk perception are often equivocated in other studies, Reference Wachinger, Renn, Begg and Kuhlicke8 or even measured within the same self-report scales, Reference Krzyzanowski, Terry and Williams11 theory and evidence show that risk perception is not equivalent to fear, worry, or concern, because people can, and often do, accurately estimate future hazard’s likelihood and severity, while reporting little fear about such hazards. Inconsistent findings about the direction of the association between risk perception and preparedness are partly due to questionnaires measuring fear and risk perception within the same item and/or factor. Reference Wachinger, Renn, Begg and Kuhlicke8,Reference Lechowska9,Reference Krzyzanowski, Terry and Williams11,Reference Conway, Woodard and Zubrod12 Even when risk perception is measured independently of fear, effects on preparedness vary by disaster type. Reference Weber, Schulenberg and Lair7
The Extended Parallel Process Model (EPPM; Supplementary Figure S1) is a social psychology theory explaining individual responses to threats, Reference Witte10 which has been applied to disaster preparedness as an explanation for the mixed empirical findings. Reference Weber, Schulenberg and Lair7 The EPPM posits that self-efficacy and accurate risk perception are both necessary for effective response, whereas fear is not. Reference Witte10 In theory, individuals with high self-efficacy but low risk perception are essentially overestimating their preparedness and therefore not taking sufficient preparedness actions. Further, according to the EPPM, fear is highest among individuals who have high risk perception but low self-efficacy; such individuals take the threat seriously (eg, high perceived severity of COVID-19), but because they lack self-efficacy, they do not engage in productive actions (eg, doing pandemic preparedness and response behaviors [PPRBs]). Instead, their behaviors are aimed at reducing fear (eg, through denial about the pandemic’s severity).
Limitations of the EPPM and current empirical literature include the lack of attention to disaster collective efficacy, or an individual’s belief that actions by community members will be successful in preventing and reducing the impact of a hazard on the community. The link between collective efficacy and preparedness has rarely been studied for any hazard; one of the few studies on this topic found a 1-item measure of social cohesion (a collective efficacy component) longitudinally predicted hurricane preparedness. Reference Mash, Fullerton and Morganstein13 Considering the collective nature of PPRBs, like social distancing precautions and vaccination, research is needed to examine collective efficacy as a predictor of PPRBs.
The present study tested the EPPM in the context of the early months of COVID-19, with an additional collective efficacy component (Supplementary Figure S1). To promote equity in disaster preparedness, we longitudinally surveyed an intersectionally disaster-vulnerable sample of university students and their partners, who were international, Asian, and/or housing insecure. Given the mixed empirical findings for self-efficacy and risk perception as predictors of preparedness, our hypotheses about these 2 predictors directly stemmed from the EPPM theory. Augmenting this, we theorized that collective efficacy would have the same directions of effects as self-efficacy. We explored whether it would outweigh self-efficacy as a predictor of preparedness, given its relevance for the collective nature of PPRBs. Hypothesis 1 (H1): Within- and between-person perceived severity of the COVID-19 pandemic, self-efficacy, and collective efficacy will positively predict PPRBs. Hypothesis 2 (H2): Within- and between-person fear of COVID-19 would negatively predict PPRBs.
Methods
Participants and Procedure
The study was approved by the IRB at The University of Mississippi. Participants were recruited by responding to announcements in the e-newsletter of the university’s international programs office, which invited individuals “quarantined in [university] campus housing” to participate. At that time, approximately 200 housing insecure students were permitted to remain in campus housing, most of whom were international students, unable to return to their countries of origin. Participants completed an online survey for 14 waves spanning May–October 2020. After baseline completion (N = 84), unless the participant requested to withdraw (n = 1), researchers sent participants the survey every 7 days for 14 weeks. This resulted in a final sample of N = 54 who completed ≥ 2 of 14 waves, for a total of 560 observations. Participants were paid $5 per wave. Table 1 shows participant demographics; over half the sample identified as international students (77.8%), Asian/Asian American (55.6%), housing insecure (79.6%), or heterosexual/cisgender (75.9%).
Table 1. Participant demographics
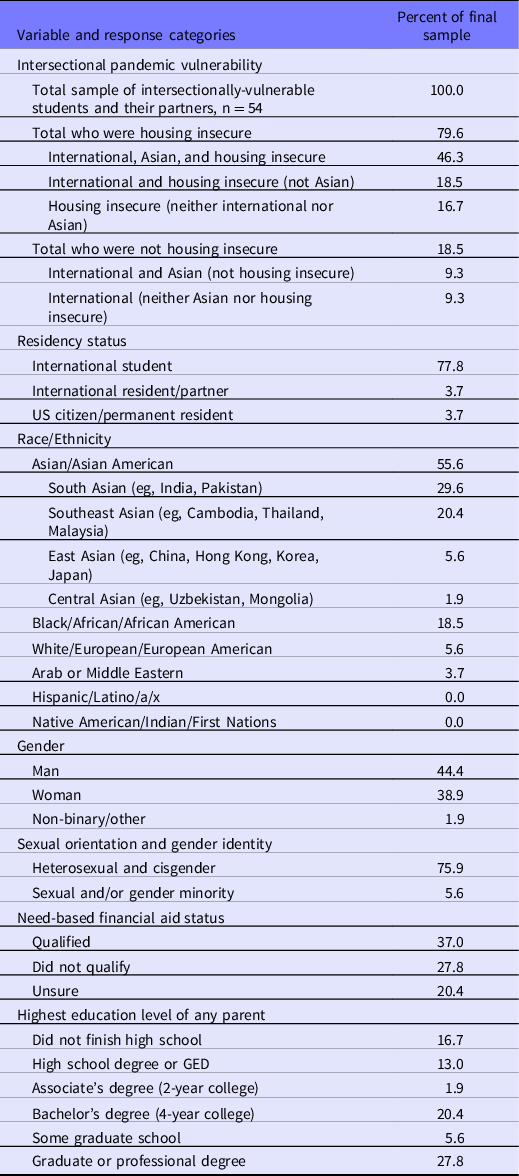
Percentages that do not total 100 are due to missing data.
Measures
Other than baseline-only demographic questions (see Table 1), participants were asked the same questions each week, all of which are described in detail in Online Supplementary File S3. A 3-item sum score for Pandemic-Specific Self-Efficacy included 2 items adapted from the PhenX Toolkit COVID-19 Protocol Reference Krzyzanowski, Terry and Williams11 and 1 item on confidence responding to natural hazards, Reference Tkachuck, Schulenberg and Lair4 adapted for COVID-19. Responses were on a 5-point Likert-type scale. Sum scores range from 3–15, and higher scores indicate greater pandemic self-efficacy. Pandemic Collective Efficacy was assessed with 5 items from the United Action factor of the Community Collective Efficacy Scale, Reference Carroll, Rosson and Zhou14 adapted to refer specifically to the COVID-19 pandemic. Response options were on a 5-point Likert-type scale. Total sum scores range from 5 to 25, with higher scores indicating greater perceived pandemic collective efficacy.
Perceived Severity, in combination with perceived likelihood, constitutes risk perception, per our definition in accord with the EPPM. Because the pandemic was ongoing, we measured the severity component of risk perception but not the likelihood component. As described above, risk perception (perceived likelihood + perceived severity) has often been measured in combination with items or scales on negative emotions (fear, worry, or concern) for both natural hazards Reference Wachinger, Renn, Begg and Kuhlicke8 and pandemics. Reference Krzyzanowski, Terry and Williams11 To clarify the mixed findings in the literature on fear and risk perception, and in accord with the EPPM theory, we wanted to measure risk perception separately from fear, yet at the time of this study, no established scale was known to the researchers for measuring these constructs separately regarding a current, ongoing hazard. Thus, perceived severity was assessed with a question developed for this study: Compared to the flu (influenza) outbreaks each year, how severe do you think the COVID-19 outbreak is? Responses were on a 5-point Likert-type scale, ranging from 1 (“less serious than the yearly flu outbreak”) to 5 (“much more serious than the yearly flu outbreak”); higher scores indicated a greater perceived severity.
Fear of the Pandemic was assessed using the first 5 items from the Coronavirus Threat Questionnaire. Reference Conway, Woodard and Zubrod12 This scale clearly measures how much worry, anxiety, and fear the respondent feels about COVID-19 (see S3) and does not assess perceived likelihood and severity of COVID-19. The scale’s name reflects the frequent, poor differentiation between the constructs of risk perception (an assessment of likelihood and severity) and fear (an emotional reaction). For example, 1 item is, “I am afraid of the coronavirus (COVID-19).” The sixth item appears to measure preparedness and was omitted here due to poor face validity and poor factor loadings in the original psychometric study. Reference Conway, Woodard and Zubrod12 Responses are on a 5-point Likert-type scale. Sum scores for our 5-item version range from 5 to 25; higher scores indicate a greater fear of COVID-19.
Pandemic Preparedness/Response Behavior (PPRB) was measured based on guidelines for individual COVID-19 PPRBs from the Centers for Disease Control and Prevention (CDC). 15 Instructions were, “In the past 7 days, have you…? (Check all that apply.)” followed by a list of behaviors involving social distancing (8 items), sanitation (4 items), and other actions (6 items, eg, “Read or watched guidelines for what to do to prevent COVID-19”). Endorsed behaviors were scored 1, then 5 social distancing items were reverse scored. Items were summed, with higher scores indicating a greater past-week engagement in PPRBs.
Data Analysis
All analyses were conducted using R statistical software. Data cleaning involved merging data sets from each wave, by participant ID number. Descriptive statistics across all observations were computed for the 54 participants who had participated in at least 2 waves. Using the nlme package, multilevel modeling (MLM) of PPRBs was conducted with random intercept models and data nested by participant. Fixed effect predictors were within- and between-person perceived severity (testing H1), self-efficacy (H1), collective efficacy (H1), and fear (H2).
Results
Descriptive statistics are shown in Table 2. All variables were approximately normally distributed, all skew ≤ |1.10|, all kurtosis ≤ |1.40|. Participants typically engaged in 7 out of 18, or less than half, of the behaviors recommended by the CDC weekly. Engagement in social distancing was low compared with the CDC guidelines, 15 with participants engaging in about 2 of 8 recommended social distancing behaviors weekly. For self-efficacy, collective efficacy, and fear, mean scores were moderate, meaning they corresponded to responses of 3 (“neutral”) on the 1–5 Likert-type scales. On average, the COVID-19 pandemic was perceived as more severe than the typical annual influenza outbreak.
Table 2. Descriptive statistics and multilevel model of pandemic preparedness and response behaviors
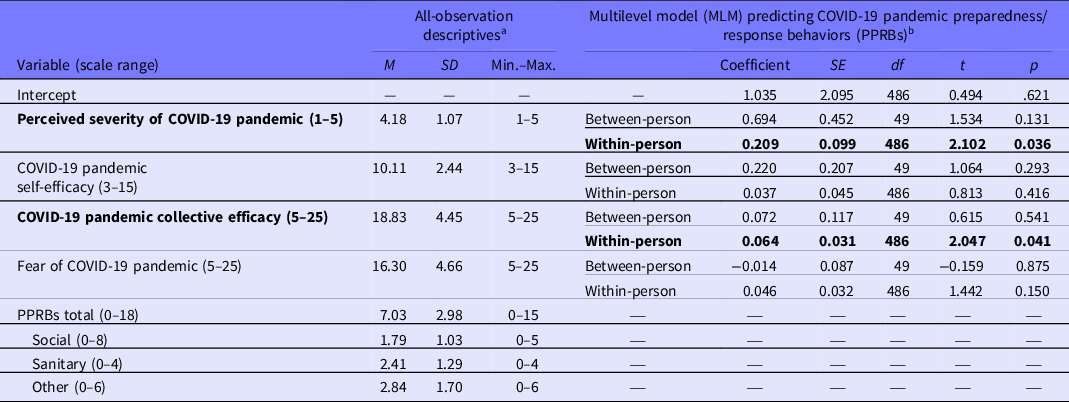
M, mean; SD, standard deviation; COVID-19, the coronavirus pandemic that began in December 2019.
a N participants = 54, N observations in descriptives = 547 to 560;
b N participants = 54, N observations in MLM = 544.
Fixed effects R 2 = .1335. Within-person scores were person-centered at zero. Between-person scores reflect overall means for each participant.
Results of the MLM testing H1 and H2 are also shown in Table 2 and depicted in Supplemental Figure S2. Altogether, the fixed effects (ie, effects of the hypothesized variables) accounted for 13.35% of the variance in the pandemic prevention behaviors total sum score, R 2 = .1335. Greater within-person perceived pandemic severity and greater within-person collective efficacy predicted greater PPRB (see Table 2). In other words, participants engaged in more PPRBs in the weeks they had greater perceived severity and/or greater collective efficacy. No between-person effects were significant nor were within-person effects of self-efficacy and fear significant (see Table 2). Post hoc sensitivity analysis showed that the MLM was sufficiently powered to detect small effects for all predictors.
Discussion
The within-person effects of perceived severity and collective efficacy on PPRBs show intersectionally disaster-vulnerable university students followed the recommended PPRBs (like social distancing, sanitation, and mask-wearing) to a greater extent during the weeks when they (1) had more confidence that collective action could reduce or prevent the harm of COVID-19 and (2) perceived the pandemic was more severe. Hypothesized effects of self-efficacy and fear on PPRBs were not supported. Supplemental Figure S2 shows the aspects of the theoretical model that were supported in our study.
Effects of collective efficacy may be related to the collective nature of PPRBs, which explicitly involve the entire community sharing in the responsibility and efforts to maintain social distancing. Disaster preparedness behaviors measured in prior research are typically individual or household-level actions (eg, assembling supplies, planning where to go during a tornado warning). Reference Malmin3,Reference Weber, Schulenberg and Lair7 In contrast, social distancing and mask-wearing involve mutual prevention efforts to aid the members of one’s own community, not just to prevent harm specifically to oneself. Confidence in collective action might therefore be key to mobilizing PPRBs involving mutual effort and mutual benefit.
The link between PPRBs and within-person perceived severity, but not fear, addresses several shortcomings of the disaster risk perception literature. One is that risk perception (perceived severity and perceived likelihood) and negative emotions about disasters (worry, fear) are often conflated in risk perception measures Reference Wachinger, Renn, Begg and Kuhlicke8,Reference Lechowska9,Reference Krzyzanowski, Terry and Williams11 and are conceptually indistinct throughout the empirical literature on disaster preparedness. Even when perceived likelihood has been measured specifically, findings have been mixed regarding the association of perceived likelihood with disaster preparedness, and these studies have largely measured only between-person differences at a single time point. Reference Tkachuck, Schulenberg and Lair4,Reference Weber, Schulenberg and Lair7 In contrast, the present study showed that perceived severity, controlling for fear, was positively associated with PPRBs at the within-person level. This suggests that risk perception fluctuates during a prolonged disaster, and its link to effective actions is contextual. Thus, application of the EPPM to chronic disasters should account for fluctuating perceptions over time.
Neither within-person nor between-person fear of COVID-19 was significantly associated with PPRBs. Fear and preparedness were hypothesized to be inversely related because of the EPPM theory that individuals experiencing a large-scale pandemic are either more afraid (high risk perception and low self/collective efficacy) or more prepared (high risk perception and high self/collective efficacy) but unlikely to be both (Supplementary Figure S1). While the lack of a significant association does not definitively support this assertion, fear also did not appear to have a positive effect on PPRBs. Taken together, findings on fear and risk perception support their differentiation as separate constructs, with different relationships to effective disaster preparedness and response.
Our findings are applicable to public health efforts surrounding disaster preparedness, prevention, and response. Equity in disaster policy and emergency management entails clear guidelines for individuals who cannot avoid known risk factors like housing insecurity. For example, stay-at-home orders during COVID-19 and recommendations to isolate in small households, coupled with international travel bans, resulted in conflicting guidelines for housing-insecure international students. The welfare of intersectionally disaster-vulnerable individuals must be an utmost priority when developing and disseminating guidelines, policies, and emergency management plans.
Furthermore, concentrated efforts to promote preparedness amongst intersectionally disaster-vulnerable populations are critical. Our findings suggest that collective efficacy messaging may be more impactful than self-efficacy-laden messaging, for students with housing insecurity, international students, and their partners. Policy-makers, university administrators, and disaster management leaders must acknowledge that fear is a normal reaction to a disaster, even more so for individuals at intersectionally high risk of disaster-related harm (eg, Asian international students with housing insecurity, quarantined communally during the COVID-19 pandemic). Simultaneously, such leaders must recognize fear is not necessary to spur effective action. Rather than stoking fear, accurate information should be disseminated about the likelihood of a hazard occurring and its likely severity if/when it occurs. Finally, our findings of within-person effects underscore that at no point in a disaster’s progression should leaders give up on bolstering effective action.
Limitations
In the absence of gold standard, pandemic-specific measures at the time of data collection, the best available measures were used. Measures from the PhenX toolkit Reference Krzyzanowski, Terry and Williams11 were used where possible, for consistency with other early COVID-19 studies. Interpretation of descriptive data was limited by the lack of established normative scores. While post hoc sensitivity analysis showed that the final sample size was sufficient to detect small effects, the small sample size and specific demographics limit generalizability. Other disaster-vulnerable populations not included, or not the focus of this study, include African Americans, families with children, older adults, undocumented US residents, and other housing insecure populations. Although the longitudinal design revealed contextual, within-person effects that cannot be inferred from cross-sectional studies, causal inference is not possible. While we found within-person effects for collective efficacy in predicting disaster preparedness, acculturation is not constant, so collectivism may have been a confounding variable. Cross-cultural sampling with collectivism as a covariate could clarify reasons for the importance of collective efficacy for PPRBs, compared with self-efficacy.
Conclusions
Intersectionally disaster-vulnerable individuals, such as Asian international students communally-housed during COVID-19 due to housing insecurity, must be considered when formulating policies and guidelines and must be the focus of concentrated preparedness efforts. For housing insecure, predominantly international, university students and their partners who were quarantined communally during early COVID-19, weekly fluctuations in collective efficacy and perceived severity positively predicted pandemic preparedness/response behaviors. While these correlational findings should not be overstated, public health information about disasters already involves messages about risk perception, fear appeals, and confidence, so accurate risk perception, not fear appeals, should be highlighted in preparedness/response guidelines. Initiatives to promote collective actions like vaccination, mask-wearing, and social distancing might benefit from endeavoring to bolster collective efficacy. Initiatives involving self-efficacy may benefit from expanding to collective efficacy.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/dmp.2023.87
Acknowledgments
We thank the Office of International Programs at University of Mississippi and Yash Bhambhani, PhD, for their assistance. The majority of this research was conducted while Drs. Weber, Torres, and Ho were graduate students with the Department of Psychology and the Clinical-Disaster Research Center at University of Mississippi.
Funding statement
This research was supported by a Quick Response award from the Natural Hazards Center at University of Colorado (Award #1635593). The Quick Response program is based on work supported by the National Science Foundation. Writing of this manuscript was partially financially supported by the Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowship Program in Mental Illness Research and Treatment. Any opinions, findings, conclusions, or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the Natural Hazards Center, the National Science Foundation, the Department of Veterans Affairs, the United States Government, or the academic institutions with which the authors are affiliated.
Competing interest
The authors have no conflicts of interest to declare.





 Open access
Open access